
Hematological Toxicities with PARP Inhibitors in Prostate Cancer: A Systematic Review and Meta-Analysis of Phase II/III Randomized Controlled Trials

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Analysis
3. Results
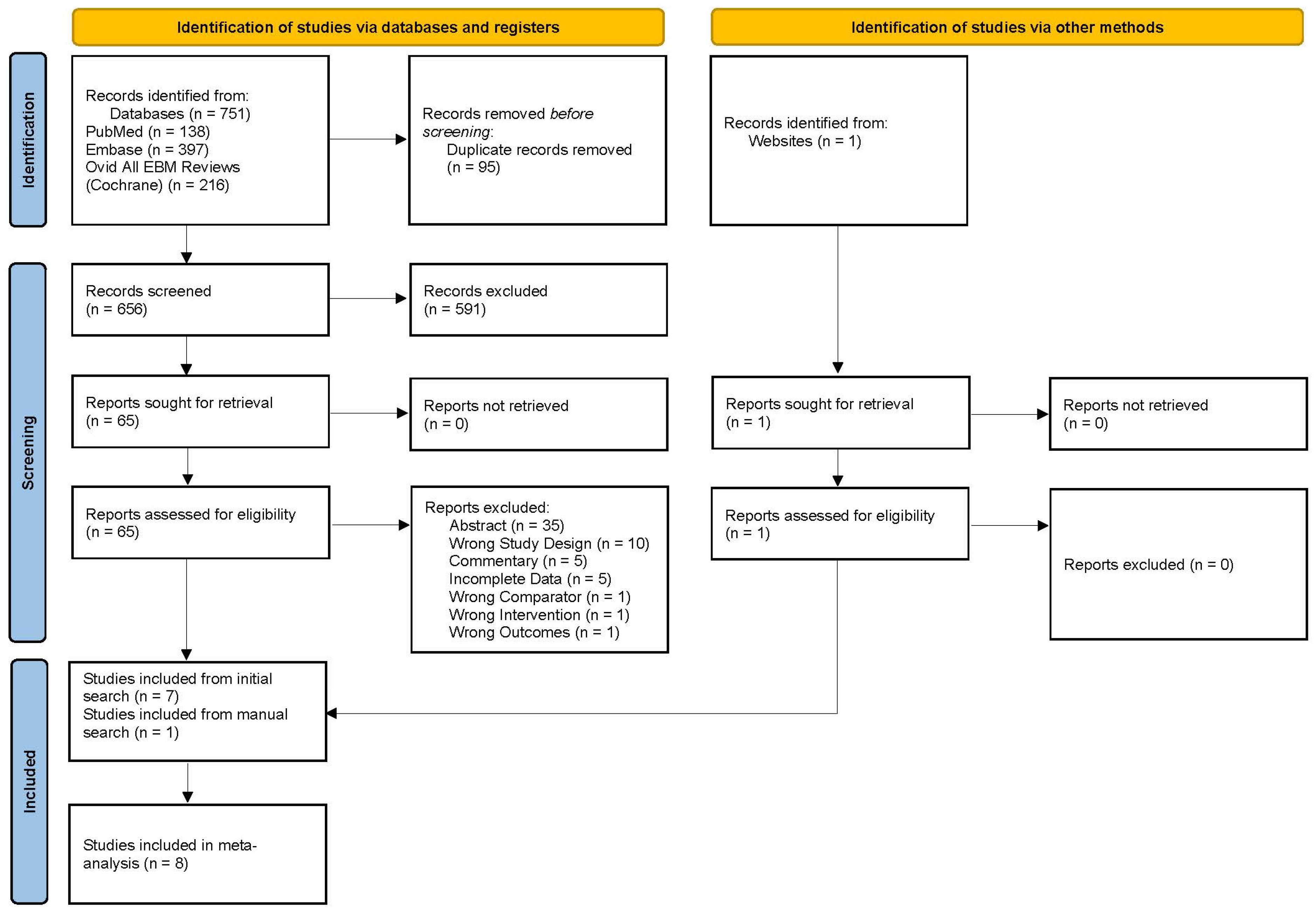
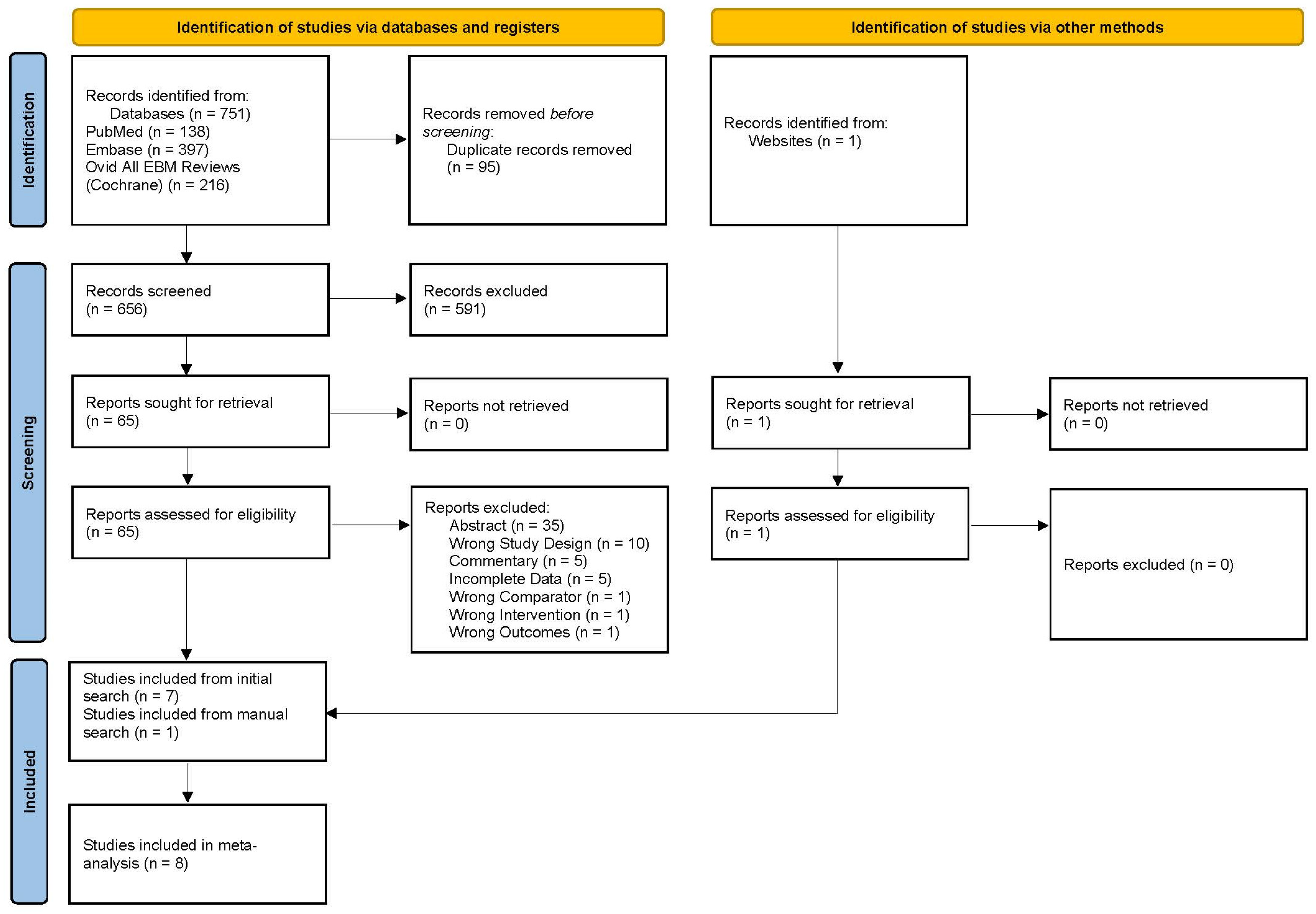
3.1. Study Selection and Population Characteristics
3.2. Risk of Bias and Quality of Evidence
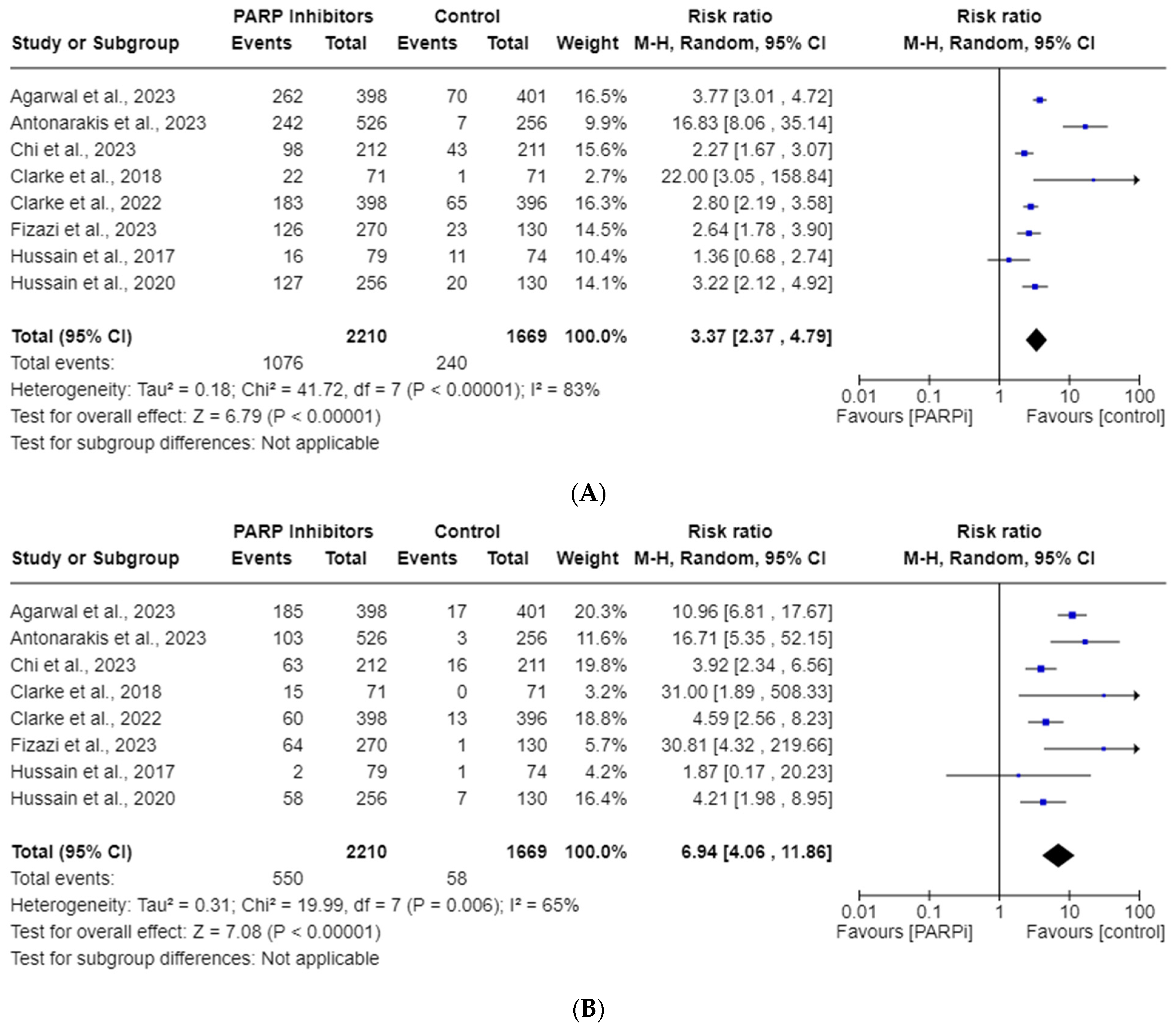
3.3. PARPi Risk of All-Grade and High-Grade Anemia
3.4. PARPi Risk of All-Grade and High-Grade Thrombocytopenia
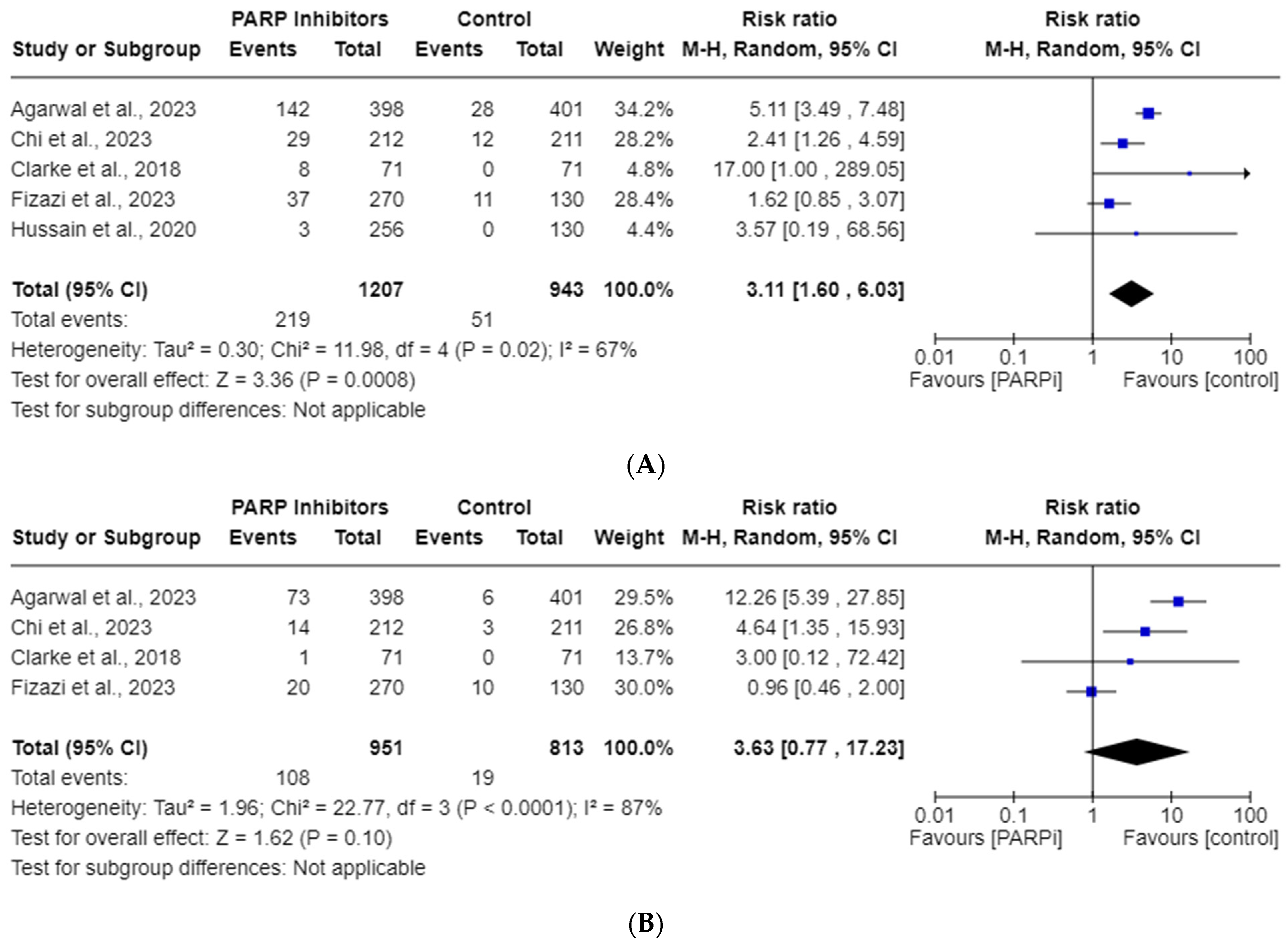
3.5. PARPi Risk of All-Grade and High-Grade Neutropenia
3.6. Subgroup Analysis
3.7. Publication Bias
4. Discussion
4.1. PARP Trapping—A Plausible Mechanism of Hematological Toxicities?
4.2. Management of Hematological AEs
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Sekhoacha, M.; Riet, K.; Motloung, P.; Gumenku, L.; Adegoke, A.; Mashele, S. Prostate Cancer Review: Genetics, Diagnosis, Treatment Options, and Alternative Approaches. Molecules 2022, 27, 5730. [Google Scholar] [CrossRef]
- Kim, T.J.; Lee, Y.H.; Koo, K.C. Current Status and Future Perspectives of Androgen Receptor Inhibition Therapy for Prostate Cancer: A Comprehensive Review. Biomolecules 2021, 11, 492. [Google Scholar] [CrossRef]
- Gillessen, S.; Armstrong, A.; Attard, G.; Beer, T.M.; Beltran, H.; Bjartell, A.; Bossi, A.; Briganti, A.; Bristow, R.G.; Bulbul, M.; et al. Management of Patients with Advanced Prostate Cancer: Report from the Advanced Prostate Cancer Consensus Conference 2021. Eur. Urol. 2022, 82, 115–141. [Google Scholar] [CrossRef]
- Vogl, U.M.; Beer, T.M.; Davis, I.D.; Shore, N.D.; Sweeney, C.J.; Ost, P.; Attard, G.; Bossi, A.; de Bono, J.; Drake, C.G.; et al. Lack of consensus identifies important areas for future clinical research: Advanced Prostate Cancer Consensus Conference (APCCC) 2019 findings. Eur. J. Cancer 2022, 160, 24–60. [Google Scholar] [CrossRef]
- Sayegh, N.; Swami, U.; Agarwal, N. Recent Advances in the Management of Metastatic Prostate Cancer. JCO Oncol. Pract. 2022, 18, 45–55. [Google Scholar] [CrossRef]
- Tisseverasinghe, S.; Bahoric, B.; Anidjar, M.; Probst, S.; Niazi, T. Advances in PARP Inhibitors for Prostate Cancer. Cancers 2023, 15, 1849. [Google Scholar] [CrossRef]
- Sumanasuriya, S.; De Bono, J. Treatment of Advanced Prostate Cancer-A Review of Current Therapies and Future Promise. Cold Spring Harb. Perspect Med. 2018, 8, a030635. [Google Scholar] [CrossRef] [PubMed]
- Ku, S.Y.; Gleave, M.E.; Beltran, H. Towards precision oncology in advanced prostate cancer. Nat. Rev. Urol. 2019, 16, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Rose, M.; Burgess, J.T.; O’Byrne, K.; Richard, D.J.; Bolderson, E. PARP Inhibitors: Clinical Relevance, Mechanisms of Action and Tumor Resistance. Front. Cell Dev. Biol. 2020, 8, 564601. [Google Scholar] [CrossRef] [PubMed]
- Caron, M.-C.; Sharma, A.K.; O’Sullivan, J.; Myler, L.R.; Ferreira, M.T.; Rodrigue, A.; Coulombe, Y.; Ethier, C.; Gagné, J.-P.; Langelier, M.-F.; et al. Poly(ADP-ribose) polymerase-1 antagonizes DNA resection at double-strand breaks. Nat. Commun. 2019, 10, 2954. [Google Scholar] [CrossRef] [PubMed]
- Ashworth, A. A synthetic lethal therapeutic approach: Poly(ADP) ribose polymerase inhibitors for the treatment of cancers deficient in DNA double-strand break repair. J. Clin. Oncol. 2008, 26, 3785–3790. [Google Scholar] [CrossRef] [PubMed]
- Bryant, H.E.; Schultz, N.; Thomas, H.D.; Parker, K.M.; Flower, D.; Lopez, E.; Kyle, S.; Meuth, M.; Curtin, N.J.; Helleday, T. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature 2007, 447, 346. [Google Scholar] [CrossRef]
- Taylor, A.K.; Kosoff, D.; Emamekhoo, H.; Lang, J.M.; Kyriakopoulos, C.E. PARP inhibitors in metastatic prostate cancer. Front. Oncol. 2023, 13, 1159557. [Google Scholar] [CrossRef]
- Catalano, M.; Generali, D.; Gatti, M.; Riboli, B.; Paganini, L.; Nesi, G.; Roviello, G. DNA repair deficiency as circulating biomarker in prostate cancer. Front. Oncol. 2023, 13, 1115241. [Google Scholar] [CrossRef]
- Robinson, D.; Van Allen, E.M.; Wu, Y.M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.M.; Montgomery, B.; Taplin, M.E.; Pritchard, C.C.; Attard, G.; et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef]
- Mateo, J.; Carreira, S.; Sandhu, S.; Miranda, S.; Mossop, H.; Perez-Lopez, R.; Nava Rodrigues, D.; Robinson, D.; Omlin, A.; Tunariu, N.; et al. DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer. N. Engl. J. Med. 2015, 373, 1697–1708. [Google Scholar] [CrossRef]
- AUA University. Episode 208: The Role of PARP Inhibitors in Advanced Prostate Cancer; AUA University: Linthicum, MD, USA, 2023. [Google Scholar]
- Nuhn, P.; De Bono, J.S.; Fizazi, K.; Freedland, S.J.; Grilli, M.; Kantoff, P.W.; Sonpavde, G.; Sternberg, C.N.; Yegnasubramanian, S.; Antonarakis, E.S. Update on Systemic Prostate Cancer Therapies: Management of Metastatic Castration-resistant Prostate Cancer in the Era of Precision Oncology. Eur. Urol. 2019, 75, 88–99. [Google Scholar] [CrossRef]
- Lowrance, W.; Dreicer, R.; Jarrard, D.F.; Scarpato, K.R.; Kim, S.K.; Kirkby, E.; Buckley, D.I.; Griffin, J.C.; Cookson, M.S. Updates to Advanced Prostate Cancer: AUA/SUO Guideline (2023). J. Urol. 2023, 209, 1082–1090. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves Niraparib and Abiraterone Acetate Plus Prednisone for BRCA-Mutated Metastatic Castration-Resistant Prostate Cancer. Last Updated 11 August 2023. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-niraparib-and-abiraterone-acetate-plus-prednisone-brca-mutated-metastatic-castration (accessed on 12 August 2023).
- Abida, W.; Patnaik, A.; Campbell, D.; Shapiro, J.; Bryce, A.H.; McDermott, R.; Sautois, B.; Vogelzang, N.J.; Bambury, R.M.; Voog, E.; et al. Rucaparib in Men With Metastatic Castration-Resistant Prostate Cancer Harboring a BRCA1 or BRCA2 Gene Alteration. J. Clin. Oncol. 2020, 38, 3763–3772. [Google Scholar] [CrossRef]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Hussain, M.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 383, 2345–2357. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves Talazoparib with Enzalutamide for HRR Gene-Mutated Metastatic Castration-Resistant Prostate Cancer. Last Updated 20 June 2023. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-talazoparib-enzalutamide-hrr-gene-mutated-metastatic-castration-resistant-prostate (accessed on 12 August 2023).
- U.S. Food and Drug Administration. FDA Approves Olaparib with Abiraterone and Prednisone (or Prednisolone) for BRCA-Mutated Metastatic Castration-Resistant Prostate Cancer. Last Updated 31 May 2023. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-disco-burst-edition-fda-approval-lynparza-olaparib-abiraterone-and-prednisone-brca-mutated (accessed on 12 August 2023).
- Hussain, M.; Daignault-Newton, S.; Twardowski, P.W.; Albany, C.; Stein, M.N.; Kunju, L.P.; Siddiqui, J.; Wu, Y.M.; Robinson, D.; Lonigro, R.J.; et al. Targeting Androgen Receptor and DNA Repair in Metastatic Castration-Resistant Prostate Cancer: Results From NCI 9012. J. Clin. Oncol. 2018, 36, 991–999. [Google Scholar] [CrossRef]
- Ruiz-Schutz, V.C.; Gomes, L.M.; Mariano, R.C.; de Almeida, D.V.P.; Pimenta, J.M.; Dal Molin, G.Z.; Kater, F.R.; Yamamura, R.; Correa Neto, N.F.; Maluf, F.C.; et al. Risk of fatigue and anemia in patients with advanced cancer treated with olaparib: A meta-analysis of randomized controlled trials. Crit. Rev. Oncol. Hematol. 2019, 141, 163–173. [Google Scholar] [CrossRef]
- Ricci, A.D.; Rizzo, A.; Novelli, M.; Tavolari, S.; Palloni, A.; Tober, N.; Abbati, F.; Mollica, V.; Lorenzo, S.D.E.; Turchetti, D.; et al. Specific Toxicity of Maintenance Olaparib Versus Placebo in Advanced Malignancies: A Systematic Review and Meta-analysis. Anticancer. Res. 2020, 40, 597–608. [Google Scholar] [CrossRef]
- Zhou, J.X.; Feng, L.J.; Zhang, X. Risk of severe hematologic toxicities in cancer patients treated with PARP inhibitors: A meta-analysis of randomized controlled trials. Drug Des. Devel. Ther. 2017, 11, 3009–3017. [Google Scholar] [CrossRef]
- Wang, C.; Li, J. Haematologic toxicities with PARP inhibitors in cancer patients: An up-to-date meta-analysis of 29 randomized controlled trials. J. Clin. Pharm. Ther. 2021, 46, 571–584. [Google Scholar] [CrossRef]
- Shu, Y.; Ding, Y.; He, X.; Liu, Y.; Wu, P.; Zhang, Q. Hematological toxicities in PARP inhibitors: A real-world study using FDA adverse event reporting system (FAERS) database. Cancer Med. 2023, 12, 3365–3375. [Google Scholar] [CrossRef]
- Agarwal, N.; Azad, A.A.; Carles, J.; Fay, A.P.; Matsubara, N.; Heinrich, D.; Szczylik, C.; De Giorgi, U.; Young Joung, J.; Fong, P.C.C.; et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomised, placebo-controlled, phase 3 trial. Lancet 2023, 402, 291–303. [Google Scholar] [CrossRef]
- Antonarakis, E.S.; Park, S.H.; Goh, J.C.; Shin, S.J.; Lee, J.L.; Mehra, N.; McDermott, R.; Sala-Gonzalez, N.; Fong, P.C.; Greil, R.; et al. Pembrolizumab Plus Olaparib for Patients With Previously Treated and Biomarker-Unselected Metastatic Castration-Resistant Prostate Cancer: The Randomized, Open-Label, Phase III KEYLYNK-010 Trial. J. Clin. Oncol. 2023, 41, 3839–3850. [Google Scholar] [CrossRef]
- Chi, K.N.; Rathkopf, D.; Smith, M.R.; Efstathiou, E.; Attard, G.; Olmos, D.; Lee, J.Y.; Small, E.J.; Gomes, A.J.P.d.S.; Roubaud, G.; et al. Niraparib and Abiraterone Acetate for Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2023, 41, 3339–3351. [Google Scholar] [CrossRef]
- Fizazi, K.; Piulats, J.M.; Reaume, M.N.; Ostler, P.; McDermott, R.; Gingerich, J.R.; Pintus, E.; Sridhar, S.S.; Bambury, R.M.; Emmenegger, U.; et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N. Engl. J. Med. 2023, 388, 719–732. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- National Cancer Institute (NIH). Common Terminology Criteria for Adverse Events (CTCAE). Last Updated April 2021. Available online: https://ctep.cancer.gov/ (accessed on 9 June 2023).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Clarke, N.; Wiechno, P.; Alekseev, B.; Sala, N.; Jones, R.; Kocak, I.; Chiuri, V.E.; Jassem, J.; Fléchon, A.; Redfern, C.; et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer: A randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 2018, 19, 975–986. [Google Scholar] [CrossRef]
- Clarke, N.W.; Armstrong, A.J.; Thiery-Vuillemin, A.; Oya, M.; Shore, N.; Loredo, E.; Procopio, G.; de Menezes, J.; Girotto, G.; Arslan, C. Abiraterone and olaparib for metastatic castration-resistant prostate cancer. NEJM Evid. 2022, 1, EVIDoa2200043. [Google Scholar] [CrossRef]
- Mateo, J.; Porta, N.; Bianchini, D.; McGovern, U.; Elliott, T.; Jones, R.; Syndikus, I.; Ralph, C.; Jain, S.; Varughese, M.; et al. Olaparib in patients with metastatic castration-resistant prostate cancer with DNA repair gene aberrations (TOPARP-B): A multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2020, 21, 162–174. [Google Scholar] [CrossRef]
- Smith, M.R.; Scher, H.I.; Sandhu, S.; Efstathiou, E.; Lara, P.N., Jr.; Yu, E.Y.; George, D.J.; Chi, K.N.; Saad, F.; Ståhl, O.; et al. Niraparib in patients with metastatic castration-resistant prostate cancer and DNA repair gene defects (GALAHAD): A multicentre, open-label, phase 2 trial. Lancet Oncol. 2022, 23, 362–373. [Google Scholar] [CrossRef]
- de Bono, J.S.; Mehra, N.; Scagliotti, G.V.; Castro, E.; Dorff, T.; Stirling, A.; Stenzl, A.; Fleming, M.T.; Higano, C.S.; Saad, F.; et al. Talazoparib monotherapy in metastatic castration-resistant prostate cancer with DNA repair alterations (TALAPRO-1): An open-label, phase 2 trial. Lancet Oncol. 2021, 22, 1250–1264. [Google Scholar] [CrossRef]
- Chi, K.N.; Fleshner, N.; Chiuri, V.E.; Van Bruwaene, S.; Hafron, J.; McNeel, D.G.; De Porre, P.; Maul, R.S.; Daksh, M.; Zhong, X.; et al. Niraparib with Abiraterone Acetate and Prednisone for Metastatic Castration-Resistant Prostate Cancer: Phase II QUEST Study Results. Oncologist 2023, 28, e309–e312. [Google Scholar] [CrossRef]
- Karzai, F.; VanderWeele, D.; Madan, R.A.; Owens, H.; Cordes, L.M.; Hankin, A.; Couvillon, A.; Nichols, E.; Bilusic, M.; Beshiri, M.L.; et al. Activity of durvalumab plus olaparib in metastatic castration-resistant prostate cancer in men with and without DNA damage repair mutations. J. Immunother Cancer 2018, 6, 141. [Google Scholar] [CrossRef]
- Fizazi, K.; Retz, M.; Petrylak, D.P.; Goh, J.C.; Perez-Gracia, J.; Lacombe, L.; Zschäbitz, S.; Burotto, M.; Mahammedi, H.; Gravis, G.; et al. Nivolumab plus rucaparib for metastatic castration-resistant prostate cancer: Results from the phase 2 CheckMate 9KD trial. J. Immunother Cancer 2022, 10, e004761. [Google Scholar] [CrossRef]
- Yap, T.A.; Bardia, A.; Dvorkin, M.; Galsky, M.D.; Beck, J.T.; Wise, D.R.; Karyakin, O.; Rubovszky, G.; Kislov, N.; Rohrberg, K.; et al. Avelumab Plus Talazoparib in Patients With Advanced Solid Tumors: The JAVELIN PARP Medley Nonrandomized Controlled Trial. JAMA Oncol. 2023, 9, 40–50. [Google Scholar] [CrossRef]
- Reichert, Z.R.; Devitt, M.E.; Alumkal, J.J.; Smith, D.C.; Caram, M.V.; Palmbos, P.; Vaishampayan, U.N.; Alva, A.S.; Braun, T.; Yentz, S.E.; et al. Targeting resistant prostate cancer, with or without DNA repair defects, using the combination of ceralasertib (ATR inhibitor) and olaparib (the TRAP trial). J. Clin. Oncol. 2022, 40, 88. [Google Scholar] [CrossRef]
- Bao, S.; Yue, Y.; Hua, Y.; Zeng, T.; Yang, Y.; Yang, F.; Yan, X.; Sun, C.; Yang, M.; Fu, Z.; et al. Safety profile of poly (ADP-ribose) polymerase (PARP) inhibitors in cancer: A network meta-analysis of randomized controlled trials. Ann. Transl. Med. 2021, 9, 1229. [Google Scholar] [CrossRef]
- Sultan, A.; Swarup, S.; Zaw, M.; Han, M.M.; Myat, Y.M.; Aung, H.H.; Zin, M.M.M.; Panigrahi, K.; Thein, K.Z. A systematic review and meta- analysis of randomized controlled trials to evaluate the risk of hematological toxicities in patients with cancer treated with poly adenosine diphosphate ribose polymerase (PARP) inhibitors. J. Clin. Oncol. 2018, 36, 217. [Google Scholar] [CrossRef]
- Rizzo, A.; Mollica, V.; Merler, S.; Morelli, F.; Sorgentoni, G.; Oderda, M.; Santoni, M.; Massari, F. Incidence of grade 3–4 adverse events, dose reduction, and treatment discontinuation in castration-resistant prostate cancer patients receiving PARP inhibitors: A meta-analysis. Expert Opin. Drug Metab. Toxicol. 2022, 18, 235–240. [Google Scholar] [CrossRef]
- Guo, X.X.; Wu, H.L.; Shi, H.Y.; Su, L.; Zhang, X. The efficacy and safety of olaparib in the treatment of cancers: A meta-analysis of randomized controlled trials. Cancer Manag. Res. 2018, 10, 2553–2562. [Google Scholar] [CrossRef]
- Nindra, U.; Hong, J.H.; Balakrishnar, B.; Pal, A.; Chua, W. Review of Toxicities of PARP Inhibitors in Metastatic Castrate Resistant Prostate Cancer. Clin. Genitourin. Cancer 2023, 21, 183–193. [Google Scholar] [CrossRef]
- Hao, J.; Liu, Y.; Zhang, T.; He, J.; Zhao, H.; An, R.; Xue, Y. Efficacy and safety of PARP inhibitors in the treatment of advanced ovarian cancer: An updated systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Oncol./Hematol. 2021, 157, 103145. [Google Scholar] [CrossRef]
- Ren, N.; Zhang, L.; Yu, J.; Guan, S.; Dai, X.; Sun, L.; Ying, M. Efficacy and Safety of PARP Inhibitor Combination Therapy in Recurrent Ovarian Cancer: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 638295. [Google Scholar] [CrossRef]
- Sayyid, R.K.; Klaassen, Z.; Berlin, A.; Roy, S.; Brandão, L.R.; Bernardino, R.; Chavarriaga, J.; Jiang, D.M.; Spratt, D.E.; Fleshner, N.E.; et al. Poly(adenosine diphosphate-ribose) polymerase inhibitor combinations in first-line metastatic castrate-resistant prostate cancer setting: A systematic review and meta-analysis. BJU Int. 2023. online ahead of print. [Google Scholar] [CrossRef]
- Hopkins, T.A.; Shi, Y.; Rodriguez, L.E.; Solomon, L.R.; Donawho, C.K.; DiGiammarino, E.L.; Panchal, S.C.; Wilsbacher, J.L.; Gao, W.; Olson, A.M.; et al. Mechanistic Dissection of PARP1 Trapping and the Impact on In Vivo Tolerability and Efficacy of PARP Inhibitors. Mol. Cancer Res. 2015, 13, 1465–1477. [Google Scholar] [CrossRef]
- Farrés, J.; Llacuna, L.; Martin-Caballero, J.; Martínez, C.; Lozano, J.J.; Ampurdanés, C.; López-Contreras, A.J.; Florensa, L.; Navarro, J.; Ottina, E.; et al. PARP-2 sustains erythropoiesis in mice by limiting replicative stress in erythroid progenitors. Cell Death Differ. 2015, 22, 1144–1157. [Google Scholar] [CrossRef]
- Lin, X.; Jiang, W.; Rudolph, J.; Lee, B.J.; Luger, K.; Zha, S. PARP inhibitors trap PARP2 and alter the mode of recruitment of PARP2 at DNA damage sites. Nucleic. Acids Res. 2022, 50, 3958–3973. [Google Scholar] [CrossRef]
- Murai, J.; Huang, S.-y.N.; Das, B.B.; Renaud, A.; Zhang, Y.; Doroshow, J.H.; Ji, J.; Takeda, S.; Pommier, Y. Trapping of PARP1 and PARP2 by Clinical PARP Inhibitors. Cancer Res. 2012, 72, 5588–5599. [Google Scholar] [CrossRef]
- Hopkins, T.A.; Ainsworth, W.B.; Ellis, P.A.; Donawho, C.K.; DiGiammarino, E.L.; Panchal, S.C.; Abraham, V.C.; Algire, M.A.; Shi, Y.; Olson, A.M.; et al. PARP1 Trapping by PARP Inhibitors Drives Cytotoxicity in Both Cancer Cells and Healthy Bone Marrow. Mol. Cancer Res. 2019, 17, 409–419. [Google Scholar] [CrossRef]
- Gilreath, J.A.; Stenehjem, D.D.; Rodgers, G.M. Diagnosis and treatment of cancer-related anemia. Am. J. Hematol. 2014, 89, 203–212. [Google Scholar] [CrossRef]
- Demetri, G.D.; Kris, M.; Wade, J.; Degos, L.; Cella, D. Quality-of-life benefit in chemotherapy patients treated with epoetin alfa is independent of disease response or tumor type: Results from a prospective community oncology study. Procrit Study Group. J. Clin. Oncol. 1998, 16, 3412–3425. [Google Scholar] [CrossRef] [PubMed]
- Al-Samkari, H. Thrombopoietin receptor agonists for chemotherapy-induced thrombocytopenia: A new solution for an old problem. Hematology 2022, 2022, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Giovannetti, E.; Zinzani, P.L.; Danesi, R. Pharmacologic rationale for early G-CSF prophylaxis in cancer patients and role of pharmacogenetics in treatment optimization. Crit. Rev. Oncol. Hematol. 2009, 72, 21–44. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Yamada, Y. Efficacy of oral ferric citrate hydrate treatment for anemia caused by niraparib: A case report. J. Med. Case Rep. 2022, 16, 440. [Google Scholar] [CrossRef] [PubMed]
- Yohannan, B.; McIntyre, K.; Feldman, M. Severe folate deficiency anemia associated with the use of a PARP inhibitor (olaparib) in a patient with fallopian tube cancer. Case Rep. Intern. Med. 2018, 6, 1. [Google Scholar] [CrossRef]
- Dirix, L.; Swaisland, H.; Verheul, H.M.; Rottey, S.; Leunen, K.; Jerusalem, G.; Rolfo, C.; Nielsen, D.; Molife, L.R.; Kristeleit, R.; et al. Effect of Itraconazole and Rifampin on the Pharmacokinetics of Olaparib in Patients With Advanced Solid Tumors: Results of Two Phase I Open-label Studies. Clin. Ther. 2016, 38, 2286–2299. [Google Scholar] [CrossRef] [PubMed]
- Aoki, D.; Chiyoda, T. PARP inhibitors and quality of life in ovarian cancer. Lancet Oncol. 2018, 19, 1012–1014. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Study Name, Country | Pub. Year | NCT Number | RCT | Interventions | Sample Size | Median Age (Years) | Baseline Median Serum PSA (ug/L) | Gleason Score ≥ 8 | Median Treatment Duration (Months) | HRR Mutation Status | BRCA 1/2 Mutation Status | Prior Taxane | Most Reported SE * | Drug Discontinuation *b | Dose Reduction *b | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Interventions | Control | PARPi (n) | Control (n) | PARPi (n) | Control (n) | PARPi (n) | Control (n) | PARPi (n, %) | Control (n; %) | PARPi (n) | Control (n) | PARPi (n, %) | Control (n; %) | PARPi (n, %) | Control (n; %) | PARPi (n, %) | Control (n; %) | PARPi (n, %) | Control (n; %) | PARPi (n, %) | Control (n; %) | PARPi (n, %) | Control (n; %) | |||||
| Agarwal et al. [33] | TALAPRO-2, USA a | 2023 | NCT03395197 | III | Talazoparib and Enzalutamide | Placebo and Enzalutamide | 402 | 403 | 71 | 71 | 18.2 | 16.2 | 281 (70) | 283 (70) | 19.8 | 16.1 | 85 (21) | 84 (21) | 27 (7) | 32 (8) | 86 (21) | 93 (23) | Anemia 262 (66) | Fatigue 118 (29) | 76 (19) | 49 (12) | 223 (56) | 29 (7) |
| Antonarakis et al. [34] | KEYLYNK-010, USA a | 2023 | NCT03834519 | III | Olaparib and Pembrolizumab | Abireterone or Enzalutamide | 529 | 264 | 71 | 69 | 52.9 | 42.6 | 367 (69.4) | 184 (69.7) | 5 | 4.1 | 138 (26.1) | 59 (22.3) | 52 (9.8) | 24 (9.1) | 529 (100) | 264 (100) | Anemia 242 (46) | Fatigue 42 (16.4) | 57 (10.8) | 4 (1.6) | NR | NR |
| Chi et al. [35] | MAGNITUDE, Canada a | 2023 | NCT03748641 | III | Niraparib and Abiraterone plus Prednisone | Placebo and Abiraterone plus Prednisone | 212 | 211 | 69 | 69 | 21.4 | 17.4 | 144 (68.2) | 142 (67.6) | 13.8 | 12.1 | 212 (100) | 211 (100) | 98 (46.3) | 92 (43.6) | 41 (19.3) | 44 (20.9) | Anemia 98 (46.2) | Hypertension/ Back Pain 44 (20.9) | 23 (10.8) | 10 (4.7) | 42 (19.8) | 7 (3.3) |
| Clarke et al. [42] | PROpel, UK a | 2018 | NCT01972217 | II | Olaparib and Abiraterone plus Prednisone or Prednisolone | Placebo and Abiraterone plus Prednisone or Prednisolone | 71 | 71 | 70 | 67 | 86 | 47 | NR | NR | 10.3 | 8.4 | 11 (15) | 10 (14) | 2 (2.8) | 4 (5.6) | 71 (100) | 71 (100) | Nausea 27 (38) | Nausea 14 (20) | 21 (30) | 7 (10) | 13 (18) | 0 (0) |
| Clarke et al. [43] | PROpel, UK a | 2022 | NCT03732820 | III | Olaparib and Abiraterone plus Prednisone or Prednisolone | Placebo and Abiraterone plus Prednisone or Prednisolone | 399 | 397 | 69 | 70 | 17.9 | 16.8 | 265 (66.4) | 258 (65) | 17.5 | 15.7 | 111 (27.8) | 115 (29.0) | 47 (11.8) | 38 (9.6) | 97 (24.3) | 98 (24.7) | Anemia 183 (46.0) | Fatigue 112 (28.3) | 55 (13.8) | 31 (7.8) | 80 (20.1) | 22 (5.6) |
| Fizazi et al. [36] | TRITON3, France a | 2023 | NCT02975934 | III | Rucaparib | Docetaxel or Abiraterone or Enzalatuamide | 270 | 135 | 70 | 71 | 26.9 | 28.8 | 173 (64) | 96 (71) | 8.3 | 5.1 | 270 (100) | 135 (100) | 201 (74) | 101 (75) | 63 (23) | 28 (21) | Fatigue 165 (61) | Fatigue 82 (63) | 40 (15) | 28 (22) | 104 (39) | 32 (25) |
| Hussain et al. [27] | NCI 9012, USA | 2017 | NCT01576172 | II | Veliparib and Abiraterone plus Prednisone | Abiraterone plus Prednisone | 79 | 74 | 68 | 69 | 36.4 | 32.7 | NR | NR | 9 | 9 | UNK | UNK | UNK | UNK | 23 (30.3) | 16 (20.8) | Nausea 42 (53) | Fatigue 20 (27) | NR | NR | NR | NR |
| Hussain et al. [24] | PROfound, USA a | 2020 | NCT02987543 | III | Olaparib | Enzalutamide or Abiraterone plus Prednisone | 256 | 131 | 69 | 69 | 68.2 | 106.5 | 183 (71) | 95 (73) | 7.6 | 3.9 | 256 (100) | 131 (100) | 89 (35) | 52 (40) | 170 (66) | 84 (64) | Anemia 127 (50) | Fatigue 43 (33) | 51 (20) | 11 (8) | 60 (23) | 7 (5) |
| All-Grade | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Anemia | Thrombocytopenia | Neutropenia | |||||||
| RR (95% CI) | p-Value | p-Value for Overall Subgroup Differences | RR (95% CI) | p-Value | p-Value for Overall Subgroup Differences | RR (95% CI) | p-Value | p-Value for Overall Subgroup Differences | |
| PARPi of Choice | |||||||||
| Niraparib | 2.27 [1.67, 3.07] | <0.00001 | 0.005 | 2.49 [1.49, 4.15] | 0.0005 | 0.03 | 2.41 [1.26, 4.59] | 0.008 | 0.01 |
| Olaparib | 6.01 [2.51, 14.40] | <0.0001 | 4.59 [0.25, 84.56] | 0.31 | 8.05 [1.04, 62.24] | 0.05 | |||
| Rucaparib | 2.64 [1.78, 3.90] | <0.00001 | 48.82 [3.04, 785.15] | 0.006 | 1.62 [0.85, 3.07] | 0.14 | |||
| Talazoparib | 3.77 [3.01, 4.72] | <0.00001 | 7.05 [4.10, 12.13] | <0.00001 | 5.11 [3.49, 7.48] | <0.00001 | |||
| Veliparib | 1.36 [0.68, 2.74] | 0.39 | 2.50 [0.69, 9.06] | 0.16 | NE | NE | |||
| Treatment Duration | |||||||||
| ≤12 Months | 4.43 [1.90, 10.32] | <0.00001 | 0.36 | 9.85 [3.33, 29.16] | <0.0001 | 0.18 | 2.73 [0.74, 10.12] | 0.13 | 0.7 |
| >12 Months | 2.92 [2.19, 3.90] | <0.00001 | 4.48 [3.10, 6.46] | <0.00001 | 3.67 [1.76, 7.65] | 0.0005 | |||
| Monotherapy vs. Combination Therapy | |||||||||
| PARPi vs. Cancer Drug | 2.90 [2.17, 3.86] | <0.00001 | 0.91 | 26.90 [3.72, 194.73] | 0.001 | 0.14 | 1.68 [0.90, 3.14] | 0.1 | 0.07 |
| PARPi plus Cancer Drug vs. Cancer Drug | 4.78 [0.31, 74.80] | 0.27 | 2.50 [0.69, 9.06] | 0.16 | NE | NE | |||
| PARPi plus Cancer Drug vs. Placebo plus Cancer Drug | 3.07 [2.20, 4.29] | <0.00001 | 4.48 [3.10, 6.46] | <0.00001 | 4.01 [2.00, 8.03] | <0.0001 | |||
| Combination Drug | |||||||||
| Abiraterone | 2.44 [1.62, 3.68] | <0.0001 | <0.0001 | 2.49 [1.55, 4.01] | 0.0002 | 0.005 | 4.00 [0.70, 23.00] | 0.12 | 0.79 |
| Enzalutamide | 3.77 [3.01, 4.72] | <0.00001 | 7.05 [4.10, 12.13] | <0.00001 | 5.11 [3.49, 7.48] | <0.00001 | |||
| Pembrolizumab | 16.83 [8.06, 35.14] | <0.00001 | NE | NE | NE | NE | |||
| RCT Trial | |||||||||
| Phase II | 3.03 [1.65, 5.58] | 0.0004 | 0.62 | 2.50 [0.69, 9.06] | 0.16 | 0.26 | 17.00 [1.00, 289.05] | 0.05 | 0.28 |
| Phase III | 3.55 [3.11, 4.04] | <0.00001 | 5.38 [3.73, 7.76] | <0.00001 | 3.57 [2.69, 4.74] | <0.00001 | |||
| High-Grade | |||||||||
| Anemia | Thrombocytopenia | Neutropenia | |||||||
| RR (95% CI) | p-Value | p-Value for Overall Subgroup Differences | RR (95% CI) | p-Value | p-Value for Overall Subgroup Differences | RR (95% CI) | p-Value | p-Value for Overall Subgroup Differences | |
| PARPi of Choice | |||||||||
| Niraparib | 5.15 [2.86, 9.28] | <0.00001 | 0.004 | 2.79 [1.02, 7.60] | 0.05 | 0.48 | 4.64 [1.35, 15.93] | 0.01 | 0.0001 |
| Olaparib | 8.21 [3.76, 17.91] | <0.00001 | NE | NE | 3.00 [0.12, 72.42] | 0.5 | |||
| Rucaparib | 40.08 [5.49, 292.44] | 0.0003 | 15.95 [0.96, 263.84] | 0.05 | 0.96 [0.46, 2.00] | 0.92 | |||
| Talazoparib | 19.62 [11.62, 33.14] | <0.00001 | 7.30 [2.59, 20.59] | 0.0002 | 12.26 [5.39, 27.85] | <0.00001 | |||
| Veliparib | 1.90 [0.17, 21.36] | 0.6 | 4.69 [0.23, 96.05] | 0.32 | NE | NE | |||
| Treatment Duration | |||||||||
| ≤12 Months | 10.22 [5.82, 17.93] | <0.00001 | 0.19 | 11.07 [1.37, 89.44] | 0.02 | 0.46 | 1.02 [0.5, 2.08] | 0.96 | 0.0004 |
| >12 Months | 6.70 [4.98, 9.02] | <0.00001 | 4.79 [2.36, 9.73] | <0.0001 | 8.43 [3.31, 21.49] | <0.00001 | |||
| Monotherapy vs. Combination Therapy | |||||||||
| PARPi vs. Cancer Drug | 9.59 [1.12, 82.12] | 0.04 | 0.94 | 15.95 [0.96, 263.84] | 0.05 | 0.72 | 0.96 [0.46, 2.00] | 0.92 | <0.0001 |
| PARPi plus Cancer Drug vs. Cancer Drug | 7.15 [0.83, 61.45] | 0.07 | 4.69 [0.23, 96.05] | 0.32 | NE | NE | |||
| PARPi plus Cancer Drug vs. Placebo plus Cancer Drug | 6.38 [3.29, 12.39] | <0.00001 | 4.79 [2.36, 9.73] | <0.0001 | 8.43 [4.11, 17.32] | <0.00001 | |||
| Combination Drug | |||||||||
| Abiraterone | 4.27 [2.93, 6.23] | <0.00001 | 0.002 | 2.96 [1.15, 7.67] | 0.03 | 0.21 | 4.41 [1.40, 13.89] | 0.01 | 0.16 |
| Enzalutamide | 10.96 [6.81, 17.67] | <0.00001 | 7.30 [2.59, 20.59] | 0.0002 | 12.26 [5.39, 27.85] | <0.00001 | |||
| Pembrolizumab | 16.71 [5.35, 52.15] | <0.00001 | NE | NE | NE | NE | |||
| RCT Trial | |||||||||
| Phase II | 11.38 [2.20, 58.69] | 0.004 | 0.63 | 4.69 [0.23, 96.05] | 0.32 | 0.91 | 3.00 [0.12, 72.42] | 0.5 | 0.9 |
| Phase III | 7.52 [5.74, 9.86] | <0.00001 | 5.57 [2.78, 11.16] | <0.00001 | 3.75 [0.65, 21.68] | 0.14 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bowling, G.C.; Swargaloganathan, P.; Heintz, C.; Madan, R.A.; Eldhose, B.; Dobi, A.; Chesnut, G.T. Hematological Toxicities with PARP Inhibitors in Prostate Cancer: A Systematic Review and Meta-Analysis of Phase II/III Randomized Controlled Trials. Cancers 2023, 15, 4904. https://doi.org/10.3390/cancers15194904
Bowling GC, Swargaloganathan P, Heintz C, Madan RA, Eldhose B, Dobi A, Chesnut GT. Hematological Toxicities with PARP Inhibitors in Prostate Cancer: A Systematic Review and Meta-Analysis of Phase II/III Randomized Controlled Trials. Cancers. 2023; 15(19):4904. https://doi.org/10.3390/cancers15194904
Chicago/Turabian StyleBowling, Gartrell C., Piragash Swargaloganathan, Carly Heintz, Ravi A. Madan, Binil Eldhose, Albert Dobi, and Gregory T. Chesnut. 2023. "Hematological Toxicities with PARP Inhibitors in Prostate Cancer: A Systematic Review and Meta-Analysis of Phase II/III Randomized Controlled Trials" Cancers 15, no. 19: 4904. https://doi.org/10.3390/cancers15194904
APA StyleBowling, G. C., Swargaloganathan, P., Heintz, C., Madan, R. A., Eldhose, B., Dobi, A., & Chesnut, G. T. (2023). Hematological Toxicities with PARP Inhibitors in Prostate Cancer: A Systematic Review and Meta-Analysis of Phase II/III Randomized Controlled Trials. Cancers, 15(19), 4904. https://doi.org/10.3390/cancers15194904