
Influence of Neoadjuvant Chemotherapy on Survival Outcomes of Radical Cystectomy in Pathologically Proven Positive and Negative Lymph Nodes


 , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
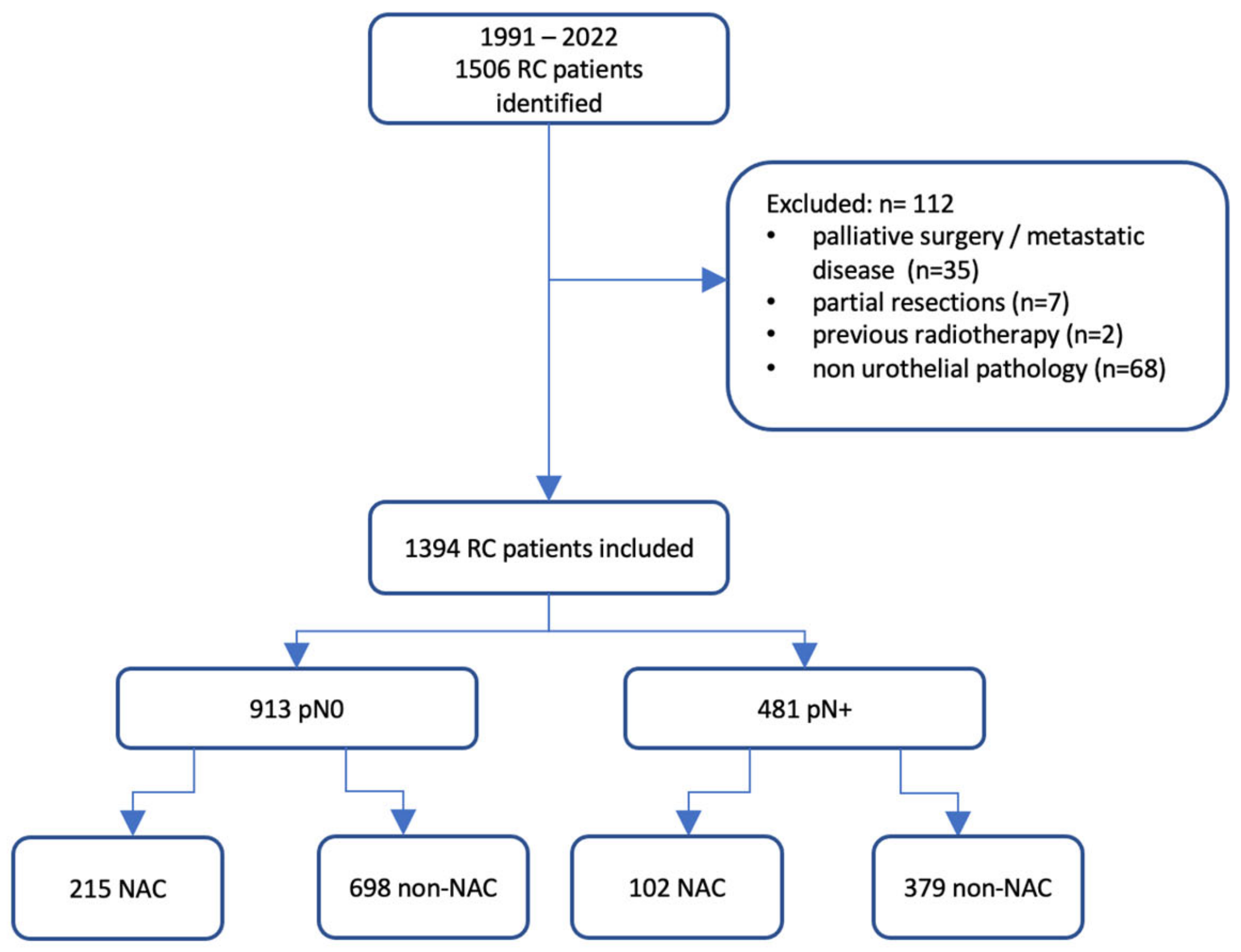
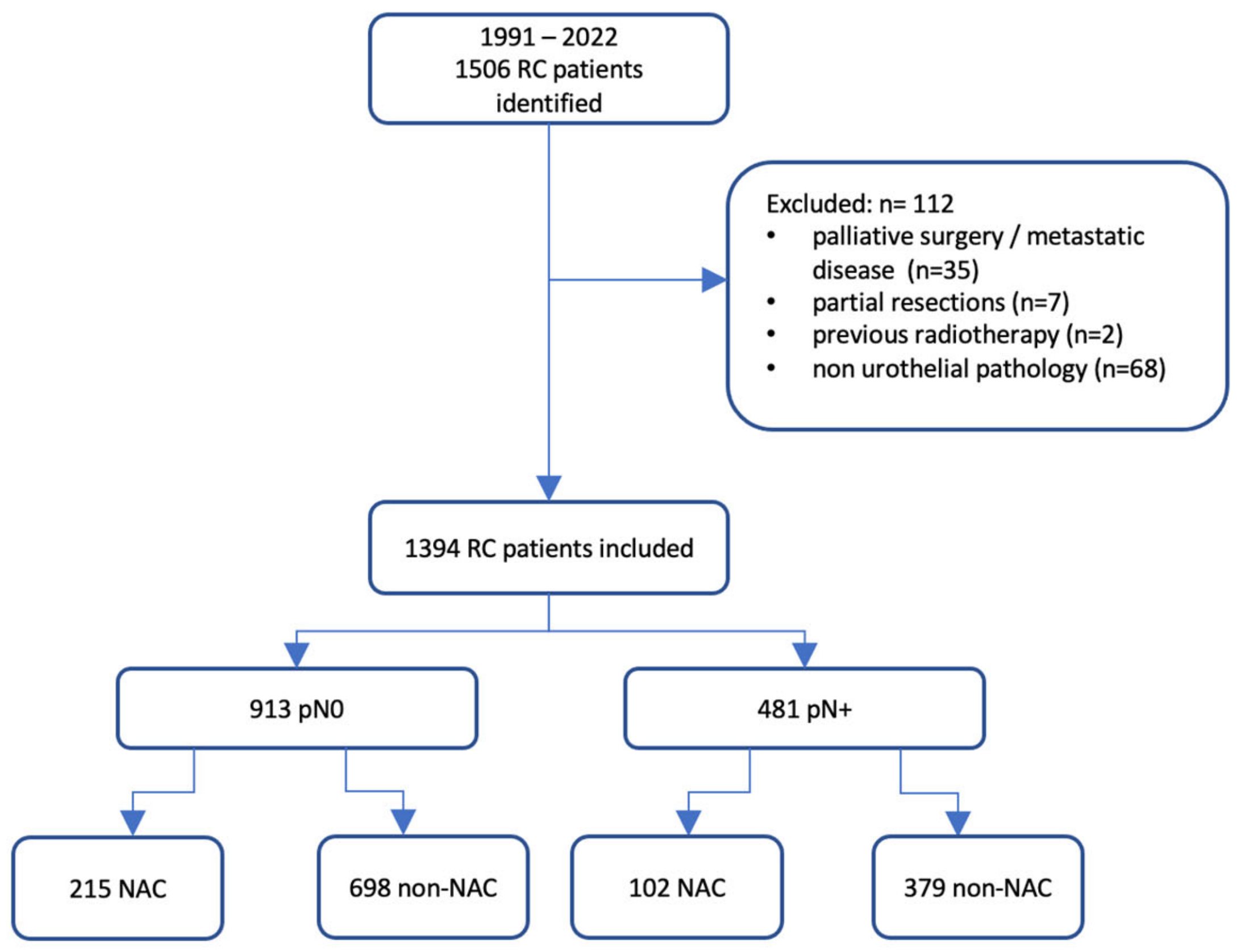
2. Materials and Methods
Statistical Analysis
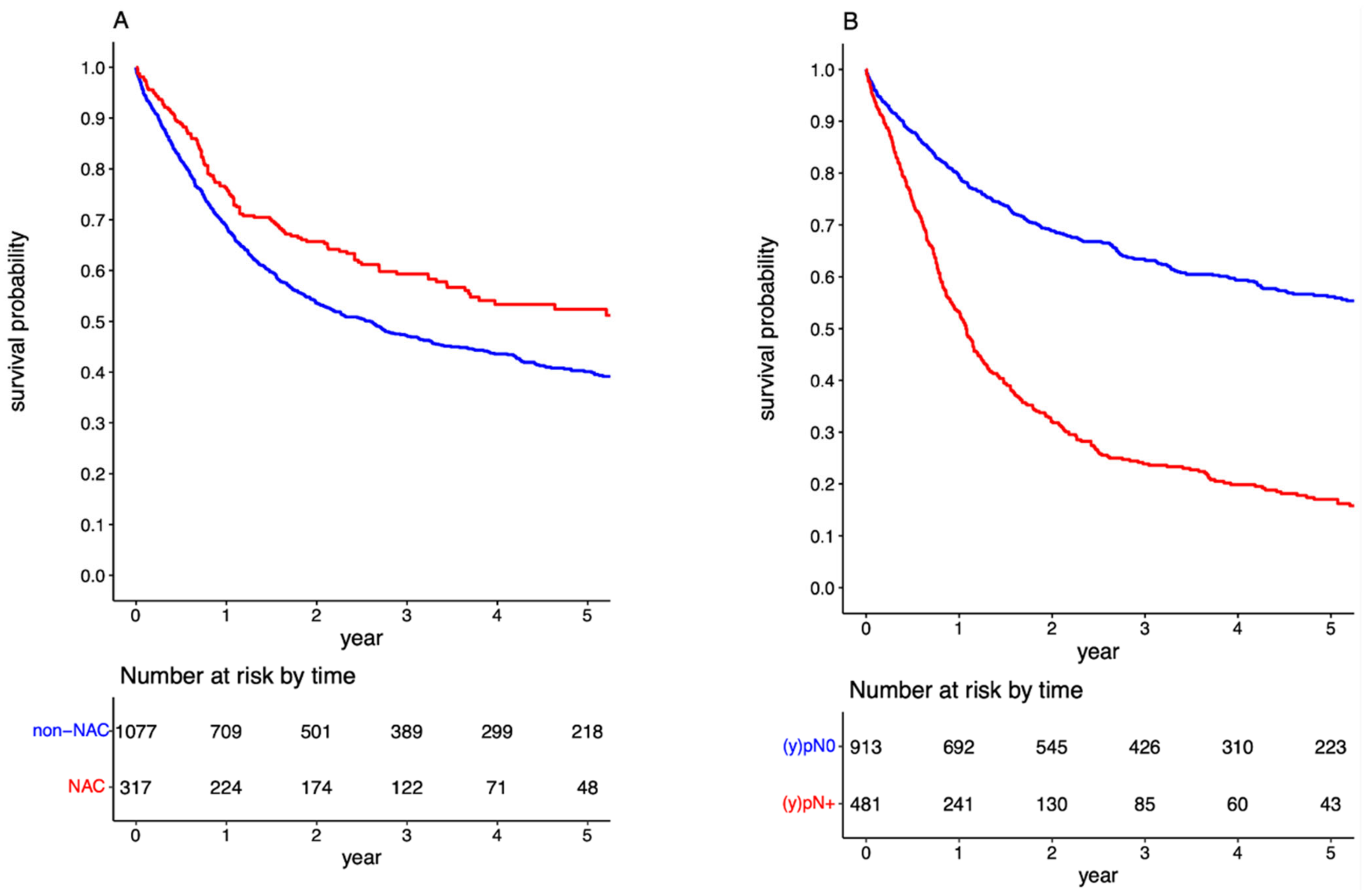
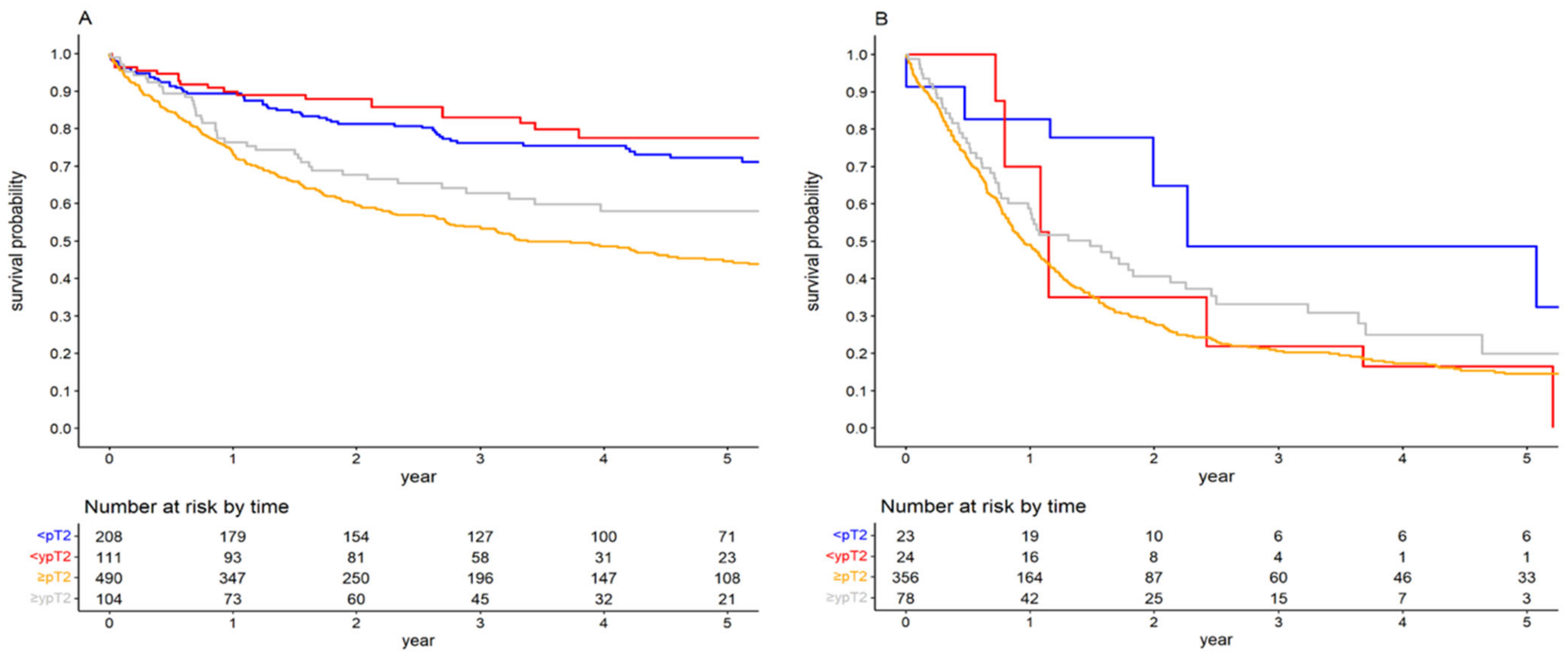
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Møller, C.T.; Støer, N.C.; Blindheim, A.; Berge, V.; Tafjord, G.; Fosså, S.D.; Andreassen, B.K. Downstaging and survival after neoadjuvant chemotherapy for bladder cancer in Norway; a population-based study. BMC Cancer 2022, 22, 1301. [Google Scholar] [CrossRef]
- Lemiński, A.; Kaczmarek, K.; Byrski, T.; Słojewski, M. Neoadjuvant chemotherapy with dose-dense MVAC is associated with improved survival after radical cystectomy compared to other cytotoxic regimens: A tertiary centre experience. PLoS ONE 2021, 16, e0259526. [Google Scholar] [CrossRef] [PubMed]
- Vale, C.L. Neoadjuvant chemotherapy in invasive bladder cancer: An update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur. Urol. 2005, 48, 202–205, discussion 205. [Google Scholar] [CrossRef]
- Kaczmarek, K.; Lemiński, A.; Małkiewicz, B.; Gurwin, A.; Lisiński, J.; Słojewski, M. Diminishing the gender-related disparity in survival among chemotherapy pretreated patients after radical cystectomy: A multicentre observational study. J. Clin. Med. 2023, 12, 1260. [Google Scholar] [CrossRef]
- Horwich, A.; Babjuk, M.; Bellmunt, J.; Bruins, H.M.; De Reijke, T.M.; De Santis, M.; Gillessen, S.; James, N.; Maclennan, S.; Palou, J.; et al. EAU–ESMO consensus statements on the management of advanced and variant bladder cancer: An international collaborative multi-stakeholder effort under the auspices of the EAU and ESMO Guidelines Committees. Ann. Oncol. 2019, 30, 1697–1727. [Google Scholar] [CrossRef] [PubMed]
- van Hoogstraten, L.M.C.; van Gennep, E.J.; Kiemeney, L.A.L.M.; Witjes, J.A.; Voskuilen, C.S.; Deelen, M.; Mertens, L.S.; Meijer, R.P.; Boormans, J.L.; Robbrecht, D.G.J.; et al. Occult lymph node metastases in patients without residual muscle-invasive bladder cancer after radical cystectomy with or without neoadjuvant chemotherapy: A nationwide study of 5417 patients. World J. Urol. 2022, 40, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Zargar-Shoshtari, K.; Zargar, H.; Lotan, Y.; Shah, J.B.; Van Rhijn, B.W.; Daneshmand, S.; Spiess, P.E.; Black, P.C. Multi-institutional analysis of the outcomes of patients with clinically node-positive urothelial bladder cancer treated with induction chemotherapy and radical cystectomy. J. Urol. 2016, 195, 53–59. [Google Scholar] [CrossRef]
- Hermans, T.J.N.; Fransen van de Putte, E.E.; Horenblas, S.; Meijer, R.P.; Boormans, J.L.; Aben, K.K.H.; van der Heijden, M.S.; de Wit, R.; Beerepoot, L.V.; Verhoeven, R.H.; et al. Pathological downstaging and survival after induction chemotherapy and radical cystectomy for clinically node-positive bladder cancer have been reported in a nationwide population-based study. Eur. J. Cancer 2016, 69, 1–8. [Google Scholar] [CrossRef]
- Kaczmarek, K.; Małkiewicz, B.; Lemiński, A. Adequate pelvic lymph node dissection in radical cystectomy in the era of neoadjuvant chemotherapy: A meta-analysis and systematic review. Cancers 2023, 15, 4040. [Google Scholar] [CrossRef]
- McMahon, C.J.; Rofsky, N.M.; Pedrosa, I. Lymphatic metastases from pelvic tumours: Anatomic classification, characterisation, and staging. Radiology 2010, 254, 31–46. [Google Scholar] [CrossRef]
- Hwang, E.C.; Sathianathen, N.J.; Imamura, M.; Kuntz, G.M.; Risk, M.C.; Dahm, P. Extended versus standard lymph node dissection for urothelial carcinoma of the bladder in patients undergoing radical cystectomy. Cochrane Database Syst. Rev. 2019, 5, CD013336. [Google Scholar] [CrossRef] [PubMed]
- Galsky, M.D.; Hahn, N.M.; Rosenberg, J.; Sonpavde, G.; Hutson, T.; Oh, W.K.; Dreicer, R.; Vogelzang, N.; Sternberg, C.; Bajorin, D.F.; et al. Consensus definition of patients with metastatic urothelial carcinoma who are unfit for cisplatin-based chemotherapy. Lancet Oncol. 2011, 12, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Sherif, A.; Rintala, E.; Mestad, O.; Nilsson, J.; Holmberg, L.; Nilsson, S.; Malmström, P.U.; Nordic Urothelial Cancer Group. Neoadjuvant cisplatin-methotrexate chemotherapy for invasive bladder cancer—Nordic cystectomy trial 2. Scand. J. Urol. Nephrol. 2002, 36, 419–425. [Google Scholar] [CrossRef] [PubMed]
- von der Maase, H.; Hansen, S.W.; Roberts, J.T.; Dogliotti, L.; Oliver, T.; Moore, M.J.; Bodrogi, I.; Albers, P.; Knuth, A.; Lippert, C.M.; et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: Results of a large, randomized, multinational, multicenter, phase III study. J. Clin. Oncol. 2000, 18, 3068–3077. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; Yagoda, A.; Scher, H.I.; Watson, R.C.; Geller, N.; Herr, H.W.; Morse, M.J.; Sogani, P.C.; Vaughan, E.D.; Bander, N.; et al. Methotrexate, vinblastine, doxorubicin, and cisplatin for advanced transitional cell carcinoma of the urothelium. Efficacy and patterns of response and relapse. Cancer 1989, 15, 2448–2458. [Google Scholar] [CrossRef]
- Plimack, E.R.; Hoffman-Censits, J.H.; Viterbo, R.; Trabulsi, E.J.; Ross, E.A.; Greenberg, R.E.; Chen, D.Y.; Lallas, C.D.; Wong, Y.N.; Lin, J.; et al. Accelerated methotrexate, vinblastine, doxorubicin, and cisplatin is safe, effective, and efficient neoadjuvant treatment for muscle-invasive bladder cancer: Results of a multicenter phase II study with molecular correlates of response and toxicity. J. Clin. Oncol. 2014, 32, 1895–1901. [Google Scholar] [CrossRef]
- Lemiński, A.; Michalski, W.; Masojć, B.; Kaczmarek, K.; Małkiewicz, B.; Kienitz, J.; Zawisza-Lemińska, B.; Falco, M.; Słojewski, M. Combined modality of bladder-sparing therapy for muscle-invasive bladder cancer: How (should) we administer it? Narrative reviews. J. Clin. Med. 2023, 12, 1560. [Google Scholar] [CrossRef] [PubMed]
- Giacalone, N.J.; Shipley, W.U.; Clayman, R.H.; Niemierko, A.; Drumm, M.; Heney, N.M.; Michaelson, M.D.; Lee, R.J.; Saylor, P.J.; Wszolek, M.F.; et al. Long-term outcomes after bladder-preserving trimodality therapy for patients with muscle-invasive bladder cancer: An updated analysis of the Massachusetts General Hospital experience. Eur. Urol. 2017, 71, 952–960. [Google Scholar] [CrossRef]
- Kulkarni, G.S.; Hermanns, T.; Wei, Y.; Bhindi, B.; Satkunasivam, R.; Athanasopoulos, P.; Bostrom, P.J.; Kuk, C.; Li, K.; Templeton, A.J.; et al. Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in a multidisciplinary bladder cancer clinic. J. Clin. Oncol. 2017, 35, 2299–2305. [Google Scholar] [CrossRef]
- Ploussard, G.; Daneshmand, S.; Efstathiou, J.A.; Herr, H.W.; James, N.D.; Rödel, C.M.; Shariat, S.F.; Shipley, W.U.; Sternberg, C.N.; Thalmann, G.N.; et al. Critical analysis of bladder-sparing with trimodal therapy in muscle-invasive bladder cancer: A systematic review. Eur. Urol. 2014, 66, 120–137. [Google Scholar] [CrossRef]
- James, N.D.; Hussain, S.A.; Hall, E.; Jenkins, P.; Tremlett, J.; Rawlings, C.; Crundwell, M.; Sizer, B.; Sreenivasan, T.; Hendron, C.; et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N. Engl. J. Med. 2012, 366, 1477–1488. [Google Scholar] [CrossRef]
- Mitin, T.; Hunt, D.; Shipley, W.U.; Kaufman, D.S.; Uzzo, R.; Wu, C.L.; Buyyounouski, M.K.; Sandler, H.; Zietman, A.L. Transurethral surgery and twice-daily radiation plus paclitaxel-cisplatin or fluorouracil-cisplatin with selective bladder preservation and adjuvant chemotherapy for patients with muscle invasive bladder cancer (RTOG 0233): A randomised multicentre phase 2 trial. Lancet Oncol. 2013, 14, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, A.; Swindell, R.; Logue, J.P.; Elliott, P.A.; Livsey, J.E.; Wise, M.; Symonds, P.; Wylie, J.P.; Ramani, V.; Sangar, V.; et al. Phase II study of conformal hypofractionated radiotherapy with concurrent gemcitabine for muscle-invasive bladder cancer. J. Clin. Oncol. 2011, 29, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Premo, C.; Apolo, A.B.; Agarwal, P.K.; Citrin, D.E. Trimodality therapy in bladder cancer: Who, what, and when? Urol. Clin. N. Am. 2015, 42, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Tunio, M.A.; Hashmi, A.; Qayyum, A.; Mohsin, R.; Zaeem, A. Whole-pelvis or bladder-only chemoradiation for lymph node-negative invasive bladder cancer: Single-institution experience. Int. J. Radiat. Oncol. 2012, 82, e457–e462. [Google Scholar] [CrossRef] [PubMed]
- Lemiński, A.; Kaczmarek, K.; Michalski, W.; Małkiewicz, B.; Kotfis, K.; Słojewski, M. Influence of lymph node count on oncological outcomes of radical cystectomy in chemotherapy pre-treated and chemotherapy-naïve patients with muscle-invasive bladder cancer. J. Clin. Med. 2021, 10, 4923. [Google Scholar] [CrossRef]
- Mertens, L.S.; Meijer, R.P.; Meinhardt, W.; van der Poel, H.G.; Bex, A.; Kerst, J.M.; van der Heijden, M.S.; Bergman, A.M.; Horenblas, S.; van Rhijn, B.W. Occult lymph node metastases in patients with carcinoma invading bladder muscle: Incidence after neoadjuvant chemotherapy and cystectomy vs. after cystectomy alone. BJU Int. 2014, 114, 67–74. [Google Scholar] [CrossRef]
- Ploussard, G.; Pradere, B.; Beauval, J.B.; Chevreau, C.; Almeras, C.; Suc, E.; Gautier, J.R.; Laurenty, A.P.; Roumiguié, M.; Loison, G.; et al. Survival outcomes of patients with pathologically positive lymph nodes at the time of radical, with or without neoadjuvant chemotherapy. J. Clin. Med. 2020, 9, 1962. [Google Scholar] [CrossRef]
- Jeong, H.; Park, K.J.; Lee, Y.; Kim, H.D.; Kim, J.H.; Yoon, S.; Hong, B.; Lee, J.L. Prognosis and role of adjuvant chemotherapy in patients with node-positive bladder cancer treated with neoadjuvant chemotherapy followed by surgery. Cancer Res. Treat. 2022, 54, 226–233. [Google Scholar] [CrossRef]
- Seisen, T.; Jamzadeh, A.; Leow, J.J.; Rouprêt, M.; Cole, A.P.; Lipsitz, S.R.; Kibel, A.S.; Nguyen, P.L.; Sun, M.; Menon, M.; et al. Adjuvant chemotherapy vs. observation in patients with adverse pathological features of radical cystectomy previously treated with neoadjuvant chemotherapy. JAMA Oncol. 2018, 4, 225–229. [Google Scholar] [CrossRef]
- Zargar-Shoshtari, K.; Kongnyuy, M.; Sharma, P.; Fishman, M.N.; Gilbert, S.M.; Poch, M.A.; Pow-Sang, J.M.; Spiess, P.E.; Zhang, J.; Sexton, W.J. Clinical role of additional adjuvant chemotherapy in patients with locally advanced urothelial carcinoma after neoadjuvant chemotherapy and cystectomy. World J. Urol. 2016, 34, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, C.N.; Skoneczna, I.; Kerst, J.M.; Albers, P.; Fossa, S.D.; Agerbaek, M.; Dumez, H.; de Santis, M.; Théodore, C.; Leahy, M.G.; et al. Immediate versus deferred chemotherapy after radical cystectomy in patients with pT3-pT4 or N+ M0 urothelial carcinoma of the bladder (EORTC 30994): An intergroup, open-label, randomised phase 3 trial. Lancet Oncol. 2015, 16, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Donat, S.M.; Shabsigh, A.; Savage, C.; Cronin, A.M.; Bochner, B.H.; Dalbagni, G.; Herr, H.W.; Milowsky, M.I. Potential impact of postoperative early complications on the timing of adjuvant chemotherapy in patients undergoing radical cystectomy: A high-volume tertiary cancer centre experience. Eur. Urol. 2009, 55, 177–185. [Google Scholar] [CrossRef]
- Lewis, G.D.; Haque, W.; Verma, V.; Butler, E.B.; Teh, B.S. The role of adjuvant radiation therapy in locally advanced bladder cancer. Bl. Cancer 2018, 4, 205–213. [Google Scholar] [CrossRef]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.; Park, S.H.; et al. First results from the phase 3 CheckMate 274 trial of adjuvant nivolumab vs. placebo in patients who underwent radical surgery for high-risk muscle-invasive urothelial carcinoma (MIUC). J. Clin. Oncol. 2021, 39 (Suppl. S6), 391. [Google Scholar] [CrossRef]
- Barone, B.; Calogero, A.; Scafuri, L.; Ferro, M.; Lucarelli, G.; Di Zazzo, E.; Sicignano, E.; Falcone, A.; Romano, L.; De Luca, L.; et al. Immune checkpoint inhibitors as a neoadjuvant/adjuvant treatment of muscle-invasive bladder cancer: A systematic review. Cancers 2022, 14, 2545. [Google Scholar] [CrossRef] [PubMed]
- Iacovino, M.L.; Miceli, C.C.; De Felice, M.; Barone, B.; Pompella, L.; Chiancone, F.; Di Zazzo, E.; Tirino, G.; Della Corte, C.M.; Imbimbo, C.; et al. Novel therapeutic opportunities in neoadjuvant setting in urothelial cancers: A new horizon opened by molecular classification and immune checkpoint inhibitors. Int. J. Mol. Sci. 2022, 23, 1133. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | (y)pN0 | (y)pN+ | Total | p Value |
|---|---|---|---|---|
| Totals, No. | 913 | 481 | 1394 | |
| Age, years | 0.426 | |||
| Mean | 64.951 | 65.358 | ||
| SD | 9.235 | 8.741 | ||
| Gender, No. | 0.391 | |||
| Male | 737 | 379 | 1116 | |
| Female | 176 | 102 | 278 | |
| ASA score, No. | <0.001 | |||
| 1 | 61 | 8 | 69 | |
| 2 | 552 | 281 | 833 | |
| 3 | 271 | 182 | 453 | |
| 4 | 29 | 9 | 38 | |
| Clinical T stage, No. | <0.001 | |||
| cT2 | 256 | 39 | 295 | |
| cT3 | 501 | 244 | 745 | |
| cT4 | 156 | 198 | 354 | |
| Pathological T stage, No. | <0.001 | |||
| pT0 | 119 | 12 | 131 | |
| pTis/Ta/T1 | 200 | 35 | 235 | |
| pT2 | 227 | 41 | 268 | |
| pT3 | 204 | 193 | 397 | |
| pT4 | 163 | 200 | 363 | |
| Cancer grade, No. | <0.001 | |||
| Low | 95 | 14 | 166 | |
| High | 818 | 467 | 1228 | |
| Chemotherapy regimen, No. | 0.092 | |||
| None | 698 | 379 | 1077 | |
| MVAC | 51 | 29 | 80 | |
| ddMVAC | 68 | 21 | 89 | |
| Gemcitabine-cisplatin | 76 | 48 | 124 | |
| Gemcitabine-carboplatin | 8 | 2 | 10 | |
| Gemcitabine-paclitaxel | 12 | 2 | 14 | |
| Cycles of chemotherapy, No. | ||||
| <3 | 59 | 44 | 103 | 0.005 |
| ≥3 | 156 | 58 | 214 |
| All Patients | ||||||||
|---|---|---|---|---|---|---|---|---|
| HR | Lower 95%CI | Upper 95%CI | p | HR | Lower 95%CI | Upper 95%CI | p | |
| (y)pN0 | (y)pN+ | |||||||
| Age, years | 1.016 | 1.005 | 1.028 | 0.005 | 1.017 | 1.005 | 1.029 | 0.007 |
| Gender | ||||||||
| Male | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| Female | 1.070 | 0.832 | 1.376 | 0.599 | 1.017 | 0.792 | 1.307 | 0.894 |
| ASA score | ||||||||
| 1–2 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| 3–4 | 1.244 | 1.010 | 1.532 | 0.040 | 1.404 | 1.143 | 1.725 | 0.001 |
| Pathological T stage | ||||||||
| ≤pT2 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| >pT2 | 2.224 | 1.790 | 2.762 | <0.001 | 2.037 | 1.479 | 2.806 | <0.001 |
| Cancer grade | ||||||||
| Low | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| High | 1.274 | 0.837 | 1.941 | 0.259 | 0.885 | 0.414 | 1.892 | 0.752 |
| NAC | ||||||||
| No | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| Yes | 0.692 | 0.524 | 0.915 | 0.010 | 0.927 | 0.713 | 1.205 | 0.572 |
| <(y)pT2 | ||||||||
| (y)pN0 | (y)pN+ | |||||||
| Age, years | 1.036 | 1.010 | 1.063 | 0.007 | 1.063 | 0.970 | 1.164 | 0.191 |
| Gender | ||||||||
| Male | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| Female | 1.380 | 0.796 | 2.391 | 0.251 | 2.599 | 0.660 | 10.240 | 0.172 |
| ASA score | ||||||||
| 1–2 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| 3–4 | 2.139 | 1.362 | 3.359 | 0.001 | 5.670 | 1.781 | 18.054 | 0.003 |
| Cancer grade | ||||||||
| Low | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| High | 1.037 | 0.635 | 1.693 | 0.885 | 1.672 | 0.396 | 7.063 | 0.484 |
| NAC | ||||||||
| No | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| Yes | 0.572 | 0.343 | 0.951 | 0.031 | 3.111 | 1.249 | 7.746 | 0.015 |
| ≥(y)pT2 | ||||||||
| (y)pN0 | (y)pN+ | |||||||
| Age, years | 1.015 | 1.003 | 1.028 | 0.017 | 1.016 | 1.003 | 1.029 | 0.015 |
| Gender | ||||||||
| Male | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| Female | 0.994 | 0.747 | 1.323 | 0.967 | 0.983 | 0.758 | 1.274 | 0.895 |
| ASA score | ||||||||
| 1–2 | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| 3–4 | 1.229 | 0.970 | 1.556 | 0.087 | 1.329 | 1.074 | 1.644 | 0.009 |
| Cancer grade | ||||||||
| Low | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| High | 3.484 | 0.861 | 14.108 | 0.080 | 0.825 | 0.307 | 2.220 | 0.703 |
| NAC | ||||||||
| No | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. | ||
| Yes | 0.692 | 0.493 | 0.971 | 0.033 | 0.758 | 0.562 | 1.022 | 0.069 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaczmarek, K.; Małkiewicz, B.; Skonieczna-Żydecka, K.; Lemiński, A. Influence of Neoadjuvant Chemotherapy on Survival Outcomes of Radical Cystectomy in Pathologically Proven Positive and Negative Lymph Nodes. Cancers 2023, 15, 4901. https://doi.org/10.3390/cancers15194901
Kaczmarek K, Małkiewicz B, Skonieczna-Żydecka K, Lemiński A. Influence of Neoadjuvant Chemotherapy on Survival Outcomes of Radical Cystectomy in Pathologically Proven Positive and Negative Lymph Nodes. Cancers. 2023; 15(19):4901. https://doi.org/10.3390/cancers15194901
Chicago/Turabian StyleKaczmarek, Krystian, Bartosz Małkiewicz, Karolina Skonieczna-Żydecka, and Artur Lemiński. 2023. "Influence of Neoadjuvant Chemotherapy on Survival Outcomes of Radical Cystectomy in Pathologically Proven Positive and Negative Lymph Nodes" Cancers 15, no. 19: 4901. https://doi.org/10.3390/cancers15194901
APA StyleKaczmarek, K., Małkiewicz, B., Skonieczna-Żydecka, K., & Lemiński, A. (2023). Influence of Neoadjuvant Chemotherapy on Survival Outcomes of Radical Cystectomy in Pathologically Proven Positive and Negative Lymph Nodes. Cancers, 15(19), 4901. https://doi.org/10.3390/cancers15194901