
Intraoperative Imaging and Optical Visualization Techniques for Brain Tumor Resection: A Narrative Review
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Optical Visualization Techniques for Brain Tumor Resection
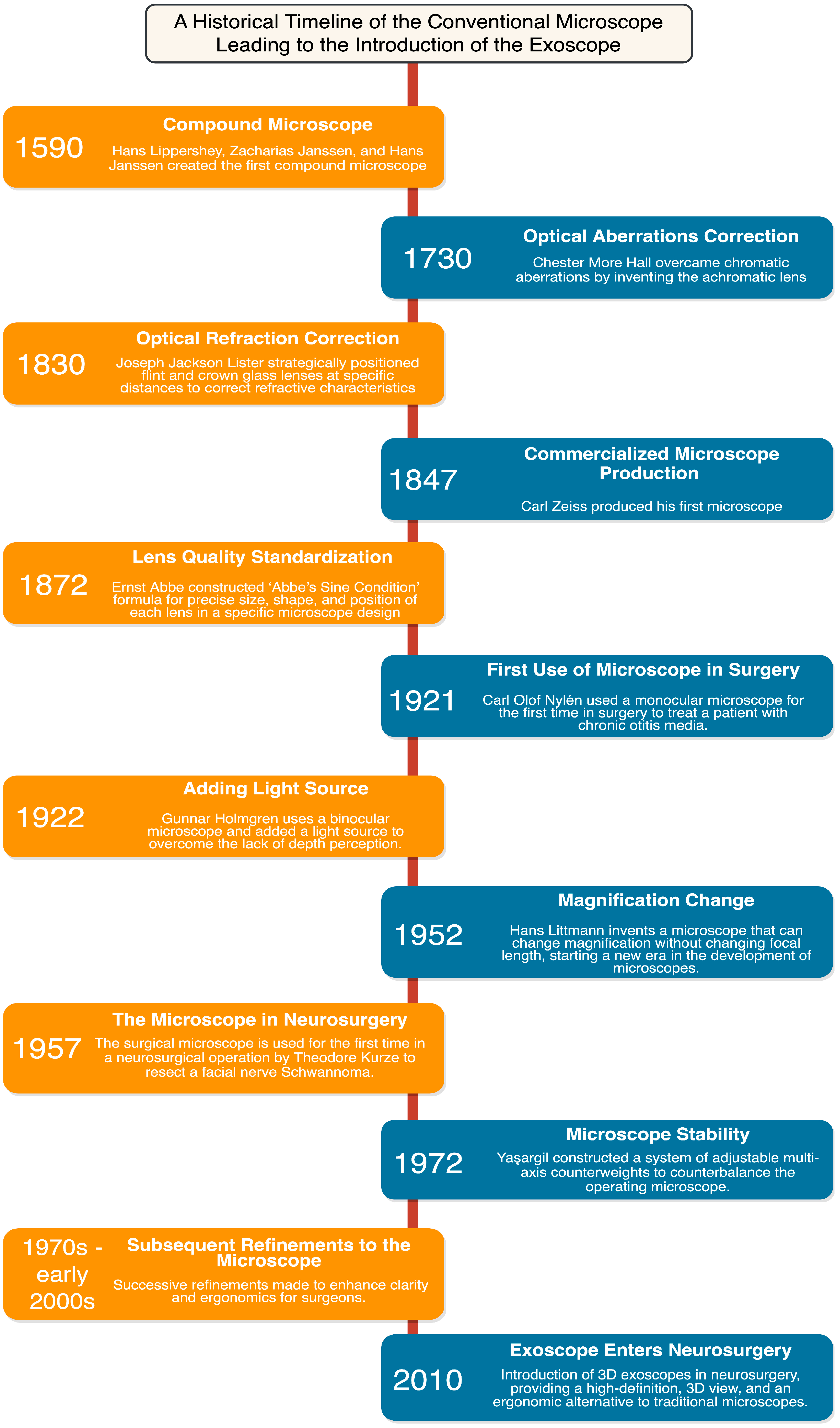
2.1. A Historical Lens on the Evolution of Optical Neurosurgical Oncology
2.2. Conventional Operating Microscope
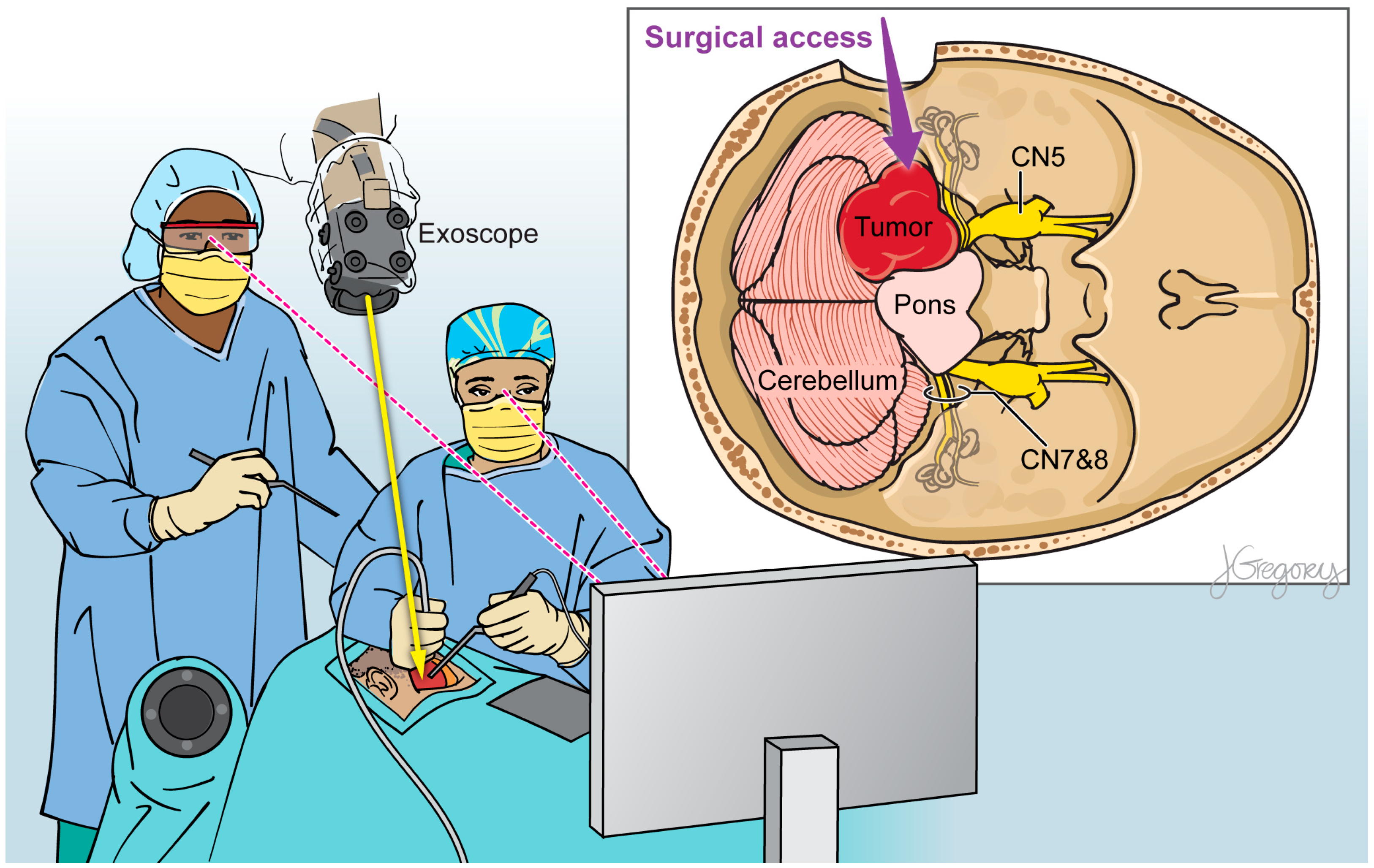
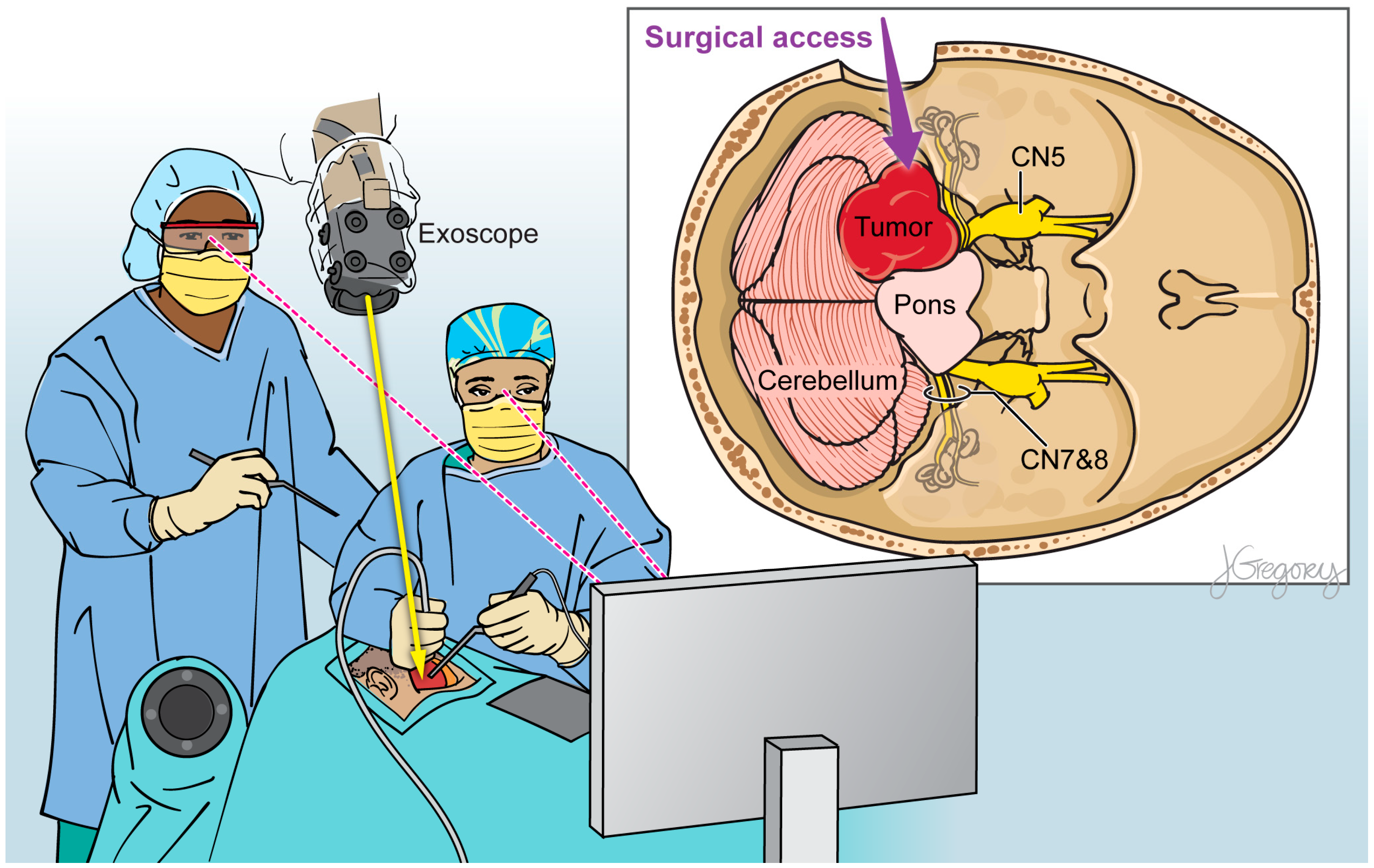
2.3. Exoscope
2.4. Fluorescence-Guided Neurosurgery
3. Intraoperative Handheld Visualization and Diagnostic Techniques
3.1. Raman Spectroscopy
3.2. Confocal Microscopy
4. Conventional Imaging Techniques for Intraoperative Tumor Resection
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Verburg, N.; de Witt Hamer, P.C. State-of-the-Art Imaging for Glioma Surgery. Neurosurg. Rev. 2021, 44, 1331–1343. [Google Scholar] [CrossRef] [PubMed]
- Noh, T.; Mustroph, M.; Golby, A.J. Intraoperative Imaging for High-Grade Glioma Surgery. Neurosurg. Clin. N. Am. 2021, 32, 47. [Google Scholar] [CrossRef] [PubMed]
- Dixon, L.; Lim, A.; Grech-Sollars, M.; Nandi, D.; Camp, S. Intraoperative Ultrasound in Brain Tumor Surgery: A Review and Implementation Guide. Neurosurg. Rev. 2022, 45, 2503–2515. [Google Scholar] [CrossRef] [PubMed]
- Schupper, A.J.; Roa, J.A.; Hadjipanayis, C.G. Contemporary Intraoperative Visualization for GBM with Use of Exoscope, 5-ALA Fluorescence-Guided Surgery and Tractography. Neurosurg. Focus Video 2022, 6, V5. [Google Scholar] [CrossRef]
- Jenkinson, M.D.; Barone, D.G.; Bryant, A.; Vale, L.; Bulbeck, H.; Lawrie, T.A.; Hart, M.G.; Watts, C. Intraoperative Imaging Technology to Maximise Extent of Resection for Glioma. Cochrane Database Syst. Rev. 2018, 1. [Google Scholar] [CrossRef]
- Hervey-Jumper, S.L.; Berger, M.S. Maximizing Safe Resection of Low- and High-Grade Glioma. J. Neurooncol. 2016, 130, 269–282. [Google Scholar] [CrossRef]
- Muto, J.; Mine, Y.; Nakagawa, Y.; Joko, M.; Kagami, H.; Inaba, M.; Hasegawa, M.; Lee, J.Y.K.; Hirose, Y. Intraoperative Real-Time near-Infrared Optical Imaging for the Identification of Metastatic Brain Tumors via Microscope and Exoscope. Neurosurg. Focus 2021, 50, E11. [Google Scholar] [CrossRef]
- Stummer, W.; Pichlmeier, U.; Meinel, T.; Wiestler, O.D.; Zanella, F.; Reulen, H.J. Fluorescence-Guided Surgery with 5-Aminolevulinic Acid for Resection of Malignant Glioma: A Randomised Controlled Multicentre Phase III Trial. Lancet Oncol. 2006, 7, 392–401. [Google Scholar] [CrossRef]
- Winther, R.R.; Hjermstad, M.J.; Skovlund, E.; Aass, N.; Helseth, E.; Kaasa, S.; Yri, O.E.; Vik-Mo, E.O. Surgery for Brain Metastases-Impact of the Extent of Resection. Acta Neurochir. 2022, 164, 2773–2780. [Google Scholar] [CrossRef]
- Delgado-López, P.D.; Corrales-García, E.M. Survival in Glioblastoma: A Review on the Impact of Treatment Modalities. Clin. Transl. Oncol. 2016, 18, 1062–1071. [Google Scholar] [CrossRef]
- Choque-Velasquez, J.; Resendiz-Nieves, J.; Jahromi, B.R.; Colasanti, R.; Raj, R.; Vehviläinen, J.; Tynninen, O.; Collan, J.; Niemelä, M.; Hernesniemi, J. Extent of Resection and Long-Term Survival of Pineal Region Tumors in Helsinki Neurosurgery. World Neurosurg. 2019, 131, e379–e391. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, A.; Zhang, H.; Cui, M.; Lin, X.; Huang, S.; Tang, Z.; Hou, Y.; Zubair Iqbal, M.; Kong, X. ROS-Responsive Chlorin E6 and Silk Fibroin Loaded Ultrathin Magnetic Hydroxyapatite Nanorods for T1-Magnetic Resonance Imaging Guided Photodynamic Therapy in Vitro. Colloids Surf. A Physicochem. Eng. Asp. 2023, 656, 130513. [Google Scholar] [CrossRef]
- Mushtaq, A.; Ma, X.; Farheen, J.; Lin, X.; Tayyab, M.; Iqbal, M.Z.; Kong, X. Facile Synthesis of Metformin Loaded Mn3O4-HAp Magnetic Hydroxyapatite Nanocomposites for T1-Magnetic Resonance Imaging Guided Targeted Chemo-Phototherapy in Vitro. Colloids Surf. A Physicochem. Eng. Asp. 2023, 674, 131911. [Google Scholar] [CrossRef]
- Restelli, F.; Mathis, A.M.; Höhne, J.; Mazzapicchi, E.; Acerbi, F.; Pollo, B.; Quint, K. Confocal Laser Imaging in Neurosurgery: A Comprehensive Review of Sodium Fluorescein-Based CONVIVO Preclinical and Clinical Applications. Front. Oncol. 2022, 12, 998384. [Google Scholar] [CrossRef]
- Livermore, L.J.; Isabelle, M.; Mac Bell, I.; Scott, C.; Walsby-Tickle, J.; Gannon, J.; Plaha, P.; Vallance, C.; Ansorge, O. Rapid Intraoperative Molecular Genetic Classification of Gliomas Using Raman Spectroscopy. Neurooncol. Adv. 2019, 1, vdz008. [Google Scholar] [CrossRef]
- Kabuto, M.; Kubota, T.; Kobayashi, H.; Nakagawa, T.; Ishii, H.; Takeuchi, H.; Kitai, R.; Kodera, T. Experimental and Clinical Study of Detection of Glioma at Surgery Using Fluorescent Imaging by a Surgical Microscope after Fluorescein Administration. Neurol. Res. 1997, 19, 9–16. [Google Scholar] [CrossRef]
- Montemurro, N.; Scerrati, A.; Ricciardi, L.; Trevisi, G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. J. Clin. Med. 2021, 11, 223. [Google Scholar] [CrossRef]
- Uluç, K.; Kujoth, G.C.; Başkaya, M.K. Operating Microscopes: Past, Present, and Future. Neurosurg. Focus 2009, 27, E4. [Google Scholar] [CrossRef]
- Kriss, T.C.; Kriss, V.M. History of the Operating Microscope: From Magnifying Glass to Microneurosurgery. Neurosurgery 1998, 42, 899–908. [Google Scholar] [CrossRef]
- Splinter, R.; Hooper, B.A. An Introduction to Biomedical Optics; CRC Press: Boca Raton, FL, USA, 2006; pp. 1–602. [Google Scholar] [CrossRef]
- Nylean, C.O. The Microscope in Aural Surgery, Its First Use and Later Development. Acta Otolaryngol. 1954, 43, 226–240. [Google Scholar] [CrossRef]
- Schultheiss, D.; Denil, J. History of the Microscope and Development of Microsurgery: A Revolution for Reproductive Tract Surgery. Andrologia 2002, 34, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Barraquer, J.I. The History of the Microscope in Ocular Surgery. J. Microsurg. 1980, 1, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Link, T.E.; Bisson, E.; Horgan, M.A.; Tranmer, B.I.; Raymond, M.P. Donaghy: A Pioneer in Microneurosurgery. J. Neurosurg. 2010, 112, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Liczbik, O.; Goertz, S.; Wiśniewski, J.; Kurlandt, P.; Libionka, W.; Adamski, S.; Kloc, W. From Magnifying Glass to Operative Microscopy—The Historical and Modern Role of the Microscope in Microsurgery. Pol. J. Pathol. 2019, 70, 14–20. [Google Scholar] [CrossRef]
- Belykh, E.; Miller, E.J.; Patel, A.A.; Bozkurt, B.; Yagmurlu, K.; Robinson, T.R.; Nakaji, P.; Spetzler, R.F.; Lawton, M.T.; Nelson, L.Y.; et al. Optical Characterization of Neurosurgical Operating Microscopes: Quantitative Fluorescence and Assessment of PpIX Photobleaching. Sci. Rep. 2018, 8, 12543. [Google Scholar] [CrossRef]
- Lemee, J.M.; Corniola, M.V.; Da Broi, M.; Joswig, H.; Scheie, D.; Schaller, K.; Helseth, E.; Meling, T.R. Extent of Resection in Meningioma: Predictive Factors and Clinical Implications. Sci. Rep. 2019, 9, 5944. [Google Scholar] [CrossRef]
- Sanai, N.; Polley, M.Y.; McDermott, M.W.; Parsa, A.T.; Berger, M.S. An Extent of Resection Threshold for Newly Diagnosed Glioblastomas: Clinical Article. J. Neurosurg. 2011, 115, 3–8. [Google Scholar] [CrossRef]
- Soni, P.; Davison, M.A.; Shao, J.N.; Momin, A.; Lopez, D.; Angelov, L.; Barnett, G.H.; Lee, J.H.; Mohammadi, A.M.; Kshettry, V.R.; et al. Extent of Resection and Survival Outcomes in World Health Organization Grade II Meningiomas. J. Neurooncol. 2021, 151, 173–179. [Google Scholar] [CrossRef]
- D’Amico, R.S.; Englander, Z.K.; Canoll, P.; Bruce, J.N. Extent of Resection in Glioma–A Review of the Cutting Edge. World Neurosurg. 2017, 103, 538–549. [Google Scholar] [CrossRef]
- Tamai, S. Experimental and Clinical Reconstructive Microsurgery; Springer: Berlin/Heidelberg, Germany, 2003. [Google Scholar] [CrossRef]
- Haddad, A.F.; Aghi, M.K.; Butowski, N. Novel Intraoperative Strategies for Enhancing Tumor Control: Future Directions. Neuro Oncol. 2022, 24, S25–S32. [Google Scholar] [CrossRef]
- Langer, D.J.; White, T.G.; Schulder, M.; Boockvar, J.A.; Labib, M.; Lawton, M.T. Advances in Intraoperative Optics: A Brief Review of Current Exoscope Platforms. Oper. Neurosurg. 2020, 19, 84–93. [Google Scholar] [CrossRef]
- Piloni, M.; Bailo, M.; Gagliardi, F.; Mortini, P. Resection of Intracranial Tumors with a Robotic-Assisted Digital Microscope: A Preliminary Experience with Robotic Scope. World Neurosurg. 2021, 152, e205–e211. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.W.; Nakajima, T.; Brodwater, B.; Pavlidis, J.; Friets, E.; Fagan, E.; Hartov, A.; Strohbehn, J. Further Development and Clinical Application of the Stereotactic Operating Microscope. Stereotact. Funct. Neurosurg. 1992, 58, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Muscas, G.; Battista, F.; Boschi, A.; Morone, F.; Della Puppa, A. A Single-Center Experience with the Olympus ORBEYE 4K-3D Exoscope for Microsurgery of Complex Cranial Cases: Technical Nuances and Learning Curve. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2021, 82, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Schupper, A.J.; Price, G.; Hadjipanayis, C.G. Robotic-Assisted Digital Exoscope for Resection of Cerebral Metastases: A Case Series. Oper. Neurosurg. 2021, 21, 436–444. [Google Scholar] [CrossRef]
- Pafitanis, G.; Hadjiandreou, M.; Alamri, A.; Uff, C.; Walsh, D.; Myers, S. The Exoscope versus Operating Microscope in Microvascular Surgery: A Simulation Non-Inferiority Trial. Arch. Plast. Surg. 2020, 47, 242. [Google Scholar] [CrossRef]
- Abunimer, A.M.; Abou-Al-Shaar, H.; White, T.G.; Park, J.; Schulder, M. The Utility of High-Definition 2-Dimensional Stereotactic Exoscope in Cranial and Spinal Procedures. World Neurosurg. 2022, 158, e231–e236. [Google Scholar] [CrossRef]
- Della Pepa, G.M.; Mattogno, P.; Menna, G.; Agostini, L.; Olivi, A.; Doglietto, F. A Comparative Analysis with Exoscope and Optical Microscope for Intraoperative Visualization and Surgical Workflow in 5-Aminolevulinic Acid-Guided Resection of High-Grade Gliomas. World Neurosurg. 2023, 170, 133–137. [Google Scholar] [CrossRef]
- Reddy, R.; Chu, K.; Deebel, N.A.; Ory, J.; Weber, A.; Terlecki, R.; Ramasamy, R. A Comparative Analysis of Ergonomic Risk Utilizing the 4K-3D Exoscope Versus Standard Operating Microscope for Male Fertility Microsurgery. Urology 2023, 172, 115–120. [Google Scholar] [CrossRef]
- Veldeman, M.; Rossmann, T.; Huhtakangas, J.; Nurminen, V.; Eisenring, C.; Sinkkonen, S.T.; Niemela, M.; Lehecka, M. Three-Dimensional Exoscopic Versus Microscopic Resection of Vestibular Schwannomas: A Comparative Series. Oper. Neurosurg. 2023, 24, 507–513. [Google Scholar] [CrossRef]
- Schupper, A.J.; Hrabarchuk, E.I.; McCarthy, L.; Hadjipanayis, C.G. Improving Surgeon Well-Being: Ergonomics in Neurosurgery. World Neurosurg. 2023, 175, e1220–e1225. [Google Scholar] [CrossRef] [PubMed]
- Schupper, A.J.; Eskandari, R.; Kosnik-Infinger, L.; Olivera, R.; Nangunoori, R.; Patel, S.; Williamson, R.; Yu, A.; Hadjipanayis, C.G. A Multicenter Study Investigating the Surgeon Experience with a Robotic-Assisted Exoscope as Part of the Neurosurgical Armamentarium. World Neurosurg. 2023, 173, e571–e577. [Google Scholar] [CrossRef] [PubMed]
- Vogelbaum, M.A.; Kroll, D.; Etame, A.; Tran, N.; Liu, J.; Ford, A.; Sparr, E.; Kim, Y.; Forsyth, P.; Sahebjam, S.; et al. A Prospective Validation Study of the First 3D Digital Exoscope for Visualization of 5-ALA–Induced Fluorescence in High-Grade Gliomas. World Neurosurg. 2021, 149, e498–e503. [Google Scholar] [CrossRef] [PubMed]
- Bakhsheshian, J.; Strickland, B.A.; Jackson, C.; Chaichana, K.L.; Young, R.; Pradilla, G.; Chen, J.W.; Bailes, J.; Zada, G. Multicenter Investigation of Channel-Based Subcortical Trans-Sulcal Exoscopic Resection of Metastatic Brain Tumors: A Retrospective Case Series. Oper. Neurosurg. 2019, 16, 159–166. [Google Scholar] [CrossRef]
- Baron, R.B.; Lakomkin, N.; Schupper, A.J.; Nistal, D.; Nael, K.; Price, G.; Hadjipanayis, C.G. Postoperative Outcomes Following Glioblastoma Resection Using a Robot-Assisted Digital Surgical Exoscope: A Case Series. J. Neurooncol. 2020, 148, 519–527. [Google Scholar] [CrossRef]
- Muhammad, S.; Lehecka, M.; Niemelä, M. Preliminary Experience with a Digital Robotic Exoscope in Cranial and Spinal Surgery: A Review of the Synaptive Modus V System. Acta Neurochir. 2019, 161, 2175. [Google Scholar] [CrossRef]
- Price, G.; Schupper, A.; Kalagara, R.; Chennareddy, S.; He, C.; Zhang, J.Y.; Sudhir, S.; Rentzeperis, F.; Wanna, G.; Hadjipanayis, C. Application of the Robotic-Assisted Digital Exoscope for Resection of Posterior Fossa Tumors in Adults: A Series of 45 Cases. Oper. Neurosurg. 2023, 11, 10–227. [Google Scholar] [CrossRef]
- Ariffin, M.H.M.; Ibrahim, K.; Baharudin, A.; Tamil, A.M. Early Experience, Setup, Learning Curve, Benefits, and Complications Associated with Exoscope and Three-Dimensional 4K Hybrid Digital Visualizations in Minimally Invasive Spine Surgery. Asian Spine J. 2020, 14, 59–65. [Google Scholar] [CrossRef]
- De Jesus Encarnacion Ramirez, M.; Peralta, I.; Ramirez, I.; Dauly, V.; Mainer, G.; Nurmukhametov, R.; Efe, I.E. Development of a Novel Low-Cost Exoscope to Expand Access to Microneurosurgical Care in Low- and Middle-Income Countries. World Neurosurg. 2022, 163, 5–10. [Google Scholar] [CrossRef]
- Matsui, C.; Banda, C.H.; Okada, Y.; Shiraishi, M.; Shimizu, K.; Mitsui, K.; Danno, K.; Ishiura, R.; Narushima, M. Shaping the Future of Microsurgery: Combination of Exoscope and Smart Glasses. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 893–939. [Google Scholar] [CrossRef]
- Hadjipanayis, C.G.; Widhalm, G.; Stummer, W. What Is the Surgical Benefit of Utilizing 5-Aminolevulinic Acid for Fluorescence-Guided Surgery of Malignant Gliomas? Neurosurgery 2015, 77, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Roberts, D.W.; Sanai, N.; Liu, J.T.C. Visualization Technologies for 5-ALA-Based Fluorescence-Guided Surgeries. J. Neurooncol. 2019, 141, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Schebesch, K.M.; Brawanski, A.; Hohenberger, C.; Höhne, J. Fluorescein Sodium-Guided Surgery of Malignant Brain Tumors: History, Current Concepts, and Future Project. Turk. Neurosurg. 2016, 26, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Schupper, A.J.; Rao, M.; Mohammadi, N.; Baron, R.; Lee, J.Y.K.; Acerbi, F.; Hadjipanayis, C.G. Fluorescence-Guided Surgery: A Review on Timing and Use in Brain Tumor Surgery. Front. Neurol. 2021, 12, 682151. [Google Scholar] [CrossRef]
- Acerbi, F.; Broggi, M.; Eoli, M.; Anghileri, E.; Cavallo, C.; Boffano, C.; Cordella, R.; Cuppini, L.; Pollo, B.; Schiariti, M.; et al. Is Fluorescein-Guided Technique Able to Help in Resection of High-Grade Gliomas? Neurosurg. Focus 2014, 36, E5. [Google Scholar] [CrossRef]
- Acerbi, F.; Broggi, M.; Schebesch, K.M.; Höhne, J.; Cavallo, C.; De Laurentis, C.; Eoli, M.; Anghileri, E.; Servida, M.; Boffano, C.; et al. Fluorescein-Guided Surgery for Resection of High-Grade Gliomas: A Multicentric Prospective Phase II Study (FLUOGLIO). Clin. Cancer Res. 2018, 24, 52–61. [Google Scholar] [CrossRef]
- Ung, T.H.; Kellner, C.; Neira, J.A.; Wang, S.H.J.; D’Amico, R.; Faust, P.L.; Canoll, P.; Feldstein, N.A.; Bruce, J.N. The Use of Fluorescein Sodium in the Biopsy and Gross-Total Resection of a Tectal Plate Glioma. J. Neurosurg. Pediatr. 2015, 16, 732–735. [Google Scholar] [CrossRef]
- Molina, E.S.; Wölfer, J.; Ewelt, C.; Ehrhardt, A.; Brokinkel, B.; Stummer, W. Dual-Labeling with 5-Aminolevulinic Acid and Fluorescein for Fluorescence-Guided Resection of High-Grade Gliomas: Technical Note. J. Neurosurg. 2018, 128, 399–405. [Google Scholar] [CrossRef]
- Acerbi, F.; Vetrano, I.G.; Sattin, T.; de Laurentis, C.; Bosio, L.; Rossini, Z.; Broggi, M.; Schiariti, M.; Ferroli, P. The Role of Indocyanine Green Videoangiography with FLOW 800 Analysis for the Surgical Management of Central Nervous System Tumors: An Update. Neurosurg. Focus 2018, 44, E6. [Google Scholar] [CrossRef]
- Marchese, E.; della Pepa, G.M.; la Rocca, G.; Albanese, A.; Ius, T.; Simboli, G.A.; Sabatino, G. Application of Indocyanine Green Video Angiography in Vascular Neurosurgery. J. Neurosurg. Sci. 2019, 63, 656–660. [Google Scholar] [CrossRef]
- Cho, S.S.; Teng, C.W.; De Ravin, E.; Singh, Y.B.; Lee, J.Y.K. Assessment and Comparison of Three Dimensional Exoscopes for Near-Infrared Fluorescence-Guided Surgery Using Second-Window Indocyanine-Green. J. Korean Neurosurg. Soc. 2022, 65, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.S.; Salinas, R.; De Ravin, E.; Teng, C.W.; Li, C.; Abdullah, K.G.; Buch, L.; Hussain, J.; Ahmed, F.; Dorsey, J.; et al. Near-Infrared Imaging with Second-Window Indocyanine Green in Newly Diagnosed High-Grade Gliomas Predicts Gadolinium Enhancement on Postoperative Magnetic Resonance Imaging. Mol. Imaging Biol. 2020, 22, 1427–1437. [Google Scholar] [CrossRef] [PubMed]
- Polikarpov, D.M.; Campbell, D.H.; McRobb, L.S.; Wu, J.; Lund, M.E.; Lu, Y.; Deyev, S.M.; Davidson, A.S.; Walsh, B.J.; Zvyagin, A.V.; et al. Near-Infrared Molecular Imaging of Glioblastoma by Miltuximab®-IRDye800CW as a Potential Tool for Fluorescence-Guided Surgery. Cancers 2020, 12, 984. [Google Scholar] [CrossRef] [PubMed]
- Patil, C.G.; Walker, D.G.; Miller, D.M.; Butte, P.; Morrison, B.; Kittle, D.S.; Hansen, S.J.; Nufer, K.L.; Byrnes-Blake, K.A.; Yamada, M.; et al. Phase 1 Safety, Pharmacokinetics, and Fluorescence Imaging Study of Tozuleristide (BLZ-100) in Adults With Newly Diagnosed or Recurrent Gliomas. Neurosurgery 2019, 85, E641–E649. [Google Scholar] [CrossRef]
- Zhou, Q.; Vega Leonel, J.C.M.; Santoso, M.R.; Wilson, C.; van den Berg, N.S.; Chan, C.T.; Aryal, M.; Vogel, H.; Cayrol, R.; Mandella, M.J.; et al. Molecular Imaging of a Fluorescent Antibody against Epidermal Growth Factor Receptor Detects High-Grade Glioma. Sci. Rep. 2021, 11, 5710. [Google Scholar] [CrossRef]
- Weichert, J.P.; Clark, P.A.; Kandela, I.K.; Vaccaro, A.M.; Clarke, W.; Longino, M.A.; Pinchuk, A.N.; Farhoud, M.; Swanson, K.I.; Floberg, J.M.; et al. Alkylphosphocholine Analogs for Broad-Spectrum Cancer Imaging and Therapy. Sci. Transl. Med. 2014, 6, 240ra75. [Google Scholar] [CrossRef]
- Bonosi, L.; Marrone, S.; Benigno, U.E.; Buscemi, F.; Musso, S.; Porzio, M.; Silven, M.P.; Torregrossa, F.; Grasso, G. Maximal Safe Resection in Glioblastoma Surgery: A Systematic Review of Advanced Intraoperative Image-Guided Techniques. Brain Sci. 2023, 13, 216. [Google Scholar] [CrossRef]
- Spille, D.C.; Bunk, E.C.; Thomas, C.; Özdemir, Z.; Wagner, A.; Akkurt, B.H.; Mannil, M.; Paulus, W.; Grauer, O.M.; Stummer, W.; et al. Protoporphyrin IX (PpIX) Fluorescence during Meningioma Surgery: Correlations with Histological Findings and Expression of Heme Pathway Molecules. Cancers 2023, 15, 304. [Google Scholar] [CrossRef]
- Hadjipanayis, C.G.; Stummer, W. 5-ALA and FDA Approval for Glioma Surgery. J. Neurooncol. 2019, 141, 479–486. [Google Scholar] [CrossRef]
- Stepp, H.; Stummer, W. 5-ALA in the Management of Malignant Glioma. Lasers Surg. Med. 2018, 50, 399–419. [Google Scholar] [CrossRef]
- Su, X.; Huang, Q.F.; Chen, H.L.; Chen, J. Fluorescence-Guided Resection of High-Grade Gliomas: A Systematic Review and Meta-Analysis. Photodiagnosis Photodyn. Ther. 2014, 11, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Eatz, T.A.; Eichberg, D.G.; Lu, V.M.; Di, L.; Komotar, R.J.; Ivan, M.E. Intraoperative 5-ALA Fluorescence-Guided Resection of High-Grade Glioma Leads to Greater Extent of Resection with Better Outcomes: A Systematic Review. J. Neurooncol. 2022, 156, 233–256. [Google Scholar] [CrossRef]
- Molina, E.S.; Hellwig, S.J.; Walke, A.; Jeibmann, A.; Stepp, H.; Stummer, W. Development and Validation of a Triple-LED Surgical Loupe Device for Fluorescence-Guided Resections with 5-ALA. J. Neurosurg. 2021, 137, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Giantini-Larsen, A.M.; Parker, W.E.; Cho, S.S.; Goldberg, J.L.; Carnevale, J.A.; Michael, A.P.; Teng, C.W.; De Ravin, E.; Brennan, C.W.; Lee, J.Y.K.; et al. The Evolution of 5-Aminolevulinic Acid Fluorescence Visualization: Time for a Headlamp/Loupe Combination. World Neurosurg. 2022, 159, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Bettag, C.; Hussein, A.; Schatlo, B.; Barrantes-Freer, A.; Abboud, T.; Rohde, V.; Mielke, D. Endoscope-Assisted Visualization of 5-Aminolevulinic Acid Fluorescence in Surgery for Brain Metastases. J. Neurosurg. 2022, 137, 1650–1655. [Google Scholar] [CrossRef]
- Lau, D.; Hervey-Jumper, S.L.; Chang, S.; Molinaro, A.M.; McDermott, M.W.; Phillips, J.J.; Berger, M.S. A Prospective Phase II Clinical Trial of 5-Aminolevulinic Acid to Assess the Correlation of Intraoperative Fluorescence Intensity and Degree of Histologic Cellularity during Resection of High-Grade Gliomas. J. Neurosurg. 2016, 124, 1300–1309. [Google Scholar] [CrossRef]
- Kundu, S.; Das, S.; Patra, A. Fluorescence Correlation Spectroscopy and Fluorescence Lifetime Imaging Microscopy for Deciphering the Morphological Evolution of Supramolecular Self-Assembly. Chem. Commun. 2023, 59, 8017–8031. [Google Scholar] [CrossRef]
- Sun, Y.; Hatami, N.; Yee, M.; Phipps, J.; Elson, D.S.; Gorin, F.; Schrot, R.J.; Marcu, L. Fluorescence Lifetime Imaging Microscopy for Brain Tumor Image-Guided Surgery. J. Biomed. Opt. 2010, 15, 056022. [Google Scholar] [CrossRef]
- Tamura, Y.; Kuroiwa, T.; Kajimoto, Y.; Miki, Y.; Miyatake, S.I.; Tsuji, M. Endoscopic Identification and Biopsy Sampling of an Intraventricular Malignant Glioma Using a 5-Aminolevulinic Acid–Induced Protoporphyrin IX Fluorescence Imaging System: Technical Note. J. Neurosurg. 2007, 106, 507–510. [Google Scholar] [CrossRef]
- Potapov, A.A.; Usachev, D.J.; Loshakov, V.A.; Cherekaev, V.A.; Kornienko, V.N.; Pronin, I.N.; Kobiakov, G.L.; Kalinin, P.L.; Gavrilov, A.G.; Stummer, W.; et al. First Experience in 5-ALA Fluorescence-Guided and Endoscopically Assisted Microsurgery of Brain Tumors. Med. Laser Appl. 2008, 23, 202–208. [Google Scholar] [CrossRef]
- Belykh, E.; Miller, E.J.; Hu, D.; Martirosyan, N.L.; Woolf, E.C.; Scheck, A.C.; Byvaltsev, V.A.; Nakaji, P.; Nelson, L.Y.; Seibel, E.J.; et al. Scanning Fiber Endoscope Improves Detection of 5-Aminolevulinic Acid–Induced Protoporphyrin IX Fluorescence at the Boundary of Infiltrative Glioma. World Neurosurg. 2018, 113, e51–e69. [Google Scholar] [CrossRef]
- Devitt, G.; Howard, K.; Mudher, A.; Mahajan, S. Raman Spectroscopy: An Emerging Tool in Neurodegenerative Disease Research and Diagnosis. ACS Chem. Neurosci. 2018, 9, 404–420. [Google Scholar] [CrossRef] [PubMed]
- Neuschmelting, V.; Harmsen, S.; Beziere, N.; Lockau, H.; Hsu, H.T.; Huang, R.; Razansky, D.; Ntziachristos, V.; Kircher, M.F. Dual-Modality Surface-Enhanced Resonance Raman Scattering and Multispectral Optoacoustic Tomography Nanoparticle Approach for Brain Tumor Delineation. Small 2018, 14, 1800740. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, J.C.; Wang, Z.; Huang, S. Raman Spectroscopy on Brain Disorders: Transition from Fundamental Research to Clinical Applications. Biosensors 2022, 13, 27. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Chai, H.; Tang, Q. Advances in the Intraoperative Delineation of Malignant Glioma Margin. Front. Oncol. 2023, 13, 1114450. [Google Scholar] [CrossRef] [PubMed]
- Terrones, O.; Olazar-Intxausti, J.; Anso, I.; Lorizate, M.; Nieto-Garai, J.A.; Contreras, F.X. Raman Spectroscopy as a Tool to Study the Pathophysiology of Brain Diseases. Int. J. Mol. Sci. 2023, 24, 2384. [Google Scholar] [CrossRef] [PubMed]
- Jermyn, M.; Mok, K.; Mercier, J.; Desroches, J.; Pichette, J.; Saint-Arnaud, K.; Bernstein, L.; Guiot, M.C.; Petrecca, K.; Leblond, F. Intraoperative Brain Cancer Detection with Raman Spectroscopy in Humans. Sci. Transl. Med. 2015, 7, 274ra19. [Google Scholar] [CrossRef]
- Hollon, T.C.; Pandian, B.; Adapa, A.R.; Urias, E.; Save, A.V.; Khalsa, S.S.S.; Eichberg, D.G.; D’Amico, R.S.; Farooq, Z.U.; Lewis, S.; et al. Near Real-Time Intraoperative Brain Tumor Diagnosis Using Stimulated Raman Histology and Deep Neural Networks. Nat. Med. 2020, 26, 52–58. [Google Scholar] [CrossRef]
- Karabeber, H.; Huang, R.; Iacono, P.; Samii, J.M.; Pitter, K.; Holland, E.C.; Kircher, M.F. Guiding Brain Tumor Resection Using Surface-Enhanced Raman Scattering Nanoparticles and a Hand-Held Raman Scanner. ACS Nano 2014, 8, 9755. [Google Scholar] [CrossRef]
- Ramakonar, H.; Quirk, B.C.; Kirk, R.W.; Li, J.; Jacques, A.; Lind, C.R.P.; McLaughlin, R.A. Intraoperative Detection of Blood Vessels with an Imaging Needle during Neurosurgery in Humans. Sci. Adv. 2018, 4, eaav4992. [Google Scholar] [CrossRef]
- Li, S.; Li, Y.; Yi, R.; Liu, L.; Qu, J. Coherent Anti-Stokes Raman Scattering Microscopy and Its Applications. Front. Phys. 2020, 8, 598420. [Google Scholar] [CrossRef]
- Orringer, D.A.; Pandian, B.; Niknafs, Y.S.; Hollon, T.C.; Boyle, J.; Lewis, S.; Garrard, M.; Hervey-Jumper, S.L.; Garton, H.J.L.; Maher, C.O.; et al. Rapid Intraoperative Histology of Unprocessed Surgical Specimens via Fibre-Laser-Based Stimulated Raman Scattering Microscopy. Nat. Biomed. Eng. 2017, 1, 0027. [Google Scholar] [CrossRef] [PubMed]
- Hollon, T.C.; Lewis, S.; Pandian, B.; Niknafs, Y.S.; Garrard, M.R.; Garton, H.; Maher, C.O.; McFadden, K.; Snuderl, M.; Lieberman, A.P.; et al. Rapid Intraoperative Diagnosis of Pediatric Brain Tumors Using Stimulated Raman Histology. Cancer Res. 2018, 78, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Lewis, S.; Camelo-Piragua, S.; Ramkissoon, S.H.; Snuderl, M.; Venneti, S.; Fisher-Hubbard, A.; Garrard, M.; Fu, D.; Wang, A.C.; et al. Detection of Human Brain Tumor Infiltration with Quantitative Stimulated Raman Scattering Microscopy. Sci. Transl. Med. 2015, 7, 309ra163. [Google Scholar] [CrossRef]
- Desroches, J.; Lemoine, É.; Pinto, M.; Marple, E.; Urmey, K.; Diaz, R.; Guiot, M.C.; Wilson, B.C.; Petrecca, K.; Leblond, F. Development and First In-Human Use of a Raman Spectroscopy Guidance System Integrated with a Brain Biopsy Needle. J. Biophotonics 2019, 12, e201800396. [Google Scholar] [CrossRef]
- Abramczyk, H.; Imiela, A. The Biochemical, Nanomechanical and Chemometric Signatures of Brain Cancer. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2018, 188, 8–19. [Google Scholar] [CrossRef]
- Bury, D.; Morais, C.L.M.; Ashton, K.M.; Dawson, T.P.; Martin, F.L. Ex Vivo Raman Spectrochemical Analysis Using a Handheld Probe Demonstrates High Predictive Capability of Brain Tumour Status. Biosensors 2019, 9, 49. [Google Scholar] [CrossRef]
- Desroches, J.; Jermyn, M.; Mok, K.; Lemieux-Leduc, C.; Mercier, J.; St-Arnaud, K.; Urmey, K.; Guiot, M.-C.; Marple, E.; Petrecca, K.; et al. Characterization of a Raman Spectroscopy Probe System for Intraoperative Brain Tissue Classification. Biomed. Opt. Express 2015, 6, 2380. [Google Scholar] [CrossRef]
- Jermyn, M.; Mercier, J.; Aubertin, K.; Desroches, J.; Urmey, K.; Karamchandiani, J.; Marple, E.; Guiot, M.C.; Leblond, F.; Petrecca, K. Highly Accurate Detection of Cancer In Situ with Intraoperative, Label-Free, Multimodal Optical Spectroscopy. Cancer Res. 2017, 77, 3942–3950. [Google Scholar] [CrossRef]
- Eschbacher, J.; Martirosyan, N.L.; Nakaji, P.; Sanai, N.; Preul, M.C.; Smith, K.A.; Coons, S.W.; Spetzler, R.F. In Vivo Intraoperative Confocal Microscopy for Real-Time Histopathological Imaging of Brain Tumors: Clinical Article. J. Neurosurg. 2012, 116, 854–860. [Google Scholar] [CrossRef]
- Morsch, M.; Radford, R.A.W.; Don, E.K.; Lee, A.; Hortle, E.; Cole, N.J.; Chung, R.S. Triggering Cell Stress and Death Using Conventional UV Laser Confocal Microscopy. J. Vis. Exp. 2017, 3, 54983. [Google Scholar] [CrossRef]
- Wei, L.T.; Chen, Y.; Yin, C.; Borwege, S.; Sanai, N.; Liu, J.T.C. Optical-Sectioning Microscopy of Protoporphyrin IX Fluorescence in Human Gliomas: Standardization and Quantitative Comparison with Histology. J. Biomed. Opt. 2017, 22, 046005. [Google Scholar] [CrossRef] [PubMed]
- Sanai, N.; Snyder, L.A.; Honea, N.J.; Coons, S.W.; Eschbacher, J.M.; Smith, K.A.; Spetzler, R.F. Intraoperative Confocal Microscopy in the Visualization of 5-Aminolevulinic Acid Fluorescence in Low-Grade Gliomas: Clinical Article. J. Neurosurg. 2011, 115, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Höhne, J.; Schebesch, K.M.; Zoubaa, S.; Proescholdt, M.; Riemenschneider, M.J.; Schmidt, N.O. Intraoperative Imaging of Brain Tumors with Fluorescein: Confocal Laser Endomicroscopy in Neurosurgery. Clinical and User Experience. Neurosurg. Focus 2021, 50, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Abramov, I.; Park, M.T.; Belykh, E.; Dru, A.B.; Xu, Y.; Gooldy, T.C.; Scherschinski, L.; Farber, S.H.; Little, A.S.; Porter, R.W.; et al. Intraoperative Confocal Laser Endomicroscopy: Prospective in Vivo Feasibility Study of a Clinical-Grade System for Brain Tumors. J. Neurosurg. 2022, 138, 587–597. [Google Scholar] [CrossRef]
- Yin, C.; Glaser, A.K.; Leigh, S.Y.; Chen, Y.; Wei, L.; Pillai, P.C.S.; Rosenberg, M.C.; Abeytunge, S.; Peterson, G.; Glazowski, C.; et al. Miniature in Vivo MEMS-Based Line-Scanned Dual-Axis Confocal Microscope for Point-of-Care Pathology. Biomed. Opt. Express 2016, 7, 251. [Google Scholar] [CrossRef]
- Wei, L.; Yin, C.; Liu, J.T.C. Dual-Axis Confocal Microscopy for Point-of-Care Pathology. IEEE J. Sel. Top. Quantum Electron. 2019, 25, 7100910. [Google Scholar] [CrossRef]
- Liu, J.T.C.; Loewke, N.O.; Mandella, M.J.; Levenson, R.M.; Crawford, J.M.; Contag, C.H. Point-of-Care Pathology with Miniature Microscopes. Anal. Cell. Pathol. 2011, 34, 81–98. [Google Scholar] [CrossRef]
- Schichor, C.; Terpolilli, N.; Thorsteinsdottir, J.; Tonn, J.C. Intraoperative Computed Tomography in Cranial Neurosurgery. Neurosurg. Clin. N. Am. 2017, 28, 595–602. [Google Scholar] [CrossRef]
- Shalit, M.N.; Israeli, Y.; Matz, S.; Cohen, M.L. Experience with Intraoperative CT Scanning in Brain Tumors. Surg. Neurol. 1982, 17, 376–382. [Google Scholar] [CrossRef]
- Lunsford, D.L. A Dedicated CT System for the Stereotactic Operating Room. Appl. Neurophysiol. 1982, 45, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Carl, B.; Bopp, M.; Saß, B.; Pojskic, M.; Gjorgjevski, M.; Voellger, B.; Nimsky, C. Reliable Navigation Registration in Cranial and Spine Surgery Based on Intraoperative Computed Tomography. Neurosurg. Focus 2019, 47, E11. [Google Scholar] [CrossRef] [PubMed]
- Ohue, S.; Kumon, Y.; Nagato, S.; Kohno, S.; Harada, H.; Nakagawa, K.; Kikuchi, K.; Miki, H.; Ohnishi, T. Evaluation of Intraoperative Brain Shift Using an Ultrasound-Linked Navigation System for Brain Tumor Surgery. Neurol. Med. Chir. 2010, 50, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Carai, A.; De Benedictis, A.; Calloni, T.; Onorini, N.; Paternò, G.; Randi, F.; Colafati, G.S.; Mastronuzzi, A.; Marras, C.E. Intraoperative Ultrasound-Assisted Extent of Resection Assessment in Pediatric Neurosurgical Oncology. Front. Oncol. 2021, 11, 660805. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, I.A.; Lindseth, F.; Rygh, O.M.; Berntsen, E.M.; Selbekk, T.; Xu, J.; Nagelhus Hernes, T.A.; Harg, E.; Håberg, A.; Unsgaard, G. Functional Neuronavigation Combined with Intra-Operative 3D Ultrasound: Initial Experiences during Surgical Resections Close to Eloquent Brain Areas and Future Directions in Automatic Brain Shift Compensation of Preoperative Data. Acta Neurochir. 2007, 149, 365–378. [Google Scholar] [CrossRef]
- Elmesallamy, W.A.E.A. The Role of Intraoperative Ultrasound in Gross Total Resection of Brain Mass Lesions and Outcome. Egypt. J. Neurol. Psychiatry Neurosurg. 2019, 55, 1–11. [Google Scholar] [CrossRef]
- Chan, H.W.; Pressler, R.; Uff, C.; Gunny, R.; St Piers, K.; Cross, H.; Bamber, J.; Dorward, N.; Harkness, W.; Chakraborty, A. A Novel Technique of Detecting MRI-Negative Lesion in Focal Symptomatic Epilepsy: Intraoperative ShearWave Elastography. Epilepsia 2014, 55, e30–e33. [Google Scholar] [CrossRef]
- Sidhu, P.S.; Cantisani, V.; Dietrich, C.F.; Gilja, O.H.; Saftoiu, A.; Bartels, E.; Bertolotto, M.; Calliada, F.; Clevert, D.A.; Cosgrove, D.; et al. The EFSUMB Guidelines and Recommendations for the Clinical Practice of Contrast-Enhanced Ultrasound (CEUS) in Non-Hepatic Applications: Update 2017 (Long Version). Ultraschall Med. 2018, 39, e2–e44. [Google Scholar] [CrossRef]
- Del Bene, M.; Perin, A.; Casali, C.; Legnani, F.; Saladino, A.; Mattei, L.; Vetrano, I.G.; Saini, M.; DiMeco, F.; Prada, F. Advanced Ultrasound Imaging in Glioma Surgery: Beyond Gray-Scale B-Mode. Front. Oncol. 2018, 8, 576. [Google Scholar] [CrossRef]
- Coburger, J.; Merkel, A.; Scherer, M.; Schwartz, F.; Gessler, F.; Roder, C.; Pala, A.; König, R.; Bullinger, L.; Nagel, G.; et al. Low-Grade Glioma Surgery in Intraoperative Magnetic Resonance Imaging: Results of a Multicenter Retrospective Assessment of the German Study Group for Intraoperative Magnetic Resonance Imaging. Neurosurgery 2016, 78, 775–785. [Google Scholar] [CrossRef]
- Lo, Y.T.; Lee, H.; Shui, C.; Lamba, N.; Korde, R.; Devi, S.; Chawla, S.; Nam, Y.; Patel, R.; Doucette, J.; et al. Intraoperative Magnetic Resonance Imaging for Low-Grade and High-Grade Gliomas: What Is the Evidence? A Meta-Analysis. World Neurosurg. 2021, 149, 232–243.e3. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C.M.; Jones, P.S.; Weinberg, J.S. Intraoperative MRI for Brain Tumors. J. Neurooncol. 2021, 151, 479–490. [Google Scholar] [CrossRef]
- Lippmann, H.; Kruggel, F. Quasi-Real-Time Neurosurgery Support by MRI Processing via Grid Computing. Neurosurg. Clin. N. Am. 2005, 16, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Roder, C.; Stummer, W.; Coburger, J.; Scherer, M.; Haas, P.; von der Brelie, C.; Kamp, M.A.; Löhr, M.; Hamisch, C.A.; Skardelly, M.; et al. Intraoperative MRI-Guided Resection Is Not Superior to 5-Aminolevulinic Acid Guidance in Newly Diagnosed Glioblastoma: A Prospective Controlled Multicenter Clinical Trial. J. Clin. Oncol. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Zhang, X.; Sisniega, A.; Zbijewski, W.B.; Lee, J.; Jones, C.K.; Wu, P.; Han, R.; Uneri, A.; Vagdargi, P.; Helm, P.A.; et al. Combining Physics-Based Models with Deep Learning Image Synthesis and Uncertainty in Intraoperative Cone-Beam CT of the Brain. Med. Phys. 2023, 50, 2607–2624. [Google Scholar] [CrossRef] [PubMed]
- Ozer, E.; Bilecen, A.E.; Ozer, N.B.; Yanikoglu, B. Intraoperative Cytological Diagnosis of Brain Tumours: A Preliminary Study Using a Deep Learning Model. Cytopathology 2023, 34, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.C.; Wang, F.; Chen, X.L.; Yu, X.G.; Ma, X.D.; Zhou, D.B.; Zhu, R.Y.; Xu, B.N. nan Impact of Virtual and Augmented Reality Based on Intraoperative Magnetic Resonance Imaging and Functional Neuronavigation in Glioma Surgery Involving Eloquent Areas. World Neurosurg. 2016, 96, 375–382. [Google Scholar] [CrossRef]
- Mazur, T.; Mansour, T.R.; Mugge, L.; Medhkour, A. Virtual Reality-Based Simulators for Cranial Tumor Surgery: A Systematic Review. World Neurosurg. 2018, 110, 414–422. [Google Scholar] [CrossRef]
- Aleo, D.; Elshaer, Z.; Pfnür, A.; Schuler, P.J.; Fontanella, M.M.; Wirtz, C.R.; Pala, A.; Coburger, J. Evaluation of a Navigated 3D Ultrasound Integration for Brain Tumor Surgery: First Results of an Ongoing Prospective Study. Curr. Oncol. 2022, 29, 6594–6609. [Google Scholar] [CrossRef]
- Matsumae, M.; Nishiyama, J.; Kuroda, K. Intraoperative MR Imaging during Glioma Resection. Magn. Reson. Med. Sci. 2022, 21, 148–167. [Google Scholar] [CrossRef]
- Mikhail, M.; Mithani, K.; Ibrahim, G.M. Presurgical and Intraoperative Augmented Reality in Neuro-Oncologic Surgery: Clinical Experiences and Limitations. World Neurosurg. 2019, 128, 268–276. [Google Scholar] [CrossRef]
- Pennacchietti, V.; Stoelzel, K.; Tietze, A.; Lankes, E.; Schaumann, A.; Uecker, F.C.; Thomale, U.W. First Experience with Augmented Reality Neuronavigation in Endoscopic Assisted Midline Skull Base Pathologies in Children. Childs Nerv. Syst. 2021, 37, 1525–1534. [Google Scholar] [CrossRef] [PubMed]
- Zeiger, J.; Costa, A.; Bederson, J.; Shrivastava, R.K.; Iloreta, A.M.C. Use of Mixed Reality Visualization in Endoscopic Endonasal Skull Base Surgery. Oper. Neurosurg. 2020, 19, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Dang, A.; Dang, D.; Vallish, B.N. Extent of Use of Artificial Intelligence & Machine Learning Protocols in Cancer Diagnosis: A Scoping Review. Indian J. Med. Res. 2023, 157, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Fürtjes, G.; Reinecke, D.; von Spreckelsen, N.; Meißner, A.K.; Rueß, D.; Timmer, M.; Freudiger, C.; Ion-Margineanu, A.; Khalid, F.; Watrinet, K.; et al. Intraoperative Microscopic Autofluorescence Detection and Characterization in Brain Tumors Using Stimulated Raman Histology and Two-Photon Fluorescence. Front. Oncol. 2023, 13, 1146031. [Google Scholar] [CrossRef]
- Cardone, D.; Trevisi, G.; Perpetuini, D.; Filippini, C.; Merla, A.; Mangiola, A. Intraoperative Thermal Infrared Imaging in Neurosurgery: Machine Learning Approaches for Advanced Segmentation of Tumors. Phys. Eng. Sci. Med. 2023, 46, 325–337. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Modality | Concept Description | Advantages | Limitations |
|---|---|---|---|
| Intraoperative Ultrasound (iUS) | Utilizes high-frequency sound waves to create images of the brain during surgery | Provides dynamic feedback; enhances tumor localization | Limited by operator experience; may not be effective for all tumor types |
| Intraoperative Magnetic Resonance Imaging (iMRI) | Utilizes magnetic fields and radio waves to create detailed images of the brain during surgery | High-resolution imaging; detect brain shift | Requires significant infrastructure; may prolong surgery time |
| Intraoperative Computed Tomography (iCT) | Utilizes X-ray technology to create cross-sectional images of the brain during surgery | Rapid image acquisition; Seamless incorporation into surgery | Exposure to ionizing radiation; lower soft tissue contrast compared to MRI |
| Surgical Microscope | An optical instrument with high magnification used during brain tumor surgery for precise visualization | High-definition visualization; differentiation between healthy tissue and tumor; facilitates maximal safe resection; can record surgical procedures in high-definition | Restricted field of view; limited maneuverability due to bulk and weight; operator fatigue due to ergonomics |
| Exoscope | A high-definition camera that offers a panoramic view of the surgical area | Improved magnification and illumination; better depth of field; enhances ergonomics for surgeons | Potential learning curve for new users; cost of integration into the surgical workflow |
| Fluorescence-Guided Surgery (FGS) | Utilizes fluorescent agents to delineate tumor tissue during surgery, providing real-time intraoperative tumor visualization | Real-time visualization; facilitates maximal safe tumor resection | Limited by the availability of fluorescent agents; may not be effective for all tumor types |
| Raman Spectroscopy | Uses monochromatic light for real-time, high-resolution biochemical tissue analysis at molecular level | Distinguishes tumor cells from healthy brain tissue with high accuracy; objective and automated feedback | Weak signal intensity; challenges in data acquisition and processing times for real-time applicability |
| Confocal Microscopy | Uses spatial filters for high-contrast, micron-scale resolution imaging | High-contrast and detailed images; visualization of structures in three-dimensional volume; employs detection of fluorescence markers for tumor visualization | Motion artifacts due to slow frame rates; relies on specific agents; lacks adjustable imaging depth |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bin-Alamer, O.; Abou-Al-Shaar, H.; Gersey, Z.C.; Huq, S.; Kallos, J.A.; McCarthy, D.J.; Head, J.R.; Andrews, E.; Zhang, X.; Hadjipanayis, C.G. Intraoperative Imaging and Optical Visualization Techniques for Brain Tumor Resection: A Narrative Review. Cancers 2023, 15, 4890. https://doi.org/10.3390/cancers15194890
Bin-Alamer O, Abou-Al-Shaar H, Gersey ZC, Huq S, Kallos JA, McCarthy DJ, Head JR, Andrews E, Zhang X, Hadjipanayis CG. Intraoperative Imaging and Optical Visualization Techniques for Brain Tumor Resection: A Narrative Review. Cancers. 2023; 15(19):4890. https://doi.org/10.3390/cancers15194890
Chicago/Turabian StyleBin-Alamer, Othman, Hussam Abou-Al-Shaar, Zachary C. Gersey, Sakibul Huq, Justiss A. Kallos, David J. McCarthy, Jeffery R. Head, Edward Andrews, Xiaoran Zhang, and Constantinos G. Hadjipanayis. 2023. "Intraoperative Imaging and Optical Visualization Techniques for Brain Tumor Resection: A Narrative Review" Cancers 15, no. 19: 4890. https://doi.org/10.3390/cancers15194890
APA StyleBin-Alamer, O., Abou-Al-Shaar, H., Gersey, Z. C., Huq, S., Kallos, J. A., McCarthy, D. J., Head, J. R., Andrews, E., Zhang, X., & Hadjipanayis, C. G. (2023). Intraoperative Imaging and Optical Visualization Techniques for Brain Tumor Resection: A Narrative Review. Cancers, 15(19), 4890. https://doi.org/10.3390/cancers15194890