
Holmium-166 Transarterial Radioembolization for the Treatment of Intrahepatic Cholangiocarcinoma: A Case Series

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Study Procedures
2.3. Outcome Measures
3. Results
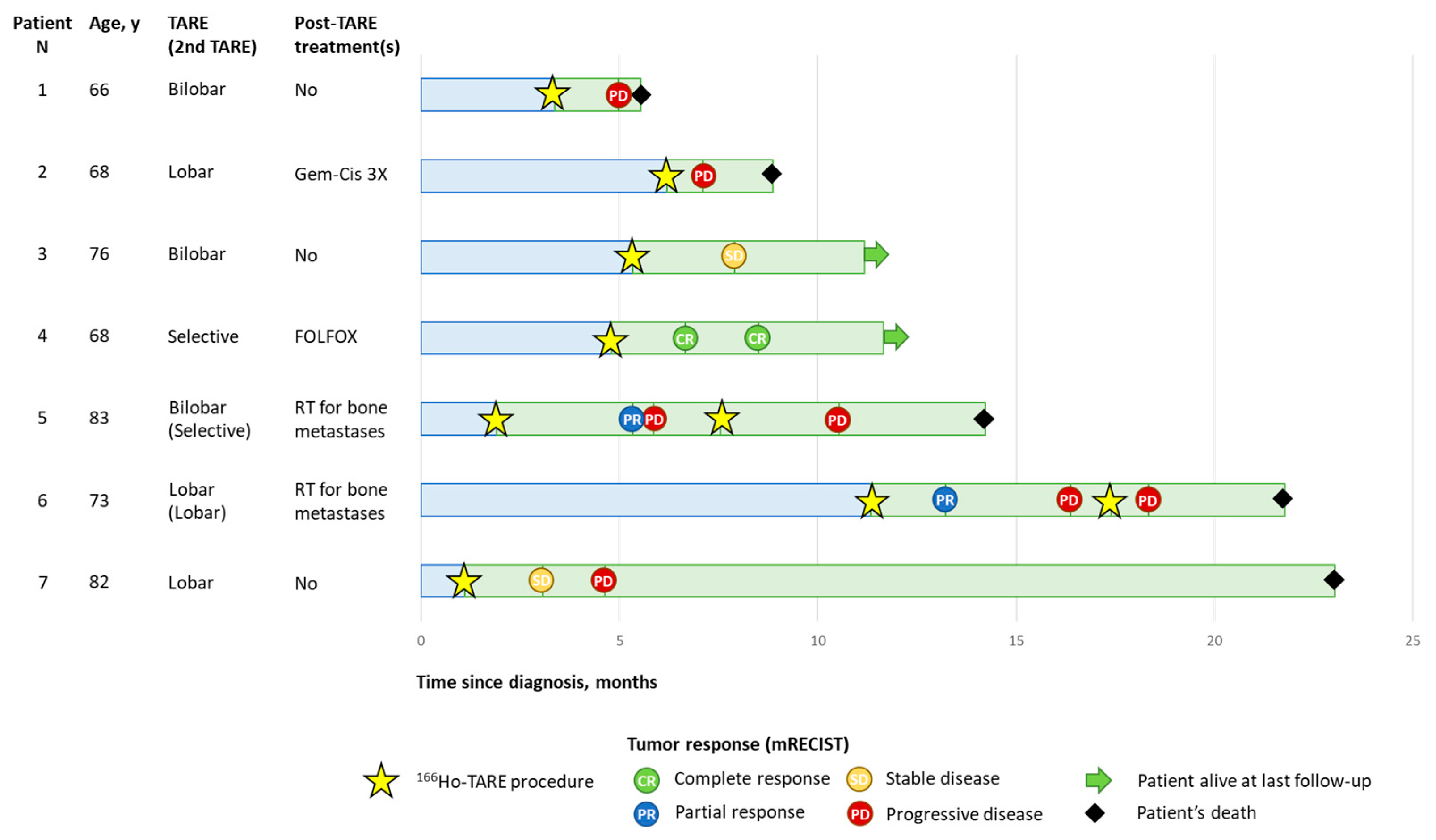
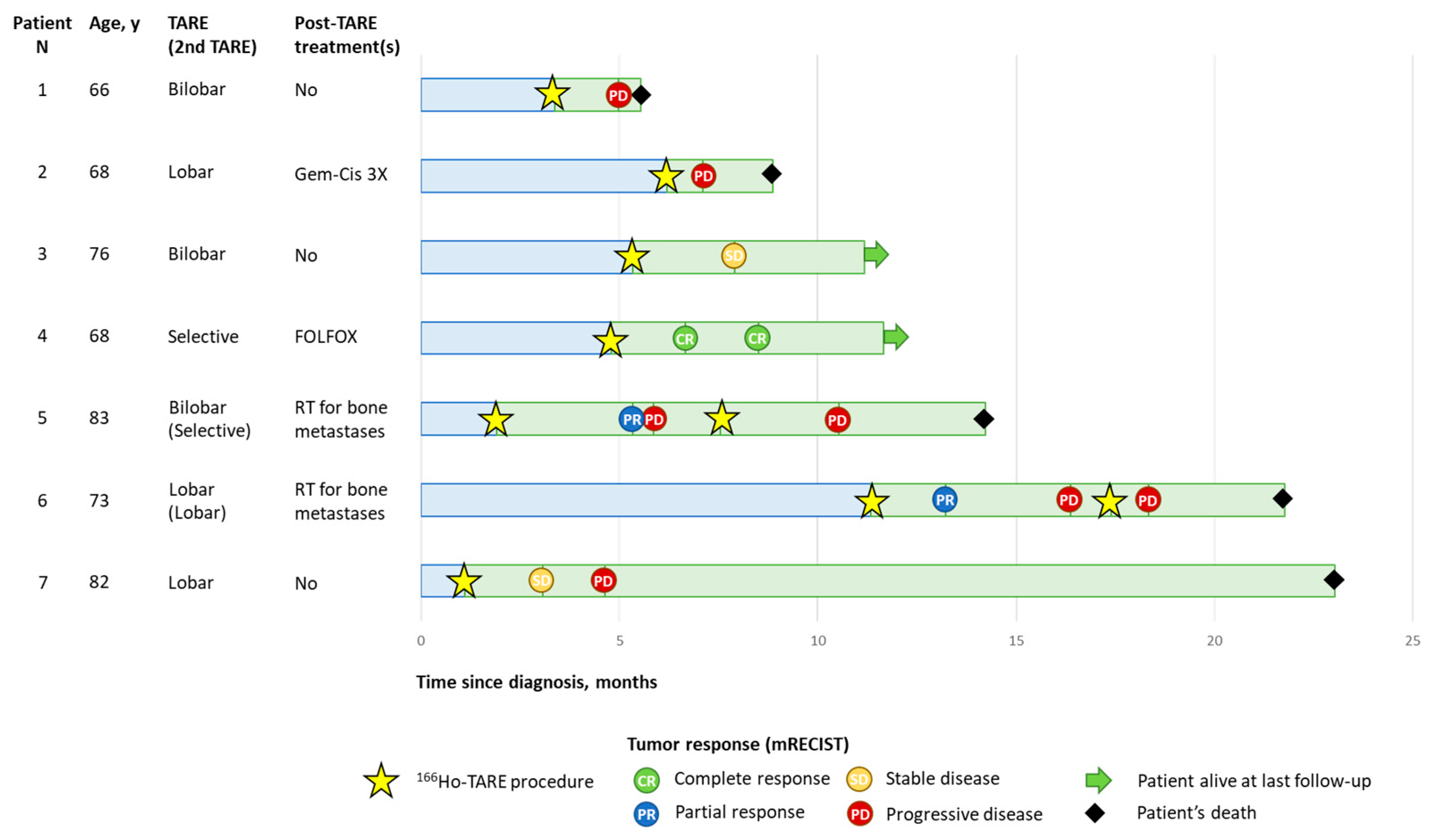
3.1. Case Series
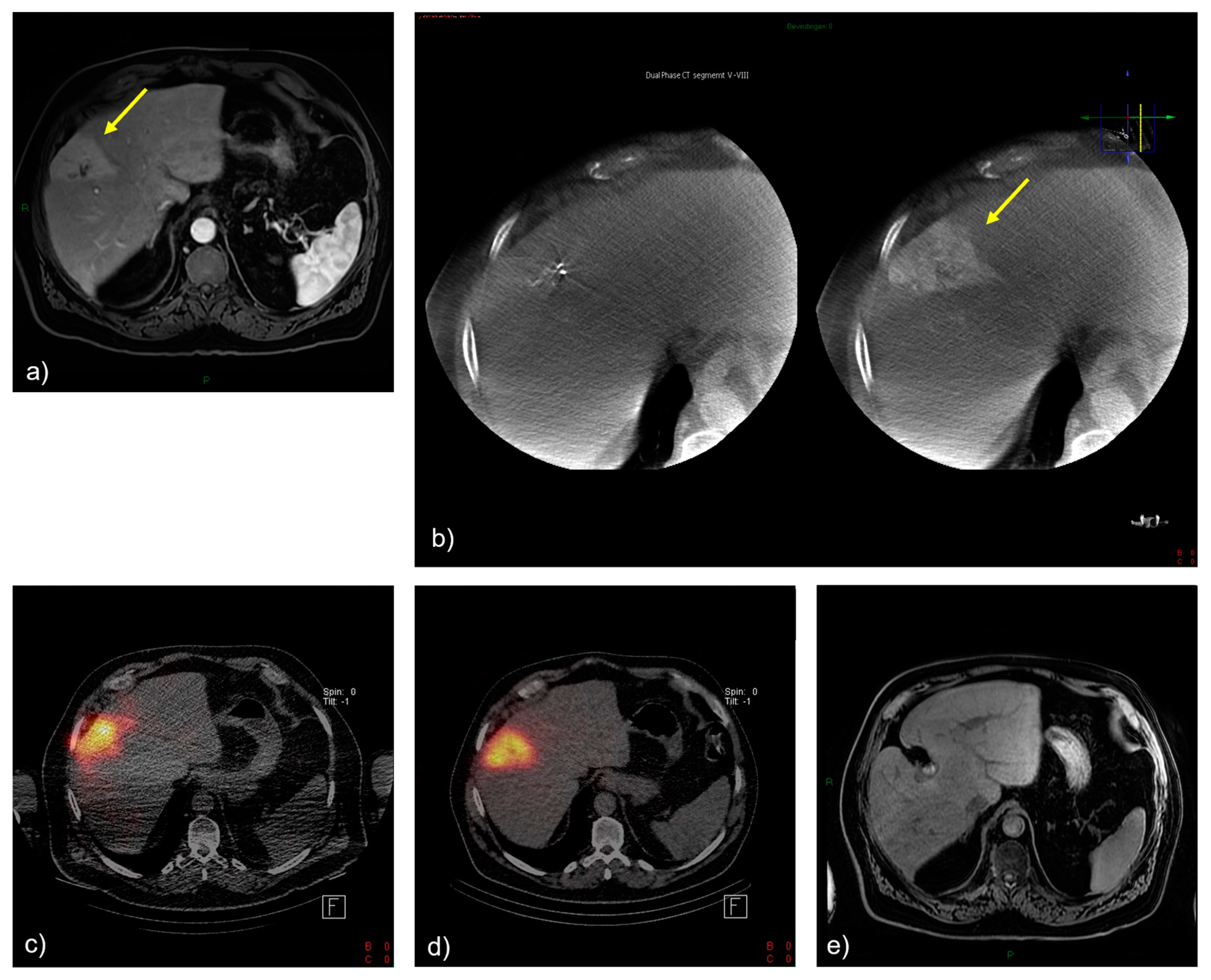
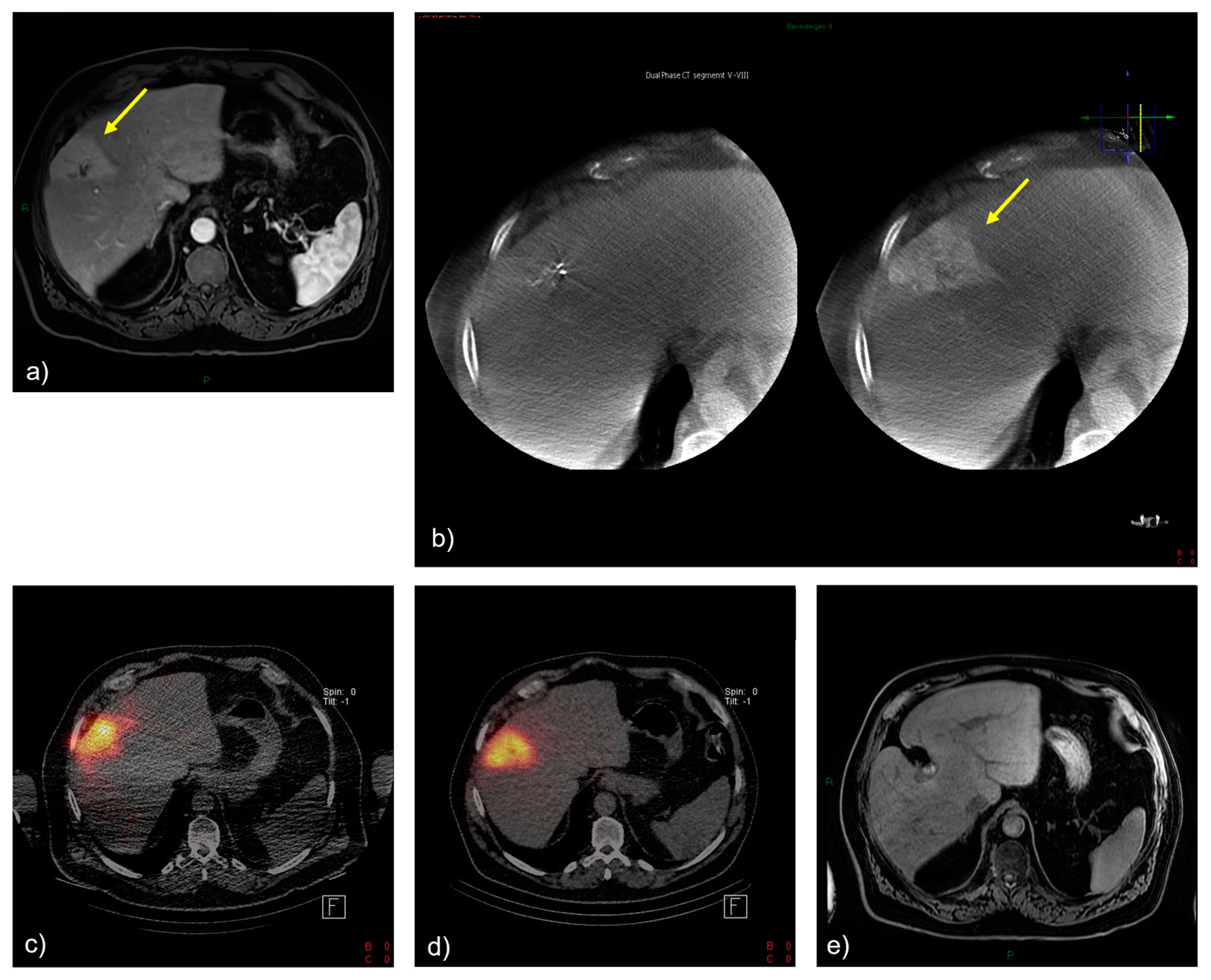
3.2. Selected Case 1 (Patient N 4, Figure 2)
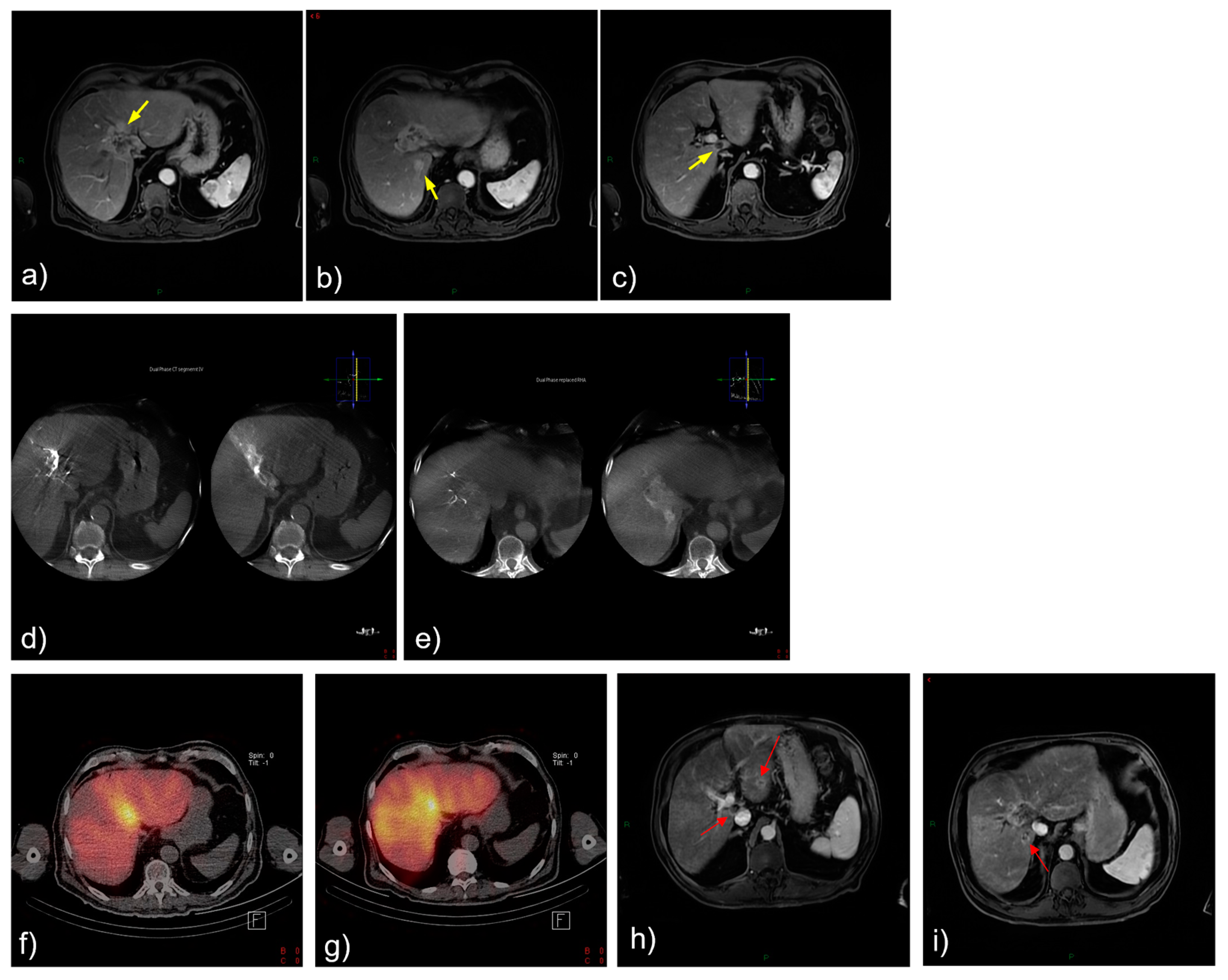
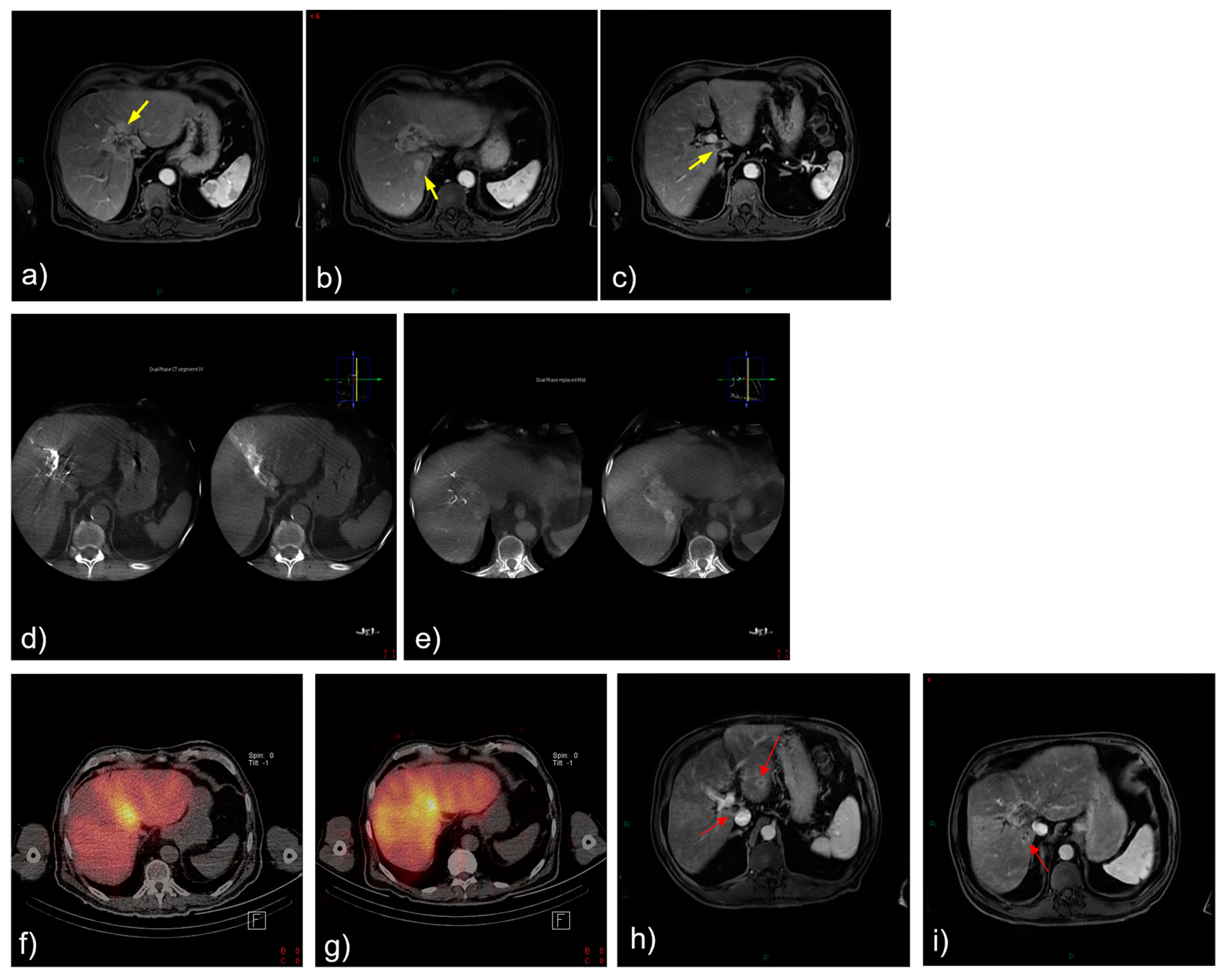
3.3. Selected Case 2 (Patient N 5, Figure 3)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mauro, E.; Ferrer-Fabrega, J.; Sauri, T.; Soler, A.; Cobo, A.; Burrel, M.; Iserte, G.; Forner, A. New Challenges in the Management of Cholangiocarcinoma: The Role of Liver Transplantation, Locoregional Therapies, and Systemic Therapy. Cancers 2023, 15, 1244. [Google Scholar] [CrossRef] [PubMed]
- Bertuccio, P.; Malvezzi, M.; Carioli, G.; Hashim, D.; Boffetta, P.; El-Serag, H.B.; La Vecchia, C.; Negri, E. Global trends in mortality from intrahepatic and extrahepatic cholangiocarcinoma. J. Hepatol. 2019, 71, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Fondevila, C.; Donadon, M.; Gringeri, E.; Mocchegiani, F.; Schlitt, H.J.; Ijzermans, J.N.M.; Vivarelli, M.; Zieniewicz, K.; Olde Damink, S.W.M.; et al. Surgery for cholangiocarcinoma. Liver Int. 2019, 39, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Oh, D.-Y.; He, A.R.; Qin, S.; Chen, L.-T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Lee, M.A.; Kitano, M.; et al. Durvalumab plus Gemcitabine and Cisplatin in Advanced Biliary Tract Cancer. NEJM Evid. 2022, 1, EVIDoa2200015. [Google Scholar] [CrossRef]
- Mosconi, C.; Calandri, M.; Javle, M.; Odisio, B.C. Interventional radiology approaches for intra-hepatic cholangiocarcinoma. Chin. Clin. Oncol. 2020, 9, 8. [Google Scholar] [CrossRef]
- Edeline, J.; Lamarca, A.; McNamara, M.G.; Jacobs, T.; Hubner, R.A.; Palmer, D.; Groot Koerkamp, B.; Johnson, P.; Guiu, B.; Valle, J.W. Locoregional therapies in patients with intrahepatic cholangiocarcinoma, A systematic review and pooled analysis. Cancer Treat. Rev. 2021, 99, 102258. [Google Scholar] [CrossRef]
- Memon, K.; Lewandowski, R.J.; Kulik, L.; Riaz, A.; Mulcahy, M.F.; Salem, R. Radioembolization for primary and metastatic liver cancer. Semin. Radiat. Oncol. 2011, 21, 294–302. [Google Scholar] [CrossRef]
- Schartz, D.A.; Porter, M.; Schartz, E.; Kallas, J.; Gupta, A.; Butani, D.; Cantos, A. Transarterial Yttrium-90 Radioembolization for Unresectable Intrahepatic Cholangiocarcinoma: A Systematic Review and Meta-Analysis. J. Vasc. Interv. Radiol. 2022, 33, 679–686. [Google Scholar] [CrossRef]
- Elschot, M.; Nijsen, J.F.; Lam, M.G.; Smits, M.L.J.; Prince, J.F.; Viergever, M.A.; van den Bosch, M.A.A.J.; Zonnenberg, B.A.; de Jong, H.W.A.M. 99mTc-MAA overestimates the absorbed dose to the lungs in radioembolization: A quantitative evaluation in patients treated with 166Ho-microspheres. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1965–1975. [Google Scholar] [CrossRef]
- Levillain, H.; Duran Derijckere, I.; Ameye, L.; Guiot, T.; Braat, A.; Meyer, C.; Vancerlinden, B.; Reynaert, N.; Hendlisz, A.; Lam, M.; et al. Personalised radioembolization improves outcomes in refractory intra-hepatic cholangiocarcinoma: A multicenter study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2270–2279. [Google Scholar] [CrossRef]
- Garin, E.; Tselikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; de Baere, T.; Assenat, E.; Tacher, V.; Robert, C.; Terroir-Cassou-Mounat, M.; et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): A randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Schaarschmidt, B.M.; Kloeckner, R.; Dertnig, T.; Demircioglu, A.; Müller, L.; Auer, T.A.; Dos Santos, D.P.; Steinle, V.; Miederer, M.; Gebauer, B.; et al. Real-Life Experience in the Treatment of Intrahepatic Cholangiocarcinoma by 90Y Radioembolization: A Multicenter Retrospective Study. J. Nucl. Med. 2023, 64, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Prince, J.F.; van den Bosch, M.; Nijsen, J.F.W.; Smits, M.L.J.; van den Hoven, A.F.; Nikolakopoulos, S.; Wessels, F.J.; Bruijnen, R.C.G.; Braat, M.N.G.J.A.; Zonnenberg, B.A.; et al. Efficacy of Radioembolization with (166)Ho-Microspheres in Salvage Patients with Liver Metastases: A Phase 2 Study. J. Nucl. Med. 2018, 59, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Reinders, M.T.M.; van Erpecum, K.J.; Smits, M.L.J.; Braat, A.J.A.T.; de Bruijne, J.; Bruijnen, R.; Sprengers, D.; de Man, R.A.; Vegt, E.; Ijzermans, J.N.M.; et al. Safety and Efficacy of (166)Ho Radioembolization in Hepatocellular Carcinoma: The HEPAR Primary Study. J. Nucl. Med. 2022, 63, 1891–1898. [Google Scholar] [CrossRef]
- Bastiaannet, R.; van Roekel, C.; Smits, M.L.J.; Elias, S.G.; van Amsterdam, W.A.C.; Doan, D.; Prince, J.F.; Bruijnen, R.C.G.; de Jong, H.W.A.M.; Lam, M.G.E.H. First Evidence for a Dose-Response Relationship in Patients Treated with (166)Ho Radioembolization: A Prospective Study. J. Nucl. Med. 2020, 61, 608–612. [Google Scholar] [CrossRef]
- Van Roekel, C.; Bastiaannet, R.; Smits, M.L.J.; Bruijnen, R.C.; Braat, A.J.A.T.; de Jong, H.W.A.M.; Elias, S.G.; Lam, M.G.E.H. Dose-Effect Relationships of (166)Ho Radioembolization in Colorectal Cancer. J. Nucl. Med. 2021, 62, 272–279. [Google Scholar] [CrossRef]
- Depalo, T.; Boni, G.; Ghinolfi, D.; Bozzi, E.; Cervelli, R.; Catalano, G.; Volterrani, D.; Bargellini, I. Potential Benefits of Holmium-166 Radioembolization as a Neoadjuvant Treatment of Intrahepatic Cholangiocarcinoma. CardioVascular Interv. Radiol. 2021, 44, 345–347. [Google Scholar] [CrossRef]
- Weber, M.; Lam, M.; Chiesa, C.; Konijnenberg, M.; Cremonesi, M.; Flamen, P.; Gnesin, S.; Bodei, L.; Kracmerova, T.; Luster, M.; et al. EANM procedure guideline for the treatment of liver cancer and liver metastases with intra-arterial radioactive compounds. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1682–1699. [Google Scholar] [CrossRef]
- Freites-Martinez, A.; Santana, N.; Arias-Santiago, S.; Viera, A. Using the Common Terminology Criteria for Adverse Events (CTCAE—Version 5.0) to Evaluate the Severity of Adverse Events of Anticancer Therapies. Actas Dermo-Sifiliogr. 2021, 112, 90–92. [Google Scholar] [CrossRef]
- Ness, J.R.; Molvar, C. Radioembolization of Intrahepatic Cholangiocarcinoma: Patient Selection, Outcomes, and Competing Therapies. Semin. Intervent. Radiol. 2021, 38, 438–444. [Google Scholar] [CrossRef]
- Laidlaw, G.L.; Johnson, G.E. Recognizing and Managing Adverse Events in Y-90 Radioembolization. Semin. Intervent. Radiol. 2021, 38, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Reinders, M.T.M.; Smits, M.L.J.; van Roekel, C.; Braat, A. Holmium-166 Microsphere Radioembolization of Hepatic Malignancies. Semin. Nucl. Med. 2019, 49, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Van Roekel, C.; Smits, M.L.J.; Prince, J.F.; Bruijnen, R.C.G.; van den Bosch, M.; Lam, M. Quality of life in patients with liver tumors treated with holmium-166 radioembolization. Clin. Exp. Metastasis 2020, 37, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.C.G., 2nd; Simo, K.A.; Hansen, P.; Rocha, F.; Philips, P.; McMasters, K.M.; Tatum, C.M.; Kelly, L.R.; Driscoll, M.; Sharma, V.R.; et al. Drug-Eluting Bead, Irinotecan Therapy of Unresectable Intrahepatic Cholangiocarcinoma (DELTIC) with Concomitant Systemic Gemcitabine and Cisplatin. Ann. Surg. Oncol. 2022, 29, 5462–5473. [Google Scholar] [CrossRef]
- Smits, M.L.; Elschot, M.; van den Bosch, M.A.; van de Maat, G.H.; van het Schip, A.D.; Zonnenberg, B.A.; Seevinck, P.R.; Verkooijen, H.M.; Bakker, C.J.; de Jong, H.W.A.M.; et al. In vivo dosimetry based on SPECT and MR imaging of 166Ho-microspheres for treatment of liver malignancies. J. Nucl. Med. 2013, 54, 2093–2100. [Google Scholar] [CrossRef]
- Chin, R.I.; Bommireddy, A.; Fraum, T.J.; Ludwig, D.R.; Huang, Y.; Zoberi, J.E.; Garcia-Ramirez, J.L.; Maughan, N.M.; Chapman, W.; Korenblat, K.; et al. Clinical Outcomes of Patients with Unresectable Primary Liver Cancer Treated With Yttrium-90 Radioembolization With an Escalated Dose. Adv. Radiat. Oncol. 2022, 7, 100948. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| No. | Sex | Age at Diagnosis (Years) | PS | Comorbidities | Tumor Distribution | T-N-M | Systemic Treatment before TARE | Target Volume (mL) | N of TARE Procedures | Administered Activity (GBq) | Tumor Dose (Gy) | Normal Liver Dose (Gy) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 66 | 0 | AHT, DM2, asthma, metastatic esophageal cancer | Bilobar | 2-0-0 | Carbotaxol, Cis-5FU | 1845 | 1 | 7 | 71 | 44 |
| 2 | Male | 68 | 0 | DM2 | Lobar | 4-1-1 | Cisplatinum–gemcitabine | 2787 | 1 | 5.6 | 80 | 23 |
| 3 | Male | 76 | 0 | AHT, DM2, iCVA, HF with reduced ejection fraction, pacemaker | Bilobar | 4-1-0 | Gemcitabine–oxaliplatin | 1660 | 1 | 4.26 | 67 | 34 |
| 4 | Male | 68 | 0 | AHT, DM2, iCMP, OSAS | Segmental | 1-1-0 | Cisplatinum–gemcitabine | 451 | 1 | 5.24 | 280 | 22 |
| 5 | Male | 83 | 2 | AHT, colon cancer, mechanical AVP | Bilobar | 2-1-1 | None | 1693 | 2 | 4.5 | 75 | 38 |
| 6 | Male | 73 | 0 | AHT, DM2, OSAS | Lobar | 3-1-1 | Cisplatinum–gemcitabine, FOLFOX | 1680 | 2 | 4.94 | 70 | 31 |
| 7 | Male | 82 | 0 | HF with reduced ejection fraction | Segmental | 4-0-0 | None | 1397 | 1 | 4.22 | 103 | 38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vermeulen, S.; De Keukeleire, K.; Dorny, N.; Colle, I.; Van Den Bossche, B.; Nuttens, V.; Ooms, D.; De Bondt, P.; De Winter, O. Holmium-166 Transarterial Radioembolization for the Treatment of Intrahepatic Cholangiocarcinoma: A Case Series. Cancers 2023, 15, 4791. https://doi.org/10.3390/cancers15194791
Vermeulen S, De Keukeleire K, Dorny N, Colle I, Van Den Bossche B, Nuttens V, Ooms D, De Bondt P, De Winter O. Holmium-166 Transarterial Radioembolization for the Treatment of Intrahepatic Cholangiocarcinoma: A Case Series. Cancers. 2023; 15(19):4791. https://doi.org/10.3390/cancers15194791
Chicago/Turabian StyleVermeulen, Sim, Katrien De Keukeleire, Nicole Dorny, Isabelle Colle, Bert Van Den Bossche, Victor Nuttens, Dirk Ooms, Pieter De Bondt, and Olivier De Winter. 2023. "Holmium-166 Transarterial Radioembolization for the Treatment of Intrahepatic Cholangiocarcinoma: A Case Series" Cancers 15, no. 19: 4791. https://doi.org/10.3390/cancers15194791
APA StyleVermeulen, S., De Keukeleire, K., Dorny, N., Colle, I., Van Den Bossche, B., Nuttens, V., Ooms, D., De Bondt, P., & De Winter, O. (2023). Holmium-166 Transarterial Radioembolization for the Treatment of Intrahepatic Cholangiocarcinoma: A Case Series. Cancers, 15(19), 4791. https://doi.org/10.3390/cancers15194791