
Plasma Clot Properties in Patients with Pancreatic Cancer



Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Blood Sampling
2.3. Routine Laboratory Parameters
2.4. Plasma Clot Formation Assay
2.5. Statistics
3. Results
3.1. Clinical Characteristics and Routine Laboratory Parameters
3.2. Plasma Clot Formation
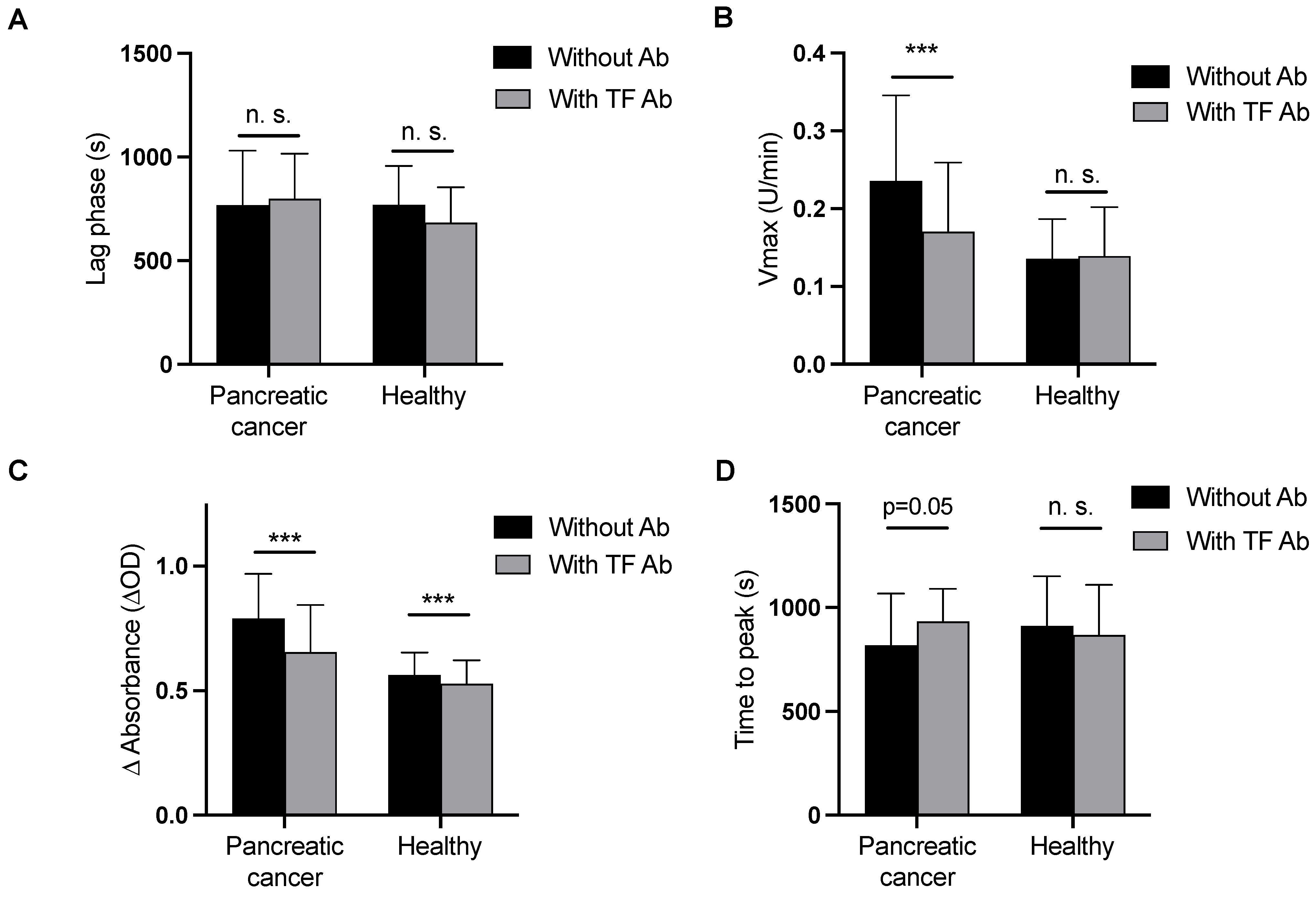
3.3. Modified Plasma Clot Formation Assay (Clotting Induced by CaCl2 and Phospholipids) in the Absence and Presence of a Tissue Factor Blocking Antibody
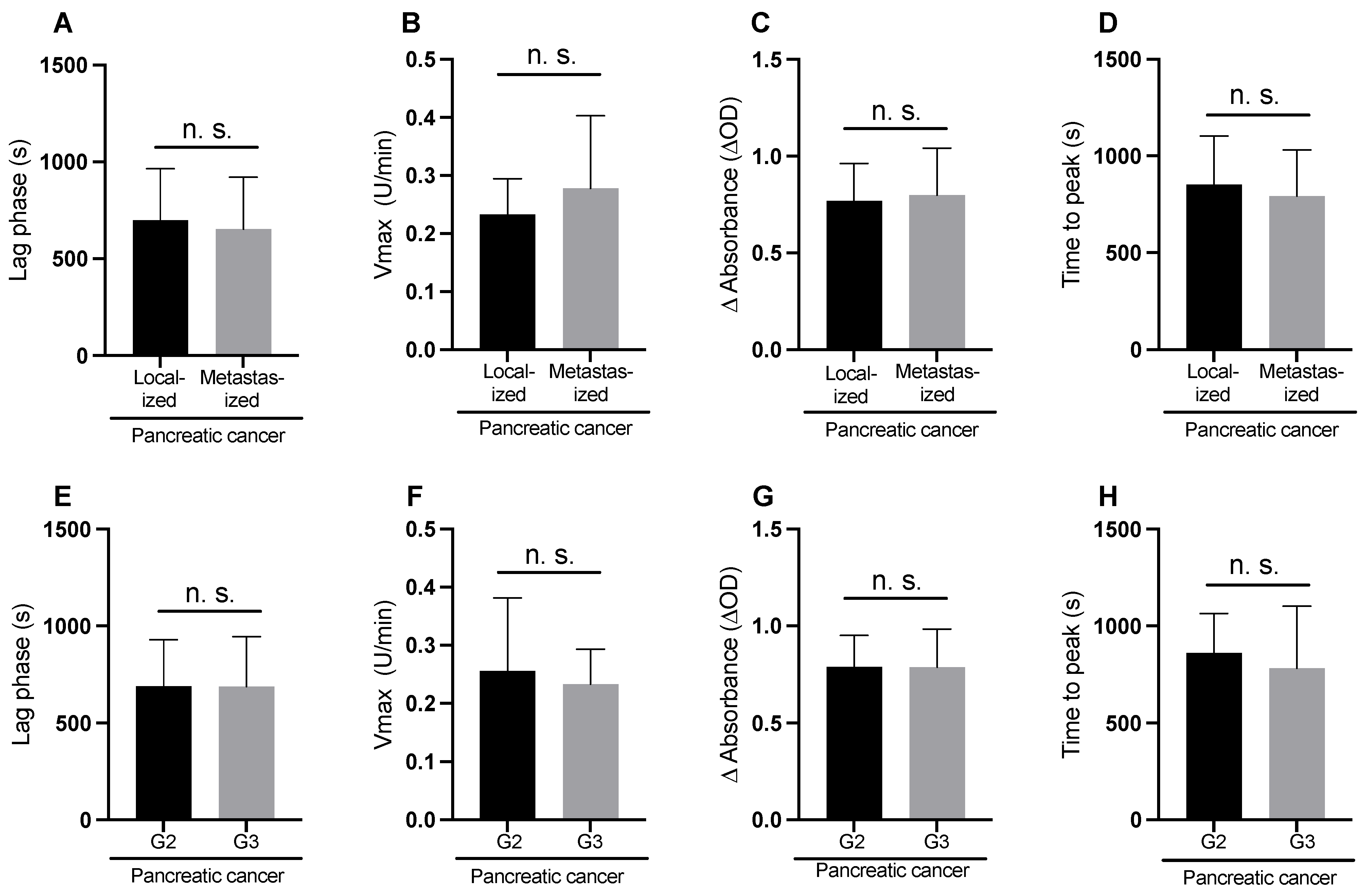
3.4. Modified Plasma Clot Formation Assay According to Tumor Stage and Grade
3.5. Standard Clot Formation Assay (Clotting Induced by CaCl2, Phospholipids, and Lipidated Tissue Factor)
3.6. Correlations between Plasma Clot Properties and Routine Laboratory Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Monroe, D.M.; Hoffman, M. The clotting system—A major player in wound healing. Haemophilia 2012, 18 (Suppl. S5), 11–16. [Google Scholar] [CrossRef]
- Spronk, H.M.; Govers-Riemslag, J.W.; ten Cate, H. The blood coagulation system as a molecular machine. Bioessays 2003, 25, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- Billroth, T. Lectures on Surgical Pathology and Therapeutics; The New Sydenham Society, 1878. [Google Scholar]
- Palumbo, J.S.; Kombrinck, K.W.; Drew, A.F.; Grimes, T.S.; Kiser, J.H.; Degen, J.L.; Bugge, T.H. Fibrinogen is an important determinant of the metastatic potential of circulating tumor cells. Blood 2000, 96, 3302–3309. [Google Scholar] [PubMed]
- Costantini, V.; Zacharski, L.R. The role of fibrin in tumor metastasis. Cancer Metastasis Rev. 1992, 11, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, J.S.; Talmage, K.E.; Massari, J.V.; La Jeunesse, C.M.; Flick, M.J.; Kombrinck, K.W.; Jirouskova, M.; Degen, J.L. Platelets and fibrin (ogen) increase metastatic potential by impeding natural killer cell-mediated elimination of tumor cells. Blood 2005, 105, 178–185. [Google Scholar] [CrossRef]
- De Souza, A.L.; Saif, M.W. Thromboembolism and pancreatic cancer. JOP 2014, 15, 292–294. [Google Scholar] [CrossRef]
- Khorana, A.A.; Fine, R.L. Pancreatic cancer and thromboembolic disease. Lancet Oncol. 2004, 5, 655–663. [Google Scholar] [CrossRef]
- Ay, C.; Dunkler, D.; Pirker, R.; Thaler, J.; Quehenberger, P.; Wagner, O.; Zielinski, C.; Pabinger, I. High D-dimer levels are associated with poor prognosis in cancer patients. Haematologica 2012, 97, 1158–1164. [Google Scholar] [CrossRef]
- Ay, C.; Pabinger, I.; Cohen, A.T. Cancer-associated venous thromboembolism: Burden, mechanisms, and management. Thromb. Haemost. 2017, 117, 219–230. [Google Scholar] [CrossRef]
- Wojtukiewicz, M.Z.; Rucinska, M.; Zacharski, L.R.; Kozlowski, L.; Zimnoch, L.; Piotrowski, Z.; Kudryk, B.J.; Kisiel, W. Localization of blood coagulation factors in situ in pancreatic carcinoma. Thromb. Haemost. 2001, 86, 1416–1420. [Google Scholar]
- Dvorak, H.F. Tumor Stroma, Tumor Blood Vessels, and Antiangiogenesis Therapy. Cancer J. 2015, 21, 237–243. [Google Scholar] [CrossRef]
- Nagy, J.A.; Brown, L.F.; Senger, D.R.; Lanir, N.; Van de Water, L.; Dvorak, A.M.; Dvorak, H.F. Pathogenesis of tumor stroma generation: A critical role for leaky blood vessels and fibrin deposition. Biochim. Biophys. Acta 1989, 948, 305–326. [Google Scholar] [CrossRef] [PubMed]
- Obonai, T.; Fuchigami, H.; Furuya, F.; Kozuka, N.; Yasunaga, M.; Matsumura, Y. Tumour imaging by the detection of fibrin clots in tumour stroma using an anti-fibrin Fab fragment. Sci. Rep. 2016, 6, 23613. [Google Scholar] [CrossRef] [PubMed]
- Kwaan, H.C.; Lindholm, P.F. Fibrin and Fibrinolysis in Cancer. Semin. Thromb. Hemost. 2019, 45, 413–422. [Google Scholar] [CrossRef]
- Date, K.; Hall, J.; Greenman, J.; Maraveyas, A.; Madden, L.A. Tumour and microparticle tissue factor expression and cancer thrombosis. Thromb. Res. 2013, 131, 109–115. [Google Scholar] [CrossRef]
- van Es, N.; Hisada, Y.; Di Nisio, M.; Cesarman, G.; Kleinjan, A.; Mahe, I.; Otten, H.M.; Kamphuisen, P.W.; Berckmans, R.J.; Buller, H.R.; et al. Extracellular vesicles exposing tissue factor for the prediction of venous thromboembolism in patients with cancer: A prospective cohort study. Thromb. Res. 2018, 166, 54–59. [Google Scholar] [CrossRef]
- Thaler, J.; Ay, C.; Mackman, N.; Metz-Schimmerl, S.; Stift, J.; Kaider, A.; Mullauer, L.; Gnant, M.; Scheithauer, W.; Pabinger, I. Microparticle-associated tissue factor activity in patients with pancreatic cancer: Correlation with clinicopathological features. Eur. J. Clin. Investig. 2013, 43, 277–285. [Google Scholar] [CrossRef]
- Wolberg, A.S. Thrombin generation and fibrin clot structure. Blood Rev. 2007, 21, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Gebhart, J.; Laczkovics, C.; Posch, F.; Ay, C.; Reitter-Pfoertner, S.E.; Haslacher, H.; Muszbek, L.; Wolberg, A.S.; Pabinger, I. Plasma clot properties in patients with a mild-to-moderate bleeding tendency of unknown cause. Ann. Hematol. 2015, 94, 1301–1310. [Google Scholar] [CrossRef]
- Undas, A.; Nowakowski, T.; Ciesla-Dul, M.; Sadowski, J. Abnormal plasma fibrin clot characteristics are associated with worse clinical outcome in patients with peripheral arterial disease and thromboangiitis obliterans. Atherosclerosis 2011, 215, 481–486. [Google Scholar] [CrossRef]
- Gray, L.D.; Hussey, M.A.; Larson, B.M.; Machlus, K.R.; Campbell, R.A.; Koch, G.; Ezban, M.; Hedner, U.; Wolberg, A.S. Recombinant factor VIIa analog NN1731 (V158D/E296V/M298Q-FVIIa) enhances fibrin formation, structure and stability in lipidated hemophilic plasma. Thromb. Res. 2011, 128, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Butenas, S.; Bouchard, B.A.; Brummel-Ziedins, K.E.; Parhami-Seren, B.; Mann, K.G. Tissue factor activity in whole blood. Blood 2005, 105, 2764–2770. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.; Xu, Q.; Qian, J.; Zhou, J.Y. Aberrant Factors of Fibrinolysis and Coagulation in Pancreatic Cancer. Onco Targets Ther. 2021, 14, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Tesselaar, M.E.; Romijn, F.P.; Van Der Linden, I.K.; Prins, F.A.; Bertina, R.M.; Osanto, S. Microparticle-associated tissue factor activity: A link between cancer and thrombosis? J. Thromb. Haemost. 2007, 5, 520–527. [Google Scholar] [CrossRef]
- Thaler, J.; Ay, C.; Mackman, N.; Bertina, R.M.; Kaider, A.; Marosi, C.; Key, N.S.; Barcel, D.A.; Scheithauer, W.; Kornek, G.; et al. Microparticle-associated tissue factor activity, venous thromboembolism and mortality in pancreatic, gastric, colorectal and brain cancer patients. J. Thromb. Haemost. 2012, 10, 1363–1370. [Google Scholar] [CrossRef]
- Bharthuar, A.; Khorana, A.A.; Hutson, A.; Wang, J.G.; Key, N.S.; Mackman, N.; Iyer, R.V. Circulating microparticle tissue factor, thromboembolism and survival in pancreaticobiliary cancers. Thromb. Res. 2013, 132, 180–184. [Google Scholar] [CrossRef]
- Rochefort, M.M.; Ankeny, J.S.; Kadera, B.E.; Donald, G.W.; Isacoff, W.; Wainberg, Z.A.; Hines, O.J.; Donahue, T.R.; Reber, H.A.; Tomlinson, J.S. Impact of tumor grade on pancreatic cancer prognosis: Validation of a novel TNMG staging system. Ann. Surg. Oncol. 2013, 20, 4322–4329. [Google Scholar] [CrossRef]
- Matsuno, S.; Egawa, S.; Fukuyama, S.; Motoi, F.; Sunamura, M.; Isaji, S.; Imaizumi, T.; Okada, S.; Kato, H.; Suda, K.; et al. Pancreatic Cancer Registry in Japan: 20 years of experience. Pancreas 2004, 28, 219–230. [Google Scholar] [CrossRef]
- Lee, R.D.; Barcel, D.A.; Williams, J.C.; Wang, J.G.; Boles, J.C.; Manly, D.A.; Key, N.S.; Mackman, N. Pre-analytical and analytical variables affecting the measurement of plasma-derived microparticle tissue factor activity. Thromb. Res. 2012, 129, 80–85. [Google Scholar] [CrossRef]
- Chen, V.M.; Hogg, P.J. Encryption and decryption of tissue factor. J. Thromb. Haemost. 2013, 11 (Suppl. S1), 277–284. [Google Scholar] [CrossRef]
- Khorana, A.A.; Francis, C.W.; Menzies, K.E.; Wang, J.G.; Hyrien, O.; Hathcock, J.; Mackman, N.; Taubman, M.B. Plasma tissue factor may be predictive of venous thromboembolism in pancreatic cancer. J. Thromb. Haemost. 2008, 6, 1983–1985. [Google Scholar] [CrossRef] [PubMed]
- Nopp, S.; Kraemmer, D.; Ay, C. Factor XI Inhibitors for Prevention and Treatment of Venous Thromboembolism: A Review on the Rationale and Update on Current Evidence. Front. Cardiovasc. Med. 2022, 9, 903029. [Google Scholar] [CrossRef] [PubMed]
- Verhamme, P.; Yi, B.A.; Segers, A.; Salter, J.; Bloomfield, D.; Buller, H.R.; Raskob, G.E.; Weitz, J.I.; Investigators, A.-T. Abelacimab for Prevention of Venous Thromboembolism. N. Engl. J. Med. 2021, 385, 609–617. [Google Scholar] [CrossRef]
- Braunwald, E. Inhibitors of factor XI: Game changers of anti-thrombotic therapy? Eur. Heart J. 2022, 44, 1018–1019. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pancreatic Cancer | Healthy | p-Value | |
|---|---|---|---|
| Basic Clinical Characteristics | |||
| Number, n | 40 | 40 | n.s. |
| Sex, female, n (%) | 23 (58%) | 23 (58%) | n.s. |
| Age, years | 66 (56–72) | 55 (44–62) | <0.001 |
| Tumor stage, n (%) | Localized: 21 (53%) Metastatic: 19 (47%) | - | - |
| Tumor differentiation, n (%) | High (G1): 0 Moderate (G2): 26 (65%) Poor (G3): 14 (35%) | - | - |
| Comorbidities, n (%) | Hypertension: 22 (55%) Diabetes: 11 (27.5%) Coronary heart disease: 4 (10%) COPD: 2 (5%) | - | - |
| Anticoagulation with low molecular weight heparin, n (%) | Prophylactic: 6 (15%) Therapeutic: 0 | ||
| Routine laboratory parameters (median, 25th–75th percentile) | |||
| Prothrombin time, % | 86 (76–112) | 92 (83–104) | n.s. |
| aPTT, s | 33.9 (31.8–38.9) | 34.5 (32.8–36.3) | n.s. |
| Fibrinogen, µg/mL | 418 (366–491) | 306 (264–352) | <0.001 |
| D-dimer, µg/ml | 1.38 (0.75–2.90) | 0.26 (0.26–0.41) | <0.001 |
| Platelet count, 109/L | 269 (212–348) | 274 (219–297) | n.s. |
| Leukocyte count (×109/L) | 6.32 (5.02–8.50) | 6.26(5.43–6.94) | n.s. |
| CRP (mg/dL) | 1.57 (0.34–2.96) | 0.10 (0.06–0.23) | <0.001 |
| Ca 19-9 (U/mL) | 235.5 (30.6–1102) | - | - |
| Pancreatic Cancer | Healthy | p-Value | |
|---|---|---|---|
| Plasma clot formation parameters (median, 25th–75th percentile) | |||
| - Modified plasma clot formation assay (addition of CaCl2 + phospholipids) | |||
| Lag phase (s) | 688 (606–925) | 736 (629–895) | n.s. |
| Vmax (U/min) | 0.235 (0.170–0.346) | 0.136 (0.116–0.185) | <0.001 |
| ΔAbs (ΔOD) | 0.789 (0.609–0.968) | 0.563 (0.450–0.652) | <0.001 |
| TTP (s) | 818 (726–1065) | 912 (741–1148) | n.s. |
| - Modified plasma clot formation assay + anti tissue factor antibody | |||
| Lag phase (s) | 799 (660–987) | 683 (550–853) | n.s. |
| Vmax (U/min) | 0.170 (0.132–0.259) | 0.139 (0.109–0.201) | 0.006 |
| ΔAbs (ΔOD) | 0.654 (0.541–0.840) | 0.528 (0.443–0.616) | 0.001 |
| TTP (s) | 933 (852–1088) | 867 (711–1107) | n.s. |
| - Standard plasma clot formation assay (addition of CaCl2 + phospholipids + lipidated tissue factor) | |||
| Lag phase (s) | 267 (235–319) | 182 (162–206) | <0.001 |
| Vmax (U/min) | 0.209 (0.151–0.273) | 0.216 (0.163–0.237) | 0.86 |
| ΔAbs (ΔOD) | 0.801 (0.685–0.103) | 0.730 (0.589–0.794) | 0.03 |
| TTP (s) | 390 (340–482) | 294 (260–314) | <0.001 |
| (A) Modified Plasma Clot Formation Assay | (B) Modified Plasma Clot Formation Assay + Tissue Factor Blocking Antibody | (C) Standard Plasma Clot Formation Assay | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vmax | ΔAbs | Lag Phase | Time to Peak | Vmax | ΔAbs | Lag Phase | Time to Peak | Vmax | ΔAbs | Lag Phase | Time to Peak | |
| Prothrombin time, % | 0.359 * | 0.362 * | −0.041 | 0.071 | 0.434 * | 0.261 | −0.101 | −0.018 | 0.322 | 0.285 | −0.211 | −0.78 |
| aPTT, s | 0.108 | −0.114 | 0.019 | 0.002 | −0.123 | −0.145 | −0.097 | −0.090 | −0.0105 | −0.150 | −0.064 | 0.152 |
| Fibrinogen, mg/dL | 0.126 | 0.541 ** | 0.307 | 0.255 | 0.326 | 0.605 ** | 0.128 | 0.112 | 0.597 *** | 0.768 *** | 0.170 | 0.144 |
| D-dimer, μg/mL | 0.395 * | 0.164 | −0.262 | −0.226 | 0.318 * | 0.145 | −0.192 | −0.334 * | 0.042 | −0.045 | 0.274 | 0.206 |
| Platelet count, G/L | 0.049 | 0.119 | 0.081 | 0.020 | −0.134 | 0.104 | 0.035 | −0.013 | 0.131 | 0.190 | 0.052 | 0.124 |
| Leukocyte count (×109/L) | 0.276 | 0.037 | −0.130 | −0.280 | 0.086 | −0.091 | −0.071 | −0.197 | −0.006 | 0.321 | 0.207 | 0.239 |
| CRP (mg/dL) | 0.350 | 0.217 | −0.121 | −0.103 | 0.313 | 0.217 | −0.071 | −0.344 | 0.411 * | 0.223 | 0.143 | 0.092 |
| Ca 19-9 | 0.097 | 0.102 | 0.071 | 0.033 | −0.065 | 0.095 | −0.059 | 0.056 | 0.325 * | 0.093 | 0.089 | −0.082 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thaler, J.; Prager, G.; Pabinger, I.; Ay, C. Plasma Clot Properties in Patients with Pancreatic Cancer. Cancers 2023, 15, 4030. https://doi.org/10.3390/cancers15164030
Thaler J, Prager G, Pabinger I, Ay C. Plasma Clot Properties in Patients with Pancreatic Cancer. Cancers. 2023; 15(16):4030. https://doi.org/10.3390/cancers15164030
Chicago/Turabian StyleThaler, Johannes, Gerald Prager, Ingrid Pabinger, and Cihan Ay. 2023. "Plasma Clot Properties in Patients with Pancreatic Cancer" Cancers 15, no. 16: 4030. https://doi.org/10.3390/cancers15164030
APA StyleThaler, J., Prager, G., Pabinger, I., & Ay, C. (2023). Plasma Clot Properties in Patients with Pancreatic Cancer. Cancers, 15(16), 4030. https://doi.org/10.3390/cancers15164030