
Avatar-Based Strategies for Breast Cancer Patients: A Systematic Review
 , , and
, , and 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. General Description
2.2. Selection Criteria
2.3. Outcomes
2.4. Search Methodology
2.5. Data Collection and Analysis
2.6. Data Extraction and Management
2.7. Quality of Studies Included
2.8. Statistical Analysis
3. Results
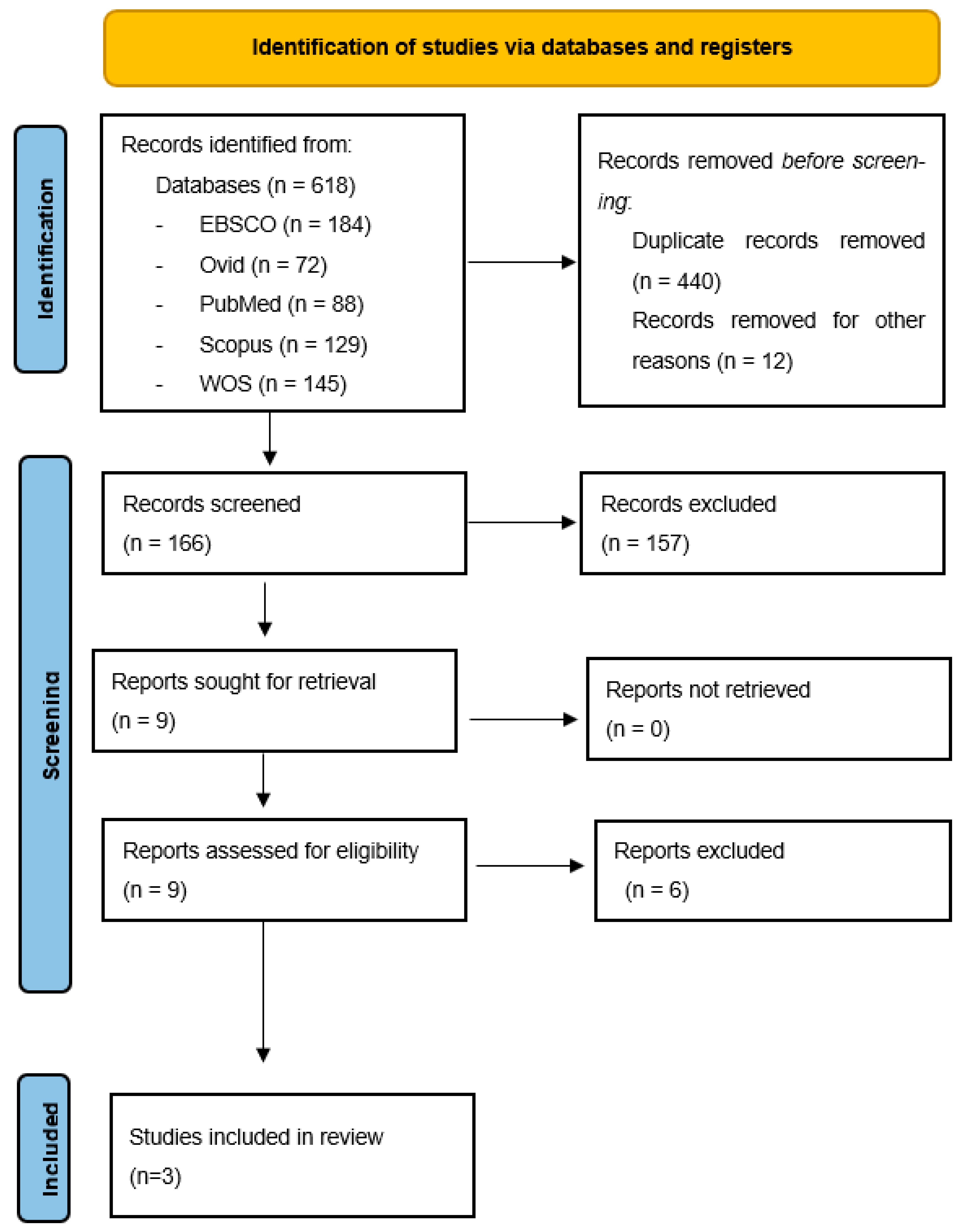
3.1. Study Selection and Inclusion
3.2. General Characteristics of the Studies Included
Assessment of Methodological Quality of Included Studies
3.3. Primary Outcomes
3.3.1. Training Using Avatar
3.3.2. Measured QoL and Well-Being and the Instrument Used
3.3.3. Usefulness to Improve QoL and/or Psychological Well-Being
3.4. Secondary Outcomes
3.4.1. Main Advantages and Disadvantages
3.4.2. Patients’ Satisfaction
4. Discussion
5. Conclusions
5.1. Clinical and Researcher Implications
5.2. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Durosini, I.; Triberti, S.; Pravettoni, G. Breast cancer survivors’ attitudes towards internet-based psychotherapy. Annu. Rev. Cyber Ther. Telemed. 2020, 18, 201–205. [Google Scholar]
- Lahart, I.M.; Metsios, G.S.; Nevill, A.M.; Carmichael, A.R. Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies. Acta Oncol. 2015, 54, 635–654. [Google Scholar] [CrossRef]
- Arnold, M.; Morgan, E.; Rumgay, H.; Mafra, A.; Singh, D.; Laversanne, M.; Vignat, J.; Gralow, J.R.; Cardoso, F.; Siesling, S.; et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast 2022, 66, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Hipp, L.E.; Hulswit, B.B.; Milliron, K.J. Clinical tools and counseling considerations for breast cancer risk assessment and evaluation for hereditary cancer risk. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 82, 12–29. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Nucci, D.; Balzarini, M.; Acito, M.; Moretti, M.; Villarini, A.; Villarini, M. E-Coaching: The DianaWeb study to prevent breast cancer recurrences. Clin. Ter. 2020, 171, e59–e65. [Google Scholar] [CrossRef]
- Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. eHealth for improving quality of life in breast cancer patients: A systematic review. Cancer Treat. Rev. 2019, 74, 1–14. [Google Scholar] [CrossRef]
- Marzorati, C.; Riva, S.; Pravettoni, G. Who Is a Cancer Survivor? A Systematic Review of Published Definitions. J. Cancer Educ. 2017, 32, 228–237. [Google Scholar] [CrossRef]
- Sebri, V.; Savioni, L.; Triberti, S.; Durosini, I.; Mazzocco, K.; Pravettoni, G. Do You Transfer Your Skills? From Sports to Health Management in Cancer Patients. Front. Psychol. 2020, 11, 546. [Google Scholar] [CrossRef]
- Wilmoth, M.C. The aftermath of breast cancer: An altered sexual self. Cancer Nurs. 2001, 24, 278–286. [Google Scholar] [CrossRef]
- Jabłoński, M.J.; Mirucka, B.; Streb, J.; Słowik, A.J.; Jach, R. Exploring the relationship between the body self and the sense of coherence in women after surgical treatment for breast cancer. Psycho-Oncology 2019, 28, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Renzi, C.; Vadilonga, V.; Gandini, S.; Perinel, G.; Rotmensz, N.; Didier, F.; Rescigno, M.; Pravettoni, G. Stress exposure in significant relationships is associated with lymph node status in breast cancer. PLoS ONE 2016, 11, e0149443. [Google Scholar] [CrossRef]
- Boquiren, V.M.; Esplen, M.J.; Wong, J.; Toner, B.; Warner, E. Exploring the influence of gender-role socialization and objectified body consciousness on body image disturbance in breast cancer survivors. Psycho-Oncology 2013, 22, 2177–2185. [Google Scholar] [CrossRef]
- Falk Dahl, C.A.; Reinertsen, K.V.; Nesvold, I.; Fosså, S.D.; Dahl, A.A. A study of body image in long-term breast cancer survivors. Cancer 2010, 116, 3549–3557. [Google Scholar] [CrossRef] [PubMed]
- Chopra, D.; De La Garza, R. Depressive, anxiety, and distress symptoms among cancer patients who endorse appearance problems. Palliat. Support Care 2018, 17, 328–332. [Google Scholar] [CrossRef]
- Paterson, C.L.; Lengacher, C.A.; Donovan, K.A.; Kip, K.E.; Tofthagen, C.S. Body Image in Younger Breast Cancer Survivors: A Systematic Review. Cancer Nurs. 2016, 39, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Crosswell, A.D.; Stanton, A.L.; Crespi, C.M.; Winston, D.; Arevalo, J.; Ma, J.; Cole, S.W.; Ganz, P.A. Mindfulness meditation for younger breast cancer survivors: A randomized controlled trial. Cancer 2015, 121, 1231–1240. [Google Scholar] [CrossRef] [PubMed]
- Gotay, C.C.; Kawamoto, C.T.; Bottomley, A.; Efficace, F. The prognostic significance of patient-reported outcomes in cancer clinical trials. J. Clin. Oncol. 2008, 26, 1355–1363. [Google Scholar] [CrossRef]
- Ashing-Giwa, K.T. The contextual model of HRQoL: A paradigm for expanding the HRQoL framework. Qual. Life Res. 2005, 14, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Jung, S.; Lee, J.E.; Shim, E.; Kim, N.H.; Kim, Z.; Sohn, G.; Youn, H.J.; Kim, K.S.; Kim, H. A review of breast cancer survivorship issues from survivors’ perspectives. J. Breast Cancer 2014, 17, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Class, M.; Gomez-Duarte, J.; Graves, K.; Ashing-Giwa, K. A contextual approach to understanding breast cancer survivorship among Latinas. Psychooncology 2012, 21, 115–124. [Google Scholar] [CrossRef]
- Friedrich, M.; Zenger, M.; Hinz, A. Response shift effects of quality of life assessments in breast cancer survivors. Eur. J. Cancer Care 2019, 28, e12979. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhao, Q.; Cao, P.; Ren, G. Resilience and Quality of Life: Exploring the Mediator Role of Social Support in Patients with Breast Cancer. Med. Sci. Monit. 2017, 23, 5969–5979. [Google Scholar] [CrossRef]
- Chou, A.F.; Stewart, S.L.; Wild, R.C.; Bloom, J.R. Social support and survival in young women with breast carcinoma. Psycho-Oncology 2012, 21, 125–133. [Google Scholar] [CrossRef]
- Salonen, P.; Tarkka, M.T.; Kellokumpu-Lehtinen, P.L.; Koivisto, A.M.; Aalto, P.; Kaunonen, M. Effect of social support on changes in quality of life in early breast cancer patients: A longitudinal study. Scand. J. Caring Sci. 2013, 27, 396–405. [Google Scholar] [CrossRef]
- Andreu, Y.; Galdon, M.J.; Dura, E.; Martínez, P.; Pérez, S.; Murgui, S. A longitudinal study of psychosocial distress in breast cancer: Prevalence and risk factors. Psychol. Health 2012, 27, 72–87. [Google Scholar] [CrossRef]
- Kim, J.; Han, J.Y.; Shaw, B.; McTavish, F.; Gustafson, D. The roles of social support and coping strategies in predicting breast cancer patients’ emotional well-being: Testing mediation and moderation models. J. Health Psychol. 2010, 15, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Jaremka, L.M.; Alfano, C.M.; Glaser, R.; Povoski, S.P.; Lipari, A.M.; Agnese, D.M.; Farrar, W.B.; Yee, L.D.; Carson, W.E., 3rd; et al. Social support predicts inflammation, pain, and depressive symptoms: Longitudinal relationships among breast cancer survivors. Psychoneuroendocrinology 2014, 42, 38–44. [Google Scholar] [CrossRef]
- Epplein, M.; Zheng, Y.; Zheng, W.; Chen, Z.; Gu, K.; Penson, D.; Lu, W.; Shu, X.O. Quality of life after breast cancer diagnosis and survival. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 406–412. [Google Scholar] [CrossRef]
- Drageset, S.; Lindstrøm, T.C.; Giske, T.; Underlid, K. Women’s experiences of social support during the first year following primary breast cancer surgery. Scand. J. Caring Sci. 2016, 30, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Sebri, V.; Mazzoni, D.; Triberti, S.; Pravettoni, G. The impact of unsupportive social support on the injured self in breast cancer patients. Front. Psychol. 2021, 12, 2211. [Google Scholar] [CrossRef] [PubMed]
- Urech, C.; Grossert, A.; Alder, J.; Scherer, S.; Handschin, B.; Kasenda, B.; Borislavova, B.; Degen, S.; Erb, J.; Faessler, A.; et al. Web-Based Stress Management for Newly Diagnosed Patients With Cancer (STREAM): A Randomized, Wait-List Controlled Intervention Study. J. Clin. Oncol. 2018, 36, 780–788. [Google Scholar] [CrossRef]
- Sousa, P.M.; Ferreira, I.M.; Filipe, M.J.; Guerra, P.M.; Ferreira, R.A.; Lages, M.C.; Dixe, M.A. Aceitação de um programa mHealth para prevenção da obesidade em adolescentes: Estudo misto sequencial. Rev. Enferm. Ref. 2020, 5, e20039. [Google Scholar] [CrossRef]
- Triberti, S.; Chirico, A. Healthy Avatars, Healthy People. In Transformative Healthcare Practice through Patient Engagement; Graffigna, G., Ed.; IGI Global: Hersey, PA, USA, 2016; pp. 247–275. [Google Scholar]
- Triberti, S.; Riva, G. Positive Technology for Enhancing the Patient Engagement Experiences. In Patient Engagement: A Consumer-Centered Model to Innovate Healthcare; De Gruyter Open: Berlin, Germany, 2015; pp. 44–55. [Google Scholar]
- Triberti, S.; Durosini, I.; Aschieri, F.; Villani, D.; Riva, G. A frame effect in avatar customization: How users’ attitudes towards their avatars may change depending on virtual context. Annu. Rev. CyberTherapy Telemed. 2017, 15, 92–97. Available online: http://hdl.handle.net/10807/119584 (accessed on 1 June 2023).
- Triberti, S.; Durosini, I.; Aschieri, F.; Villani, D.; Riva, G. Changing Avatars, Changing Selves? The Influence of Social and Contextual Expectations on Digital Rendition of Identity. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 501–507. [Google Scholar] [CrossRef]
- Andrade, A.D.; Anam, R.; Karanam, C.; Downey, P.; Ruiz, J.G. An overactive bladder online self-management program with embedded avatars: A randomized controlled trial of efficacy. Urology 2015, 85, 561–567. [Google Scholar] [CrossRef]
- Franco, M.; Monfort, C.; Piñas-Mesa, A.; Rincon, E. Could Avatar Therapy Enhance Mental Health in Chronic Patients? A Systematic Review. Electronics 2021, 10, 2212. [Google Scholar] [CrossRef]
- Rehm, I.C.; Foenander, E.; Wallace, K.; Abbott, J.M.; Kyrios, M.; Thomas, N. What Role Can Avatars Play in e-Mental Health Interventions? Exploring New Models of Client–Therapist Interaction. Front. Psychiatry 2016, 7, 186. [Google Scholar] [CrossRef] [PubMed]
- Del Aguila, J.; González-Gualda, L.M.; Játiva, M.A.; Fernández-Sotos, P.; Fernández-Caballero, A.; García, A.S. How interpersonal distance between avatar and human influences facial affect recognition in immersive virtual reality. Front. Psychol. 2021, 12, 675515. [Google Scholar] [CrossRef]
- Bourke, C.; Douglas, K.; Porter, R. Processing of facial emotion expression in major depression: A review. Aust. N. Z. J. Psychiatry 2010, 44, 681–696. [Google Scholar] [CrossRef]
- Botella, C.; García-Palacios, A.; Quero, S.; Baños, R.M.; Bretón-López, J.M. Realidad virtual y tratamientos psicológicos: Una revisión. Psicol. Conduct. 2006, 3, 491–510. [Google Scholar]
- Kumazaki, H.; Warren, Z.; Swanson, A.; Yoshikawa, Y.; Matsumoto, Y.; Yoshimura, Y.; Shimaya, J.; Ishiguro, H.; Sarkar, N.; Wade, J. Brief report: Evaluating the utility of varied technological agents to elicit social attention from children with autism spectrum disorders. J. Autism Dev. Disord. 2019, 49, 1700–1708. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.N.K.; Hetherington, L.; Wheeler, S. Second life: An overview of the potential of 3-D virtual worlds in medical and health education. Health Inf. Libr. J. 2007, 24, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Sundar, S.S. Visualizing ideal self vs. actual self through avatars: Impact on preventive health outcomes. Comput. Hum. Behav. 2012, 28, 1356–1364. [Google Scholar] [CrossRef]
- Wonggom, P.; Kourbelis, C.; Newman, P.; Du, H.; Clark, R.A. Effectiveness of avatar-based technology in patient education for improving chronic disease knowledge and self-care behavior: A systematic review. JBI Evid. Synth. 2019, 17, 1101–1129. [Google Scholar] [CrossRef]
- Triberti, S.; Argenton, L. Psicologia dei Videogiochi: Come i Mondi Virtuali Influenzano Mente e Comportamento; Apogeo: Milano, Italy, 2013. [Google Scholar]
- Barello, S.; Graffigna, G. Engaging patients to recover life projectuality: An Italian cross-disease framework. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2014, 24, 1087–1096. [Google Scholar] [CrossRef]
- Miller, E.; Polson, D. Apps, Avatars, and Robots: The Future of Mental Healthcare. Issues Ment. Health Nurs. 2019, 40, 208–214. [Google Scholar] [CrossRef]
- O’Connor, S. Virtual Reality and Avatars in Health care. Clin. Nurs. Res. 2019, 28, 523–528. [Google Scholar] [CrossRef]
- Graffigna, G.; Barello, S.; Triberti, S. Patient Engagement: A Consumer-Centered Model to Innovate Healthcare; DeGruyter Open: Berlin, Germany, 2015. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research; CRC Press: Boca Raton, FL, USA, 1990. [Google Scholar]
- Pluye, P.; Gagnon, M.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.; Griffiths, F.; Nicolau, B. Mixed Methods Appraisal Tool (MMAT), Version 2018. Registration of Copyright 2018. p. 1148552. Available online: file:///C:/Users/MDPI/Downloads/bmjopen-2021-February-11-2--inline-supplementary-material-3.pdf (accessed on 30 July 2023).
- Baxter, J. ‘Keep strong, remember everything you have learnt’: Constructing support and solidarity through online interaction within a UK cancer support group. Discourse Soc. 2018, 29, 363–379. [Google Scholar] [CrossRef]
- De Maria Marchiano, R.; Di Sante, G.; Piro, G.; Carbone, C.; Tortora, G.; Boldrini, L.; Pietragalla, A.; Daniele, G.; Tredicine, M.; Cesario, A.; et al. Translational research in the era of precision medicine: Where we are and where we will go. J. Pers. Med. 2021, 11, 216. [Google Scholar] [CrossRef]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Rampertaap, K.; El-Shammaa, N.; Hiotis, K.; Scagliola, J.; Yu, G.; Wang, Y. mHealth self-care interventions: Managing symptoms following breast cancer treatment. Mhealth 2016, 2, 28. [Google Scholar] [CrossRef]
- Putranto, D.; Rochmawati, E. Mobile applications for managing symptoms of patients with cancer at home: A scoping review. Int. J. Nurs. Pract. 2020, 26, e12842. [Google Scholar] [CrossRef]
- Ryu, S.; Price, S.K. Embodied storytelling and meaning-making at the end of life: VoicingHan avatar life-review for palliative care in cancer patients. Arts Health 2021, 14, 326–340. [Google Scholar] [CrossRef]
- Dang, M.; Noreika, D.; Ryu, S.; Sima, A.; Ashton, H.; Ondris, B.; Coley, F.; Nestler, J.; Fabbro, E.D. Feasibility of Delivering an Avatar-Facilitated Life Review Intervention for Patients with Cancer. J. Palliat. Med. 2021, 24, 520–526. [Google Scholar] [CrossRef]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Wang, Y.; Scagliola, J.; Hiotis, K.; Rampertaap, K.; El-Shammaa, N. Usability and feasibility of health IT interventions to enhance Self-Care for Lymphedema Symptom Management in breast cancer survivors. Internet Interv. 2016, 5, 56–64. [Google Scholar] [CrossRef]
- Triberti, S.; Gorini, A.; Savioni, L.; Sebri, V.; Pravettoni, G. Avatars and the Disease: Digital Customization as a Resource for Self-Perception Assessment in Breast Cancer Patients. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 558–564. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Peterman, A.H.; Fitchett, G.; Brady, M.J.; Hernandez, L.; Cella, D. Measuring spiritual well-being in people with cancer: The functional assessment of chronic illness therapy--Spiritual Well-being Scale (FACIT-Sp). Ann. Behav. Med. 2002, 24, 49–58. [Google Scholar] [CrossRef]
- Jocham, H.R.; Dassen, T.; Widdershoven, G.; Halfens, R. Reliability and validity of the EORTC QLQ-C30 in palliative care cancer patients. Cent. Eur. J. Med. 2009, 4, 348–357. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Shafii, T.; Benson, S.K.; Morrison, D.M.; Hughes, J.P.; Golden, M.R.; Holmes, K.K. A pilot randomised controlled trial of an interactive computer-based intervention for sexual health in adolescents and young adults. BMJ Sex. Transm. Dis. 2015, 91, A33. [Google Scholar] [CrossRef][Green Version]
- Andersen, R. A Behavioral Model of Families’ Use of Health Services; Research series; Center for Health Administration Studies; University of Chicago: Chicago, IL, USA, 1968; Volume 25. [Google Scholar]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Savioni, L.; Triberti, S.; Durosini, I.; Sebri, V.; Pravettoni, G. Cancer patients’ participation and commitment to psychological interventions: A scoping review. Psychol. Health 2022, 37, 1022–1055. [Google Scholar] [CrossRef]
- Yee, N.; Bailenson, J. The proteus effect: The effect of transformed self-representation on behavior. Hum. Commun. Res. 2007, 33, 271–290. [Google Scholar] [CrossRef]
- Oyanagi, A.; Narumi, T.; Lugrin, J.-L.; Aoyama, K.; Ito, K.; Amemiya, T.; Hirose, M. The Possibility of Inducing the Proteus Effect for Social VR Users. In HCI International 2022—Late Breaking Papers: Interacting with eXtended Reality and Artificial Intelligence; Chen, J.Y.C., Fragomeni, G., Degen, H., Ntoa, S., Eds.; Springer: Cham, Switzerland, 2022; Volume 13518, pp. 143–158. [Google Scholar] [CrossRef]
- Yoon, G.; Vargas, P.T. Know thy avatar: The unintended effect of virtual-self representation on behavior. Psychol. Sci. 2014, 25, 1043–1045. [Google Scholar] [CrossRef]
- Ratan, R.; Sah, Y.J. Leveling up on stereotype threat: The role of avatar customization and avatar embodiment. Comput. Hum. Behav. 2015, 50, 367–374. [Google Scholar] [CrossRef]
- Fu, M.R.; Axelrod, D.; Guth, A.A.; Scagliola, J.; Rampertaap, K.; El-Shammaa, N.; Qiu, J.M.; McTernan, M.L.; Frye, L.; Park, C.S. A web-and mobile-based intervention for women treated for breast cancer to manage chronic pain and symptoms related to lymphedema: Results of a randomized clinical trial. JMIR Cancer 2022, 8, e29485. [Google Scholar] [CrossRef]
- Bacchini, D.; De Angelis, G.; Fanara, A. Identity formation in adolescent and emerging adult regular players of massively multiplayer online role-playing games (MMORPG). Comput. Hum. Behav. 2017, 73, 191–199. [Google Scholar] [CrossRef]
- Lin, H.; Wang, H. Avatar creation in virtual worlds: Behaviors and motivations. Comput. Hum. Behav. 2014, 34, 213–218. [Google Scholar] [CrossRef]
- Vasalou, A.; Joinson, A.N. Me, myself and I: The role of interactional context on self-presentation through avatars. Comput. Hum. Behav. 2009, 25, 510–520. [Google Scholar] [CrossRef]
- Villani, D.; Gatti, E.; Triberti, S.; Confalonieri, E.; Riva, G. Exploration of virtual body-representation in adolescence: The role of age and sex in avatar customization. SpringerPlus 2016, 5, 740. [Google Scholar] [CrossRef]
- Beck, S.L.; Eaton, L.H.; Echeverria, C.; Mooney, K.H. SymptomCare@Home: Developing an integrated symptom monitoring and management system for outpatients receiving chemotherapy. Comput. Inform. Nurs. 2017, 35, 520–529. [Google Scholar] [CrossRef]
- Chung, W.W.; Agbayani, C.G.; Martinez, A.; Le, V.; Cortes, H.; Har, K.; Fortier, M.A. Improving Children’s cancer pain management in the home setting: Development and formative evaluation of a web-based program for parents. Comput. Biol. Med. 2018, 1, 146–152. [Google Scholar] [CrossRef]
- Fishbein, J.N.; Nisotel, L.E.; MacDonald, J.J.; Amoyal Pensak, N.; Jacobs, J.M.; Flanagan, C.; Greer, J.A. Mobile application to promote adherence to oral chemotherapy and symptom management: A protocol for design and development. JMIR Res. Protoc. 2017, 6, e62. [Google Scholar] [CrossRef]
- Slater, P.J.; Fielden, P.E.; Bradford, N.K. The Oncology Family App: Providing information and support for families caring for their child with cancer. J. Pediatr. Oncol. Nurs. 2018, 35, 94–102. [Google Scholar] [CrossRef]
- Fortier, M.A.; Chung, W.W.; Martinez, A.; Gago-Masague, S.; Sender, L. Pain buddy: A novel use of m-health in the management of children’s cancer pain. Comput. Biol. Med. 2016, 76, 202–214. [Google Scholar] [CrossRef]
- Kessel, K.A.; Vogel, M.M.; Kessel, C.; Bier, H.; Biedermann, T.; Friess, H.; Herschbach, P.; von Eisenhart-Rothe, R.; Meyer, B.; Kiechle, M.; et al. Mobile health in oncology: A patient survey about app-assisted cancer care. JMIR Mhealth Uhealth 2017, 5, e81. [Google Scholar] [CrossRef]
- Knight, A. From nurse to service user: A personal cancer narrative. Br. J. Nurs. 2018, 27, S18–S21. [Google Scholar] [CrossRef]
- Rincon, E.; Monteiro-Guerra, F.; Rivera-Romero, O.; Dorronzoro-Zubiete, E.; Sanchez-Bocanegra, C.L.; Gabarron, E. Mobile Phone Apps for Quality of Life and Well-Being Assessment in Breast and Prostate Cancer Patients: Systematic Review. JMIR Mhealth Uhealth 2017, 5, e187. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015, 4, 1. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]


{kind=link}
| Study | Publication Year | Country | Study Design |
|---|---|---|---|
| Dang et al. [61] | 2021 | USA | Mixed method |
| Fu et al. [62] | 2016 | USA | Mixed method |
| Triberti et al. [63] | 2019 | Italy | Quantitative |
| Study | Aim | Sample Size (Mean Age) | Only Breast Cancer Patients/Stage | Patients Randomized |
|---|---|---|---|---|
| Dang et al. [61] | Establish the feasibility and acceptability of an avatar-facilitated life review intervention. | 12 (24–65+ years) | No/NP | No |
| Fu et al. [62] | Test the TOLF system to evaluate the reliability, validity, and efficacy of mHealth assessment as well as usability, feasibility, acceptability, and efficacy of mHealth self-care interventions for lymphedema symptoms among the end user of breast cancer survivors. | 355 (21–80 years) | Yes/NP | No |
| Triberti et al. [63] | Examine how breast cancer affects avatar-conveyed multiple representations and if attitudes toward avatars are related to anxiety and depression. | 22 (49.4) | Yes/NP | No |
| Study | Training Using Avatars | QoL c and Well-Being Assessment | Useful to Improve QoL/Well-Being |
|---|---|---|---|
| Dang et al. [61] | VoicingHan via a Perception Neuron a and a Logitech® wireless headset | Yes EORTC QLQ-C30 b, FACIT-Sp c, ESAS d | No/Yes |
| Fu et al. [62] | TOLF e (app and website) | Yes BCLE-SEI f | Yes/Yes |
| Triberti et al. [63] | Profile Avatar Maker 2 (app) | No/Yes PHQ-9 g, GAD-7 h | Not applicable |
| Study | Main Advantages | Main Disadvantages | Patients’ Satisfaction |
|---|---|---|---|
| Dang et al. [61] | High feasibility; avatars in VR enhance patient communication and engagement, and promote the expression of identity | Selection bias; intervention requires space and technical expertise | High |
| Fu et al. [62] | Patient-targeted; usability tested; feasible, user-friendly; avatar tailored to the specific population | Homogeneous sample in some characteristics | High |
| Triberti et al. [63] | The experience of a chronic illness (cancer) was used as an independent source of information to represent a facet of the self. Patient´s privacy preserved. | Lack of measurement in avatar characteristics and in the ability and satisfaction of the participants with their avatar creation | Unknown |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Guidonet, I.; Andrade-Pino, P.; Monfort-Vinuesa, C.; Rincon, E. Avatar-Based Strategies for Breast Cancer Patients: A Systematic Review. Cancers 2023, 15, 4031. https://doi.org/10.3390/cancers15164031
Rodríguez-Guidonet I, Andrade-Pino P, Monfort-Vinuesa C, Rincon E. Avatar-Based Strategies for Breast Cancer Patients: A Systematic Review. Cancers. 2023; 15(16):4031. https://doi.org/10.3390/cancers15164031
Chicago/Turabian StyleRodríguez-Guidonet, Irene, Paula Andrade-Pino, Carlos Monfort-Vinuesa, and Esther Rincon. 2023. "Avatar-Based Strategies for Breast Cancer Patients: A Systematic Review" Cancers 15, no. 16: 4031. https://doi.org/10.3390/cancers15164031
APA StyleRodríguez-Guidonet, I., Andrade-Pino, P., Monfort-Vinuesa, C., & Rincon, E. (2023). Avatar-Based Strategies for Breast Cancer Patients: A Systematic Review. Cancers, 15(16), 4031. https://doi.org/10.3390/cancers15164031