

What Is Most Important to Family Caregivers When Helping Patients Make Treatment-Related Decisions: Findings from a National Survey

 , , , , , , ,
, , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Measures
3.1. Demographic and Clinical Characteristics
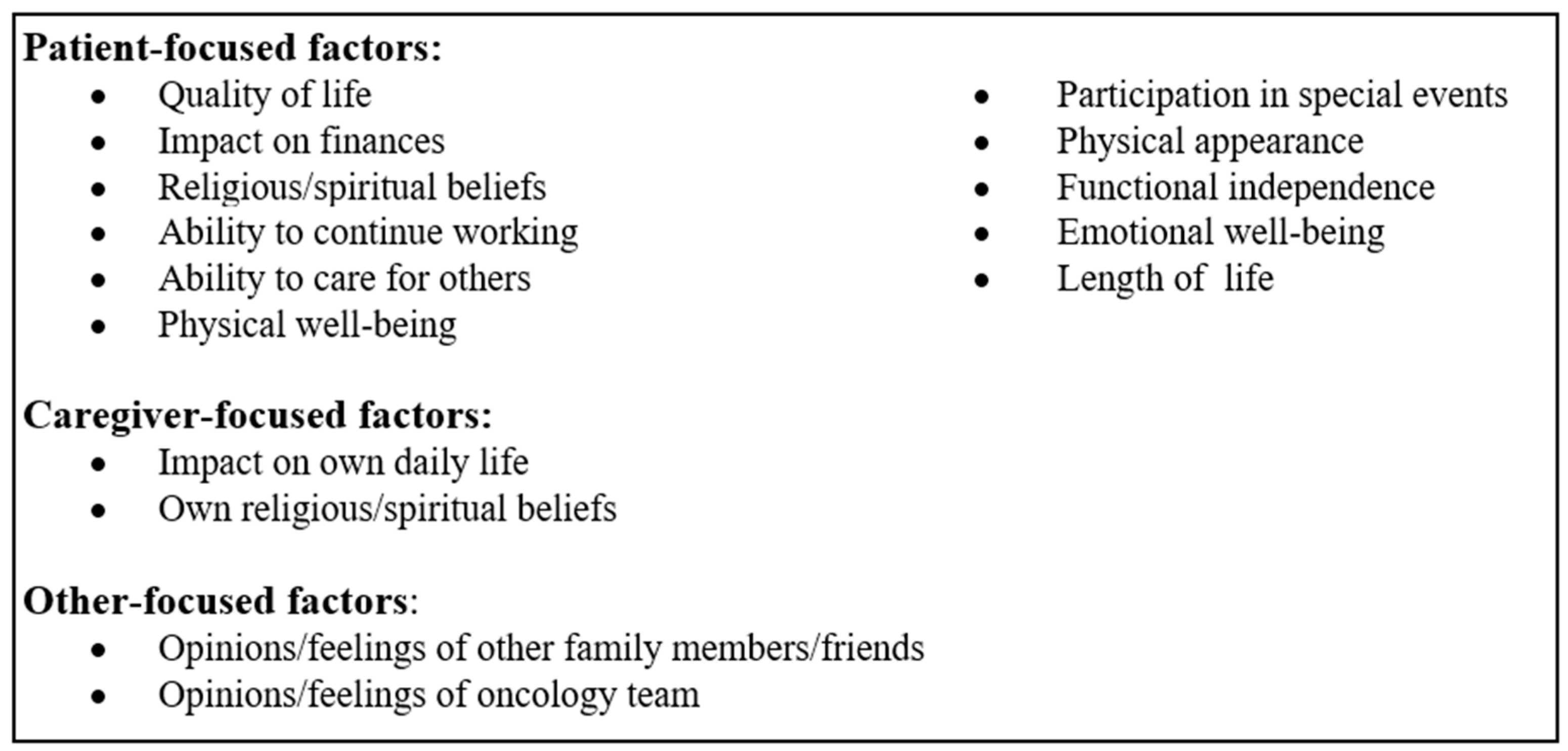
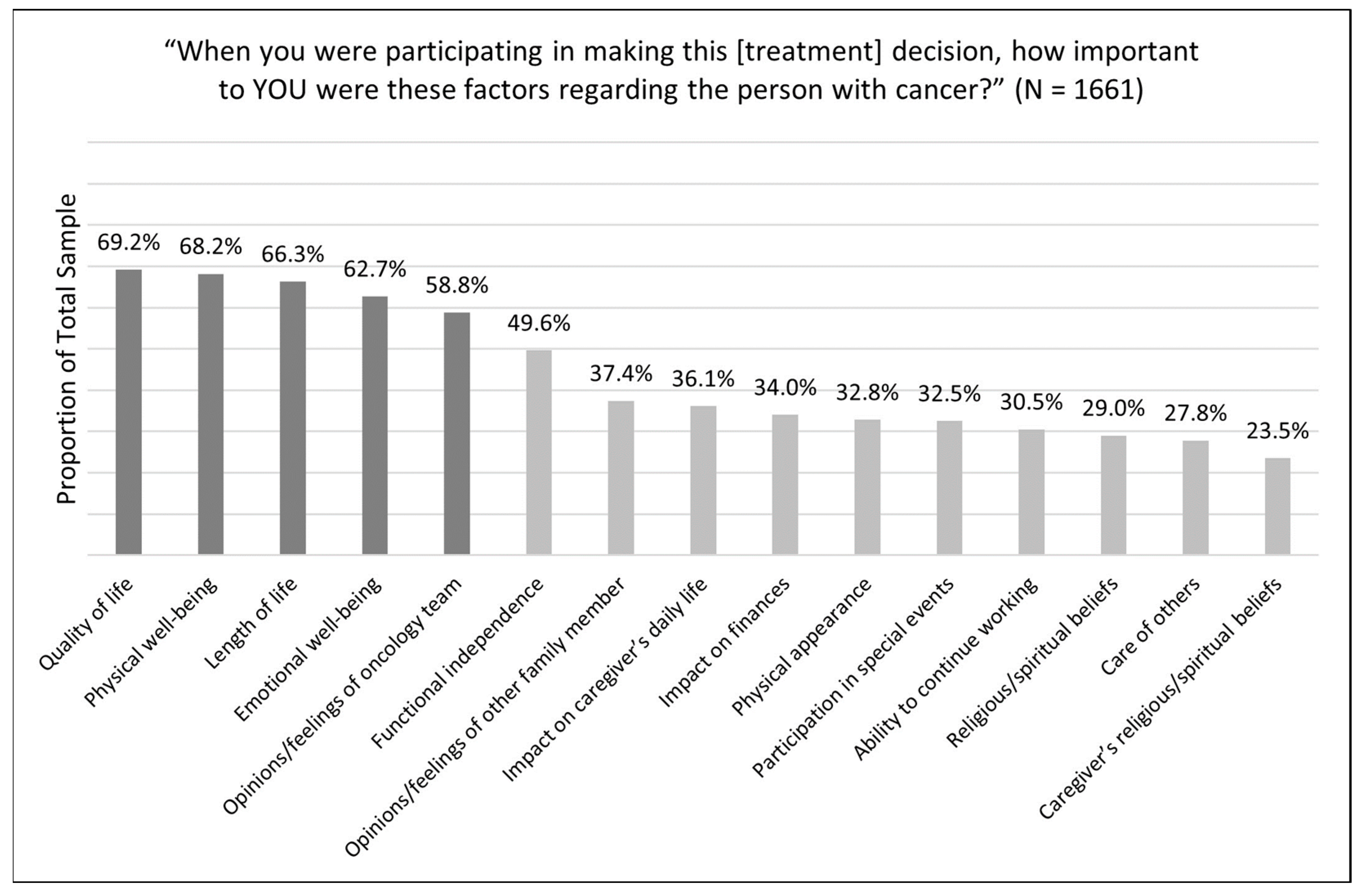
3.2. Items to Measure Treatment Decision Making and Caregiver Factors
4. Statistical Methods
5. Results
6. Discussion
6.1. Limitations
6.2. Clinical Implications
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Witteman, H.O.; Ndjaboue, R.; Vaisson, G.; Dansokho, S.C.; Arnold, B.; Bridges, J.F.P.; Comeau, S.; Fagerlin, A.; Gavaruzzi, T.; Marcoux, M.; et al. Clarifying values: An updated and expanded systematic review and meta-analysis. Med. Decis. Mak. 2021, 41, 801–820. [Google Scholar] [CrossRef]
- Yates, J.F.; de Oliveira, S. Culture and decision making. Organ. Behav. Hum. Decis. Process 2016, 136, 106–118. [Google Scholar] [CrossRef]
- Sagiv, L.; Roccas, S. How do values affect behavior? Let me count the ways. Pers. Soc. Psychol. Rev. 2021, 25, 295–316. [Google Scholar] [CrossRef]
- Karimi-Dehkordi, M.; Spiers, J.; Clark, A.M. An evolutionary concept analysis of “patients’ values”. Nurs. Outlook 2019, 67, 523–539. [Google Scholar] [CrossRef] [PubMed]
- Bechthold, A.C.; Knoepke, C.E.; Ejem, D.B.; McIlvennan, C.K.; Wells, R.D.; Matlock, D.D.; Bakitas, M.A.; Dionne-Odom, J.N. How values are discussed, reflected upon, and acted on by patients and family caregivers in the context of heart failure: A scoping review. Med. Decis. Mak. 2023, 43, 508–520. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Costello, D.M.; Naik, A.D.; Davenport, C.; Hernandez-Bigos, K.; Van Liew, J.R.; Esterson, J.; Kiwak, E.; Dindo, L. Outcome goals and health care preferences of older adults with multiple chronic conditions. JAMA Netw. Open 2021, 4, e211271. [Google Scholar] [CrossRef]
- National Consensus Project for Quality Palliative Care. Clinical Practice Guidelines for Quality Palliative Care, 4th ed.; National Coalition for Hospice and Palliative Care: Richmond, VA, USA, 2018; Available online: https://www.nationalcoalitionhpc.org/ncp (accessed on 5 July 2023).
- Hussaini, Q.; Smith, T.J. Incorporating palliative care into oncology practice: Why and how. Clin. Adv. Hematol. Oncol. 2021, 19, 390–395. [Google Scholar]
- Agency for Healthcare Research and Quality. The SHARE Approach—Essential Steps of Shared Decision Making: Expanded Reference Guide with Sample Conversation Starters. Updated September 2020. Available online: https://www.ahrq.gov/health-literacy/professional-training/shared-decision/tool/resource-2.html (accessed on 5 July 2023).
- Alston, C.; Berger, Z.; Brownlee, S.; Mslgroup, Q.; Elwyn, G.; Fowler, F.; Hall, L.K.; Moulton, B.; Paget, L.; Shebel, B.H.; et al. Shared Decision-Making Strategies for Best Care: Patient Decision Aids; NAM Perspectives; National Academy of Medicine: Washington, DC, USA, 2014. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Roundtable on Value&Science-Driven Health Care; Yong, P.L.; Olsen, L.; McGinnis, J.M. (Eds.) Value in Health Care: Accounting for Cost, Quality, Safety, Outcomes, and Innovation; National Academies Press (US): Washington, DC, USA, 2010. [Google Scholar]
- National Academies of Sciences, Engineering, and Medicine. Improving the Evidence Base for Treatment Decision Making for Older Adults with Cancer: Proceedings of a Workshop in Brief; The National Academies Press: Washington, DC, USA, 2021; Available online: https://nap.nationalacademies.org/catalog/26157/improving-the-evidence-base-for-treatment-decision-making-for-older-adults-with-cancer (accessed on 5 July 2023).
- Bennett, R.; DeGuzman, P.B.; LeBaron, V.; Wilson, D.; Jones, R.A. Exploration of shared decision making in oncology within the United States: A scoping review. Support. Care Cancer 2022, 31, 94. [Google Scholar] [CrossRef]
- Dionne-Odom, J.N.; Ejem, D.; Wells, R.; Barnato, A.E.; Taylor, R.A.; Rocque, G.B.; Turkman, Y.E.; Kenny, M.; Ivankova, N.V.; Bakitas, M.A.; et al. How family caregivers of persons with advanced cancer assist with upstream healthcare decision-making: A qualitative study. PLoS ONE 2019, 14, e0212967. [Google Scholar] [CrossRef]
- Laidsaar-Powell, R.C.; Butow, P.N.; Bu, S.; Charles, C.; Gafni, A.; Lam, W.; Jansen, J.; McCaffery, K.; Shepherd, H.; Tattersall, M.; et al. Physician-patient-companion communication and decision-making: A systematic review of triadic medical consultations. Patient Educ. Couns. 2013, 91, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Lamore, K.; Montalescot, L.; Untas, A. Treatment decision-making in chronic diseases: What are the family members’ roles, needs and attitudes? A systematic review. Patient Educ. Couns. 2017, 100, 2172–2181. [Google Scholar] [CrossRef] [PubMed]
- Garvelink, M.M.; Ngangue, P.A.; Adekpedjou, R.; Diouf, N.T.; Goh, L.; Blair, L.; Légaré, F. A synthesis of knowledge about caregiver decision making finds gaps in support for those who care for aging loved ones. Health Aff. 2016, 35, 619–626. [Google Scholar] [CrossRef]
- Gieseler, F.; Heidenreich, A.; Schubert, J.; Frielitz, F.; Rehmann-Sutter, C.; Wörler, F.; Schües, C.; Hübner, J.; Elsner, S.; Block, K.; et al. The role of family confidants and caregivers in the care of older cancer patients: Extending the concept of “shared decision-making”. Health Sci. Rep. 2021, 4, e281. [Google Scholar] [CrossRef] [PubMed]
- Kelley, K.; Clark, B.; Brown, V.; Sitzia, J. Good practice in the conduct and reporting of survey research. Int. J. Qual. Health Care 2003, 15, 261–266. [Google Scholar] [CrossRef]
- Dionne-Odom, J.N.; Ornstein, K.A.; Azuero, A.; Harrell, E.R.; Gazaway, S.; Watts, K.A.; Ejem, D.; Bechthold, A.C.; Lee, K.; Puga, F.; et al. Bias reported by family caregivers in support received when assisting patients with cancer-related decision-making. Cancer Med. 2023, 12, 3567–3576. [Google Scholar] [CrossRef] [PubMed]
- CancerCare. Cancer Caregivers: National Research Report on Shared Treatment Decision-Making; CancerCare: New York, NY, USA, 2022; Available online: https://media.cancercare.org/documents/272/original/CancerCare_DecisionMakingReport_20220715.pdf (accessed on 5 July 2023).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum: Mahwah, NJ, USA, 1988. [Google Scholar]
- Hobbs, G.S.; Landrum, M.B.; Arora, N.K.; Ganz, P.A.; van Ryn, M.; Weeks, J.C.; Mack, J.W.; Keating, N.L. The role of families in decisions regarding cancer treatments. Cancer 2015, 121, 1079–1087. [Google Scholar] [CrossRef]
- LeBlanc, T.W.; Bloom, N.; Wolf, S.P.; Lowman, S.G.; Pollak, K.I.; Steinhauser, K.E.; Ariely, D.; Tulsky, J.A. Triadic treatment decision-making in advanced cancer: A pilot study of the roles and perceptions of patients, caregivers, and oncologists. Support. Care Cancer 2018, 26, 1197–1205. [Google Scholar] [CrossRef]
- Thorne, S.; Hislop, T.G.; Kim-Sing, C.; Oglov, V.; Oliffe, J.L.; Stajduhar, K.I. Changing communication needs and preferences across the cancer care trajectory: Insights from the patient perspective. Support. Care Cancer 2014, 22, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Brom, L.; Pasman, H.R.; Widdershoven, G.A.; Van Der Vorst, M.J.D.L.; Reijneveld, J.C.; Postma, T.J.; Onwuteaka-Philipsen, B.D. Patients’ preferences for participation in treatment decision-making at the end of life: Qualitative interviews with advanced cancer patients. PLoS ONE 2014, 9, e100435. [Google Scholar] [CrossRef]
- Yennurajalingam, S.; Rodrigues, L.F.; Shamieh, O.M.; Tricou, C.; Filbet, M.; Naing, K.; Ramaswamy, A.; Perez-Cruz, P.E.; Bautista, M.J.S.; Bunge, S.; et al. Decisional control preferences among patients with advanced cancer: An international multicenter cross-sectional survey. Palliat. Med. 2018, 32, 870–880. [Google Scholar] [CrossRef]
- Ozdemir, S.; Ng, S.; Chaudhry, I.; Malhotra, C.; Finkelstein, E.A. A prospective cohort study of decision-making role preferences of patients with advanced cancer and their family caregivers. Cancer 2023, 129, 1443–1452. [Google Scholar] [CrossRef] [PubMed]
- Maida, V.; Peck, J.; Ennis, M.; Brar, N.; Maida, A.R. Preferences for active and aggressive intervention among patients with advanced cancer. BMC Cancer 2010, 10, 592. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.N.; Chen, C.H.; Liu, T.W.; Lin, Y.C.; Lee, S.C.; Tang, S.T. Preferences for aggressive end-of-life care and their determinants among Taiwanese terminally ill cancer patients. Cancer Nurs. 2015, 38, E9–E18. [Google Scholar] [CrossRef]
- Yadav, S.; Turner, K.; Xie, Z.; Chen, G.; Islam, J.Y.; Suk, R.; Hong, Y.-R. Utilization of inpatient palliative care services among adolescents and young adults with cancer: Evidence from national inpatient sample 2016–2019. Palliat Support Care 2023, 1–8. [Google Scholar] [CrossRef]
- Tanco, K.; Rhondali, W.; Park, M.; Liu, D.; Bruera, E. Predictors of trust in the medical profession among cancer patients receiving palliative care: A preliminary study. J. Palliat. Med. 2016, 19, 991–994. [Google Scholar] [CrossRef]
- Grant, S.; Liao, K.; Miller, C.; Peterson, S.; Elting, L.; Guadagnolo, B.A. Lower levels of trust in the medical profession among white, younger, and more-educated individuals with cancer. Am. J. Clin. Oncol. 2021, 44, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, S.; Kazaz, S.N.; Semiz, H.S.; Yavuzşen, T.; Somalı, I.; Ellidokuz, H.; Öztop, I. An evaluation of the information sources of cancer patients’ relatives. a prospective survey. J. Cancer Educ. 2019, 34, 913–919. [Google Scholar] [CrossRef]
- Williams, J.S.; Fong-Gurzinsky, J.; Nagavally, S.; Walker, R.J.; Asan, O.; Ozieh, M.N.; Egede, L.E. Preferences in trust regarding the provision of cancer information among adults. J. Natl. Med. Assoc. 2021, 113, 457–464. [Google Scholar] [CrossRef]
- Chua, G.P.; Ng, Q.S.; Tan, H.K.; Ong, W.S. Caregivers of cancer patients: What are their information-seeking behaviours and resource preferences? Ecancermedicalscience 2020, 14, 1068. [Google Scholar] [CrossRef]
- Bazargan, M.; Cobb, S.; Assari, S. Discrimination and medical mistrust in a racially and ethnically diverse sample of california adults. Ann. Fam. Med. 2021, 19, 4–15. [Google Scholar] [CrossRef]
- Birkhauer, J.; Gaab, J.; Kossowsky, J.; Hasler, S.; Krummenacher, P.; Werner, C.; Gerger, H. Trust in the health care professional and health outcome: A meta-analysis. PLoS ONE 2017, 12, e0170988. [Google Scholar] [CrossRef]
- Yanez, B.; McGinty, H.L.; Buitrago, D.; Ramirez, A.G.; Penedo, F.J. Cancer outcomes in Hispanics/Latinos in the United States: An integrative review and conceptual model of determinants of health. J. Lat. Psychol. 2016, 4, 114–129. [Google Scholar] [CrossRef]
- Moreno, P.I.; Yanez, B.; Schuetz, S.J.; Wortman, K.; Gallo, L.C.; Benedict, C.; Brintz, C.E.; Cai, J.; Castaneda, S.F.; Perreira, K.M.; et al. Cancer fatalism and adherence to national cancer screening guidelines: Results from the Hispanic Community Health study/Study of Latinos (HCHS/SOL). Cancer Epidemiol. 2019, 60, 39–45. [Google Scholar] [CrossRef]
- Espinosa de Los Monteros, K.; Gallo, L.C. The relevance of fatalism in the study of Latinas’ cancer screening behavior: A systematic review of the literature. Int. J. Behav. Med. 2011, 18, 310–318. [Google Scholar] [CrossRef]
- Pérez-Stable, E.J.; Sabogal, F.; Otero-Sabogal, R.; Hiatt, R.A.; McPhee, S.J. Misconceptions about cancer among Latinos and Anglos. JAMA 1992, 268, 3219–3223. [Google Scholar] [CrossRef]
- Shen, M.J.; Gonzalez, C.; Leach, B.; Maciejewski, P.K.; Kozlov, E.; Prigerson, H.G. An examination of Latino advanced cancer patients’ and their informal caregivers’ preferences for communication about advance care planning: A qualitative study. Palliat. Support. Care 2020, 18, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Escobedo, L.E.; Cervantes, L.; Havranek, E. Barriers in healthcare for Latinx patients with limited english proficiency-a narrative review. J. Gen. Intern. Med. 2023, 38, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- National Alliance for Caregiving, AARP. 2020 Report Caregiving in the U.S. May 2020. Available online: https://www.caregiving.org/wp-content/uploads/2021/01/full-report-caregiving-in-the-united-states-01-21.pdf (accessed on 27 August 2023).
- Sagiv, L.; Schwartz, S.H. Personal values across cultures. Annu. Rev. Psychol. 2022, 73, 517–546. [Google Scholar] [CrossRef] [PubMed]
- Bechthold, A.C.; Montgomery, A.P.; Fazeli, P.L.; Dionne-Odom, J.N. Values elicitation among adults making health-related decisions: A concept analysis. Nurs. Forum 2022, 57, 885–892. [Google Scholar] [CrossRef]
- Moye, J.; Driver, J.A.; Owsiany, M.T.; Chen, L.Q.; Whitley, J.C.; Auguste, E.J.; Paik, J.M. Assessing what matters most in older adults with multicomplexity. Gerontologist 2022, 62, e224–e234. [Google Scholar] [CrossRef]
- Tatum, P.E.; Mills, S.S. Hospice and palliative care: An overview. Med. Clin. N. Am. 2020, 104, 359–373. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristic | Participated in Cancer Treatment Decision Making and Responded to ‘Deep Dive’ Questions, N = 1661 |
|---|---|
| n (%) | |
| Caregiver age | |
| 18–34 | 476 (28.7) |
| 35–54 | 839 (50.5) |
| 55 and older | 343 (20.7) |
| Missing 1 | 3 (0.2) |
| Caregiver gender | |
| Male | 793 (47.7) |
| Female | 851 (51.2) |
| Trans woman/man or gender non-conforming | 16 (1.0) |
| Missing 1 | 1 (0.1) |
| Caregiver race | |
| White | 1322 (79.6) |
| African American/Black | 183 (11.0) |
| Asian | 95 (5.7) |
| Alaskan Native, American Indian, Native Hawaiian, or Pacific Islander | 18 (1.1) |
| Missing 1 | 43 (2.6) |
| Hispanic/Latino | |
| Yes | 262 (15.8) |
| No | 1395 (84.0) |
| Missing 1 | 4 (0.2) |
| Caregiver education | |
| Postgraduate degree | 498 (30.0) |
| Some postgraduate | 109 (6.6) |
| College graduate (4 y) | 565 (34.0) |
| Vocational/Technical School (2 y) | 79 (4.8) |
| Some college | 250 (15.1) |
| High school graduate or less | 158 (9.5) |
| Missing 1 | 2 (0.1) |
| Caregiver employment status | |
| Working full time (>30 h per week) | 1153 (69.4) |
| Working part time (<30 h per week) | 217 (13.1) |
| Other (student, retired) | 171 (10.3) |
| Not employed | 89 (6.8) |
| Missing 1 | 7 (0.4) |
| Caregiver total household income | |
| ≥USD 75,000 | 1093 (65.8) |
| <USD 75,000 | 548 (33.0) |
| Missing 1 | 20 (1.2) |
| Location | |
| Urban | 1394 (83.9) |
| Rural or small town | 213 (12.8) |
| Missing 1 | 54 (3.3) |
| Caregiver-patient relationship | |
| Family member (sibling, child, parent, aunt/uncle, grandparent, cousin) | 1043 (62.8) |
| Friend | 405 (24.4) |
| Spouse/partner | 200 (12.0) |
| Missing 1 | 13 (0.8) |
| Length of time providing care | |
| Up to 1 year | 530 (31.9) |
| 1 to <3 years | 736 (44.3) |
| 3 to <5 years | 204 (12.3) |
| 5 or more years | 191 (11.5) |
| Patient’s cancer type | |
| Solid tumor cancers 2 | 1382 (83.2) |
| Breast | 363 (26.3) |
| Lung | 254 (18.4) |
| Prostate | 218 (15.8) |
| Colon/rectal | 111 (8.0) |
| Other | 436 (31.5) |
| Hematologic cancers 3 | 234 (14.1) |
| Missing 1 | 45 (2.7) |
| Patient’s cancer stage (solid tumor cancers) | |
| In remission | 48 (2.9) |
| 1–2 | 629 (37.9) |
| 3–4 | 720 (43.4) |
| Patient’s cancer stage (hematologic cancers) | |
| In remission | 26 (1.6) |
| 1–2 | 107 (6.4) |
| 3–4 | 91 (5.5) |
| Missing 1 (solid and hematologic) | 40 (2.4) |
| Patient’s insurance type | |
| Employer insurance | 791 (47.6) |
| Medicare | 436 (26.2) |
| Medicaid | 156 (9.4) |
| Marketplace exchange | 123 (7.4) |
| No insurance | 49 (3.0) |
| Missing 1 | 106 (6.4) |
| Patient’s living situation | |
| Living with caregiver | 597 (35.9) |
| Living apart from caregiver | 1046 (63.0) |
| Missing 1 | 18 (1.1) |
| Factors 1 | All Stages, N = 1661 | Early Stage, n = 736 | % 2 | Late Stage, n = 811 | % 2 | In Remission, n = 74 | % 2 | p-Value 3 |
|---|---|---|---|---|---|---|---|---|
| % | n (%) | n (%) | n (%) | |||||
| 69.2 | 526 (71.5) | +2.3 | 552 (68.1) | −1.1 | 45 (60.8) | −8.4 | 0.095 |
| 68.2 | 524 (71.2) | +3.0 | 546 (67.3) | −0.9 | 41 (55.4) | −12.8 | 0.012 * |
| 66.3 | 518 (70.4) | +4.1 | 522 (64.4) | −1.9 | 44 (59.5) | −6.8 | 0.016 * |
| 62.7 | 477 (64.8) | +2.1 | 496 (61.2) | −1.5 | 46 (62.2) | −0.5 | 0.330 |
| 58.8 | 468 (63.6) | +4.8 | 453 (55.9) | −2.9 | 42 (56.8) | −2.0 | 0.007 * |
| 49.6 | 382 (51.9) | +2.3 | 388 (47.8) | −1.8 | 34 (45.9) | −3.7 | 0.228 |
| 37.4 | 297 (40.4) | +3.0 | 293 (36.1) | −1.3 | 21 (28.4) | −9.0 | 0.055 |
| 36.1 | 269 (36.5) | +0.2 | 269 (33.2) | +1.0 | 17 (23.0) | −6.4 | 0.448 |
| 34.0 | 240 (32.6) | +2.5 | 280 (34.5) | −0.8 | 16 (21.6) | −11.0 | 0.042 |
| 32.8 | 267 (36.3) | −0.2 | 301 (37.1) | +1.7 | 22 (29.7) | −11.2 | 0.073 |
| 32.5 | 253 (34.4) | +1.9 | 261 (32.2) | −0.3 | 16 (21.6) | −10.9 | 0.076 |
| 30.5 | 219 (29.8) | +4.1 | 234 (28.9) | −2.6 | 21 (28.4) | −7.5 | 0.005 * |
| 29.0 | 255 (34.6) | +0.8 | 226 (27.9) | −0.1 | 17 (23.0) | −0.6 | 0.914 |
| 27.8 | 225 (30.6) | +2.8 | 219 (27.0) | −0.8 | 12 (16.2) | −11.6 | 0.020 * |
| 23.5 | 178 (24.2) | +0.7 | 189 (23.3) | −0.2 | 17 (23.0) | −0.5 | 0.911 |
| Characteristic | Quality of Life | Physical Well-Being | Length of Life | Emotional Well-Being | Opinions/Feelings of Oncology Team | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | p-Value 1 | n (%) | p-Value 1 | n (%) | p-Value 1 | n (%) | p-Value 1 | n (%) | p-Value 1 | |
| Caregiver age | ||||||||||
| 18–34 (n = 476) | 296 (62.2) | <0.001 * | 289 (60.7) | <0.001 * | 295 (62.0) | 0.027 | 276 (58.0) | <0.001 * | 236 (49.6) | <0.001 * |
| 35–54 (n = 839) | 583 (69.5) | 573 (68.3) | 580 (69.1) | 520 (62.0) | 502 (59.8) | |||||
| 55 and older (n = 343) | 269 (78.4) | 268 (78.1) | 223 (65.0) | 242 (70.6) | 236 (68.8) | |||||
| Caregiver gender | ||||||||||
| Male (n = 793) | 530 (66.8) | 0.055 | 526 (66.3) | 0.134 | 509 (64.2) | 0.069 | 474 (59.8) | 0.051 | 453 (57.1) | 0.006 * |
| Female (n = 851) | 610 (71.7) | 598 (70.3) | 583 (68.5) | 557 (65.5) | 520 (61.1) | |||||
| Other, trans woman/man or gender non-conforming (n = 16) | 9 (56.3) | 9 (56.3) | 8 (50.0) | 9 (56.3) | 4 (25.0) | |||||
| Caregiver race | ||||||||||
| White (n = 1322) | 923 (69.8) | 0.040 | 915 (69.2) | 0.052 | 884 (66.9) | 0.109 | 827 (62.6) | 0.503 | 802 (60.7) | 0.009 * |
| African American/Black (n = 183) | 130 (71.0) | 122 (66.7) | 125 (68.3) | 118 (64.5) | 102 (55.7) | |||||
| Asian (n = 95) | 56 (58.9) | 58 (61.1) | 57 (60.0) | 55 (57.9) | 44 (46.3) | |||||
| Other, Alaskan Native, American Indian, Native Hawaiian, or Pacific Islander (n = 18) | 9 (50.0) | 8 (44.4) | 8 (44.4) | 9 (50.0) | 7 (38.9) | |||||
| Caregiver ethnicity | ||||||||||
| Hispanic/Latino (n = 262) | 166 (63.4) | 0.024 | 159 (60.7) | 0.004 * | 145 (55.3) | <0.001 * | 150 (57.3) | 0.042 | 128 (48.9) | <0.001 * |
| Non-Hispanic/Latino (n = 1395) | 982 (70.4) | 973 (69.7) | 954 (68.4) | 891 (63.9) | 848 (60.8) | |||||
| Employment | ||||||||||
| Full-time (n = 1153) | 789 (68.4) | 0.140 | 784 (68.0) | 0.613 | 775 (67.2) | 0.135 | 721 (62.5) | 0.074 | 676 (58.6) | 0.838 |
| Part-time (n = 217) | 147 (67.7) | 144 (66.4) | 145 (66.8) | 136 (62.7) | 124 (57.1) | |||||
| Unemployed (n = 113) | 89 (78.8) | 83 (73.5) | 77 (68.1) | 82 (72.6) | 70 (61.9) | |||||
| Other, retired, student, or prefer not to say (n = 178) | 125 (70.2) | 122 (68.5) | 104 (58.4) | 102 (57.3) | 107 (60.1) | |||||
| Caregiver total household income | ||||||||||
| ≥USD 75,000 (n = 1093) | 770 (70.4) | 0.254 | 746 (68.3) | 0.823 | 738 (67.5) | 0.237 | 677 (61.9) | 0.180 | 649 (59.4) | 0.651 |
| <USD 75,000 (n = 548) | 371 (67.7) | 377 (68.8) | 354 (64.6) | 358 (65.3) | 319 (58.2) | |||||
| Caregiver-patient relationship (The patient is the caregiver’s…) | ||||||||||
| Spouse/partner (n = 200) | 139 (69.5) | 0.845 | 137 (68.5) | 0.763 | 136 (68.0) | 0.423 | 127 (63.5) | 0.980 | 121 (60.5) | 0.687 |
| Family (n = 1043) | 727 (69.7) | 716 (68.6) | 699 (67.0) | 655 (62.8) | 605 (58.0) | |||||
| Friend (n = 405) | 276 (68.1) | 270 (66.7) | 258 (63.7) | 254 (62.7) | 243 (60.0) | |||||
| Location | ||||||||||
| Rural or small town (n = 213) | 157 (73.7) | 0.171 | 151 (70.9) | 0.387 | 137 (64.3) | 0.452 | 128 (60.1) | 0.319 | 130 (61.0) | 0.516 |
| Urban (n = 1394) | 963 (69.1) | 947 (67.9) | 933 (66.9) | 887 (63.6) | 818 (58.7) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bechthold, A.C.; Azuero, A.; Puga, F.; Ejem, D.B.; Kent, E.E.; Ornstein, K.A.; Ladores, S.L.; Wilson, C.M.; Knoepke, C.E.; Miller-Sonet, E.; et al. What Is Most Important to Family Caregivers When Helping Patients Make Treatment-Related Decisions: Findings from a National Survey. Cancers 2023, 15, 4792. https://doi.org/10.3390/cancers15194792
Bechthold AC, Azuero A, Puga F, Ejem DB, Kent EE, Ornstein KA, Ladores SL, Wilson CM, Knoepke CE, Miller-Sonet E, et al. What Is Most Important to Family Caregivers When Helping Patients Make Treatment-Related Decisions: Findings from a National Survey. Cancers. 2023; 15(19):4792. https://doi.org/10.3390/cancers15194792
Chicago/Turabian StyleBechthold, Avery C., Andres Azuero, Frank Puga, Deborah B. Ejem, Erin E. Kent, Katherine A. Ornstein, Sigrid L. Ladores, Christina M. Wilson, Christopher E. Knoepke, Ellen Miller-Sonet, and et al. 2023. "What Is Most Important to Family Caregivers When Helping Patients Make Treatment-Related Decisions: Findings from a National Survey" Cancers 15, no. 19: 4792. https://doi.org/10.3390/cancers15194792
APA StyleBechthold, A. C., Azuero, A., Puga, F., Ejem, D. B., Kent, E. E., Ornstein, K. A., Ladores, S. L., Wilson, C. M., Knoepke, C. E., Miller-Sonet, E., & Odom, J. N. (2023). What Is Most Important to Family Caregivers When Helping Patients Make Treatment-Related Decisions: Findings from a National Survey. Cancers, 15(19), 4792. https://doi.org/10.3390/cancers15194792