
Comparison of Long-Term Oncological Results in Young Women with Breast Cancer between BRCA-Mutation Carriers Versus Non-Carriers: How Tumor and Genetic Risk Factors Influence the Clinical Prognosis
 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Management of BRCA-Mutation Carriers
2.2. Endpoints and Definitions
2.3. Statistical Analysis
3. Results
3.1. Comparison of Characteristics in Young Women with Breast Cancer
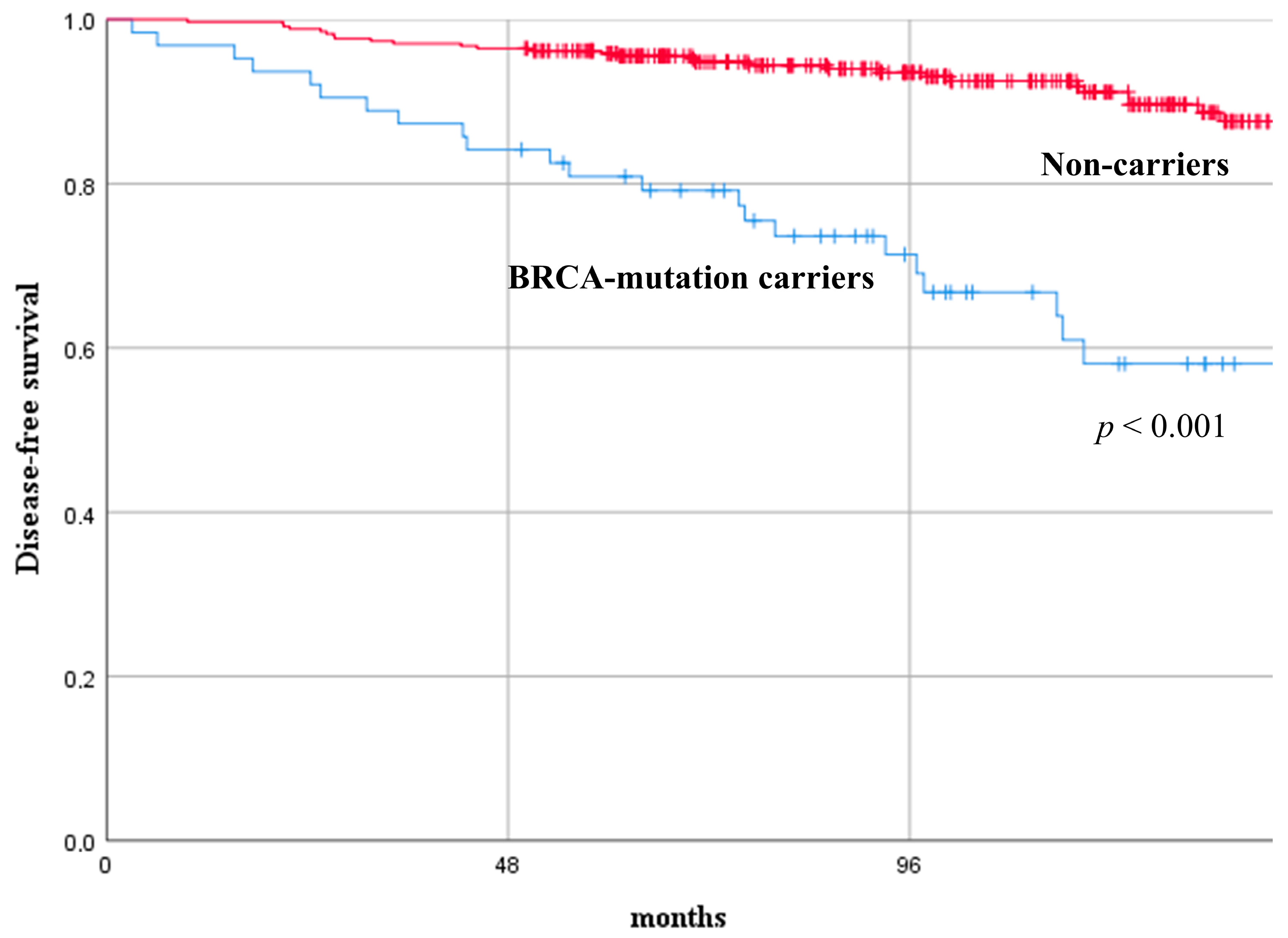
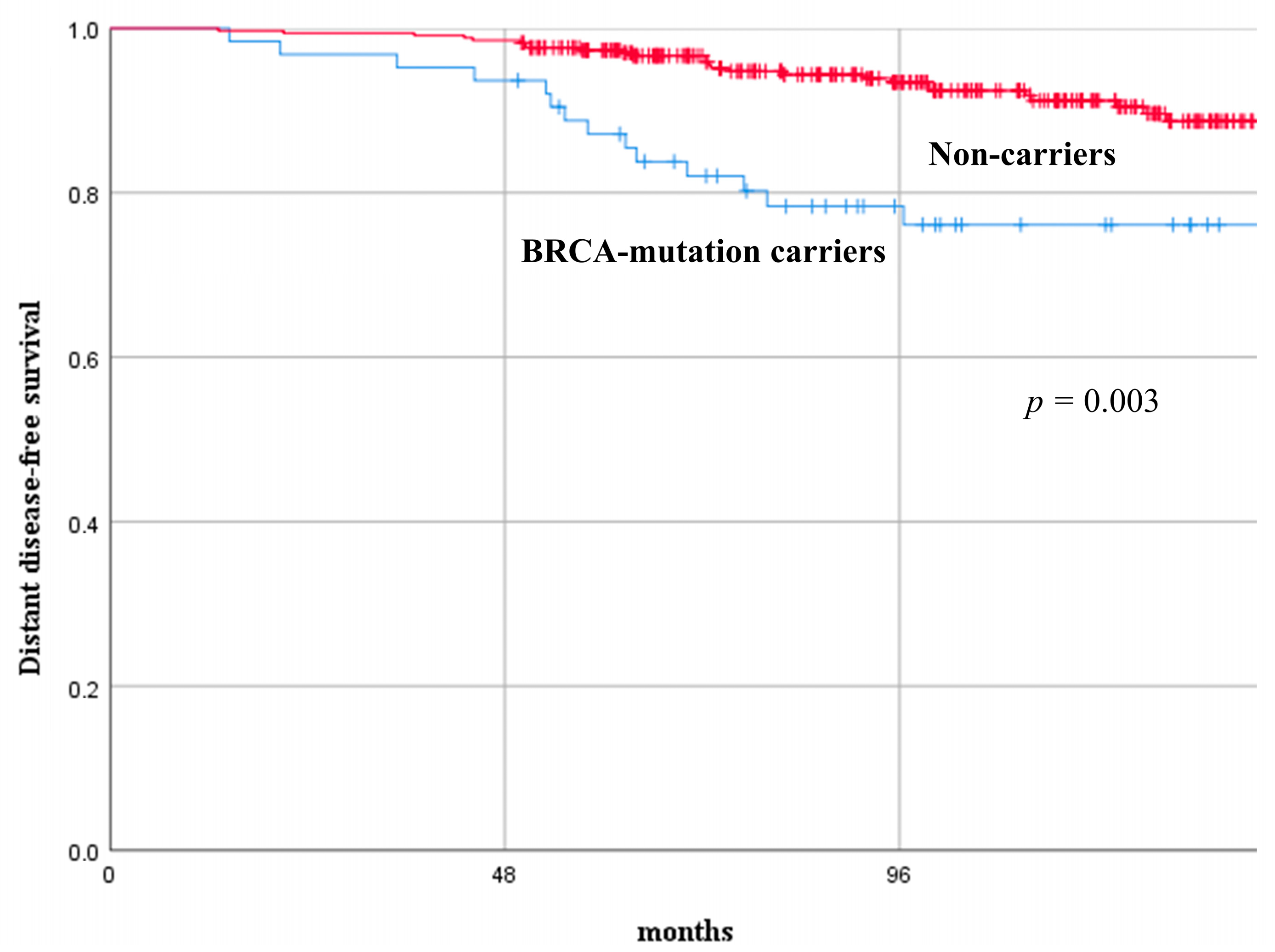
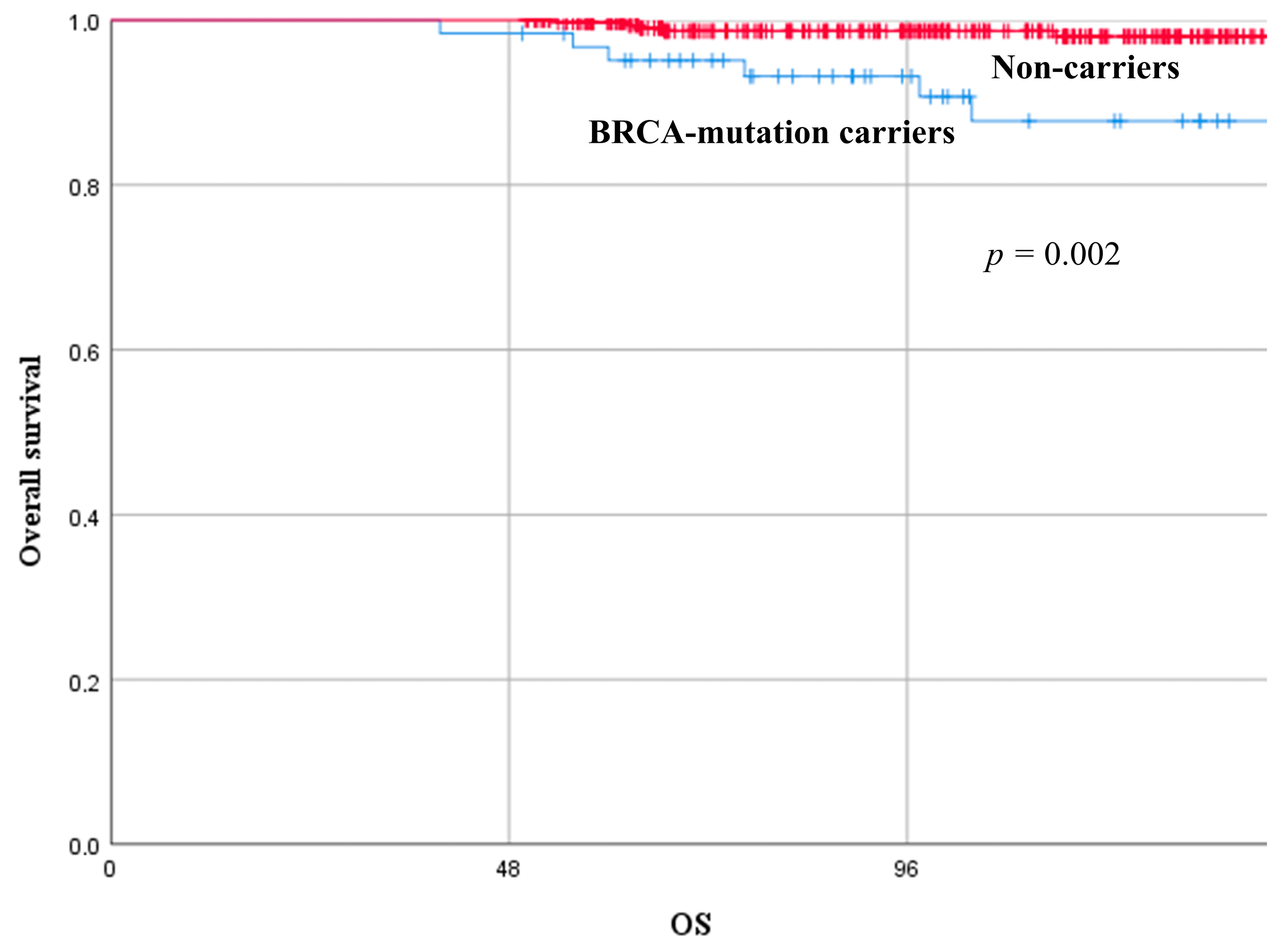
3.2. Long-Term Oncological Results and Independent Predictive Factors for Clinical Prognosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Breast cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed]
- Ellington, T.D.; Miller, J.W.; Henley, S.J.; Wilson, R.J.; Wu, M.; Richardson, L.C. Trends in Breast Cancer Incidence, by Race, Ethnicity, and Age Among Women Aged ≥ 20 Years—United States, 1999–2018. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 43–47. [Google Scholar] [CrossRef]
- Villarreal-Garza, C.; Aguila, C.; Magallanes-Hoyos, M.C.; Mohar, A.; Bargalló, E.; Meneses, A.; Cazap, E.; Gomez, H.; López-Carrillo, L.; Chávarri-Guerra, Y.; et al. Breast Cancer in Young Women in Latin America: An Unmet, Growing Burden. Oncologist 2013, 18, 1298–1306. [Google Scholar] [CrossRef]
- Schaffar, R.; Bouchardy, C.; Chappuis, P.O.; Bodmer, A.; Benhamou, S.; Rapiti, E. A population-based cohort of young women diagnosed with breast cancer in Geneva, Switzerland. PLoS ONE 2019, 14, e0222136. [Google Scholar] [CrossRef]
- Fazel, A.; Hasanpour-Heidari, S.; Salamat, F.; Rajaie, S.; Kazeminezhad, V.; Naeimi-Tabiei, M.; Jahangirrad, A.; Sedaghat, S.; Hosseinpoor, R.; Ghasemi-Kebria, F.; et al. Marked increase in breast cancer incidence in young women: A 10-year study from Northern Iran, 2004–2013. Cancer Epidemiol. 2019, 62, 101573. [Google Scholar] [CrossRef] [PubMed]
- Hassaine, Y.; Jacquet, E.; Seigneurin, A.; Delafosse, P. Evolution of breast cancer incidence in young women in a French registry from 1990 to 2018: Towards a change in screening strategy? Breast Cancer Res. 2022, 24, 87. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Kuo, Y.; Shih, Y.C.T.; Giordano, S.H.; Berenson, A.B. Trends in breast cancer mortality by stage at diagnosis among young women in the United States. Cancer 2018, 124, 3500–3509. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, S.; Freedman, R.A.; Partridge, A.H. The impact of young age at diagnosis (age < 40 years) on prognosis varies by breast cancer subtype: A U.S. SEER database analysis. Breast 2022, 61, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Nixon, A.J.; Neuberg, D.; Hayes, D.F.; Gelman, R.; Connolly, J.L.; Schnitt, S.; Abner, A.; Recht, A.; Vicini, F.; Harris, J.R. Relationship of patient age to pathologic features of the tumor and prognosis for patients with stage I or II breast cancer. J. Clin. Oncol. 1994, 12, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA Cancer J. Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef]
- Fidler, M.M.; Gupta, S.; Soerjomataram, I.; Ferlay, J.; Steliarova-Foucher, E.; Bray, F. Cancer incidence and mortality among young adults aged 20–39 years worldwide in 2012: A population-based study. Lancet Oncol. 2017, 18, 1579–1589. [Google Scholar] [CrossRef] [PubMed]
- Partridge, A.H.; Hughes, M.E.; Ottesen, R.A.; Wong, Y.-N.; Edge, S.B.; Theriault, R.L.; Blayney, D.W.; Niland, J.C.; Winer, E.P.; Weeks, J.C.; et al. The Effect of Age on Delay in Diagnosis and Stage of Breast Cancer. Oncologist 2012, 17, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Zabicki, K.; Colbert, J.A.; Dominguez, F.J.; Gadd, M.A.; Hughes, K.S.; Jones, J.L.; Specht, M.C.; Michaelson, J.S.; Smith, B.L. Breast Cancer Diagnosis in Women ≤ 40 versus 50 to 60 Years: Increasing Size and Stage Disparity Compared With Older Women Over Time. Ann. Surg. Oncol. 2006, 13, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Mazzara, C.; Pagani, O. Diagnosis and Treatment of Breast Cancer in Young Women. Curr. Treat. Options Oncol. 2019, 20, 86. [Google Scholar] [CrossRef] [PubMed]
- Sagona, A.; Gentile, D.; Anghelone, C.A.P.; Barbieri, E.; Marrazzo, E.; Antunovic, L.; Franceschini, D.; Tinterri, C. Ipsilateral Breast Cancer Recurrence: Characteristics, Treatment, and Long-Term Oncologic Results at a High-Volume Center. Clin. Breast Cancer 2021, 21, 329–336. [Google Scholar] [CrossRef]
- Azim, H.A.; Partridge, A.H. Biology of breast cancer in young women. Breast Cancer Res. 2014, 16, 427. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Pinto, A.C.; Ameye, L.; Jongen, L.; Del Mastro, L.; Puglisi, F.; Poggio, F.; Bonotto, M.; Floris, G.; Van Asten, K.; et al. The prognostic performance of Adjuvant! Online and Nottingham Prognostic Index in young breast cancer patients. Br. J. Cancer 2016, 115, 1471–1478. [Google Scholar] [CrossRef]
- Tung, N.; Lin, N.U.; Kidd, J.; Allen, B.A.; Singh, N.; Wenstrup, R.J.; Hartman, A.-R.; Winer, E.P.; Garber, J.E. Frequency of Germline Mutations in 25 Cancer Susceptibility Genes in a Sequential Series of Patients With Breast Cancer. J. Clin. Oncol. 2016, 34, 1460–1468. [Google Scholar] [CrossRef]
- Malone, K.E.; Daling, J.R.; Neal, C.; Suter, N.M.; O’Brien, C.; Cushing-Haugen, K.; Jonasdottir, T.J.; Thompson, J.D.; Ostrander, E.A. Frequency ofBRCA1/BRCA2 mutations in a population-based sample of young breast carcinoma cases. Cancer 2000, 88, 1393–1402. [Google Scholar] [CrossRef]
- Honrado, E.; Osorio, A.; Palacios, J.; Benitez, J. Pathology and gene expression of hereditary breast tumors associated with BRCA1, BRCA2 and CHEK2 gene mutations. Oncogene 2006, 25, 5837–5845. [Google Scholar] [CrossRef] [PubMed]
- Valencia, O.M.; Samuel, S.E.; Viscusi, R.K.; Riall, T.S.; Neumayer, L.A.; Aziz, H. The role of genetic testing in patients with breast cancer a review. JAMA Surg. 2017, 152, 589–594. [Google Scholar] [CrossRef]
- Lakhani, S.R.; Van De Vijver, M.J.; Jacquemier, J.; Anderson, T.J.; Osin, P.P.; McGuffog, L.; Easton, D.F. The pathology of familial breast cancer: Predictive value of immunohistochemical markers estrogen receptor, progesterone receptor, HER-2, and p53 in patients with mutations in BRCA1 and BRCA2. J. Clin. Oncol. 2002, 20, 2310–2318. [Google Scholar] [CrossRef]
- Lakhani, S.R.; Jacquemier, J.; Sloane, J.P.; Gusterson, B.A.; Anderson, T.J.; Van De Vijver, M.J.; Farid, L.M.; Venter, D.; Antoniou, A.; Storfer-Isser, A.; et al. Multifactorial analysis of differences between sporadic breast cancers and cancers involving BRCA1 and BRCA2 mutations. J. Natl. Cancer Inst. 1998, 90, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Atchley, D.P.; Albarracin, C.T.; Lopez, A.; Valero, V.; Amos, C.I.; Gonzalez-Angulo, A.M.; Hortobagyi, G.N.; Arun, B.K. Clinical and pathologic characteristics of patients with BRCA-positive and BRCA-negative breast cancer. J. Clin. Oncol. 2008, 26, 4282–4288. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, P.J.; Phillips, K.-A.; West, D.W.; Ennis, M.; Hopper, J.L.; John, E.M.; O’Malley, F.P.; Milne, R.L.; Andrulis, I.L.; Friedlander, M.L.; et al. Breast Cancer Prognosis in BRCA1 and BRCA2 Mutation Carriers: An International Prospective Breast Cancer Family Registry Population-Based Cohort Study. J. Clin. Oncol. 2012, 30, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Gentile, D.; Losurdo, A.; Sagona, A.; Zuradelli, M.; Gatzemeier, W.; Barbieri, E.; Testori, A.; Errico, V.; Bianchi, P.; Biondi, E.; et al. Surgical management of BRCA-mutation carriers: A single institution experience. Eur. J. Surg. Oncol. 2022, 48, 1706–1712. [Google Scholar] [CrossRef]
- van den Broek, A.J.; Schmidt, M.K.; van ‘t Veer, L.J.; Tollenaar, R.A.E.M.; van Leeuwen, F.E. Worse Breast Cancer Prognosis of BRCA1/BRCA2 Mutation Carriers: What’s the Evidence? A Systematic Review with Meta-Analysis. PLoS ONE 2015, 10, e0120189. [Google Scholar] [CrossRef]
- Baretta, Z.; Mocellin, S.; Goldin, E.; Olopade, O.I.; Huo, D. Effect of BRCA germline mutations on breast cancer prognosis. Med. (Baltim.) 2016, 95, e4975. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.K.; van den Broek, A.J.; Tollenaar, R.A.E.M.; Smit, V.T.H.B.M.; Westenend, P.J.; Brinkhuis, M.; Oosterhuis, W.J.W.; Wesseling, J.; Janssen-Heijnen, M.L.; Jobsen, J.J.; et al. Breast Cancer Survival of BRCA1/BRCA2 Mutation Carriers in a Hospital-Based Cohort of Young Women. JNCI J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef]
- Rennert, G.; Bisland-Naggan, S.; Barnett-Griness, O.; Bar-Joseph, N.; Zhang, S.; Rennert, H.S.; Narod, S.A. Clinical Outcomes of Breast Cancer in Carriers of BRCA1 and BRCA2 Mutations. N. Engl. J. Med. 2007, 357, 115–123. [Google Scholar] [CrossRef]
- Verhoog, L.; Brekelmans, C.; Seynaeve, C.; van den Bosch, L.; Dahmen, G.; van Geel, A.; Tilanus-Linthorst, M.; Bartels, C.; Wagner, A.; van den Ouweland, A.; et al. Survival and tumour characteristics of breast-cancer patients with germline mutations of BRCA1. Lancet 1998, 351, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Huzarski, T.; Byrski, T.; Gronwald, J.; Górski, B.; Domagała, P.; Cybulski, C.; Oszurek, O.; Szwiec, M.; Gugała, K.; Stawicka, M.; et al. Ten-Year Survival in Patients With BRCA1 -Negative and BRCA1 -Positive Breast Cancer. J. Clin. Oncol. 2013, 31, 3191–3196. [Google Scholar] [CrossRef] [PubMed]
- Copson, E.R.; Maishman, T.C.; Tapper, W.J.; Cutress, R.I.; Greville-Heygate, S.; Altman, D.G.; Eccles, B.; Gerty, S.; Durcan, L.T.; Jones, L.; et al. Germline BRCA mutation and outcome in young-onset breast cancer (POSH): A prospective cohort study. Lancet Oncol. 2018, 19, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; McShane, L.M.; Hammond, M.E.H.; Allison, K.H.; Fitzgibbons, P.; Press, M.F.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Hanna, W.; et al. Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J.; Albain, K.S.; André, F.; Bergh, J.; et al. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Azim, H.A.; Michiels, S.; Bedard, P.L.; Singhal, S.K.; Criscitiello, C.; Ignatiadis, M.; Haibe-Kains, B.; Piccart, M.J.; Sotiriou, C.; Loi, S. Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin. Cancer Res. 2012, 18, 1341–1351. [Google Scholar] [CrossRef]
- Young, S.R.; Pilarski, R.T.; Donenberg, T.; Shapiro, C.; Hammond, L.S.; Miller, J.; Brooks, K.A.; Cohen, S.; Tenenholz, B.; DeSai, D.; et al. The prevalence of BRCA1 mutations among young women with triple-negative breast cancer. BMC Cancer 2009, 9, 86. [Google Scholar] [CrossRef]
- Criscitiello, C.; Azim, H.A.; Schouten, P.C.; Linn, S.C.; Sotiriou, C. Understanding the biology of triple-negative breast cancer. Ann. Oncol. 2012, 23, vi13–vi18. [Google Scholar] [CrossRef]
- Stoppa-Lyonnet, D.; Ansquer, Y.; Dreyfus, H.; Gautier, C.; Gauthier-Villars, M.; Bourstyn, E.; Clough, K.B.; Magdelénat, H.; Pouillart, P.; Vincent-Salomon, A.; et al. Familial invasive breast cancers: Worse outcome related to BRCA1 mutations. J. Clin. Oncol. 2000, 18, 4053–4059. [Google Scholar] [CrossRef]
- Robson, M.E.; Chappuis, P.O.; Satagopan, J.; Wong, N.; Boyd, J.; Goffin, J.R.; Hudis, C.; Roberge, D.; Norton, L.; Bégin, L.R.; et al. A combined analysis of outcome following breast cancer: Differences in survival based on BRCA1/BRCA2 mutation status and administration of adjuvant treatment. Breast Cancer Res. 2003, 6, R8. [Google Scholar] [CrossRef]
- Moller, P.; Evans, D.G.; Reis, M.M.; Gregory, H.; Anderson, E.; Maehle, L.; Lalloo, F.; Howell, A.; Apold, J.; Clark, N.; et al. Surveillance for familial breast cancer: Differences in outcome according to BRCA mutation status. Int. J. Cancer 2007, 121, 1017–1020. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.A.; Jian, J.W.; Hung, C.F.; Peng, H.P.; Yang, C.F.; Cheng, H.S.; Yang, A.S. Germline breast cancer susceptibility gene mutations and breast cancer outcomes. BMC Cancer 2018, 18, 315. [Google Scholar] [CrossRef]
- Wang, C.J.; Xu, Y.; Lin, Y.; Zhu, H.J.; Zhou, Y.D.; Mao, F.; Zhang, X.H.; Huang, X.; Zhong, Y.; Sun, Q.; et al. Platinum-Based Neoadjuvant Chemotherapy for Breast Cancer With BRCA Mutations: A Meta-Analysis. Front. Oncol. 2020, 10, 592998. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Scoggins, M.E.; Hess, K.R.; Adrada, B.E.; Murthy, R.K.; Damodaran, S.; DeSnyder, S.M.; Brewster, A.M.; Barcenas, C.H.; Valero, V.; et al. Neoadjuvant talazoparib for patients with operable breast cancer with a germline BRCA pathogenic variant. J. Clin. Oncol. 2020, 38, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Kumar, T.; Hobbs, E.; Yang, F.; Chang, J.T.; Contreras, A.; Cuentas, E.R.P.; Garber, H.; Lee, S.; Lu, Y.; Scoggins, M.E.; et al. Tumor Immune Microenvironment Changes by Multiplex Immunofluorescence Staining in a Pilot Study of Neoadjuvant Talazoparib for Early-Stage Breast Cancer Patients with a Hereditary BRCA Mutation. Clin. Cancer Res. 2022, 28, 3669–3676. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | BRCA-Carriers (No. 63) Tot. (%)/Median (Range) | Non-Carriers (No. 339) Tot. (%)/Median (Range) | Univariate Analysis p-Value | Multivariate Analysis p-Value OR (95%CI) |
|---|---|---|---|---|
| Age (years) | 35 (24–40) | 37 (22–40) | ||
| - ≤35 | 38 (60.3%) | 118 (34.8%) | <0.0001 a | 0.001 a 7.699 (33.871–35.568) |
| - >35 | 25 (39.7%) | 221 (65.2%) | - | - |
| Tumor | ||||
| Grading | ||||
| - 1 | 0 (0%) | 15 (4.4%) | <0.0001 a | 0.001 a 17.119 (2.549–2.828) |
| - 2 | 21 (33.3%) | 186 (54.9%) | - | - |
| - 3 | 42 (66.7%) | 138 (40.7%) | - | |
| Dimension (mm) | 21 (5–100) | 18 (4–110) | ||
| - <18 | 22 (34.9%) | 159 (46.9%) | 0.08 | |
| - ≥18 | 41 (65.1%) | 180 (53.1%) | - | |
| Stage | ||||
| ypT0-is | 5 (7.9%) | 7 (2.1%) | 0.104 | |
| pT1 | 22 (34.9%) | 192 (56.6%) | - | |
| pT2 | 31 (49.2%) | 127 (37.5%) | - | |
| pT3 | 5 (8.0%) | 13 (3.8%) | - | |
| pN0 | 34 (54.0%) | 197 (58.1%) | 0.008 a | 0.051 5.952 (0.758–1.275) |
| pNmic | 6 (9.5%) | 7 (2.1%) | - | - |
| pN1 | 11 (17.5%) | 87 (25.7%) | - | |
| pN2 | 6 (9.5%) | 37 (10.9%) | - | |
| pN3 | 6 (9.5%) | 11 (3.2%) | - | |
| Biological subtype | ||||
| - Luminal-like | 22 (34.9%) | 218 (64.3%) | <0.0001 a | 0.001 a 52.717 (2.042–2.417) |
| - HER2+ | 5 (7.9%) | 79 (23.3%) | - | - |
| - Triple negative | 36 (57.2%) | 42 (12.4%) | - | |
| - Ki67 (%) | 55 (5–95) | 20 (1–90) | ||
| - <25 | 17 (27.0%) | 206 (60.8%) | <0.0001 a | 0.001 a 58.981 (47.135–58.505) |
| - ≥25 | 46 (73.0%) | 133 (39.2%) | - | - |
| Vascular invasion | 24 (38.1%) | 148 (43.7%) | 0.414 | |
| Treatment | ||||
| - Neoadjuvant CHT | 7 (11.1%) | 36 (10.6%) | 0.908 | |
| - Mastectomy | 33 (52.4%) | 134 (39.5%) | 0.058 | |
| - ALND | 32 (50.8%) | 140 (41.3%) | 0.163 | |
| - Radiotherapy | 32 (50.8%) | 239 (70.5%) | 0.003 a | |
| - Endocrine therapy | 27 (42.9%) | 275 (81.1%) | <0.0001 a | |
| - Adjuvant CHT | 46 (73.0%) | 190 (56.1%) | 0.005 a | |
| - Trastuzumab | 5 (7.9%) | 71 (20.9%) | 0.015 a |
| Factors | DFS HR (95%CI) p-Value | DDFS HR (95%CI) p-Value | OS HR (95%CI) p-Value |
|---|---|---|---|
| BRCA | |||
| - Carriers | Reference | Reference | Reference |
| - Non-carriers | 0.203 (0.104–0.394) 0.001 | 0.357 (0.174–0.734) 0.005 | 0.257 (0.072–1.051) 0.059 |
| Age (years) | |||
| - ≤35 | Reference | Reference | Reference |
| - >35 | 0.770 (0.437–1.360) 0.368 | 0.791 (0.445–1.408) 0.426 | 0.425 (0.122–1.487) 0.181 |
| G | |||
| -1 | Reference | Reference | Reference |
| -2 | Reference | Reference | Reference |
| -3 | 1.595 (0.799–3.185) 0.186 | 2.104 (1.037–4.265) 0.039 | 2.078 (0.391–11.053) 0.391 |
| Biological subtype | |||
| - Luminal-like | Reference | Reference | Reference |
| - HER2+ | Reference | Reference | Reference |
| - Triple-negative | 0.563 (0.316–1.002) 0.051 | 0.583 (0.321–1.058) 0.076 | 0.238 (0.070–0.812) 0.022 |
| Ki67 (%) | |||
| - <25 | Reference | Reference | Reference |
| - ≥25 | 0.678 (0.312–1.477) 0.328 | 0.766 (0.356–1.651) 0.497 | 2.234 (0.377–13.248) 0.376 |
| Neo-adjuvant CHT | |||
| - No | Reference | Reference | Reference |
| - Yes | 0.678 (0.312–1.477) 0.328 | 1.450 (0.517–4.069) 0.480 | 14.885 (2.343–94.566) 0.004 |
| Breast surgery | |||
| - BCS | Reference | Reference | Reference |
| - Mastectomy | 0.770 (0.359–1.651) 0.502 | 1.020 (0.460–2.262) 0.962 | 3.862 (0.745–20.011) 0.107 |
| ALND | |||
| - No | Reference | Reference | Reference |
| - Yes | 0.880 (0.468–1.653) 0.691 | 0.674 (0.350–1.296) 0.237 | 0.966 (0.226–4.132) 0.962 |
| RT | |||
| - No | Reference | Reference | Reference |
| - Yes | 0.916 (0.445–1.885) 0.328 | 1.073 (0.503–2.810) 0.567 | 1.527 (0.361–6.467) 0.565 |
| Hormone therapy | |||
| - No | Reference | Reference | Reference |
| - Yes | 0.584 (0.219–1.554) 0.282 | 0.669 (0.238–1.885) 0.447 | 0.160 (0.016–1.561) 0.115 |
| Adjuvant CHT | |||
| - No | Reference | Reference | Reference |
| - Yes | 1.424 (0.639–3.176) 0.387 | 1.263 (0.568–2.810) 0.568 | 3.186 (0.490–20.697) 0.225 |
| Trastuzumab | |||
| - No | Reference | Reference | n/a |
| - Yes | 0.687 (0.257–1.853) 0.454 | 0.616 (0.228–1.668) 0.340 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tinterri, C.; Di Maria Grimaldi, S.; Sagona, A.; Barbieri, E.; Darwish, S.; Bottini, A.; Canavese, G.; Gentile, D. Comparison of Long-Term Oncological Results in Young Women with Breast Cancer between BRCA-Mutation Carriers Versus Non-Carriers: How Tumor and Genetic Risk Factors Influence the Clinical Prognosis. Cancers 2023, 15, 4177. https://doi.org/10.3390/cancers15164177
Tinterri C, Di Maria Grimaldi S, Sagona A, Barbieri E, Darwish S, Bottini A, Canavese G, Gentile D. Comparison of Long-Term Oncological Results in Young Women with Breast Cancer between BRCA-Mutation Carriers Versus Non-Carriers: How Tumor and Genetic Risk Factors Influence the Clinical Prognosis. Cancers. 2023; 15(16):4177. https://doi.org/10.3390/cancers15164177
Chicago/Turabian StyleTinterri, Corrado, Simone Di Maria Grimaldi, Andrea Sagona, Erika Barbieri, Shadya Darwish, Alberto Bottini, Giuseppe Canavese, and Damiano Gentile. 2023. "Comparison of Long-Term Oncological Results in Young Women with Breast Cancer between BRCA-Mutation Carriers Versus Non-Carriers: How Tumor and Genetic Risk Factors Influence the Clinical Prognosis" Cancers 15, no. 16: 4177. https://doi.org/10.3390/cancers15164177
APA StyleTinterri, C., Di Maria Grimaldi, S., Sagona, A., Barbieri, E., Darwish, S., Bottini, A., Canavese, G., & Gentile, D. (2023). Comparison of Long-Term Oncological Results in Young Women with Breast Cancer between BRCA-Mutation Carriers Versus Non-Carriers: How Tumor and Genetic Risk Factors Influence the Clinical Prognosis. Cancers, 15(16), 4177. https://doi.org/10.3390/cancers15164177