
Clinico-Pathological Features, Outcomes and Impacts of COVID-19 Pandemic on Patients with Early-Onset Colorectal Cancer: A Single-Institution Experience
 , ,
, ,  , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, F.A. Increasing Incidence of Early-Onset Colorectal Cancer. N. Engl. J. Med. 2022, 386, 1547–1558. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Araghi, M.; Soerjomataram, I.; Bardot, A.; Ferlay, J.; Cabasag, C.J.; Morrison, D.S.; De, P.; Tervonen, H.; Walsh, P.M.; Bucher, O.; et al. Changes in colorectal cancer incidence in seven high-income countries: A population-based study. Lancet Gastroenterol. Hepatol. 2019, 4, 511–518, Erratum in Lancet Gastroenterol. Hepatol. 2019, 4, e8. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Huang, J.; Lok, V.; Wang, J.; Fung, F.; Ding, H.; Zheng, Z.-J. Differences in Incidence and Mortality Trends of Colorectal Cancer Worldwide Based on Sex, Age, and Anatomic Location. Clin. Gastroenterol. Hepatol. 2021, 19, 955–966.e61. [Google Scholar] [CrossRef]
- Peterse, E.F.P.; Meester, R.G.S.; Siegel, R.L.; Chen, J.C.; Dwyer, A.; Ahnen, D.J.; Smith, R.A.; Zauber, A.G.; Lansdorp-Vogelaar, I. The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: Microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline. Cancer 2018, 124, 2964–2973. [Google Scholar] [CrossRef]
- U.S. Preventive Services Task Force. Draft Recommendation Statement. Colorectal Cancer: Screening. October 27, 2020. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/document/RecommendationStatementDraft/colorectal-cancer-screening (accessed on 7 April 2022).
- Nguyen, L.H.; Liu, P.-H.; Zheng, X.; Keum, N.; Zong, X.; Li, X.; Wu, K.; Fuchs, C.S.; Ogino, S.; Ng, K.; et al. Sedentary Behaviors, TV Viewing Time, and Risk of Young-Onset Colorectal Cancer. JNCI Cancer Spectr. 2018, 2, pky073. [Google Scholar] [CrossRef]
- Rosato, V.; Bosetti, C.; Levi, F.; Polesel, J.; Zucchetto, A.; Negri, E.; La Vecchia, C. Risk factors for young-onset colorectal cancer. Cancer Causes Control 2013, 24, 335–341. [Google Scholar] [CrossRef]
- Rueda, M.; Robertson, Y.; Acott, A.; Rueda, S.; Keikhoff, A.; Guerrero, W.; Mancino, A.T. Association of tobacco and alcohol use with earlier development of colorectal pathology: Should screening guidelines be modified to include these risk factors? Am. J. Surg. 2012, 204, 963–968. [Google Scholar] [CrossRef]
- Gausman, V.; Dornblaser, D.; Anand, S.; Hayes, R.B.; O’Connell, K.; Du, M.; Liang, P.S. Risk Factors Associated With Early-Onset Colorectal Cancer. Clin. Gastroenterol. Hepatol. 2020, 18, 2752–2759.e2. [Google Scholar] [CrossRef]
- O’sullivan, D.E.; Sutherland, R.L.; Town, S.; Chow, K.; Fan, J.; Forbes, N.; Heitman, S.J.; Hilsden, R.J.; Brenner, D.R. Risk Factors for Early-Onset Colorectal Cancer: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 1229–1240.e5. [Google Scholar] [CrossRef] [PubMed]
- Burnett-Hartman, A.N.; Lee, J.K.; Demb, J.; Gupta, S. An Update on the Epidemiology, Molecular Characterization, Diagnosis, and Screening Strategies for Early-Onset Colorectal Cancer. Gastroenterology 2021, 160, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Di Leo, M.; Zuppardo, R.A.; Puzzono, M.; Ditonno, I.; Mannucci, A.; Antoci, G.; Raucci, A.R.; Patricelli, M.G.; Elmore, U.; Tamburini, A.M.; et al. Risk factors and clinical characteristics of early-onset colorectal cancer vs. late-onset colorectal cancer: A case-case study. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1153–1160. [Google Scholar] [CrossRef]
- Archambault, A.N.; Su, Y.-R.; Jeon, J.; Thomas, M.; Lin, Y.; Conti, D.V.; Win, A.K.; Sakoda, L.C.; Lansdorp-Vogelaar, I.; Peterse, E.F.; et al. Cumulative Burden of Colorectal Cancer–Associated Genetic Variants Is More Strongly Associated With Early-Onset vs Late-Onset Cancer. Gastroenterology 2020, 158, 1274–1286.e12. [Google Scholar] [CrossRef] [PubMed]
- Myers, E.A.; Feingold, D.L.; Forde, K.A.; Arnell, T.; Jang, J.H.; Whelan, R.L. Colorectal cancer in patients under 50 years of age: A retrospective analysis of two institutions’ experience. World J. Gastroenterol. 2013, 19, 5651–5657. [Google Scholar] [CrossRef] [PubMed]
- Kneuertz, P.J.; Chang, G.J.; Hu, C.-Y.; Rodriguez-Bigas, M.A.; Eng, C.; Vilar, E.; Skibber, J.M.; Feig, B.W.; Cormier, J.N.; You, Y.N. Overtreatment of young adults with colon cancer: More intense treatments with unmatched survival gains. JAMA Surg. 2015, 150, 402–409. [Google Scholar] [CrossRef]
- Chen, F.W.; Sundaram, V.; Chew, T.A.; Ladabaum, U. Advanced-Stage Colorectal Cancer in Persons Younger Than 50 Years Not Associated With Longer Duration of Symptoms or Time to Diagnosis. Clin. Gastroenterol. Hepatol. 2017, 15, 728–737.e3. [Google Scholar] [CrossRef]
- Lieu, C.H.; Renfro, L.A.; de Gramont, A.; Meyers, J.P.; Maughan, T.S.; Seymour, M.T.; Saltz, L.; Goldberg, R.M.; Sargent, D.J.; Eckhardt, S.G.; et al. Association of age with survival in patients with metastatic colorectal cancer: Analysis from the ARCAD Clinical Trials Program. J. Clin. Oncol. 2014, 32, 2975–2982. [Google Scholar] [CrossRef]
- Willauer, A.N.; Liu, Y.; Pereira, A.A.L.; Lam, M.; Morris, J.S.; Raghav, K.P.S.; Morris, V.K.; Menter, D.; Broaddus, R.; Meric-Bernstam, F.; et al. Clinical and molecular characterization of early-onset colorectal cancer. Cancer 2019, 125, 2002–2010. [Google Scholar] [CrossRef]
- Antelo, M.; Balaguer, F.; Shia, J.; Shen, Y.; Hur, K.; Moreira, L.; Cuatrecasas, M.; Bujanda, L.; Giraldez, M.D.; Takahashi, M.; et al. A high degree of LINE-1 hypomethylation is a unique feature of early-onset colorectal cancer. PLoS ONE 2012, 7, e45357. [Google Scholar] [CrossRef]
- Pearlman, R.; Frankel, W.L.; Swanson, B.; Zhao, W.; Yilmaz, A.; Miller, K.; Bacher, J.; Bigley, C.; Nelsen, L.; Goodfellow, P.J.; et al. Prevalence and Spectrum of Germline Cancer Susceptibility Gene Mutations Among Patients With Early-Onset Colorectal Cancer. JAMA Oncol. 2017, 3, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Rho, Y.S.; Gilabert, M.; Polom, K.; Aladashvili, A.; Kopeckova, K.; Megdanova, V.; Coleman, N.; Greally, M.; Marrelli, D.; Roviello, F.; et al. Comparing Clinical Characteristics and Outcomes of Young-onset and Late-onset Colorectal Cancer: An International Collaborative Study. Clin. Color. Cancer 2017, 16, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Blanke, C.D.; Bot, B.M.; Thomas, D.M.; Bleyer, A.; Kohne, C.-H.; Seymour, M.T.; de Gramont, A.; Goldberg, R.M.; Sargent, D.J. Impact of young age on treatment efficacy and safety in advanced colorectal cancer: A pooled analysis of patients from nine first-line phase III chemotherapy trials. J. Clin. Oncol. 2011, 29, 2781–2786. [Google Scholar] [CrossRef] [PubMed]
- Quah, H.M.; Joseph, R.; Schrag, D.; Shia, J.; Guillem, J.G.; Paty, P.B.; Temple, L.K.; Wong, W.D.; Weiser, M.R. Young Age Influences Treatment but not Outcome of Colon Cancer. Ann. Surg. Oncol. 2007, 14, 2759–2765. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.-J.; Ping, J.; Li, Y.; Adell, G.; Arbman, G.; Nodin, B.; Meng, W.-J.; Zhang, H.; Yu, Y.-Y.; Wang, C.; et al. The prognostic factors and multiple biomarkers in young patients with colorectal cancer. Sci. Rep. 2015, 5, 10645. [Google Scholar] [CrossRef]
- Myer, P.A.; Lee, J.K.; Madison, R.W.; Pradhan, K.; Newberg, J.Y.; Isasi, C.R.; Klempner, S.J.; Frampton, G.M.; Ross, J.S.; Venstrom, J.M.; et al. The Genomics of Colorectal Cancer in Populations with African and European Ancestry. Cancer Discov. 2022, 12, 1282–1293. [Google Scholar] [CrossRef]
- Cathomas, G. PIK3CA in Colorectal Cancer. Front. Oncol. 2014, 4, 35. [Google Scholar] [CrossRef]
- Khelwatty, S.A.; Puvanenthiran, S.; Essapen, S.; Bagwan, I.; Seddon, A.M.; Modjtahedi, H. HER2 Expression Is Predictive of Survival in Cetuximab Treated Patients with RAS Wild Type Metastatic Colorectal Cancer. Cancers 2021, 13, 638. [Google Scholar] [CrossRef]
- Vidal, J.; Bellosillo, B.; Santos Vivas, C.; García-Alfonso, P.; Carrato, A.; Cano, M.; García-Carbonero, R.; Élez, E.; Losa, F.; Massutí, B.; et al. Ultra-selection of metastatic colorectal cancer patients using next-generation sequencing to improve clinical efficacy of anti-EGFR therapy. Ann. Oncol. 2019, 30, 439–446. [Google Scholar] [CrossRef]
- Randon, G.; Maddalena, G.; Germani, M.M.; Pircher, C.C.; Manca, P.; Bergamo, F.; Giordano, M.; Sposetti, C.; Montagna, A.; Vetere, G.; et al. Negative Ultraselection of Patients With RAS/BRAF Wild-Type, Microsatellite-Stable Metastatic Colorectal Cancer Receiving Anti–EGFR-Based Therapy. JCO Precis. Oncol. 2022, 6, e2200037, Erratum in JCO Precis. Oncol. 2022, 6, e2200356. [Google Scholar] [CrossRef]
- Mazidimoradi, A.; Tiznobaik, A.; Salehiniya, H. Impact of the COVID-19 Pandemic on Colorectal Cancer Screening: A Systematic Review. J. Gastrointest. Cancer 2022, 53, 730–744. [Google Scholar] [CrossRef] [PubMed]
- Mentrasti, G.; Cantini, L.; Zichi, C.; D’ostilio, N.; Gelsomino, F.; Martinelli, E.; Chiari, R.; La Verde, N.; Bisonni, R.; Cognigni, V.; et al. Alarming Drop in Early Stage Colorectal Cancer Diagnoses After COVID-19 Outbreak: A Real-World Analysis from the Italian COVID-DELAY Study. Oncologist 2022, 27, e723–e730. [Google Scholar] [CrossRef] [PubMed]
- Teglia, F.; Angelini, M.; Astolfi, L.; Casolari, G.; Boffetta, P. Global Association of COVID-19 Pandemic Measures With Cancer Screening: A Systematic Review and Meta-analysis. JAMA Oncol. 2022, 8, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Baraibar, I.; García, A.; Salvà, F.; Ros, J.; Saoudi, N.; Comas, R.; Castillo, G.; Sanchis, M.; García-Álvarez, A.; Hernando, J.; et al. Impact of the COVID-19 pandemic in the early-onset colorectal cancer. Transl. Oncol. 2023, 32, 101668. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, W. Cancer diagnostic delay in the COVID-19 era: What happens next? Lancet Oncol. 2020, 21, 1000–1002. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Banerjee, S.; Cervantes, A.; Garassino, M.C.; Garrido, P.; Girard, N.; Haanen, J.; Jordan, K.; Lordick, F.; Machiels, J.P.; et al. Managing cancer patients during the COVID-19 pandemic: An ESMO multidisciplinary expert consensus. Ann. Oncol. 2020, 31, 1320–1335. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | <50 Years Old (n = 80) | ≥50 Years Old (n = 1395) | p Value |
|---|---|---|---|
| Sex (female), n (%) | 33 (41.3%) | 573 (41.1%) | 0.975 |
| Age, mean (SD) | 44.9 (4.2%) | 73 (10.5%) | 0.001 |
| ECOG PS 0-1 (compared to 2-4) n (%) | 73 (93.6%) | 1182 (87.8%) | 0.122 |
| BMI, n (%) | 0.007 | ||
|
|
| |
|
|
| |
|
|
| |
|
|
| |
| Primary tumor location, n (%) | 0.34 | ||
|
|
| |
|
|
| |
|
|
| |
| T stage at diagnosis, n (%) | 0.050 | ||
|
|
| |
|
|
| |
|
|
| |
|
|
| |
| N stage at diagnosis, n (%) | 0.001 | ||
|
|
| |
|
|
| |
|
|
| |
| Stage, n (%) | 0.002 | ||
|
|
| |
|
|
| |
|
|
| |
|
|
| |
| Stage IV at diagnosis, n (%) |
|
| 0.005 |
| Lymphovascular invasion, n (%) * | 29 (46%) | 420 (38%) | 0.171 |
| Perineural invasion, n (%) * | 21 (34%) | 246 (22%) | 0.029 |
| Budding, n (%) * | 0.050 | ||
|
|
| |
|
|
| |
| Mucinous histology, n (%) | 13 (18%) | 156 (12%) | 0.160 |
| Signet ring cell, n (%) | 5 (6%) | 30 (2%) | 0.020 |
| High grade (G3), n (%) | 13 (18%) | 98 (8%) | 0.004 |
| Deficient mismatch repair, n (%) | 11 (14%) | 115 (9%) | 0.120 |
| Mutational profile, n (%) | 0.020 | ||
|
|
| |
|
|
| |
|
|
| |
|
|
| |
| Treatment: | |||
|
|
| 0.490 |
|
|
| <0.001 |
|
|
| <0.001 |
|
|
| <0.001 |
| Pre-Pandemic Group (n = 55) | Post-Pandemic Group (n = 20) | p Value | |
|---|---|---|---|
| T4, n (%) * | 13 (34%) | 3 (60%) | 0.344 |
| Lymph node positive, n (%) * | 25 (65%) | 3 (60%) | 1.000 |
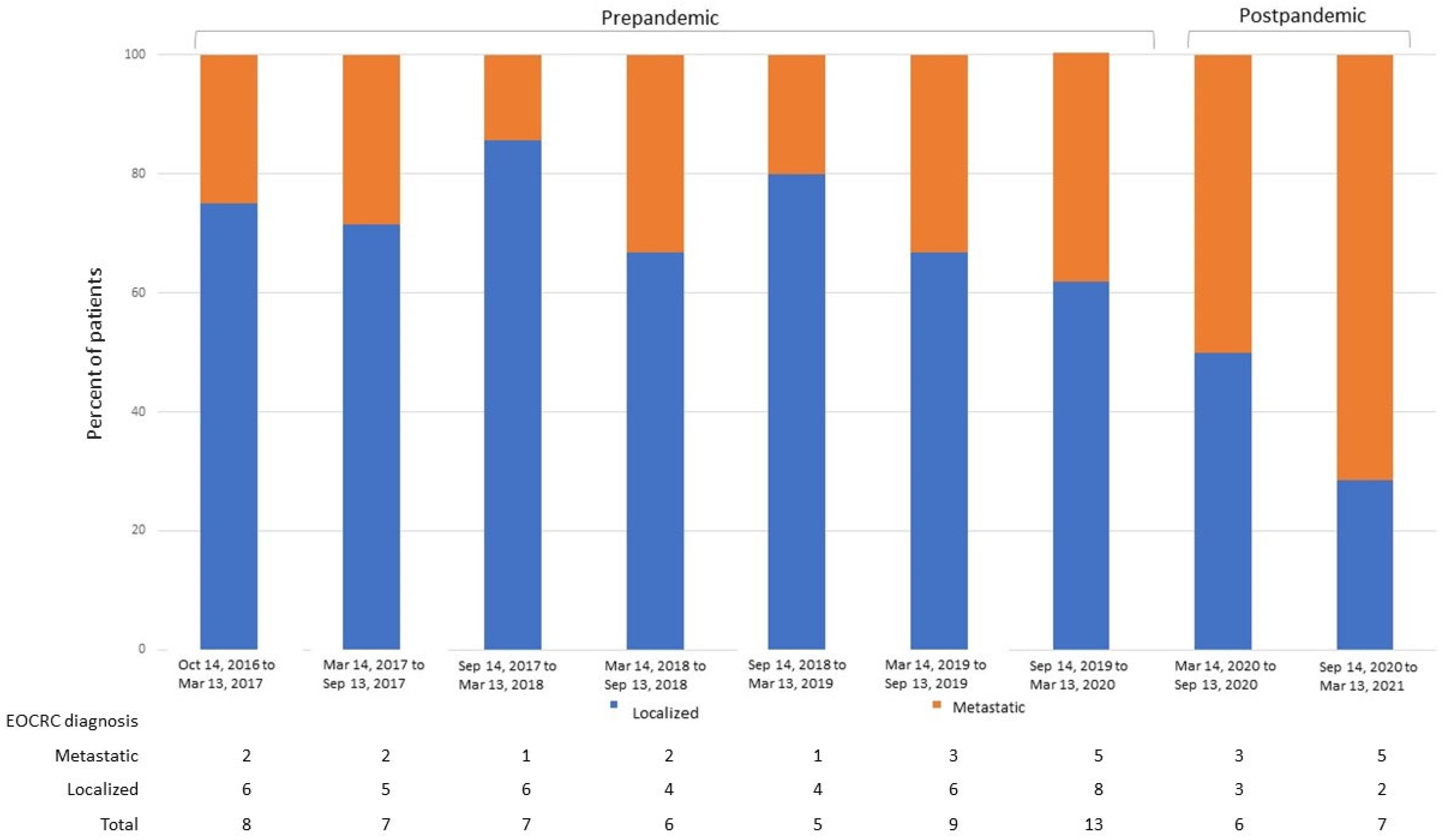
| Metastasic disease at diagnosis, n (%) | 16 (29%) | 8 (61%) | 0.028 |
| Margins affected, n (%) * | 4 (8%) | 2 (28%) | 0.17 |
| Bowel obstruction at diagnosis * | 4 (7%) | 0 (0%) | 1.000 |
| Bowel perforation at diagnosis * | 2 (3%) | 0 (0%) | 1.000 |
| Lymphovascular invasion, n (%) * | 19 (43%) | 5 (71%) | 0.232 |
| Perineural invasion, n (%) * | 14 (31%) | 4 (57%) | 0.226 |
| High tumoral budding, n (%) * | 15 (53%) | 5 (83%) | 0.364 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Perez, D.; Viñal, D.; Peña-Lopez, J.; Jimenez-Bou, D.; Ruiz-Gutierrez, I.; Martinez-Recio, S.; Alameda-Guijarro, M.; Rueda-Lara, A.; Martin-Montalvo, G.; Ghanem, I.; et al. Clinico-Pathological Features, Outcomes and Impacts of COVID-19 Pandemic on Patients with Early-Onset Colorectal Cancer: A Single-Institution Experience. Cancers 2023, 15, 4242. https://doi.org/10.3390/cancers15174242
Martinez-Perez D, Viñal D, Peña-Lopez J, Jimenez-Bou D, Ruiz-Gutierrez I, Martinez-Recio S, Alameda-Guijarro M, Rueda-Lara A, Martin-Montalvo G, Ghanem I, et al. Clinico-Pathological Features, Outcomes and Impacts of COVID-19 Pandemic on Patients with Early-Onset Colorectal Cancer: A Single-Institution Experience. Cancers. 2023; 15(17):4242. https://doi.org/10.3390/cancers15174242
Chicago/Turabian StyleMartinez-Perez, Daniel, David Viñal, Jesús Peña-Lopez, Diego Jimenez-Bou, Iciar Ruiz-Gutierrez, Sergio Martinez-Recio, María Alameda-Guijarro, Antonio Rueda-Lara, Gema Martin-Montalvo, Ismael Ghanem, and et al. 2023. "Clinico-Pathological Features, Outcomes and Impacts of COVID-19 Pandemic on Patients with Early-Onset Colorectal Cancer: A Single-Institution Experience" Cancers 15, no. 17: 4242. https://doi.org/10.3390/cancers15174242
APA StyleMartinez-Perez, D., Viñal, D., Peña-Lopez, J., Jimenez-Bou, D., Ruiz-Gutierrez, I., Martinez-Recio, S., Alameda-Guijarro, M., Rueda-Lara, A., Martin-Montalvo, G., Ghanem, I., Custodio, A. B., Trilla-Fuertes, L., Gamez-Pozo, A., Barbachano, A., Rodriguez-Cobos, J., Bustamante-Madrid, P., Fernandez-Barral, A., Burgos, A., Prieto-Nieto, M. I., ... Rodríguez-Salas, N. (2023). Clinico-Pathological Features, Outcomes and Impacts of COVID-19 Pandemic on Patients with Early-Onset Colorectal Cancer: A Single-Institution Experience. Cancers, 15(17), 4242. https://doi.org/10.3390/cancers15174242