
Efficacy of Thermal Ablation for Small-Size (0–3 cm) versus Intermediate-Size (3–5 cm) Colorectal Liver Metastases: Results from the Amsterdam Colorectal Liver Met Registry (AmCORE)

 , ,
, ,  ,
,  , ,
, , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
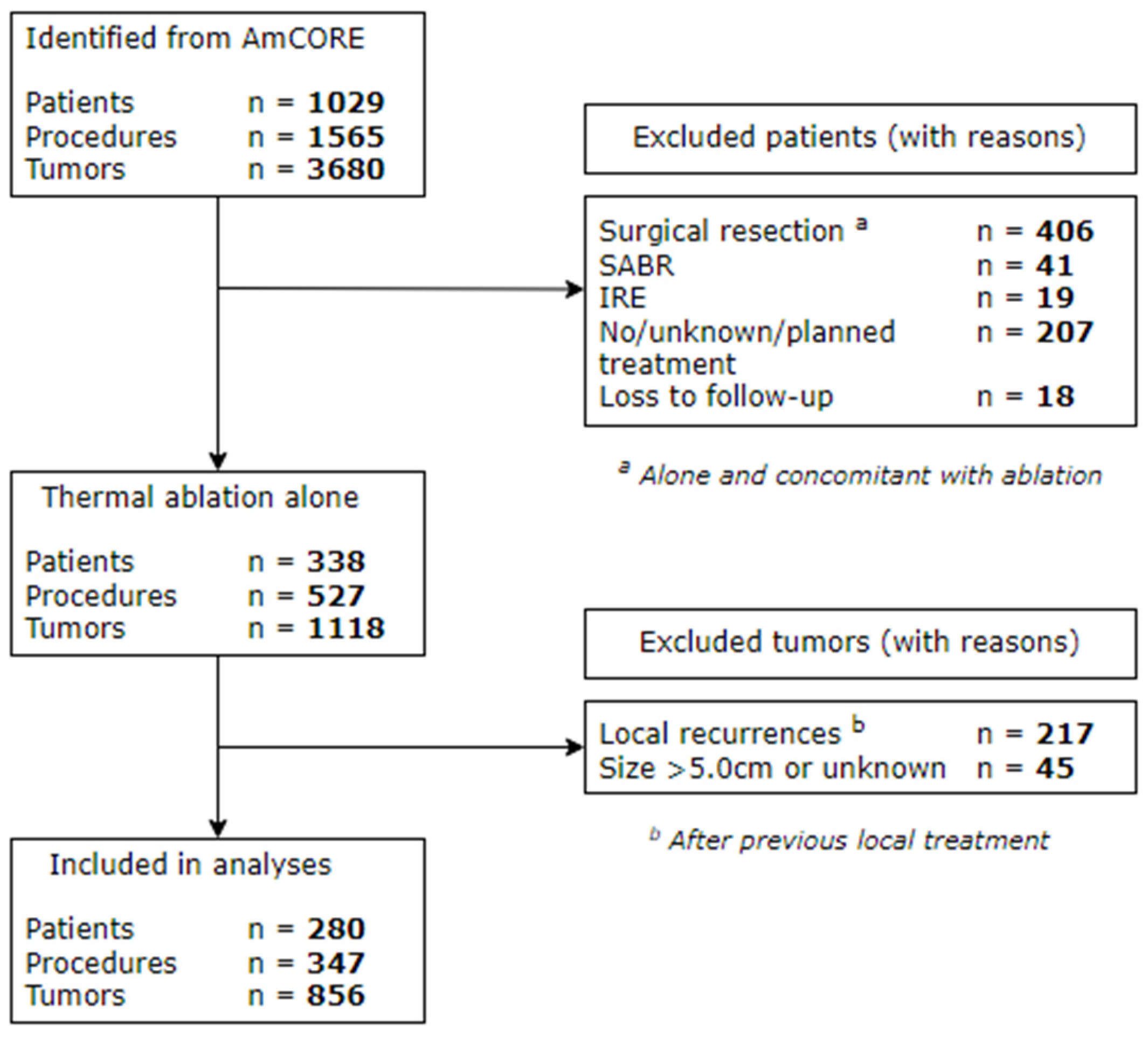
2.1. Patient Selection and Data Collection
2.2. Thermal Ablation Procedure
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient- and Disease-Related Characteristics
3.2. Procedure- and Tumor-Related Characteristics
3.3. Complications and Length of Hospital Stay
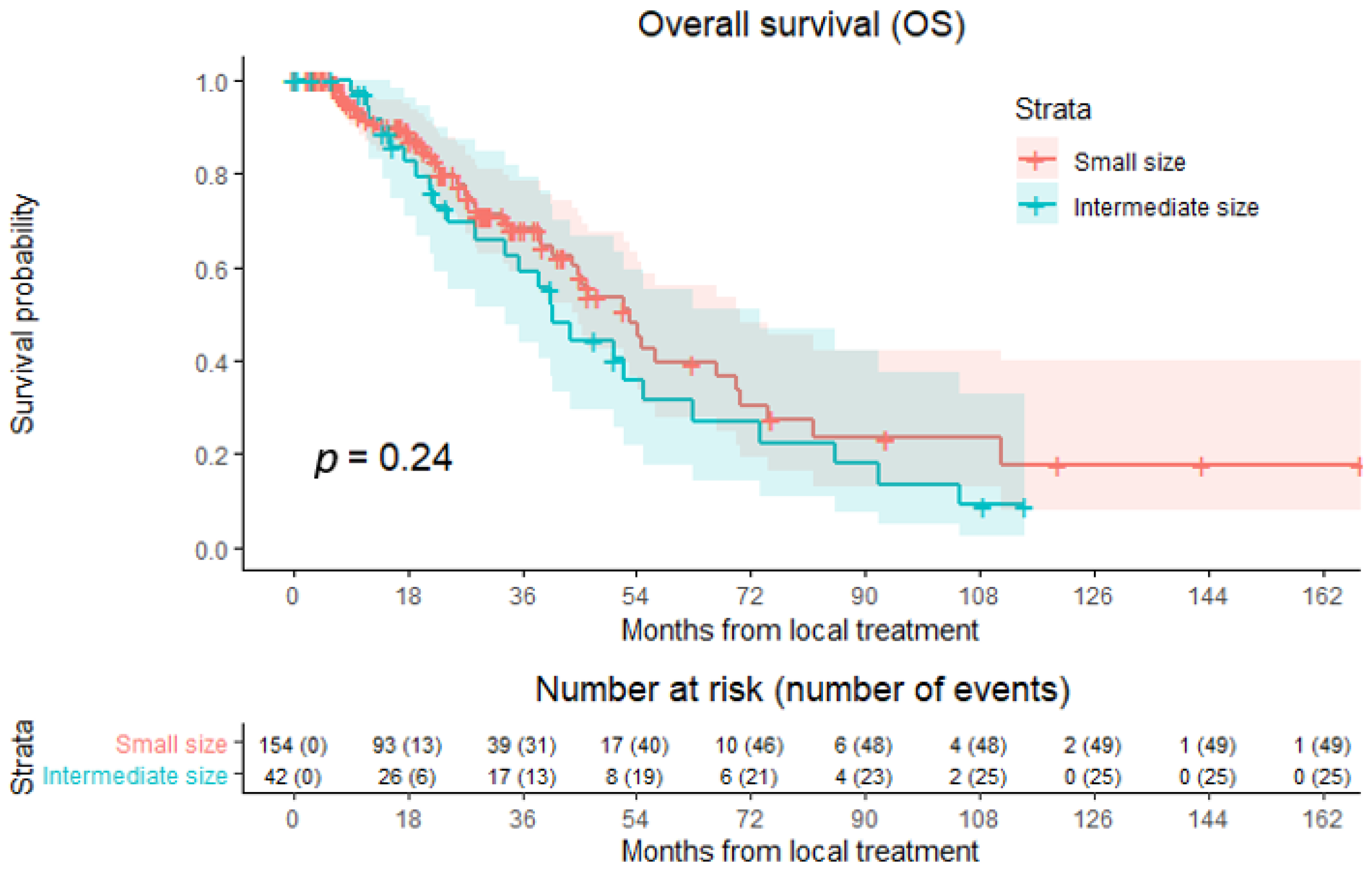
3.4. Overall Survival (OS)
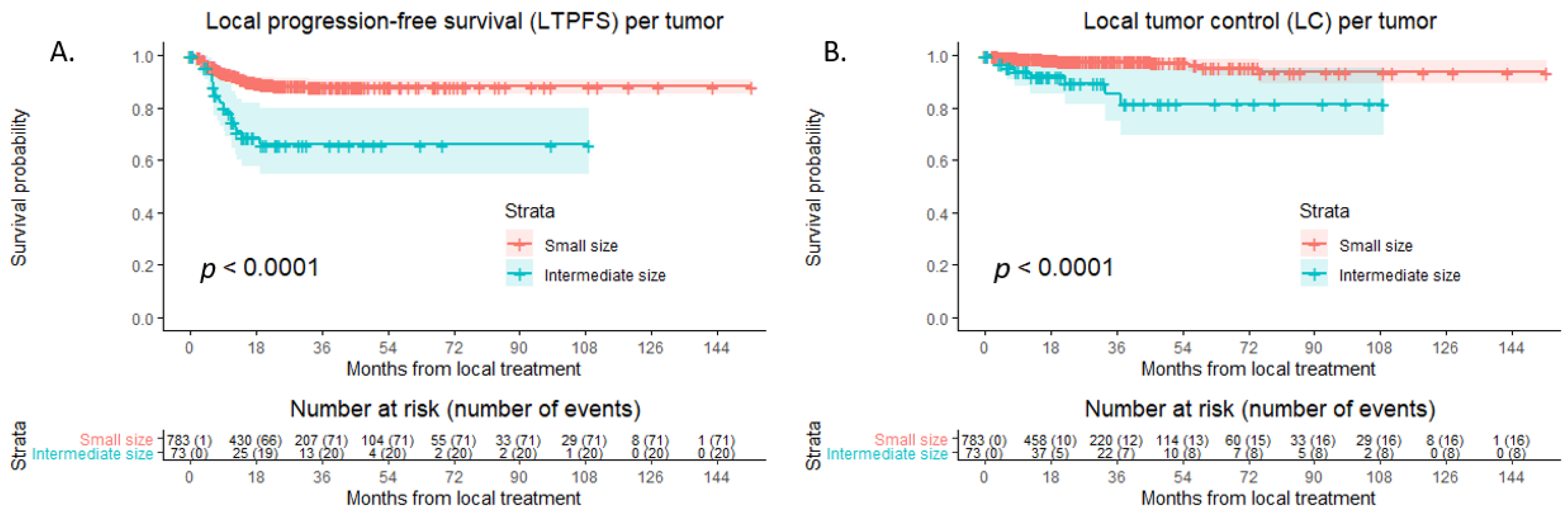
3.5. Local Tumor Progression-Free Survival (LTPFS) and Local Tumor Control (LC)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Estimated Age-Standardized Incidence Rates (World) in 2020, All Cancers, Both Sexes, All Ages. Available online: http://gco.iarc.fr/today/online-analysis-map (accessed on 4 March 2021).
- Manfredi, S.; Lepage, C.; Hatem, C.; Coatmeur, O.; Faivre, J.; Bouvier, A.M. Epidemiology and management of liver metastases from colorectal cancer. Ann. Surg. 2006, 244, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Hackl, C.; Neumann, P.; Gerken, M.; Loss, M.; Klinkhammer-Schalke, M.; Schlitt, H.J. Treatment of colorectal liver metastases in Germany: A ten-year population-based analysis of 5772 cases of primary colorectal adenocarcinoma. BMC Cancer 2014, 14, 810. [Google Scholar] [CrossRef] [PubMed]
- Engstrand, J.; Nilsson, H.; Stromberg, C.; Jonas, E.; Freedman, J. Colorectal cancer liver metastases—A population-based study on incidence, management and survival. BMC Cancer 2018, 18, 78. [Google Scholar] [CrossRef]
- Kopetz, S.; Chang, G.J.; Overman, M.J.; Eng, C.; Sargent, D.J.; Larson, D.W.; Grothey, A.; Vauthey, J.N.; Nagorney, D.M.; McWilliams, R.R. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J. Clin. Oncol. 2009, 27, 3677–3683. [Google Scholar] [CrossRef] [PubMed]
- Stangl, R.; Altendorf-Hofmann, A.; Charnley, R.M.; Scheele, J. Factors influencing the natural history of colorectal liver metastases. Lancet 1994, 343, 1405–1410. [Google Scholar] [CrossRef]
- Scheele, J.; Stangl, R.; Altendorf-Hofmann, A. Hepatic metastases from colorectal carcinoma: Impact of surgical resection on the natural history. Br. J. Surg. 1990, 77, 1241–1246. [Google Scholar] [CrossRef]
- Wagner, J.S.; Adson, M.A.; Van Heerden, J.A.; Adson, M.H.; Ilstrup, D.M. The natural history of hepatic metastases from colorectal cancer. A comparison with resective treatment. Ann. Surg. 1984, 199, 502–508. [Google Scholar] [CrossRef]
- Yang, Q.; Liao, F.; Huang, Y.; Jiang, C.; Liu, S.; He, W.; Kong, P.; Zhang, B.; Xia, L. Longterm effects of palliative local treatment of incurable metastatic lesions in colorectal cancer patients. Oncotarget 2016, 7, 21034–21045. [Google Scholar] [CrossRef][Green Version]
- Adam, R.; Avisar, E.; Ariche, A.; Giachetti, S.; Azoulay, D.; Castaing, D.; Kunstlinger, F.; Levi, F.; Bismuth, F. Five-year survival following hepatic resection after neoadjuvant therapy for nonresectable colorectal. Ann. Surg. Oncol. 2001, 8, 347–353. [Google Scholar] [CrossRef]
- House, M.G.; Ito, H.; Gonen, M.; Fong, Y.; Allen, P.J.; DeMatteo, R.P.; Brennan, M.F.; Blumgart, L.H.; Jarnagin, W.R.; D’Angelica, M.I. Survival after hepatic resection for metastatic colorectal cancer: Trends in outcomes for 1600 patients during two decades at a single institution. J. Am. Coll. Surg. 2010, 210, 744–752, 752–755. [Google Scholar] [CrossRef]
- Kanas, G.P.; Taylor, A.; Primrose, J.N.; Langeberg, W.J.; Kelsh, M.A.; Mowat, F.S.; Alexander, D.D.; Choti, M.A.; Poston, G. Survival after liver resection in metastatic colorectal cancer: Review and meta-analysis of prognostic factors. Clin. Epidemiol. 2012, 4, 283–301. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): Long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Elfrink, A.K.E.; Nieuwenhuizen, S.; van den Tol, M.P.; Burgmans, M.C.; Prevoo, W.; Coolsen, M.M.E.; van den Boezem, P.B.; van Delden, O.M.; Hagendoorn, J.; Patijn, G.A.; et al. Hospital variation in combined liver resection and thermal ablation for colorectal liver metastases and impact on short-term postoperative outcomes: A nationwide population-based study. HPB 2021, 23, 827–839. [Google Scholar] [CrossRef]
- Adam, R.; Delvart, V.; Pascal, G.; Valeanu, A.; Castaing, D.; Azoulay, D.; Giacchetti, S.; Paule, B.; Kunstlinger, F.; Ghemard, O.; et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy: A model to predict long-term survival. Ann. Surg. 2004, 240, 644–657, discussion 657–658. [Google Scholar] [CrossRef]
- Meijerink, M.R.; Puijk, R.S.; van Tilborg, A.; Henningsen, K.H.; Fernandez, L.G.; Neyt, M.; Heymans, J.; Frankema, J.S.; de Jong, K.P.; Richel, D.J.; et al. Radiofrequency and Microwave Ablation Compared to Systemic Chemotherapy and to Partial Hepatectomy in the Treatment of Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. CardioVasc. Interv. Radiol. 2018, 41, 1189–1204. [Google Scholar] [CrossRef]
- Scheffer, H.J.; Melenhorst, M.C.; Echenique, A.M.; Nielsen, K.; van Tilborg, A.A.; van den Bos, W.; Vroomen, L.G.; van den Tol, P.M.; Meijerink, M.R. Irreversible Electroporation for Colorectal Liver Metastases. Tech. Vasc. Interv. Radiol. 2015, 18, 159–169. [Google Scholar] [CrossRef]
- Correa-Gallego, C.; Fong, Y.; Gonen, M.; D’Angelica, M.I.; Allen, P.J.; DeMatteo, R.P.; Jarnagin, W.R.; Kingham, T.P. A retrospective comparison of microwave ablation vs. radiofrequency ablation for colorectal cancer hepatic metastases. Ann. Surg. Oncol. 2014, 21, 4278–4283. [Google Scholar] [CrossRef] [PubMed]
- van der Pool, A.E.; Mendez Romero, A.; Wunderink, W.; Heijmen, B.J.; Levendag, P.C.; Verhoef, C.; Ijzermans, J.N. Stereotactic body radiation therapy for colorectal liver metastases. Br. J. Surg. 2010, 97, 377–382. [Google Scholar] [CrossRef]
- Dijkstra, M.; Nieuwenhuizen, S.; Puijk, R.S.; Geboers, B.; Timmer, F.E.F.; Schouten, E.A.C.; Scheffer, H.J.; de Vries, J.J.J.; Ket, J.C.F.; Versteeg, K.S.; et al. The Role of Neoadjuvant Chemotherapy in Repeat Local Treatment of Recurrent Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 378. [Google Scholar] [CrossRef]
- Dijkstra, M.; Nieuwenhuizen, S.; Puijk, R.S.; Timmer, F.E.F.; Geboers, B.; Schouten, E.A.C.; Opperman, J.; Scheffer, H.J.; de Vries, J.J.J.; Swijnenburg, R.J.; et al. Thermal Ablation Compared to Partial Hepatectomy for Recurrent Colorectal Liver Metastases: An Amsterdam Colorectal Liver Met Registry (AmCORE) Based Study. Cancers 2021, 13, 2769. [Google Scholar] [CrossRef]
- Dijkstra, M.; Nieuwenhuizen, S.; Puijk, R.S.; Timmer, F.E.F.; Geboers, B.; Schouten, E.A.C.; Opperman, J.; Scheffer, H.J.; de Vries, J.J.J.; Versteeg, K.S.; et al. Primary Tumor Sidedness, RAS and BRAF Mutations and MSI Status as Prognostic Factors in Patients with Colorectal Liver Metastases Treated with Surgery and Thermal Ablation: Results from the Amsterdam Colorectal Liver Met Registry (AmCORE). Biomedicines 2021, 9, 962. [Google Scholar] [CrossRef]
- Dijkstra, M.; Nieuwenhuizen, S.; Puijk, R.S.; Timmer, F.E.F.; Geboers, B.; Schouten, E.A.C.; Opperman, J.; Scheffer, H.J.; de Vries, J.J.J.; Versteeg, K.S.; et al. Repeat Local Treatment of Recurrent Colorectal Liver Metastases, the Role of Neoadjuvant Chemotherapy: An Amsterdam Colorectal Liver Met Registry (AmCORE) Based Study. Cancers 2021, 13, 4997. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuizen, S.; Puijk, R.S.; van den Bemd, B.; Aldrighetti, L.; Arntz, M.; van den Boezem, P.B.; Bruynzeel, A.M.E.; Burgmans, M.C.; de Cobelli, F.; Coolsen, M.M.E.; et al. Resectability and Ablatability Criteria for the Treatment of Liver Only Colorectal Metastases: Multidisciplinary Consensus Document from the COLLISION Trial Group. Cancers 2020, 12, 1779. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, K.; van Tilborg, A.A.; Meijerink, M.R.; Macintosh, M.O.; Zonderhuis, B.M.; de Lange, E.S.; Comans, E.F.; Meijer, S.; van den Tol, M.P. Incidence and treatment of local site recurrences following RFA of colorectal liver metastases. World J. Surg. 2013, 37, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- van Tilborg, A.A.; Scheffer, H.J.; de Jong, M.C.; Vroomen, L.G.; Nielsen, K.; van Kuijk, C.; van den Tol, P.M.; Meijerink, M.R. MWA Versus RFA for Perivascular and Peribiliary CRLM: A Retrospective Patient- and Lesion-Based Analysis of Two Historical Cohorts. CardioVasc. Interv. Radiol. 2016, 39, 1438–1446. [Google Scholar] [CrossRef] [PubMed]
- Tanis, E.; Nordlinger, B.; Mauer, M.; Sorbye, H.; van Coevorden, F.; Gruenberger, T.; Schlag, P.M.; Punt, C.J.; Ledermann, J.; Ruers, T.J. Local recurrence rates after radiofrequency ablation or resection of colorectal liver metastases. Analysis of the European Organisation for Research and Treatment of Cancer #40004 and #40983. Eur. J. Cancer 2014, 50, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Solbiati, L.; Livraghi, T.; Goldberg, S.N.; Ierace, T.; Meloni, F.; Dellanoce, M.; Cova, L.; Halpern, E.F.; Gazelle, G.S. Percutaneous radio-frequency ablation of hepatic metastases from colorectal cancer: Long-term results in 117 patients. Radiology 2001, 221, 159–166. [Google Scholar] [CrossRef]
- Berber, E.; Siperstein, A. Local recurrence after laparoscopic radiofrequency ablation of liver tumors: An analysis of 1032 tumors. Ann. Surg. Oncol. 2008, 15, 2757–2764. [Google Scholar] [CrossRef]
- Van Tilborg, A.A.; Meijerink, M.R.; Sietses, C.; Van Waesberghe, J.H.; Mackintosh, M.O.; Meijer, S.; Van Kuijk, C.; Van Den Tol, P. Long-term results of radiofrequency ablation for unresectable colorectal liver metastases: A potentially curative intervention. Br. J. Radiol. 2011, 84, 556–565. [Google Scholar] [CrossRef]
- Ayav, A.; Germain, A.; Marchal, F.; Tierris, I.; Laurent, V.; Bazin, C.; Yuan, Y.; Robert, L.; Brunaud, L.; Bresler, L. Radiofrequency ablation of unresectable liver tumors: Factors associated with incomplete ablation or local recurrence. Am. J. Surg. 2010, 200, 435–439. [Google Scholar] [CrossRef]
- Nieuwenhuizen, S.; Dijkstra, M.; Puijk, R.S.; Geboers, B.; Ruarus, A.H.; Schouten, E.A.; Nielsen, K.; de Vries, J.J.J.; Bruynzeel, A.M.E.; Scheffer, H.J.; et al. Microwave Ablation, Radiofrequency Ablation, Irreversible Electroporation, and Stereotactic Ablative Body Radiotherapy for Intermediate Size (3–5 cm) Unresectable Colorectal Liver Metastases: A Systematic Review and Meta-analysis. Curr. Oncol. Rep. 2022, 24, 793–808. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Puijk, R.S.; Ahmed, M.; Adam, A.; Arai, Y.; Arellano, R.; de Baere, T.; Bale, R.; Bellera, C.; Binkert, C.A.; Brace, C.L.; et al. Consensus Guidelines for the Definition of Time-to-Event End Points in Image-guided Tumor Ablation: Results of the SIO and DATECAN Initiative. Radiology 2021, 301, 533–540. [Google Scholar] [CrossRef]
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; Chen, M.H.; Choi, B.I.; de Baere, T.; Dodd, G.D., III; et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria--a 10-year update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef]
- Crocetti, L.; de Baere, T.; Lencioni, R. Quality improvement guidelines for radiofrequency ablation of liver tumours. CardioVasc. Interv. Radiol. 2010, 33, 11–17. [Google Scholar] [CrossRef]
- Shady, W.; Petre, E.N.; Do, K.G.; Gonen, M.; Yarmohammadi, H.; Brown, K.T.; Kemeny, N.E.; D’Angelica, M.; Kingham, P.T.; Solomon, S.B.; et al. Percutaneous Microwave versus Radiofrequency Ablation of Colorectal Liver Metastases: Ablation with Clear Margins (A0) Provides the Best Local Tumor Control. J. Vasc. Interv. Radiol. 2018, 29, 268–275.e1. [Google Scholar] [CrossRef]
- Crocetti, L.; de Baére, T.; Pereira, P.L.; Tarantino, F.P. CIRSE Standards of Practice on Thermal Ablation of Liver Tumours. CardioVasc. Interv. Radiol. 2020, 43, 951–962. [Google Scholar] [CrossRef]
- Comprehensive Cancer Organisation the Netherlands (I.K.N.L.). National Evidence-Based Guideline. Colorectaalcarcinoom. 2014. Available online: http://oncoline.nl/ (accessed on 1 December 2021).
- IBM Corp. IBM® SPSS® Statistics for Windows; Version 26.0; Released 2019; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing, R for Windows Version 4.0.3; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: http://www.R-project.org/ (accessed on 1 December 2021).
- Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_8.5x11.pdf (accessed on 25 November 2020).
- Puijk, R.S.; Dijkstra, M.; van den Bemd, B.A.T.; Ruarus, A.H.; Nieuwenhuizen, S.; Geboers, B.; Timmer, F.E.F.; Schouten, E.A.C.; de Vries, J.J.J.; van der Meijs, B.B.; et al. Improved Outcomes of Thermal Ablation for Colorectal Liver Metastases: A 10-Year Analysis from the Prospective Amsterdam CORE Registry (AmCORE). CardioVasc. Interv. Radiol. 2022, 45, 1074–1089. [Google Scholar] [CrossRef]
- Puijk, R.S.; Nieuwenhuizen, S.; van den Bemd, B.A.T.; Ruarus, A.H.; Geboers, B.; Vroomen, L.; Muglia, R.; de Jong, M.C.; de Vries, J.J.J.; Scheffer, H.J.; et al. Transcatheter CT Hepatic Arteriography Compared with Conventional CT Fluoroscopy Guidance in Percutaneous Thermal Ablation to Treat Colorectal Liver Metastases: A Single-Center Comparative Analysis of 2 Historical Cohorts. J. Vasc. Interv. Radiol. 2020, 31, 1772–1783. [Google Scholar] [CrossRef]
- Puijk, R.S.; Ziedses des Plantes, V.; Nieuwenhuizen, S.; Ruarus, A.H.; Vroomen, L.; de Jong, M.C.; Geboers, B.; Hoedemaker-Boon, C.J.; Thone-Passchier, D.H.; Gercek, C.C.; et al. Propofol Compared to Midazolam Sedation and to General Anesthesia for Percutaneous Microwave Ablation in Patients with Hepatic Malignancies: A Single-Center Comparative Analysis of Three Historical Cohorts. CardioVasc. Interv. Radiol. 2019, 42, 1597–1608. [Google Scholar] [CrossRef]
- Bale, R.; Widmann, G.; Schullian, P.; Haidu, M.; Pall, G.; Klaus, A.; Weiss, H.; Biebl, M.; Margreiter, R. Percutaneous stereotactic radiofrequency ablation of colorectal liver metastases. Eur. Radiol. 2012, 22, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Zhao, J.J.; Bi, X.Y.; Zhang, Y.F.; Han, Y.; Li, Z.Y.; Zhao, H.; Cai, J.Q. Resectable recurrent colorectal liver metastasis: Can radiofrequency ablation replace repeated metastasectomy? ANZ J. Surg. 2019, 89, 908–913. [Google Scholar] [CrossRef]
- Wang, C.Z.; Yan, G.X.; Xin, H.; Liu, Z.Y. Oncological outcomes and predictors of radiofrequency ablation of colorectal cancer liver metastases. World J. Gastrointest. Oncol. 2020, 12, 1044–1055. [Google Scholar] [CrossRef]
- Puijk, R.S.; Ruarus, A.H.; Vroomen, L.; van Tilborg, A.; Scheffer, H.J.; Nielsen, K.; de Jong, M.C.; de Vries, J.J.J.; Zonderhuis, B.M.; Eker, H.H.; et al. Colorectal liver metastases: Surgery versus thermal ablation (COLLISION)—A phase III single-blind prospective randomized controlled trial. BMC Cancer 2018, 18, 821. [Google Scholar] [CrossRef]
- van Amerongen, M.J.; Jenniskens, S.F.M.; van den Boezem, P.B.; Futterer, J.J.; de Wilt, J.H.W. Radiofrequency ablation compared to surgical resection for curative treatment of patients with colorectal liver metastases—A meta-analysis. HPB 2017, 19, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuizen, S.; Dijkstra, M.; Puijk, R.S.; Timmer, F.E.F.; Nota, I.M.; Opperman, J.; van den Bemd, B.; Geboers, B.; Ruarus, A.H.; Schouten, E.A.C.; et al. Thermal Ablation versus Stereotactic Ablative Body Radiotherapy to Treat Unresectable Colorectal Liver Metastases: A Comparative Analysis from the Prospective Amsterdam CORE Registry. Cancers 2021, 13, 4303. [Google Scholar] [CrossRef]
- Mahadevan, A.; Blanck, O.; Lanciano, R.; Peddada, A.; Sundararaman, S.; D’Ambrosio, D.; Sharma, S.; Perry, D.; Kolker, J.; Davis, J. Stereotactic Body Radiotherapy (SBRT) for liver metastasis—Clinical outcomes from the international multi-institutional RSSearch(R) Patient Registry. Radiat. Oncol. 2018, 13, 26. [Google Scholar] [CrossRef]
- Scorsetti, M.; Comito, T.; Tozzi, A.; Navarria, P.; Fogliata, A.; Clerici, E.; Mancosu, P.; Reggiori, G.; Rimassa, L.; Torzilli, G.; et al. Final results of a phase II trial for stereotactic body radiation therapy for patients with inoperable liver metastases from colorectal cancer. J. Cancer Res. Clin. Oncol. 2015, 141, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Berber, B.; Ibarra, R.; Snyder, L.; Yao, M.; Fabien, J.; Milano, M.T.; Katz, A.W.; Goodman, K.; Stephans, K.; El-Gazzaz, G.; et al. Multicentre results of stereotactic body radiotherapy for secondary liver tumours. HPB 2013, 15, 851–857. [Google Scholar] [CrossRef] [PubMed]
- van der Lei, S.; Dijkstra, M.; Nieuwenhuizen, S.; Schulz, H.H.; Vos, D.J.W.; Versteeg, K.S.; Buffart, T.E.; Swijnenburg, R.J.; de Vries, J.J.J.; Bruynzeel, A.M.E.; et al. Unresectable Intermediate-Size (3–5 cm) Colorectal Liver Metastases: Stereotactic Ablative Body Radiotherapy Versus Microwave Ablation (COLLISION-XL): Protocol of a Phase II/III Multicentre Randomized Controlled Trial. CardioVasc. Interv. Radiol. 2023, 46, 1076–1085. [Google Scholar] [CrossRef]
- Geboers, B.; Ruarus, A.H.; Nieuwenhuizen, S.; Puijk, R.S.; Scheffer, H.J.; de Gruijl, T.D.; Meijerink, M.R. Needle-guided ablation of locally advanced pancreatic cancer: Cytoreduction or immunomodulation by in vivo vaccination? Chin. Clin. Oncol. 2019, 8, 61. [Google Scholar] [CrossRef]
- Ruarus, A.H.; Vroomen, L.; Puijk, R.S.; Scheffer, H.J.; Zonderhuis, B.M.; Kazemier, G.; van den Tol, M.P.; Berger, F.H.; Meijerink, M.R. Irreversible Electroporation in Hepatopancreaticobiliary Tumours. Can. Assoc. Radiol. J. 2018, 69, 38–50. [Google Scholar] [CrossRef]
- Meijerink, M.R.; Ruarus, A.H.; Vroomen, L.; Puijk, R.S.; Geboers, B.; Nieuwenhuizen, S.; van den Bemd, B.A.T.; Nielsen, K.; de Vries, J.J.J.; van Lienden, K.P.; et al. Irreversible Electroporation to Treat Unresectable Colorectal Liver Metastases (COLDFIRE-2): A Phase II, Two-Center, Single-Arm Clinical Trial. Radiology 2021, 299, 470–480. [Google Scholar] [CrossRef]
- Wang, X.; Sofocleous, C.T.; Erinjeri, J.P.; Petre, E.N.; Gonen, M.; Do, K.G.; Brown, K.T.; Covey, A.M.; Brody, L.A.; Alago, W.; et al. Margin size is an independent predictor of local tumor progression after ablation of colon cancer liver metastases. CardioVasc. Interv. Radiol. 2013, 36, 166–175. [Google Scholar] [CrossRef]
- Solbiati, M.; Muglia, R.; Goldberg, S.N.; Ierace, T.; Rotilio, A.; Passera, K.M.; Marre, I.; Solbiati, L. A novel software platform for volumetric assessment of ablation completeness. Int. J. Hyperth. 2019, 36, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Kaye, E.A.; Cornelis, F.H.; Petre, E.N.; Tyagi, N.; Shady, W.; Shi, W.; Zhang, Z.; Solomon, S.B.; Sofocleous, C.T.; Durack, J.C. Volumetric 3D assessment of ablation zones after thermal ablation of colorectal liver metastases to improve prediction of local tumor progression. Eur. Radiol. 2019, 29, 2698–2705. [Google Scholar] [CrossRef] [PubMed]
- Laimer, G.; Jaschke, N.; Schullian, P.; Putzer, D.; Eberle, G.; Solbiati, M.; Solbiati, L.; Goldberg, S.N.; Bale, R. Volumetric assessment of the periablational safety margin after thermal ablation of colorectal liver metastases. Eur. Radiol. 2021, 31, 6489–6499. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Singh, T.; Soni, S. Pre-operative Assessment of Ablation Margins for Variable Blood Perfusion Metrics in a Magnetic Resonance Imaging Based Complex Breast Tumour Anatomy: Simulation Paradigms in Thermal Therapies. Comput. Methods Programs Biomed. 2021, 198, 105781. [Google Scholar] [CrossRef]
- Singh, M. Quantitative evaluation of effects of coupled temperature elevation, thermal damage, and enlarged porosity on nanoparticle migration in tumors during magnetic nanoparticle hyperthermia. Int. Commun. Heat. Mass. Transf. 2021, 126, 105393. [Google Scholar] [CrossRef]
- van Tilborg, A.A.; Scheffer, H.J.; van der Meijs, B.B.; van Werkum, M.H.; Melenhorst, M.C.; van den Tol, P.M.; Meijerink, M.R. Transcatheter CT hepatic arteriography-guided percutaneous ablation to treat ablation site recurrences of colorectal liver metastases: The incomplete ring sign. J. Vasc. Interv. Radiol. 2015, 26, 583–587. [Google Scholar] [CrossRef]
- Puijk, R.S.; Ruarus, A.H.; Scheffer, H.J.; Vroomen, L.; van Tilborg, A.; de Vries, J.J.J.; Berger, F.H.; van den Tol, P.M.P.; Meijerink, M.R. Percutaneous Liver Tumour Ablation: Image Guidance, Endpoint Assessment, and Quality Control. Can. Assoc. Radiol. J. 2018, 69, 51–62. [Google Scholar] [CrossRef]
- van der Lei, S.; Opperman, J.; Dijkstra, M.; Kors, N.; Boon, R.; van den Bemd, B.A.T.; Timmer, F.E.F.; Nota, I.; van den Bergh, J.E.; de Vries, J.J.J.; et al. The Added Diagnostic Value of Transcatheter CT Hepatic Arteriography for Intraprocedural Detection of Previously Unknown Colorectal Liver Metastases During Percutaneous Ablation and Impact on the Definitive Treatment Plan. CardioVasc. Interv. Radiol. 2023. [Google Scholar] [CrossRef]
- Schullian, P.; Laimer, G.; Johnston, E.; Putzer, D.; Eberle, G.; Scharll, Y.; Widmann, G.; Kolbitsch, C.; Bale, R. Technical efficacy and local recurrence after stereotactic radiofrequency ablation of 2653 liver tumors: A 15-year single-center experience with evaluation of prognostic factors. Int. J. Hyperth. 2022, 39, 421–430. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total N = 280 | Small N = 221 | Intermediate N = 59 | p-Value | ||
|---|---|---|---|---|---|
| Patient-Related Characteristics | |||||
| Gender | Male | 69.3 | 67.9 | 74.6 | |
| Female | 30.7 | 32.1 | 25.4 | 0.346 a | |
| Age (years) | Mean (SD) | 65.6 (11.1) | 65.3 (11.2) | 66.8 (10.6) | 0.365 b |
| ASA physical status | 1 | 6.5 | 6.9 | 5.3 | |
| 2 | 69.8 | 72.9 | 57.9 | ||
| 3 | 23.3 | 19.7 | 36.8 | ||
| 4 | 0.4 | 0.5 | 0.0 | 0.055 c | |
| Comorbidities | None | 49.8 | 52.1 | 41.4 | |
| Minimal | 35.0 | 36.1 | 31.0 | ||
| Major | 15.2 | 11.9 | 27.6 | 0.012 c | |
| Disease-related characteristics | |||||
| Primary tumor location | Right-sided colon | 21.8 | 21.7 | 22.0 | |
| Left-sided colon | 47.1 | 48.0 | 44.1 | ||
| Rectum | 31.1 | 30.3 | 33.9 | 0.842 c | |
| Molecular profile | RASwt/mut/unknown | 11.4/7.1/81.5 | 11.3/7.7/81.0 | 11.9/33.9/54.2 | 0.196 c |
| BRAFwt/mut/unknown | 16.8/1.1/82.1 | 17.2/1.4/81.4 | 15.3/1.7/83.0 | 0.236 c | |
| MSS/MSI/unknown | 29.6/0.4/73.0 | 30.3/0.5/69.2 | 27.1/0.0/72.9 | 0.624 c | |
| Time interval to diagnosis CRLM | Metachronous | 44.2 | 40.8 | 57.4 | |
| Synchronous | 55.8 | 59.2 | 42.6 | 0.032 c | |
| Extrahepatic disease at first diagnosis of CRLM | No | 93.2 | 93.1 | 93.6 | |
| Yes | 6.8 | 6.9 | 6.4 | 1.000 c | |
| Total N = 347 | Small N = 287 | Intermediate N = 60 | p-Value | ||
| Procedure-Related Characteristics | |||||
| Preprocedural chemotherapy | No | 67.8 | 67.2 | 72.1 | |
| Yes | 32.2 | 32.8 | 27.9 | 0.603 a | |
| Procedure number in course of treatment | 1st | 57.3 | 56.1 | 65.9 | |
| 2nd–5th | 40.9 | 41.9 | 34.1 | ||
| >5th | 1.7 | 2.0 | 0.0 | 0.352 b | |
| Number of tumors | 1 | 50.1 | 46.2 | 77.3 | |
| 2–5 | 39.5 | 41.9 | 22.7 | ||
| >5 | 10.4 | 11.9 | 0.0 | <0.001 b | |
| Ablation technique | RFA | 34.9 | 33.0 | 47.7 | |
| MWA | 65.1 | 67.0 | 52.3 | 0.063 a | |
| Ablation modality | RFA | ||||
| RF3000™, LeVeen™ | 29.2 | 27.1 | 43.2 | ||
| Cool-tip™ | 3.5 | 4.1 | 0.0 | ||
| Starburst® (RITA®) | 1.2 | 1.0 | 2.3 | ||
| Others | 0.6 | 0.3 | 2.3 | ||
| MWA | |||||
| Evident™ | 2.1 | 2.0 | 2.3 | ||
| Emprint™ | 54.0 | 55.9 | 40.9 | ||
| Solero™ | 0.3 | 0.0 | 0.3 | ||
| Others | 9.1 | 9.2 | 9.1 | 0.268 b | |
| Approach | Open | 30.3 | 28.7 | 40.9 | |
| Percutaneous | 69.7 | 71.3 | 59.1 | 0.115 a | |
| Image-guidance technique | Conventional * | 48.4 | 47.2 | 56.8 | |
| CTHA | 51.6 | 52.8 | 43.2 | 0.261 a | |
| Anesthesia | Midazolam sedation | 8.7 | 9.0 | 6.8 | |
| Propofol sedation | 38.6 | 39.5 | 31.8 | ||
| General anesthesia | 52.8 | 51.5 | 61.4 | 0.471 b | |
| Total N = 856 | Small N = 783 | Intermediate N = 73 | p-Value | ||
| Tumor-Related Characteristics | |||||
| Size (mm) | Median (IQR) | 15.0 (9.0–22.0) | 13.0 (8.0–20.0) | 36.0 (33.0–40.5) | <0.001 c |
| Margin size (mm) | 0–5 | 6.5 | 5.8 | 14.5 | |
| >5 | 93.5 | 94.2 | 58.5 | 0.020 a | |
| Total N = 280 | Small N = 221 | Intermediate N = 59 | p-Value | |
|---|---|---|---|---|
| Complications | ||||
| Grade 1 | 3.6 | 3.6 | 3.4 | |
| Grade 2 | 6.1 | 6.8 | 3.4 | |
| Grade 3 | 5.0 | 4.1 | 8.5 | |
| Grade 4 | 0.4 | 0.5 | 0.0 | |
| Grade 5 | 0.0 | 0.0 | 0.0 | 0.546 a |
| Length of hospital stay | 1.0 (1.0–4.8) | 1.0 (1.0–4.0) | 4.0 (1.0–5.0) | 0.002 b |
| Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Size | Small | Reference | <0.001 | Reference | 0.004 |
| Intermediate | 5.383 (2.303–12.584) | 3.744 (1.537–9.125) | |||
| Patient-related characteristics | |||||
| Gender | Male | Reference | 0.025 | Reference | 0.008 |
| Female | 2.497 (1.120–5.569) | 2.980 (1.326–6.695) | |||
| Age | 1.043 (1.002–1.086) | 0.040 | 1.027 (0.980–1.077) | 0.266 | |
| ASA physical status | 1 | Reference | 0.444 | ||
| 2 | NA | ||||
| 3 | NA | ||||
| 4 | NA | ||||
| Comorbidities | None | Reference | 0.211 | ||
| Minimal | 0.651 (0.251–1.685) | ||||
| Major | 1.860 (0.641–5.394) | ||||
| Disease-related characteristics | |||||
| Primary tumor location | Right-sided colon | Reference | 0.793 | ||
| Left-sided colon | 0.901 (0.339–2.392) | ||||
| Rectum | 0.673 (0.205–2.208) | ||||
| First diagnosis of CRLM | Metachronous | Reference | 0.122 | ||
| Synchronous | 0.508 (0.215–1.199) | ||||
| Extrahepatic disease at first diagnosis of CRLM | No | Reference | 0.345 | ||
| Yes | 2.035 (0.465–8.899) | ||||
| Procedure-related characteristics | |||||
| Preprocedural chemotherapy | No | Reference | 0.287 | ||
| Yes | 0.633 (0.272–1.470) | ||||
| Procedure number in course of treatment | 1st | Reference | 0.223 | ||
| 2nd–5th | 2.044 (0.911–4.586) | ||||
| >5th | NA | ||||
| Number of tumors | 1 | Reference | <0.001 | Reference | 0.003 |
| 2–5 | 0.247 (0.098–0.620) | 0.281 (0.109–0.721) | |||
| >5 | 0.142 (0.046–0.437) | 0.183 (0.057–0.588) | |||
| Ablation technique | RFA | Reference | 0.916 | ||
| MWA | 0.954 (0.403–2.263) | ||||
| Approach | Open | Reference | 0.260 | ||
| Percutaneous | 1.264 (0.841–1.900) | ||||
| Image-guidance technique | Conventional * | Reference | 0.832 | ||
| CTHA | 1.097 (0.465–2.585) | ||||
| Anesthesia | Midazolam sedation | Reference | 0.116 | ||
| Propofol sedation | 0.185 (0.035–0.988) | ||||
| General anesthesia | 0.453 (0.164–1.250) | ||||
| Tumor-related characteristics | |||||
| Margin size | <5 mm | Reference | 0.008 | Reference | 0.138 |
| >5 mm | 0.221 (0.07–0.679) | 0.384 (0.109–1.359) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dijkstra, M.; van der Lei, S.; Puijk, R.S.; Schulz, H.H.; Vos, D.J.W.; Timmer, F.E.F.; Scheffer, H.J.; Buffart, T.E.; van den Tol, M.P.; Lissenberg-Witte, B.I.; et al. Efficacy of Thermal Ablation for Small-Size (0–3 cm) versus Intermediate-Size (3–5 cm) Colorectal Liver Metastases: Results from the Amsterdam Colorectal Liver Met Registry (AmCORE). Cancers 2023, 15, 4346. https://doi.org/10.3390/cancers15174346
Dijkstra M, van der Lei S, Puijk RS, Schulz HH, Vos DJW, Timmer FEF, Scheffer HJ, Buffart TE, van den Tol MP, Lissenberg-Witte BI, et al. Efficacy of Thermal Ablation for Small-Size (0–3 cm) versus Intermediate-Size (3–5 cm) Colorectal Liver Metastases: Results from the Amsterdam Colorectal Liver Met Registry (AmCORE). Cancers. 2023; 15(17):4346. https://doi.org/10.3390/cancers15174346
Chicago/Turabian StyleDijkstra, Madelon, Susan van der Lei, Robbert S. Puijk, Hannah H. Schulz, Danielle J. W. Vos, Florentine E. F. Timmer, Hester J. Scheffer, Tineke E. Buffart, M. Petrousjka van den Tol, Birgit I. Lissenberg-Witte, and et al. 2023. "Efficacy of Thermal Ablation for Small-Size (0–3 cm) versus Intermediate-Size (3–5 cm) Colorectal Liver Metastases: Results from the Amsterdam Colorectal Liver Met Registry (AmCORE)" Cancers 15, no. 17: 4346. https://doi.org/10.3390/cancers15174346
APA StyleDijkstra, M., van der Lei, S., Puijk, R. S., Schulz, H. H., Vos, D. J. W., Timmer, F. E. F., Scheffer, H. J., Buffart, T. E., van den Tol, M. P., Lissenberg-Witte, B. I., Swijnenburg, R.-J., Versteeg, K. S., & Meijerink, M. R. (2023). Efficacy of Thermal Ablation for Small-Size (0–3 cm) versus Intermediate-Size (3–5 cm) Colorectal Liver Metastases: Results from the Amsterdam Colorectal Liver Met Registry (AmCORE). Cancers, 15(17), 4346. https://doi.org/10.3390/cancers15174346