
MAGE-A10 Protein Expression in Advanced High Grade Serous Ovarian Cancer Is Associated with Resistance to First-Line Platinum-Based Chemotherapy

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Chemotherapy Treatment
2.3. Immunohistochemical Staining
2.4. Statistical Analysis
3. Results
3.1. Demographics and Clinical-Pathological Characteristics
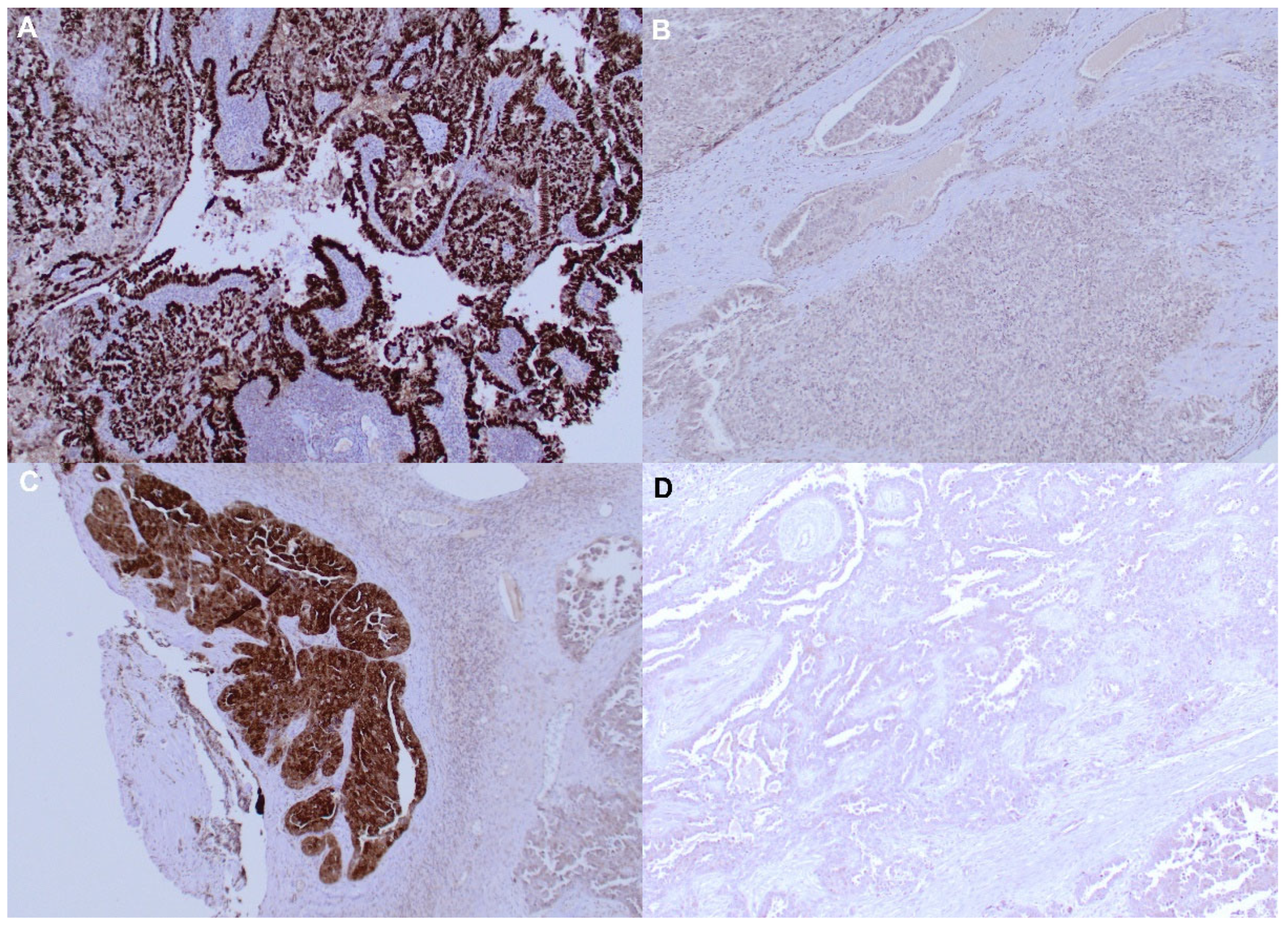
3.2. Immunohistochemistry
3.3. Response to Chemotherapy
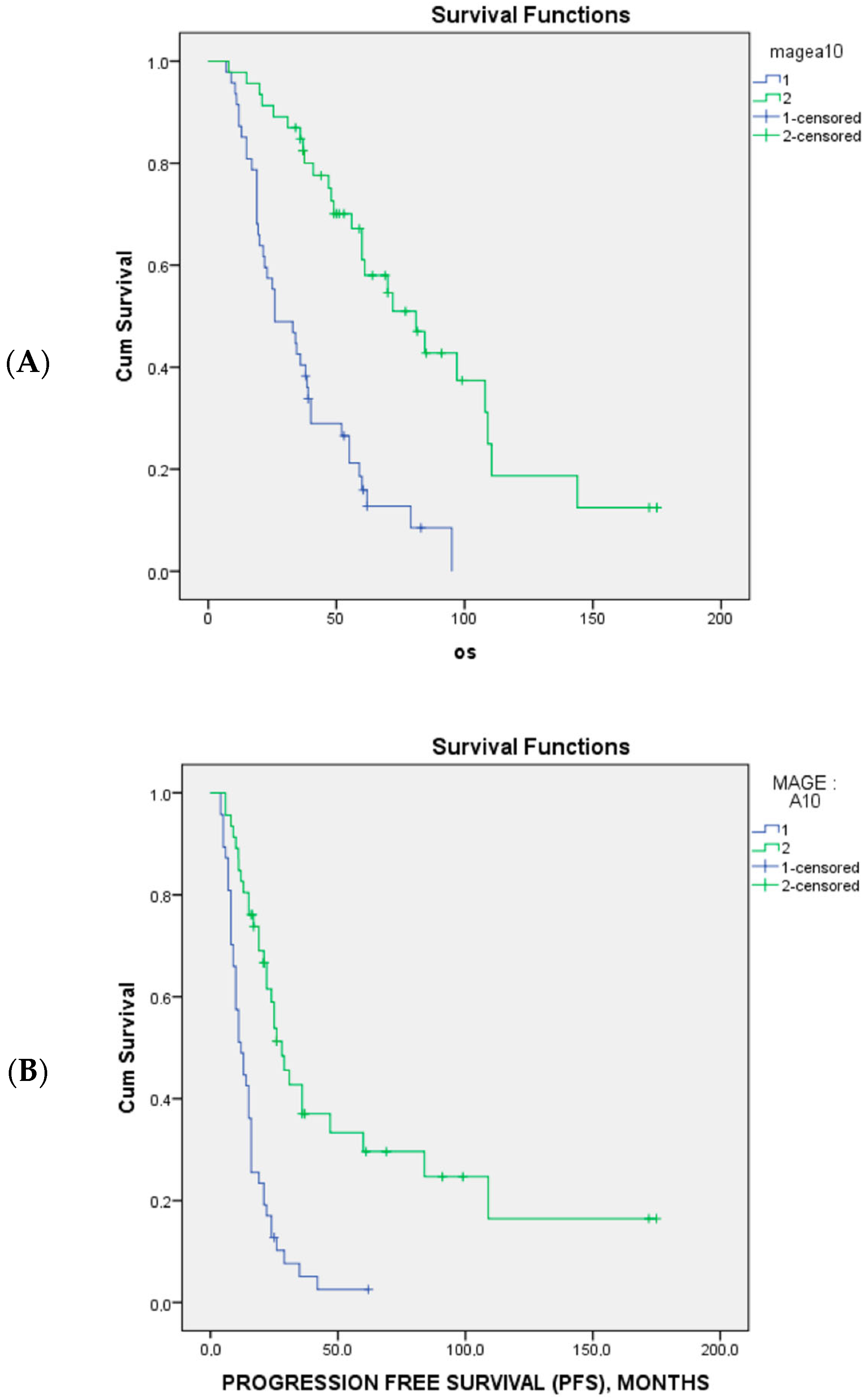
3.4. Correlation between CTA Expression and Response to Chemotherapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- SEER Cancer Statistics Factsheets: Ovary Cancer. National Cancer Institute: Bethesda, MD, USA. Available online: http://seer.cancer.gov/statfacts/html/ovary.html (accessed on 10 March 2023).
- Wilson, M.K.; Pujade-Lauraine, E.; Aoki, D.; Mirza, M.R.; Lorusso, D.; Oza, A.M.; du Bois, A.; Vergote, I.; Reuss, A.; Bacon, M.; et al. Fifth Ovarian Cancer Consensus Conference of the Gynecologic Cancer InterGroup: Recurrent disease. Ann. Oncol. 2017, 28, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Kang, Y.; Chen, L.; Wang, H.; Liu, J.; Zeng, S.; Yu, L. The Drug-Resistance Mechanisms of Five Platinum-Based Antitumor Agents. Front. Pharmacol. 2020, 11, 343. [Google Scholar] [CrossRef]
- Miše, B.P.; Telesmanić, V.D.; Tomić, S.; Šundov, D.; Čapkun, V.; Vrdoljak, E. Correlation Between E-cadherin Immunoexpression and Efficacy of First Line Platinum-Based Chemotherapy in Advanced High Grade Serous Ovarian Cancer. Pathol. Oncol. Res. 2015, 21, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Pawłowska, A.; Rekowska, A.; Kuryło, W.; Pańczyszyn, A.; Kotarski, J.; Wertel, I. Current Understanding on Why Ovarian Cancer Is Resistant to Immune Checkpoint Inhibitors. Int. J. Mol. Sci. 2023, 24, 10859. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.-L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421, Erratum in Nature 2013, 502, 258. [Google Scholar] [CrossRef]
- Juretic, A.; Jürgens-Göbel, J.; Schaefer, C.; Noppen, C.; Willimann, T.E.; Kocher, T.; Zuber, M.; Harder, F.; Heberer, M.; Spagnoli, G.C. Cytotoxic T-lymphocyte responses against mutated p21 ras peptides: An analysis of specific T-cell-receptor gene usage. Int. J. Cancer 1996, 68, 471–478. [Google Scholar] [CrossRef]
- Domínguez-Prieto, V.; Qian, S.; Villarejo-Campos, P.; Meliga, C.; González-Soares, S.; Guijo Castellano, I.; Jiménez-Galanes, S.; García-Arranz, M.; Guadalajara, H.; García-Olmo, D. Understanding CAR T cell therapy and its role in ovarian cancer and peritoneal carcinomatosis from ovarian cancer. Front. Oncol. 2023, 13, 1104547. [Google Scholar] [CrossRef]
- Simpson, A.J.; Caballero, O.L.; Jungbluth, A.; Chen, Y.T.; Old, L.J. Cancer/testis antigens, gametogenesis and cancer. Nat. Rev. Cancer 2005, 5, 615–625. [Google Scholar] [CrossRef]
- Juretic, A.; Spagnoli, G.C.; Schultz-Thater, E.; Sarcevic, B. Cancer/testis tumour-associated antigens: Immunohistochemical detection with monoclonal antibodies. Lancet Oncol. 2003, 4, 104–109. [Google Scholar] [CrossRef]
- Poojary, M.; Jishnu, P.V.; Kabekkodu, S.P. Prognostic Value of Melanoma-Associated Antigen-A (MAGE-A) Gene Expression in Various Human Cancers: A Systematic Review and Meta-analysis of 7428 Patients and 44 Studies. Mol. Diagn. Ther. 2020, 24, 537–555. [Google Scholar] [CrossRef]
- Zhao, J.; Xu, Z.; Liu, Y.; Wang, X.; Liu, X.; Gao, Y.; Jin, Y. The expression of cancer-testis antigen in ovarian cancer and the development of immunotherapy. Am. J. Cancer Res. 2022, 12, 681–694. [Google Scholar] [PubMed]
- Daudi, S.; Eng, K.H.; Mhawech-Fauceglia, P.; Morrison, C.; Miliotto, A.; Beck, A.; Matsuzaki, J.; Tsuji, T.; Groman, A.; Gnjatic, S.; et al. Expression and immune responses to MAGE antigens predict survival in epithelial ovarian cancer. PLoS ONE 2014, 9, e104099. [Google Scholar] [CrossRef] [PubMed]
- Dutoit, V.; Rubio-Godoy, V.; Dietrich, P.Y.; Quiqueres, A.L.; Schnuriger, V.; Rimoldi, D.; Liénard, D.; Speiser, D.; Guillaume, P.; Batard, P.; et al. Heterogeneous T-cell response to MAGE-A10(254-262): High avidity-specific cytolytic T lymphocytes show superior antitumor activity. Cancer Res. 2001, 61, 5850–5856. [Google Scholar] [PubMed]
- Groeper, C.; Gambazzi, F.; Zajac, P.; Bubendorf, L.; Adamina, M.; Rosenthal, R.; Zerkowski, H.R.; Heberer, M.; Spagnoli, G.C. Cancer/testis antigen expression and specific cytotoxic T lymphocyte responses in non small cell lung cancer. Int. J. Cancer 2007, 120, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Al-Khadairi, G.; Roelands, J.; Hendrickx, W.; Dermime, S.; Bedognetti, D.; Decock, J. NY-ESO-1 Based Immunotherapy of Cancer: Current Perspectives. Front. Immunol. 2018, 9, 947. [Google Scholar] [CrossRef]
- Odunsi, K. Immunotherapy in ovarian cancer. Ann. Oncol. 2017, 28 (Suppl. 8), viii1–viii7. [Google Scholar] [CrossRef]
- Prat, J.; FIGO Committee on Gynecologic Oncology. Staging Classification for Cancer of the Ovary, Fallopian Tube, and Peritoneum: Abridged Republication of Guidelines from the International Federation of Gynecology and Obstetrics (FIGO). Obstet. Gynecol. 2015, 126, 171–174. [Google Scholar] [CrossRef]
- Malpica, A.; Deavers, M.T.; Lu, K.; Bodurka, D.C.; Atkinson, E.N.; Gershenson, D.M.; Silva, E.G. Grading ovarian serous carcinoma using a two-tier system. Am. J. Surg. Pathol. 2004, 28, 496–504. [Google Scholar] [CrossRef]
- Wimberger, P.; Wehling, M.; Lehmann, N.; Kimmig, R.; Schmalfeldt, B.; Burges, A.; Harter, P.; Pfisterer, J.; du Bois, A. Influence of residual tumor on outcome in ovarian cancer patients with FIGO stage IV disease: An exploratory analysis of the AGO-OVAR (ArbeitsgemeinschaftGynaekologischeOnkologie Ovarian Cancer Study Group). Ann. Surg. Oncol. 2010, 17, 1642–1648. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Friedlander, M.; Trimble, E.; Tinker, A.; Alberts, D.; Avall-Lundqvist, E.; Brady, M.; Harter, P.; Pignata, S.; Pujade-Lauraine, E.; Sehouli, J.; et al. Clinical trials in recurrent ovarian cancer. Int. J. Gynecol. Cancer 2011, 21, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Mrklić, I.; Spagnoli, G.C.; Juretić, A.; Pogorelić, Z.; Tomić, S. Co-expression of cancer testis antigens and topoisomerase 2-alpha in triple negative breast carcinomas. Acta Histochem. 2014, 116, 740–746. [Google Scholar] [CrossRef]
- Schultz-Thater, E.; Piscuoglio, S.; Iezzi, G.; Le Magnen, C.; Zajac, P.; Carafa, V.; Terracciano, L.; Tornillo, L.; Spagnoli, G.C. MAGE-A10 is a nuclear protein frequently expressed in high percentages of tumor cells in lung, skin and urothelial malignancies. Int. J. Cancer 2011, 129, 1137–1148. [Google Scholar] [CrossRef] [PubMed]
- Schultz-Thater, E.; Noppen, C.; Gudat, F.; Dürmüller, U.; Zajac, P.; Kocher, T.; Heberer, M.; Spagnoli, G.C. NY-ESO-1 tumour associated antigen is a cytoplasmic protein detectable by specific monoclonal antibodies in cell lines and clinical specimens. Br. J. Cancer 2000, 83, 204–208. [Google Scholar] [CrossRef]
- Agarwal, R.; Kaye, S.B. Ovarian cancer: Strategies for overcoming resistance to chemotherapy. Nat. Rev. Cancer 2003, 3, 502–516. [Google Scholar] [CrossRef]
- Shen, D.W.; Pouliot, L.M.; Hall, M.D.; Gottesman, M.M. Cisplatin resistance: A cellular self-defense mechanism resulting from multiple epigenetic and genetic changes. Pharmacol. Rev. 2012, 64, 706–721. [Google Scholar] [CrossRef]
- Leung, D.; Price, Z.K.; Lokman, N.A.; Wang, W.; Goonetilleke, L.; Kadife, E.; Oehler, M.K.; Ricciardelli, C.; Kannourakis, G.; Ahmed, N. Platinum-resistance in epithelial ovarian cancer: An interplay of epithelial-mesenchymal transition interlinked with reprogrammed metabolism. J. Transl. Med. 2022, 20, 556. [Google Scholar] [CrossRef]
- Tiwari, N.; Gheldof, A.; Tatari, M.; Christofori, G. EMT as the ultimate survival mechanism of cancer cells. In Semin Cancer biology; Academic Press: Cambridge, MA, USA, 2012; Volume 22, pp. 194–207. [Google Scholar] [CrossRef]
- Li, X.F.; Ren, P.; Shen, W.Z.; Jin, X.; Zhang, J. The expression, modulation and use of cancer-testis antigens as potential biomarkers for cancer immunotherapy. Am. J. Transl. Res. 2020, 12, 7002–7019. [Google Scholar]
- Kasuga, C.; Nakahara, Y.; Ueda, S.; Hawkins, C.; Taylor, M.D.; Smith, C.A.; Rutka, J.T. Expression of MAGE and GAGE genes in medulloblastoma and modulation of resistance to chemotherapy. Laboratory investigation. J. Neurosurg. Pediatr. 2008, 1, 305–313. [Google Scholar] [CrossRef]
- Weeraratne, S.D.; Amani, V.; Neiss, A.; Teider, N.; Scott, D.K.; Pomeroy, S.L.; Cho, Y.J. miR-34a confers chemosensitivity through modulation of MAGE-A and p53 in medulloblastoma. Neuro-Oncology 2011, 13, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, S.; Kriegebaum, U.; Küchler, N.; Brands, R.C.; Linz, C.; Kübler, A.C.; Müller-Richter, U.D. Correlation of MAGE-A tumor antigens and the efficacy of various chemotherapeutic agents in head and neck carcinoma cells. Clin. Oral Investig. 2014, 18, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, S.; Zwick, L.; Scheurer, M.J.J.; Fuchs, A.R.; Brands, R.C.; Seher, A.; Böhm, H.; Kübler, A.C.; Müller-Richter, U.D.A. MAGE-A11 expression contributes to cisplatin resistance in head and neck cancer. Clin. Oral Investig. 2018, 22, 1477–1486. [Google Scholar] [CrossRef] [PubMed]
- Duan, Z.; Duan, Y.; Lamendola, D.E.; Yusuf, R.Z.; Naeem, R.; Penson, R.T.; Seiden, M.V. Overexpression of MAGE/GAGE genes in paclitaxel/doxorubicin-resistant human cancer cell lines. Clin. Cancer Res. 2003, 9, 2778–2785. [Google Scholar]
- Marcar, L.; Maclaine, N.J.; Hupp, T.R.; Meek, D.W. Mage-A cancer/testis antigens inhibit p53 function by blocking its interaction with chromatin. Cancer Res. 2010, 70, 10362–10370. [Google Scholar] [CrossRef]
- Nardiello, T.; Jungbluth, A.A.; Mei, A.; Diliberto, M.; Huang, X.; Dabrowski, A.; Andrade, V.C.; Wasserstrum, R.; Ely, S.; Niesvizky, R.; et al. MAGE-A inhibits apoptosis in proliferating myeloma cells through repression of Bax and maintenance of survivin. Clin. Cancer Res. 2011, 17, 4309–4319. [Google Scholar] [CrossRef]
- Sigalotti, L.; Fratta, E.; Coral, S.; Tanzarella, S.; Danielli, R.; Colizzi, F.; Fonsatti, E.; Traversari, C.; Altomonte, M.; Maio, M. Intratumor heterogeneity of cancer/testis antigens expression in human cutaneous melanoma is methylation-regulated and functionally reverted by 5-aza-2′-deoxycytidine. Cancer Res. 2004, 64, 9167–9171. [Google Scholar] [CrossRef]
- Yakirevich, E.; Sabo, E.; Lavie, O.; Mazareb, S.; Spagnoli, G.C.; Resnick, M.B. Expression of the MAGE-A4 and NY-ESO-1 cancer-testis antigens in serous ovarian neoplasms. Clin. Cancer Res. 2003, 9, 6453–6460. [Google Scholar]
- Xu, Y.; Wang, C.; Zhang, Y.; Jia, L.; Huang, J. Overexpression of MAGE-A9 Is Predictive of Poor Prognosis in Epithelial Ovarian Cancer. Sci. Rep. 2015, 5, 12104. [Google Scholar] [CrossRef]
- Szender, J.B.; Papanicolau-Sengos, A.; Eng, K.H.; Miliotto, A.J.; Lugade, A.A.; Gnjatic, S.; Matsuzaki, J.; Morrison, C.D.; Odunsi, K. NY-ESO-1 expression predicts an aggressive phenotype of ovarian cancer. Gynecol. Oncol. 2017, 145, 420–425. [Google Scholar] [CrossRef]
- Matak, L.; Mikuš, M.; Ćorić, M.; Spagnol, G.; Matak, M.; Vujić, G. Comparison end-to-end anastomosis with ostomy after secondary surgical cytoreduction for recurrent high-grade serous ovarian cancer: Observational single-center study. Arch. Gynecol. Obstet. 2023, 308, 231–237. [Google Scholar] [CrossRef]
- Alsalloum, A.; Shevchenko, J.A.; Sennikov, S. The Melanoma-Associated Antigen Family A (MAGE-A): A Promising Target for Cancer Immunotherapy? Cancers 2023, 15, 1779. [Google Scholar] [CrossRef]
- Dovey, S.L.; Valli, H.; Hermann, B.P.; Sukhwani, M.; Donohue, J.; Castro, C.A.; Chu, T.; Sanfilippo, J.S.; Orwig, K.E. Eliminating malignant contamination from therapeutic human spermatogonial stem cells. J. Clin. Investig. 2013, 123, 1833–1843. [Google Scholar] [CrossRef] [PubMed]
- De Plaen, E.; Arden, K.; Traversari, C.; Gaforio, J.J.; Szikora, J.P.; De Smet, C.; Brasseur, F.; van der Bruggen, P.; Lethé, B.; Lurquin, C.; et al. Structure, chromosomal localization, and expression of 12 genes of the MAGE family. Immunogenetics 1994, 40, 360–369. [Google Scholar] [CrossRef]
- Jungbluth, A.A.; Silva WAJr Iversen, K.; Frosina, D.; Zaidi, B.; Coplan, K.; Eastlake-Wade, S.K.; Castelli, S.B.; Spagnoli, G.C.; Old, L.J.; Vogel, M. Expression of cancer-testis (CT) antigens in placenta. Cancer Immun. 2007, 7, 15. [Google Scholar]
- Marchand, M.; van Baren, N.; Weynants, P.; Brichard, V.; Dréno, B.; Tessier, M.H.; Rankin, E.; Parmiani, G.; Arienti, F.; Humblet, Y.; et al. Tumor regressions observed in patients with metastatic melanoma treated with an antigenic peptide encoded by gene MAGE-3 and presented by HLA-A1. Int. J. Cancer 1999, 80, 219–230. [Google Scholar] [CrossRef]
- Marchand, M.; Punt, C.J.; Aamdal, S.; Escudier, B.; Kruit, W.H.; Keilholz, U.; Håkansson, L.; van Baren, N.; Humblet, Y.; Mulders, P.; et al. Immunisation of metastatic cancer patients with MAGE-3 protein combined with adjuvant SBAS-2: A clinical report. Eur. J. Cancer 2003, 39, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Van Baren, N.; Bonnet, M.C.; Dréno, B.; Khammari, A.; Dorval, T.; Piperno-Neumann, S.; Liénard, D.; Speiser, D.; Marchand, M.; Brichard, V.G.; et al. Tumoral and immunologic response after vaccination of melanoma patients with an ALVAC virus encoding MAGE antigens recognized by T cells. J. Clin. Oncol. 2005, 23, 9008–9021. [Google Scholar] [CrossRef]
- Patel, S.P.; Petroni, G.R.; Roszik, J.; Olson, W.C.; Wages, N.A.; Chianese-Bullock, K.A.; Smolkin, M.; Varhegyi, N.; Gaughan, E.; Smith, K.T.; et al. Phase I/II trial of a long peptide vaccine (LPV7) plus toll-like receptor (TLR) agonists with or without incomplete Freund’s adjuvant (IFA) for resected high-risk melanoma. J. Immunother. Cancer 2021, 9, e003220. [Google Scholar] [CrossRef]
- Morgan, R.A.; Chinnasamy, N.; Abate-Daga, D.; Gros, A.; Robbins, P.F.; Zheng, Z.; Feldman, S.A.; Yang, J.C.; Sherry, R.M.; Phan, G.Q.; et al. Cancer regression and neurological toxicity following anti-MAGE-A3 TCR gene therapy. J. Immunother. 2013, 36, 133–151. [Google Scholar] [CrossRef]
- Martin, A.D.; Wang, X.; Sandberg, M.L.; Negri, K.R.; Wu, M.L.; Toledo Warshaviak, D.; Gabrelow, G.B.; McElvain, M.E.; Lee, B.; Daris, M.E.; et al. Re-examination of MAGE-A3 as a T-cell Therapeutic Target. J. Immunother. 2021, 44, 95–105. [Google Scholar] [CrossRef]
- Hong, D.S.; Van Tine, B.A.; Biswas, S.; McAlpine, C.; Johnson, M.L.; Olszanski, A.J.; Clarke, J.M.; Araujo, D.; Blumenschein, G.R., Jr.; Kebriaei, P.; et al. Autologous T cell therapy for MAGE-A4+ solid cancers in HLA-A*02+ patients: A phase 1 trial. Nat Med. 2023, 29, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Tayar, J.; Fu, S.; Ke, D.; Norry, E.; Sun, A.; Miller, J.; Hong, D.S. Newly developed pseudogout arthritis after therapy with MAGE-A4 directed TCR T cells responded to treatment with tocilizumab. J. Immunother. Cancer 2021, 9, e002716. [Google Scholar] [CrossRef]
- Lu, Y.C.; Parker, L.L.; Lu, T.; Zheng, Z.; Toomey, M.A.; White, D.E.; Yao, X.; Li, Y.F.; Robbins, P.F.; Feldman, S.A.; et al. Treatment of Patients With Metastatic Cancer Using a Major Histocompatibility Complex Class II-Restricted T-Cell Receptor Targeting the Cancer Germline Antigen MAGE-A3. J. Clin. Oncol. 2017, 35, 3322–3329. [Google Scholar] [CrossRef] [PubMed]
- Davis, I.D.; Chen, Q.; Morris, L.; Quirk, J.; Stanley, M.; Tavarnesi, M.L.; Parente, P.; Cavicchiolo, T.; Hopkins, W.; Jackson, H.; et al. Blood dendritic cells generated with Flt3 ligand and CD40 ligand prime CD8+ T cells efficiently in cancer patients. J. Immunother. 2006, 29, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Blumenschein, G.R.; Devarakonda, S.; Johnson, M.; Moreno, V.; Gainor, J.; Edelman, M.J.; Heymach, J.V.; Govindan, R.; Bachier, C.; de Spéville, B.D.; et al. Phase I clinical trial evaluating the safety and efficacy of ADP-A2M10 SPEAR T cells in patients with MAGE-A10+ advanced non-small cell lung cancer. J. Immunother. Cancer 2022, 10, e003581. [Google Scholar] [CrossRef] [PubMed]
- van Baal, J.O.A.M.; van Noorden, C.J.F.; Nieuwland, R.; Van de Vijver, K.K.; Sturk, A.; van Driel, W.J.; Kenter, G.G.; Lok, C.A.R. Development of Peritoneal Carcinomatosis in Epithelial Ovarian Cancer: A Review. J. Histochem. Cytochem. 2018, 66, 67–83. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Disease Status at the End of Follow-Up | |||||
|---|---|---|---|---|---|
| Total | Dead | Alive | Alive | ||
| (N = 93) | (N = 67) | with Recurrence (N = 9) | without Recurrence (N = 17) | ||
| Age (median, IQR) | 57(37–79) | 59(37–79) | 62(49–75) | 54(44–76) | |
| PFS (median, IQR) | 16(4–175) | 14(4–109) | 22(8–42) | 37(16–175) | |
| OS (median, IQR) | 40(7–175) | 36(7–144) | 44(34–83) | 69(37–175) | |
| FIGO stage (N, %) | III | 72(77) | 50(75) | 6 | 16(94) |
| IV | 21(23) | 17(25) | 3 | 1(6) | |
| Surgery (N, %) | Optimal | 14(15) | 0 | 4 | 10(15) |
| Suboptimal | 75(81) | 9 | 12 | 54(80) | |
| Unknown | 4(4) | 0 | 1 | 3(4) | |
| Chemotherapy cycles (N, %) | 6 | 60(64) | 5 | 16 | 39(58) |
| >6 | 33(36) | 4 | 1 | 28(42) | |
| Response to chemotherapy (N, %) | CR | 62(66,7) | 40(59,7) | 6 | 16 |
| PR | 11(11,8) | 8(11,9) | 2 | 1 | |
| SD | 5(5,4) | 5(7,5) | 0 | 0 | |
| PD | 15(16,1) | 14(20,9) | 1 | 0 | |
| N (%) | |||||
|---|---|---|---|---|---|
| Response to Chemotherapy | |||||
| CR + PR = OR | SD + PD | χ² | p | ||
| MAGE A-10 | Positive | 30(41) | 17(85) | 10.4 | 0.001 |
| Negative | 43(59) | 3(15) | |||
| NY-ESO-1 | Positive | 25(34) | 8(40) | 0.045 | 0.832 |
| Negative | 48(66) | 12(60) | |||
| Chemotherapy sensitivity | Sensitive | 58(80) | 0 | 39 | <0.001 |
| Resistant | 15(20) | 20(100) | |||
| HR (95%CI) | p | |
|---|---|---|
| Age | 4.2 (1.2–14.6) | 0.025 |
| Stage | 5.7 (1.6–21) | 0.007 |
| MAGE A10 | 7.4 (1.8–29.8) | 0.005 |
| HR (CI 95%) | p | |
|---|---|---|
| Stage | 3.1 (1.0–9.9) | 0.050 |
| MAGE A10 | 6 (2.2–16.4) | <0.001 |
| Chemotherapy cycles | 1.8 (0.65–4.8) | 0.265 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lisica Šikić, N.; Petrić Miše, B.; Tomić, S.; Spagnol, G.; Matak, L.; Juretić, A.; Spagnoli, G. MAGE-A10 Protein Expression in Advanced High Grade Serous Ovarian Cancer Is Associated with Resistance to First-Line Platinum-Based Chemotherapy. Cancers 2023, 15, 4697. https://doi.org/10.3390/cancers15194697
Lisica Šikić N, Petrić Miše B, Tomić S, Spagnol G, Matak L, Juretić A, Spagnoli G. MAGE-A10 Protein Expression in Advanced High Grade Serous Ovarian Cancer Is Associated with Resistance to First-Line Platinum-Based Chemotherapy. Cancers. 2023; 15(19):4697. https://doi.org/10.3390/cancers15194697
Chicago/Turabian StyleLisica Šikić, Nataša, Branka Petrić Miše, Snježana Tomić, Giulia Spagnol, Luka Matak, Antonio Juretić, and Giulio Spagnoli. 2023. "MAGE-A10 Protein Expression in Advanced High Grade Serous Ovarian Cancer Is Associated with Resistance to First-Line Platinum-Based Chemotherapy" Cancers 15, no. 19: 4697. https://doi.org/10.3390/cancers15194697
APA StyleLisica Šikić, N., Petrić Miše, B., Tomić, S., Spagnol, G., Matak, L., Juretić, A., & Spagnoli, G. (2023). MAGE-A10 Protein Expression in Advanced High Grade Serous Ovarian Cancer Is Associated with Resistance to First-Line Platinum-Based Chemotherapy. Cancers, 15(19), 4697. https://doi.org/10.3390/cancers15194697