
Management of Metastatic Pancreatic Cancer—Comparison of Global Guidelines over the Last 5 Years

 , , ,
, , ,  , ,
, ,  , , , , ,
, , , , ,  and add
Show full author list
and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
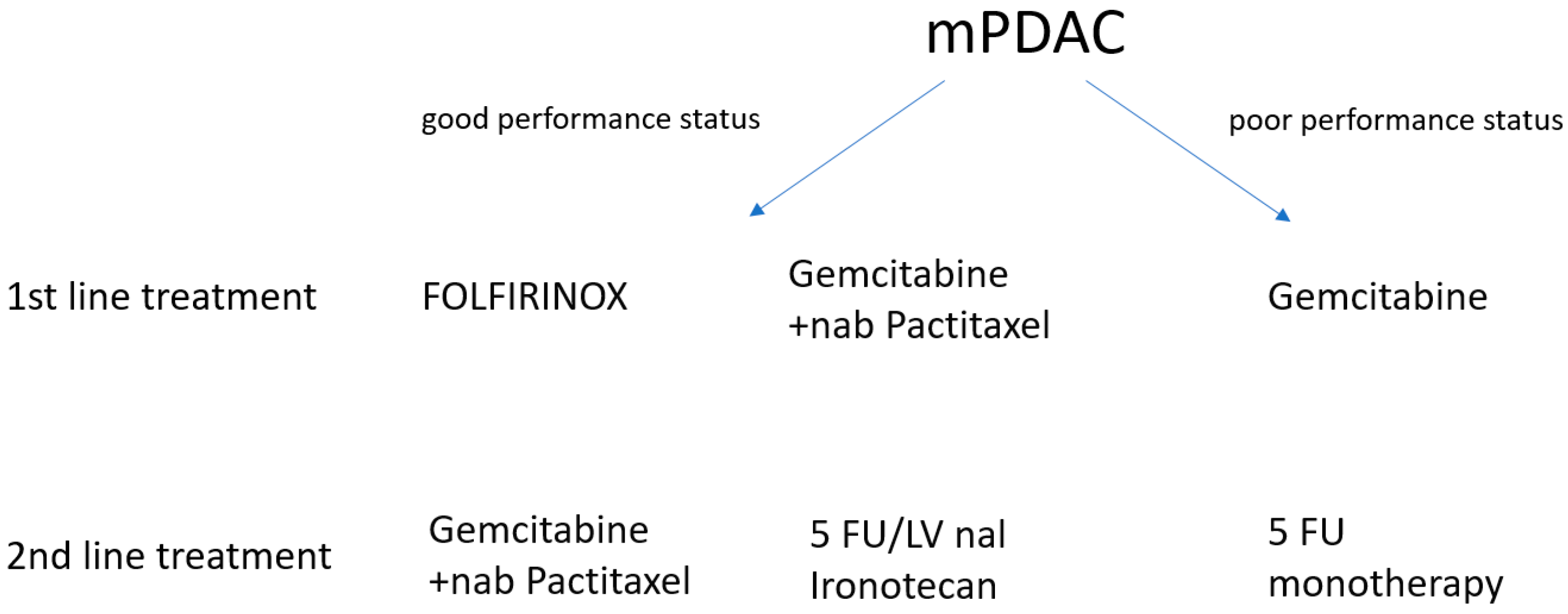
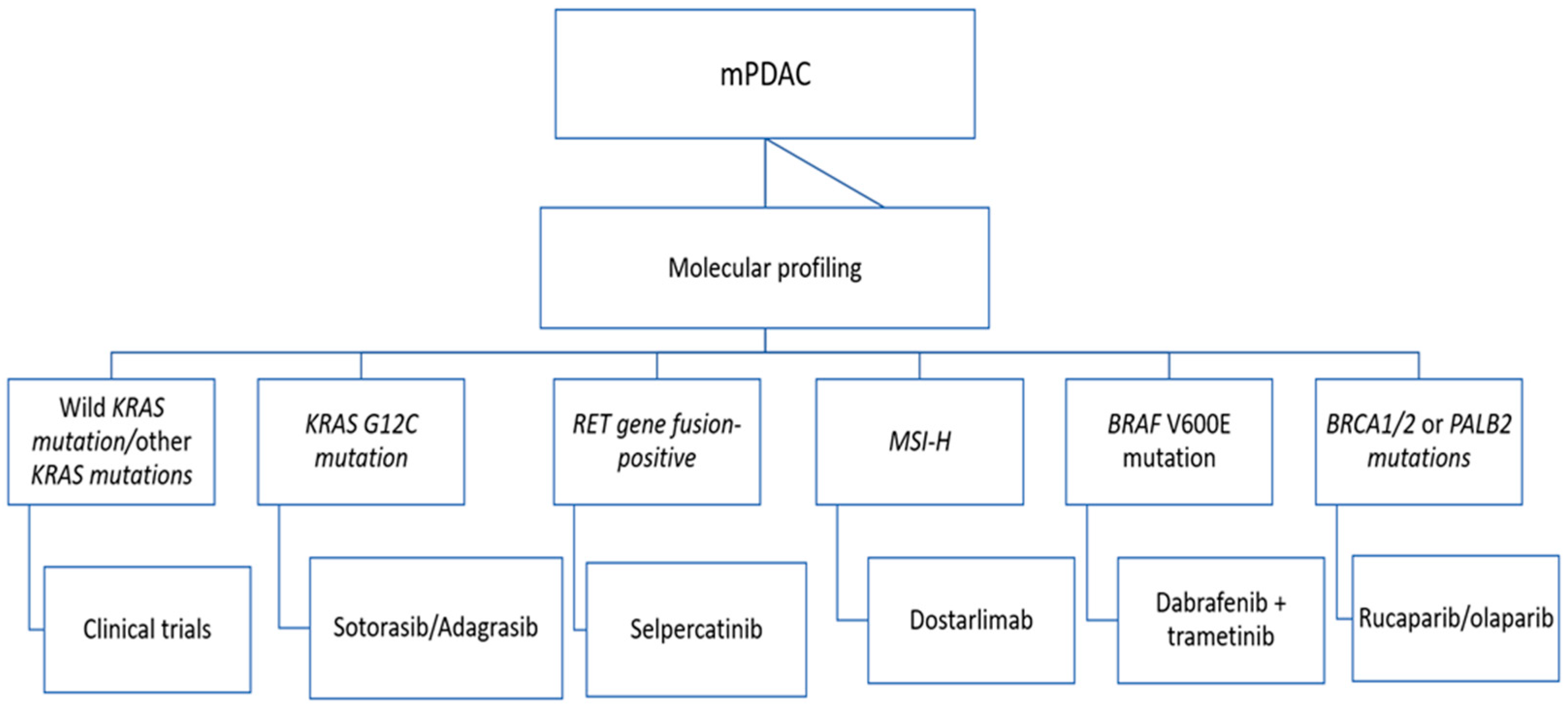
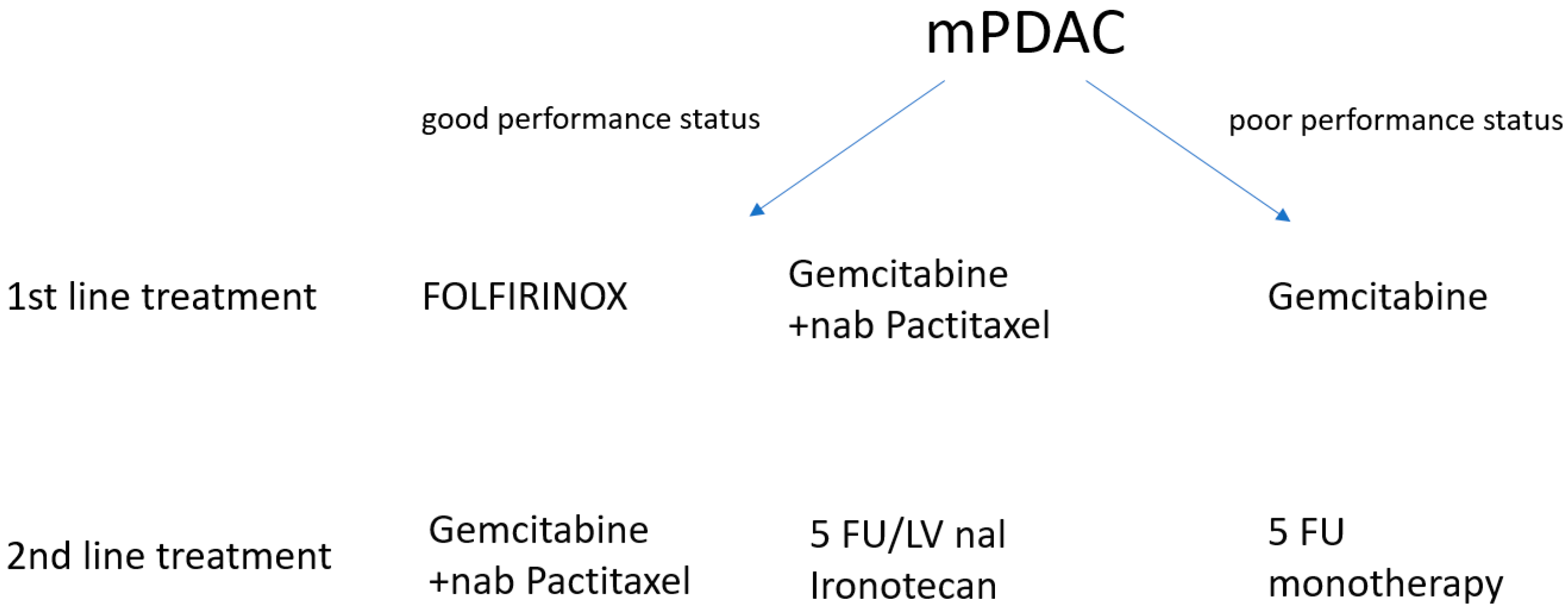
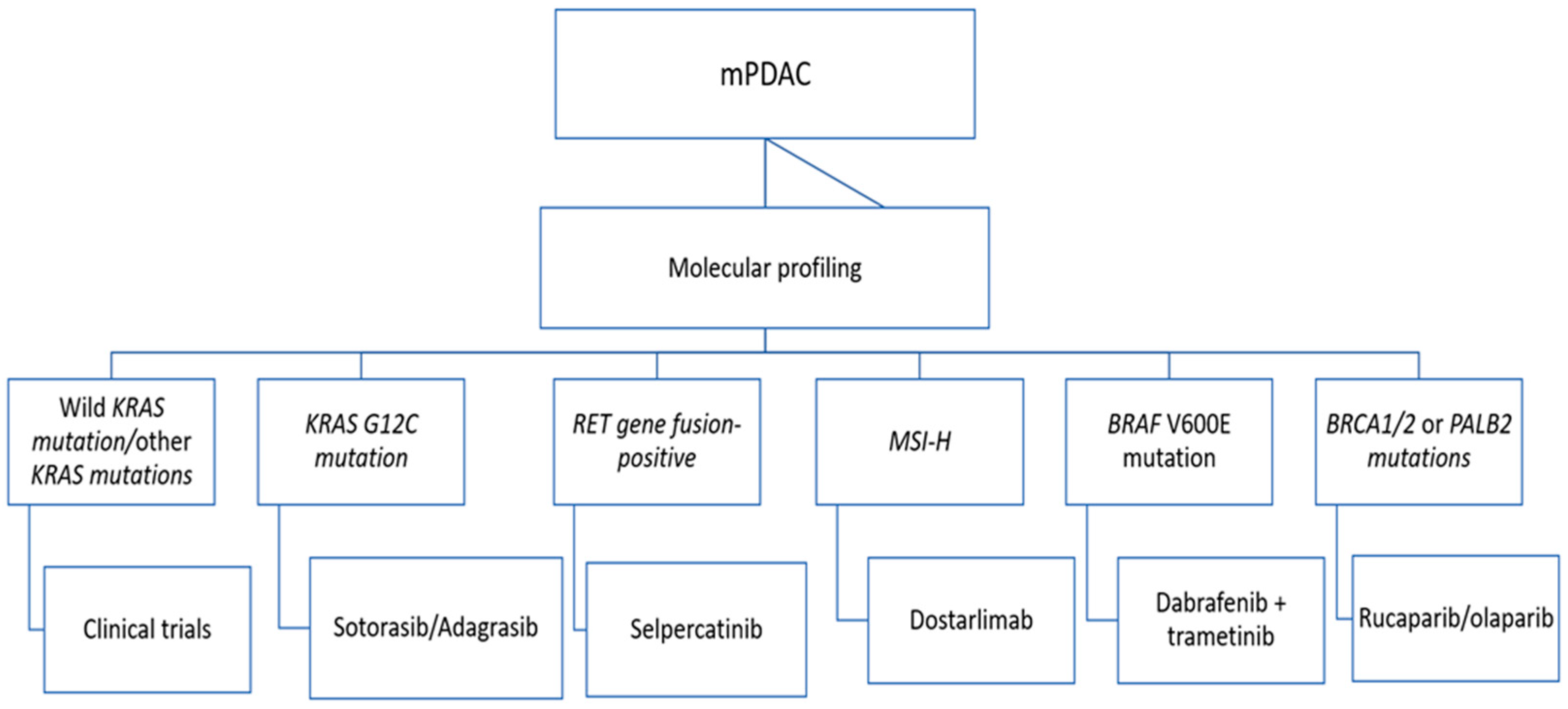
3.1. Advances in mPDAC Therapy over the Years
3.2. Changes in Guidelines over the Years
3.3. Future Research and Use of Bioinformatics
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, X.; Liu, F.; Xue, Q.; Weng, X.; Xu, F. Metastatic pancreatic cancer: Mechanisms and detection (Review). Oncol. Rep. 2021, 46, 231. [Google Scholar] [CrossRef]
- Available online: https://ecis.jrc.ec.europa.eu/ (accessed on 18 June 2023).
- Available online: https://ecis.jrc.ec.europa.eu/explorer.php?$0-0$1-All$4-1,2$3-19$6-0,85$5-2020,2020$7-8$2-All$CEstByCountry$X0_8-3$X0_19-AE27$X0_20-No$CEstBySexByCountry$X1_8-3$X1_19-AE27$X1_-1-1$CEstByIndiByCountry$X2_8-3$X2_19-AE27$X2_20-No$CEstRelative$X3_8-3$X3_9-AE27$X3_19-AE27$CEstByCountryTable$X4_19-AE27 (accessed on 20 June 2023).
- Kommalapati, A.; Tella, S.H.; Goyal, G.; Ma, W.W.; Mahipal, A. Contemporary Management of Localized Resectable Pancreatic Cancer. Cancers 2018, 10, 24. [Google Scholar] [CrossRef]
- Puleo, F.; Maréchal, R.; Demetter, P.; Bali, M.-A.; Calomme, A.; Closset, J.; Bachet, J.-B.; Deviere, J.; Van Laethem, J.-L. New challenges in perioperative management of pancreatic cancer. World J. Gastroenterol. 2015, 21, 2281–2293. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Sugiura, T.; Okamura, Y.; Ito, T.; Yamamoto, Y.; Ashida, R.; Ohgi, K.; Aramaki, T.; Endo, M.; Uesaka, K. Clinical Implication of Node-negative Resectable Pancreatic Cancer. Ann. Surg. Oncol. 2021, 28, 2257–2264. [Google Scholar] [CrossRef]
- Oweira, H.; Petrausch, U.; Helbling, D.; Schmidt, J.; Mannhart, M.; Mehrabi, A.; Schöb, O.; Giryes, A.; Decker, M.; Abdel-Rahman, O. Prognostic value of site-specific metastases in pancreatic adenocarcinoma: A Surveillance Epidemiology and End Results database analysis. World J. Gastroenterol. 2017, 23, 1872–1880. [Google Scholar] [CrossRef]
- Dreyer, S.B.; Upstill-Goddard, R.; Legrini, A.; Biankin, A.V.; Jamieson, N.B.; Chang, D.K.; Allison, S.; Beraldi, D.; Cameron, E.; Cooke, S.L.; et al. Genomic and Molecular Analyses Identify Molecular Subtypes of Pancreatic Cancer Recurrence. Gastroenterology 2022, 162, 320–324.e4. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://onkologia.org.pl/sites/default/files/publications/2023-01/nowotwory_2020.pdf (accessed on 20 June 2023).
- Dragovich, T.; Espat, J.; Erickson, R. Pancreatic Cancer Clinical Presentation: History, Physical Examination. Medscape. 2017. Available online: https://reference.medscape.com/ (accessed on 20 June 2023).
- Klein, A.P. Identifying people at a high risk of developing pancreatic cancer. Nat. Rev. Cancer 2013, 13, 66–74. [Google Scholar] [CrossRef]
- Schulte, A.; Pandeya, N.; Fawcett, J.; Fritschi, L.; Klein, K.; Risch, H.A.; Webb, P.M.; Whiteman, D.C.; Neale, R.E. Association between family cancer history and risk of pancreatic cancer. Cancer Epidemiol. 2016, 45, 145–150. [Google Scholar] [CrossRef]
- Tersmette, A.C.; Petersen, G.M.; Offerhaus, G.J.; Falatko, F.C.; Brune, K.A.; Goggins, M.; Rozenblum, E.; Wilentz, R.E.; Yeo, C.J.; Cameron, J.L.; et al. Increased risk of incident pancreatic cancer among first-degree relatives of patients with familial pancreatic cancer. Clin. Cancer Res. 2001, 7, 738–744. [Google Scholar] [PubMed]
- Silverman, D.T.; Schiffman, M.; Everhart, J.; Goldstein, A.; Lillemoe, K.D.; Swanson, G.M.; Schwartz, A.G.; Brown, L.M.; Greenberg, R.S.; Schoenberg, J.B.; et al. Diabetes mellitus, other medical conditions and familial history of cancer as risk factors for pancreatic cancer. Br. J. Cancer 1999, 80, 1830–1837. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502. [Google Scholar] [CrossRef]
- Yu, J.; Yang, X.; He, W.; Ye, W. Burden of pancreatic cancer along with attributable risk factors in Europe between 1990 and 2019, and projections until 2039. Inter. J. Cancer 2021, 149, 993–1001. [Google Scholar] [CrossRef]
- Bosetti, C.; Lucenteforte, E.; Silverman, D.T.; Petersen, G.; Bracci, P.M.; Ji, B.T.; Negri, E.; Li, D.; Risch, H.A.; Olson, S.H.; et al. Cigarette smoking and pancreatic cancer: An analysis from the International Pancreatic Cancer Case-Control Consortium (Panc4). Ann. Oncol. 2012, 23, 1880–1888. [Google Scholar] [CrossRef]
- Ding, Y.; Yu, C.; Han, Z.; Xu, S.; Li, D.; Meng, X.; Chen, D. Environmental tobacco smoke and pancreatic cancer: A case-control study. Int. J. Clin. Exp. Med. 2015, 8, 16729–16732. [Google Scholar] [PubMed]
- Wang, Y.-T.; Gou, Y.-W.; Jin, W.-W.; Xiao, M.; Fang, H.-Y. Association between alcohol intake and the risk of pancreatic cancer: A dose–response meta-analysis of cohort studies. BMC Cancer 2016, 16, 212. [Google Scholar] [CrossRef]
- Chen, F.; Childs, E.J.; Mocci, E.; Bracci, P.; Gallinger, S.; Li, D.; Neale, R.E.; Olson, S.H.; Scelo, G.; Bamlet, W.R.; et al. Analysis of Heritability and Genetic Architecture of Pancreatic Cancer: A PanC4 Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1238–1245. [Google Scholar] [CrossRef]
- Olakowski, M.; Bułdak, Ł. Current status of inherited pancreatic cancer. Hered. Cancer Clin. Pract. 2022, 20, 1–11. [Google Scholar] [CrossRef]
- Yeo, T.P. Demographics, Epidemiology, and Inheritance of Pancreatic Ductal Adenocarcinoma. Semin. Oncol. 2015, 42, 8–18. [Google Scholar] [CrossRef]
- Xu, M.; Jung, X.; Hines, O.J.; Eibl, G.; Chen, Y. Obesity and Pancreatic Cancer. Pancreas 2018, 47, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://ueg.eu/files/771/b7ee6f5f9aa5cd17ca1aea43ce848496.pdf (accessed on 20 June 2023).
- Yeo, T.P.; Hruban, R.H.; Brody, J.; Brune, K.; Fitzgerald, S.; Yeo, C.J. Assessment of “Gene–Environment” Interaction in Cases of Familial and Sporadic Pancreatic Cancer. J. Gastrointest. Surg. 2009, 13, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.E.; Hernandez, Y.G.; Frucht, H.; Lucas, A.L. Pancreatic ductal adenocarcinoma: Risk factors, screening, and early detection. World J. Gastroenterol. 2014, 20, 11182–11198. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S. Role of bacterial infections in pancreatic cancer. Carcinogenesis 2013, 34, 2193–2197. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, H.; Bording-Jorgensen, M.; Dijk, S.; Wine, E. The Complex Interplay between Chronic Inflammation, the Microbiome, and Cancer: Understanding Disease Progression and What We Can Do to Prevent It. Cancers 2018, 10, 83. [Google Scholar] [CrossRef] [PubMed]
- Ueda, S.; Ogata, S.; Tsuda, H.; Kawarabayashi, N.; Kimura, M.; Sugiura, Y.; Tamai, S.; Matsubara, O.; Hatsuse, K.; Mochizuki, H. The correlation between cytoplasmic overexpression of epidermal growth factor receptor and tumor aggressiveness: Poor prognosis in patients with pancreatic ductal adenocarcinoma. Pancreas 2004, 29, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Fudalej, M.; Kwaśniewska, D.; Nurzyński, P.; Badowska-Kozakiewicz, A.; Mękal, D.; Czerw, A.; Sygit, K.; Deptała, A. New Treatment Options in Metastatic Pancreatic Cancer. Cancers 2023, 15, 2327. [Google Scholar] [CrossRef]
- Carmichael, J.; Fink, U.; Russell, R.; Spittle, M.; Harris, A.; Spiessi, G.; Blatter, J. Phase II study of gemcitabine in patients with advanced pancreatic cancer. Br. J. Cancer 1996, 73, 101–105. [Google Scholar] [CrossRef]
- Burris, H.A., 3rd; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef]
- Moore, M.J.; Goldstein, D.; Hamm, J.; Figer, A.; Hecht, J.R.; Gallinger, S.; Au, H.J.; Murawa, P.; Walde, D.; Wolff, R.A.; et al. Erlotinib Plus Gemcitabine Compared With Gemcitabine Alone in Patients With Advanced Pancreatic Cancer: A Phase III Trial of the National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. 2007, 25, 1960–1966. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; De La Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Wang-Gillam, A.; Hubner, R.A.; Siveke, J.T.; Von Hoff, D.D.; Belanger, B.; de Jong, F.A.; Mirakhur, B.; Chen, L.-T. NAPOLI-1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: Final overall survival analysis and characteristics of long-term survivors. Eur. J. Cancer 2019, 108, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Zhang, X.; Parsons, D.W.; Lin, J.C.; Leary, R.J.; Angenendt, P.; Mankoo, P.; Carter, H.; Kamiyama, H.; Jimeno, A.; et al. Core signaling pathways in human pancreatic cancers revealed by global genomic analyses. Science 2008, 321, 1801–1806. [Google Scholar] [CrossRef] [PubMed]
- Collisson, E.A.; Sadanandam, A.; Olson, P.; Gibb, W.J.; Truitt, M.; Gu, S.; Cooc, J.; Weinkle, J.; Kim, G.E.; Jakkula, L.; et al. Subtypes of pancreatic ductal adenocarcinoma and their differing responses to therapy. Nat. Med. 2011, 17, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Moffitt, R.A.; Marayati, R.; Flate, E.L.; Volmar, K.E.; Loeza, S.G.; Hoadley, K.A.; Rashid, N.U.; Williams, L.A.; Eaton, S.C.; Chung, A.H.; et al. Virtual microdissection identifies distinct tumor- and stroma-specific subtypes of pancreatic ductal adenocarcinoma. Nat. Genet. 2015, 47, 1168–1178. [Google Scholar] [CrossRef]
- Golan, T.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef]
- Vandenbruck, Y.; Christiany, D.; Combes, F.; Loux, V.; Brun, V. Bioinformatics Tools and Workflow to Select Blood Biomarkers for Early Cancer Diagnosis: An Application to Pancreatic Cancer. Proteomics 2019, 19, 1800489. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Xu, H.; Chai, C.; Qin, Z.; Zhou, W. Integrated bioinformatics analysis of potential biomarkers for pancreatic cancer. J. Clin. Lab Anal. 2022, 36, e24381. [Google Scholar] [CrossRef]
- Ke, M.; Ji, L.; Li, Y. Bioinformatics analysis combined with experiments to explore potential prognostic factors for pancreatic cancer. Cancer Cell Int. 2020, 20, 382. [Google Scholar] [CrossRef]
- Xu, J.-S.; Liao, K.-L.; Wang, X.-Z.; He, J.; Wang, X. Combining bioinformatics techniques to explore the molecular mechanisms involved in pancreatic cancer metastasis and prognosis. J. Cell Mol. Med. 2020, 24, 14128–14138. [Google Scholar] [CrossRef]
- Available online: https://www.esmo.org/guidelines/guidelines-by-topic/gastrointestinal-cancers/pancreatic-cancer (accessed on 26 June 2023).
- Available online: https://old-prod.asco.org/sites/new-www.asco.org/files/content-files/advocacy-and-policy/documents/2020-Metastatic-Pancreatic-Cancer-Summary-Table.pdf (accessed on 26 June 2023).
- Available online: https://www.nice.org.uk/guidance/ng85 (accessed on 27 June 2023).
- Available online: https://seom.org/images/SEOM_CLINICAL_GUIDELINE_PANCREATIC_AND_BILIARY_TRACT_CANCER_2020.pdf (accessed on 28 June 2023).
- Frappart, P.O.; Hofmann, T.G. Pancreatic Ductal Adenocarcinoma (PDAC) Organoids: The Shining Light at the End of the Tunnel for Drug Response Prediction and Personalized Medicine. Cancers 2020, 12, 2750. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| ESMO 2019 | ASCO 2018 | ASCO 2020 | SEOM 2020 | NICE 2018 | NCCN 2023 |
|---|---|---|---|---|---|
First-line treatment
| First-line treatment
| First-line treatment In patients who will be potential candidates for additional treatment after first-line therapy, early screening for applicable genomic changes is recommended. Both germline and tumor testing are recommended. Other guidelines as in ASCO 2018; Second-line treatment
| First-line treatment
| First-line treatment
| First-line treatment If jaundice is present: the application of SEMS (self-expandable metal stent); Genetic testing for hereditary mutations if not previously tested; Molecular profiling of the tumor tissue, if not performed, if the patient’s condition is good or moderately good—qualification for a clinical trial (preferred) or systemic therapy (FOLFIRINOX or modified FOLFIRINOX followed by chemoradiotherapy or gemcitabine + albumin-bound paclitaxel ± followed by radiochemotherapy) if BRCA1/2 or PALB2 mutation is present—FOLFIRINOX or modified FOLFIRINOX, followed by chemoradiotherapy or Gemcitabine + cisplatinum (≥2–6 cycles) ± then chemoradiotherapy, if there is no progression of the disease after 4–6 months (at an acceptable level of toxicity), we continue the therapy from the clinical trial; in the case of poor general condition of the patient, palliative therapy or monochemotherapy or targeted therapy based on molecular profiling, as clinically indicated, or palliative radiotherapy; Maintenance therapy Use FOLFIRINOX or modified FOLFIRINOX followed by chemoradiotherapy or gemcitabine + albumin-bound paclitaxel ± then radiochemotherapy or if there is a BRCA1/2 or PALB2 mutation—FOLFIRINOX or modified FOLFIRINOX followed by chemoradiotherapy or Gemcitabine + cisplatin (≥2–6 cycles) ± then chemoradiotherapy or stop chemotherapy, if the disease progresses, the progression scheme is used if the previous therapy was based on platinum: Rucaparib (for germline or somatic BRCA1/2 or PALB2 mutations); Further therapy of metastatic disease: ntrectinib (if NTRK gene fusion is positive) Larotrectinib (if NTRK gene fusion is positive) Pembrolizumab (if MSI-H, dMMR or TMB-H [≥10 mut/Mb]) Dabrafenib + trametinib (if BRAF V600E mutation positive) Dostarlimab (if MSI-H or dMMR) Selpercatinib (if RET gene fusion is positive) Sotorazib/Adagrasib (for KRAS G12C mutation) Nivolumab + ipilimumab (if TMB-H [≥10 mut/Mb]); If previous therapy was based on gemcitabine, the following is recommended:
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pajewska, M.; Partyka, O.; Czerw, A.; Deptała, A.; Cipora, E.; Gąska, I.; Wojtaszek, M.; Sygit, K.; Sygit, M.; Krzych-Fałta, E.; et al. Management of Metastatic Pancreatic Cancer—Comparison of Global Guidelines over the Last 5 Years. Cancers 2023, 15, 4400. https://doi.org/10.3390/cancers15174400
Pajewska M, Partyka O, Czerw A, Deptała A, Cipora E, Gąska I, Wojtaszek M, Sygit K, Sygit M, Krzych-Fałta E, et al. Management of Metastatic Pancreatic Cancer—Comparison of Global Guidelines over the Last 5 Years. Cancers. 2023; 15(17):4400. https://doi.org/10.3390/cancers15174400
Chicago/Turabian StylePajewska, Monika, Olga Partyka, Aleksandra Czerw, Andrzej Deptała, Elżbieta Cipora, Izabela Gąska, Marek Wojtaszek, Katarzyna Sygit, Marian Sygit, Edyta Krzych-Fałta, and et al. 2023. "Management of Metastatic Pancreatic Cancer—Comparison of Global Guidelines over the Last 5 Years" Cancers 15, no. 17: 4400. https://doi.org/10.3390/cancers15174400
APA StylePajewska, M., Partyka, O., Czerw, A., Deptała, A., Cipora, E., Gąska, I., Wojtaszek, M., Sygit, K., Sygit, M., Krzych-Fałta, E., Schneider-Matyka, D., Cybulska, A. M., Grochans, E., Asendrych-Woźniak, A., Romanowicz, A., Drobnik, J., Bandurska, E., Ciećko, W., Maciuszek-Bartkowska, B., ... Marczak, M. (2023). Management of Metastatic Pancreatic Cancer—Comparison of Global Guidelines over the Last 5 Years. Cancers, 15(17), 4400. https://doi.org/10.3390/cancers15174400