

Xpert Bladder Cancer Monitor for the Early Detection of Non-Muscle Invasive Bladder Cancer Recurrences: Could Cystoscopy Be Substituted?

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
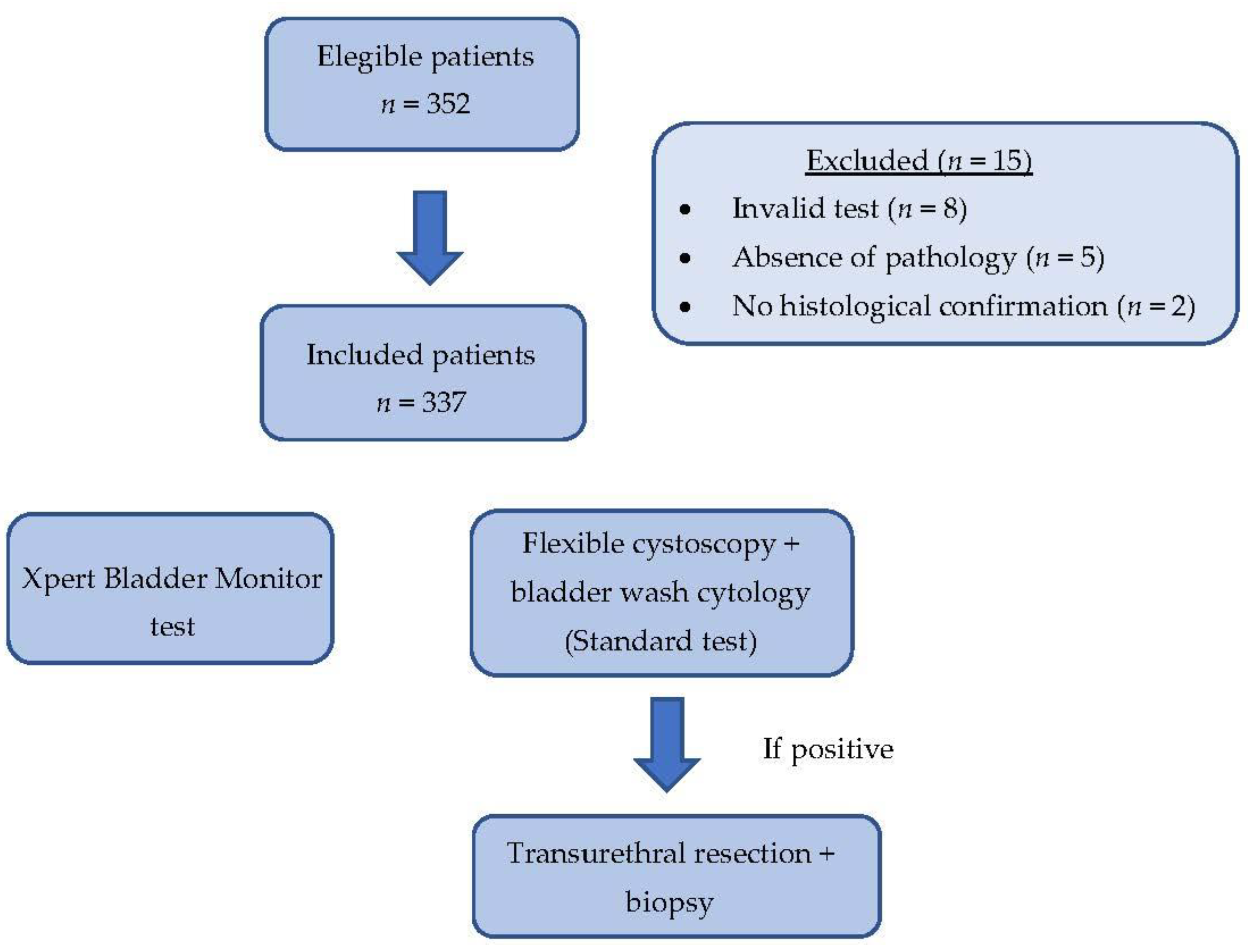
2.1. Design, Setting, and Participants
2.2. Diagnostic Procedure
2.3. Adjuvant Preventive Treatment for Recurrences
2.4. Follow-Up for Detection of Recurrences
2.5. Recurrence Suspicion and Diagnosis
2.6. XBM Assessment
2.7. XBM “False Positives” Follow-Up
2.8. Statistical Analyses
3. Results
3.1. Characteristics of Analyzed Population
3.2. Performance of XBM
3.3. Prediction of Risk of Recurrence
3.4. Follow Up on False Positives of XBM
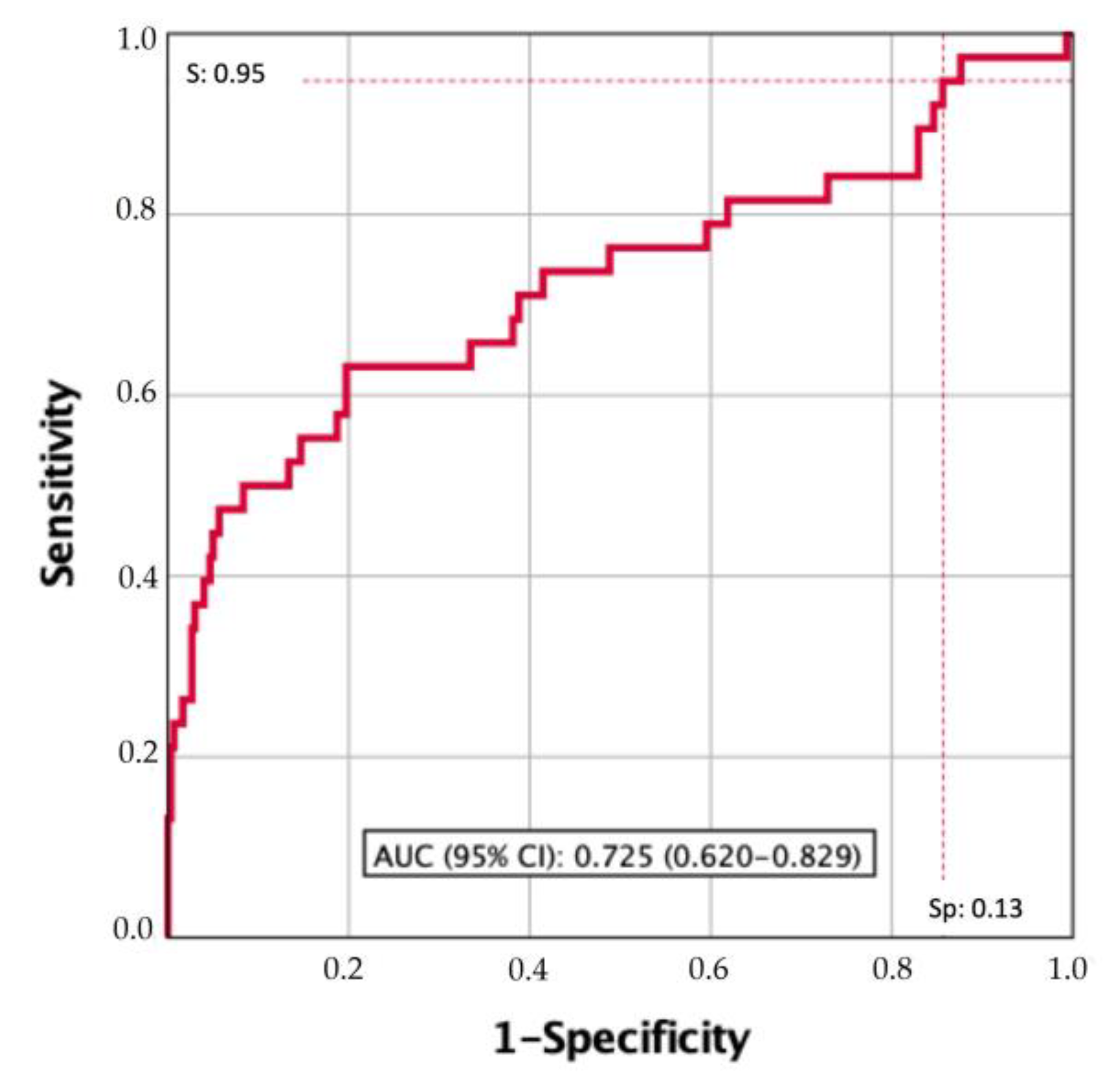
3.5. Searching for a Clinically Useful XBM Cutoff
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Pérez, M.; Souza, D.; Romero-Fernández, F.; Gómez-Bernal, G.; Gómez-Bernal, F. Estimación de las proyecciones del cáncer de vejiga en España. Actas Urol Esp 2013, 37, 286–291. [Google Scholar] [CrossRef]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef]
- Compérat, E.; Larré, S.; Rouprêt, M.; Neuzillet, Y.; Pignot, G.; Quintens, H.; Houede, N.; Roy, C.; Durand, X.; Varinot, J.; et al. Clinicopathological characteristics of urothelial bladder cancer in patients less than 40 years old. Virchows Arch. 2015, 466, 589–594. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, H.; Sun, G.; Zhang, X.; Zhao, J.; Liu, J.; Shen, P.; Shi, M.; Zeng, H. Comparison of the prognosis of primary and progressive muscle-invasive bladder cancer after radical cystectomy: A systematic review and meta-analysis. Int. J. Surg. 2018, 52, 214–220. [Google Scholar] [CrossRef]
- Burke, D.M.; Shackley, D.C.; O’Reilly, P.H. The community-based morbidity of flexible cystoscopy. BJU Int. 2002, 89, 347–349. [Google Scholar] [CrossRef]
- Herr, H.W.; Donat, S.M.; Dalbagni, G. Correlation of Cystoscopy with Histology of Recurrent Papillary Tumors of the Bladder. J. Urol. 2002, 168, 978–980. [Google Scholar] [CrossRef]
- Karakiewicz, P.I.; Benayoun, S.; Zippe, C.; Ludecke, G.; Boman, H.; Sanchez-Carbayo, M.; Casella, R.; Mian, C.; Friedrich, M.G.; Eissa, S.; et al. Institutional variability in the accuracy of urinary cytology for predicting recurrence of transitional cell carcinoma of the bladder. BJU Int. 2006, 97, 997–1001. [Google Scholar] [CrossRef]
- Bensalah, K.; Montorsi, F.; Shariat, S.F. Challenges of Cancer Biomarker Profiling {A Figure Is Presented}. Eur. Urol. 2007, 52, 1601–1609. [Google Scholar] [CrossRef]
- Sarosdy, M.; deVere White, R.D.; Soloway, M.S.; Sheinfeld, J.; Hudson, M.; Schell-er, P.F.; Jarowenko, M.; Adams, G.; Blumenstein, B.A.; Ellis, W.J.; et al. Results of A Multicenter Trial Using The Bta Test to Monitor for and Dmxvose Recurrent Bladder Cancer. J. Urol. 1995, 154, 379–384. [Google Scholar] [CrossRef]
- Raitanen, M.-P.; Aine, R.; Rintala, E.; Kallio, J.; Rajala, P.; Juusela, H.; Tammela, T.L.; FinnBladder Group. Differences Between Local and Review Urinary Cytology in Diagnosis of Bladder Cancer. An Interobserver Multicenter Analysis. Eur. Urol. 2002, 41, 284–289. [Google Scholar] [CrossRef]
- Soukup, V.; Čapoun, O.; Cohen, D.; Hernández, V.; Burger, M.; Compérat, E.; Gontero, P.; Lam, T.; Mostafid, A.H.; Palou, J.; et al. Risk Stratification Tools and Prognostic Models in Non–muscle-invasive Bladder Cancer: A Critical Assessment from the European Association of Urology Non-muscle-invasive Bladder Cancer Guidelines Panel. Eur. Urol. Focus 2020, 6, 479–489. [Google Scholar] [CrossRef]
- Hollenbeck, B.K.; Dunn, R.L.; Ye, Z.; Hollingsworth, J.M.; Skolarus, T.A.; Kim, S.P.; Montie, J.E.; Lee, C.T.; Wood, D.P.; Miller, D.C. Delays in diagnosis and bladder cancer mortality. Cancer 2010, 116, 5235–5242. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Compérat, E.; Gontero, P.; Mostafid, A.H.; Palou, J.; Van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. Non-Muscle-Invasive Bladder Cancer (TaT1 and CIS) EAU Guidelines. Eur. Urol. 2022, 31, 1–48. [Google Scholar]
- Daneshmand, S.; Konety, B.R. American Urological Association (AUA) Guideline American Urological Association Non-Muscle Invasive Bladder Cancer; American Urological Association: Linthicum, MD, USA, 2016; pp. 1–45. [Google Scholar]
- Soria, F.; Droller, M.J.; Lotan, Y.; Gontero, P.; D’andrea, D.; Gust, K.M.; Rouprêt, M.; Babjuk, M.; Palou, J.; Shariat, S.F. An up-to-date catalog of available urinary biomarkers for the surveillance of non-muscle invasive bladder cancer. World J. Urol. 2018, 36, 1981–1995. [Google Scholar] [CrossRef]
- Compérat, E.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; Palou, J.; Van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R. Non-Muscle-Invasive Bladder Cancer (TaT1 and CIS) EAU Guidelines On; EAU: Arnhem, The Netherlands, 2022. [Google Scholar]
- Lotan, Y.; Black, P.C.; Caba, L.; Chang, S.S.; Cookson, M.S.; Daneshmand, S.; Kamat, A.M.; McKiernan, J.M.; Pruthi, R.S.; Ritch, C.R.; et al. Optimal Trial Design for Studying Urinary Markers in Bladder Cancer: A Collaborative Review. Eur. Urol. Oncol. 2018, 1, 223–230. [Google Scholar] [CrossRef]
- Van Rhijn, B.W.; van der Poel, H.G.; van der Kwast, T.H. Urine Markers for Bladder Cancer Surveillance: A Systematic Review. Eur. Urol. 2005, 47, 736–748. [Google Scholar] [CrossRef]
- Mbeutcha, A.; Lucca, I.; Mathieu, R.; Lotan, Y.; Shariat, S.F. Current Status of Urinary Biomarkers for Detection and Surveillance of Bladder Cancer. Urol. Clin. North Am. 2016, 43, 47–62. [Google Scholar] [CrossRef]
- Gontero, P.; Montanari, E.; Roupret, M.; Longo, F.; Stockley, J.; Kennedy, A.; Rodriguez, O.; McCracken, S.R.; Dudderidge, T.; Sieverink, C.; et al. Comparison of the performances of the ADXBLADDER test and urinary cytology in the follow-up of non-muscle-invasive bladder cancer: A blinded prospective multicentric study. BJU Int. 2020, 127, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-L.; Wang, X.-L.; Yang, X.-H.; Wu, X.-H.; He, G.-X.; Xie, L.-M.; Cao, X.-J.; Guo, X.-G. Pooled analysis of Xpert Bladder Cancer based on the 5 mRNAs for rapid diagnosis of bladder carcinoma. World J. Surg. Oncol. 2021, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Koya, M.; Osborne, S.; Chemasle, C.; Porten, S.; Schuckman, A.; Kennedy-Smith, A. An evaluation of the real world use and clinical utility of the Cxbladder Monitor assay in the follow-up of patients previously treated for bladder cancer. BMC Urol. 2020, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Righetto, M.; Zumerle, S.; Montopoli, M.; Zattoni, F. The Bladder EpiCheck Test as a Non-Invasive Tool Based on the Identification of DNA Methylation in Bladder Cancer Cells in the Urine: A Review of Published Evidence. Int. J. Mol. Sci. 2020, 21, 6542. [Google Scholar] [CrossRef]
- Wolfs, J.R.E.; Hermans, T.J.N.; Koldewijn, E.L.; van de Kerkhof, D. Novel urinary biomarkers ADXBLADDER and bladder EpiCheck for diagnostics of bladder cancer: A review. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 161–170. [Google Scholar] [CrossRef]
- Leiblich, A. Recent Developments in the Search for Urinary Biomarkers in Bladder Cancer. Curr. Urol. Rep. 2017, 18, 100. [Google Scholar] [CrossRef]
- Van Valenberg, F.J.P.; Hiar, A.M.; Wallace, E.; Bridge, J.A.; Mayne, D.J.; Beqaj, S.; Sexton, W.J.; Lotan, Y.; Weizer, A.Z.; Jansz, G.K.; et al. Prospective Validation of an mRNA-based Urine Test for Surveillance of Patients with Bladder Cancer. Eur. Urol. 2019, 75, 853–860. [Google Scholar] [CrossRef]
- Bartel, D.P. MicroRNAs: Target Recognition and Regulatory Functions. Cell 2009, 136, 215–233. [Google Scholar] [CrossRef]
- Martin, D.; Jansson, A.H.L. MicroRNA and Cancer. Mol. Oncol. 2012, 6, 590–610. [Google Scholar] [CrossRef]
- Hanke, M.; Hoefig, K.; Merz, H.; Feller, A.C.; Kausch, I.; Jocham, D.; Warnecke, J.M.; Sczakiel, G. A robust methodology to study urine microRNA as tumor marker: microRNA-126 and microRNA-182 are related to urinary bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2010, 28, 655–661. [Google Scholar] [CrossRef]
- Gottardo, F.; Liu, C.G.; Ferracin, M.; Calin, G.A.; Fassan, M.; Bassi, P.; Sevignani, C.; Byrne, D.; Negrini, M.; Pagano, F.; et al. Micro-RNA profiling in kidney and bladder cancers. Urol. Oncol. Semin. Orig. Investig. 2007, 25, 387–392. [Google Scholar] [CrossRef]
- Yates, D.R.; Rehman, I.; Abbod, M.F.; Meuth, M.; Cross, S.S.; Linkens, D.A.; Hamdy, F.C.; Catto, J.W.F. Promoter Hypermethylation Identifies Progression Risk in Bladder Cancer. Clin. Cancer Res. 2007, 13, 2046–2053. [Google Scholar] [CrossRef]
- Catto, J.W.F.; Abbod, M.F.; Wild, P.J.; Linkens, D.A.; Pilarsky, C.; Rehman, I.; Rosario, D.J.; Denzinger, S.; Burger, M.; Stoehr, R.; et al. The Application of Artificial Intelligence to Microarray Data: Identification of a Novel Gene Signature to Identify Bladder Cancer Progression. Eur. Urol. 2010, 57, 398–406. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Laukhtina, E.; Shim, S.R.; Mori, K.; D‘andrea, D.; Soria, F.; Rajwa, P.; Mostafaei, H.; Compérat, E.; Cimadamore, A.; Moschini, M.; et al. Diagnostic Accuracy of Novel Urinary Biomarker Tests in Non–muscle-invasive Bladder Cancer: A Systematic Review and Network Meta-analysis. Eur. Urol. Oncol. 2021, 4, 927–942. [Google Scholar] [CrossRef]
- Van der Aa, M.N.; Steyerberg, E.W.; Bangma, C.; van Rhijn, B.W.; Zwarthoff, E.C.; van der Kwast, T.H. Cystoscopy Revisited as the Gold Standard for Detecting Bladder Cancer Recurrence: Diagnostic Review Bias in the Randomized, Prospective CEFUB Trial. J. Urol. 2010, 183, 76–80. [Google Scholar] [CrossRef]
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Roupret, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef]
- Mowatt, G.; Zhu, S.; Kilonzo, M.; Boachie, C.; Fraser, C.; Griffiths, T.; N’Dow, J.; Nabi, G.; Cook, J.; Vale, L. Systematic review of the clinical effectiveness and cost-effectiveness of photodynamic diagnosis and urine biomarkers (FISH, ImmunoCyt, NMP22) and cytology for the detection and follow-up of bladder cancer. Health Technol. Assess. 2010, 14, 1–331. [Google Scholar] [CrossRef]
- Compérat, E.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; Palou, J.; Van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. Non-Muscle-Invasive Bladder Cancer (TaT1 and CIS) EAU Guidelines On; EAU: Arnhem, The Netherlands, 2021. [Google Scholar]
- Niwa, N.; Matsumoto, K.; Hayakawa, N.; Ito, Y.; Maeda, T.; Akatsuka, S.; Masuda, T.; Nakamura, S.; Tanaka, N. Comparison of outcomes between ultrasonography and cystoscopy in the surveillance of patients with initially diagnosed TaG1-2 bladder cancers: A matched-pair analysis. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 386.e15–386.e21. [Google Scholar] [CrossRef]
- Roupret, M.; Gontero, P.; McCracken, S.R.C.; Dudderidge, T.; Stockley, J.; Kennedy, A.; Rodriguez, O.; Sieverink, C.; Vanié, F.; Allasia, M.; et al. Diagnostic Accuracy of MCM5 for the Detection of Recurrence in Nonmuscle Invasive Bladder Cancer Followup: A Blinded, Prospective Cohort, Multicenter European Study. J. Urol. 2020, 204, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Pichler, R.; Fritz, J.; Tulchiner, G.; Klinglmair, G.; Soleiman, A.; Horninger, W.; Klocker, H.; Heidegger, I. Increased accuracy of a novel mRNA-based urine test for bladder cancer surveillance. BJU Int. 2018, 121, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Morote, J.; Cornel, E.B.; Gakis, G.; van Valenberg, F.J.P.; Lozano, F.; Sternberg, I.A.; Willemsen, E.; Hegemann, M.L.; Paitan, Y.; et al. Performance of the Bladder EpiCheck™ Methylation Test for Patients Under Surveillance for Non–muscle-invasive Bladder Cancer: Results of a Multicenter, Prospective, Blinded Clinical Trial. Eur. Urol. Oncol. 2018, 1, 307–313. [Google Scholar] [CrossRef]
- López-Beltrán, A.; Cheng, L.; Gevaert, T.; Blanca, A.; Cimadamore, A.; Santoni, M.; Massari, F.; Scarpelli, M.; Raspollini, M.R.; Montironi, R. Current and emerging bladder cancer biomarkers with an emphasis on urine biomarkers. Expert Rev. Mol. Diagn. 2020, 20, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Catto, J.W.; Alcaraz, A.; Bjartell, A.S.; White, R.D.V.; Evans, C.P.; Fussel, S.; Hamdy, F.C.; Kallioniemi, O.; Mengual, L.; Schlomm, T.; et al. MicroRNA in Prostate, Bladder, and Kidney Cancer: A Systematic Review. Eur. Urol. 2011, 59, 671–681. [Google Scholar] [CrossRef]
- Weber, J.A.; Baxter, D.H.; Zhang, S.; Huang, D.Y.; Huang, K.H.; Lee, M.J.; Galas, D.J.; Wang, K. The MicroRNA Spectrum in 12 Body Fluids. Clin. Chem. 2010, 56, 1733–1741. [Google Scholar] [CrossRef]
- Wallace, E.; Higuchi, R.; Satya, M.; McCann, L.; Sin, M.L.; Bridge, J.A.; Wei, H.; Zhang, J.; Wong, E.; Hiar, A.; et al. Development of a 90-Minute Integrated Noninvasive Urinary Assay for Bladder Cancer Detection. J. Urol. 2018, 199, 655–662. [Google Scholar] [CrossRef]
- D’elia, C.; Folchini, D.M.; Mian, C.; Hanspeter, E.; Schwienbacher, C.; Spedicato, G.A.; Pycha, S.; Vjaters, E.; Degener, S.; Kafka, M.; et al. Diagnostic value of Xpert® Bladder Cancer Monitor in the follow-up of patients affected by non-muscle invasive bladder cancer: An update. Ther. Adv. Urol. 2021, 13, 1756287221997183. [Google Scholar] [CrossRef]
- D´elia, C.; Pycha, A.; Folchini, D.M.; Mian, C.; Hanspeter, E.; Schwienbacher, C.; Vjaters, E.; Pycha, A.; Trenti, E. Diagnostic predictive value of Xpert Bladder Cancer Monitor in the follow-up of patients affected by non-muscle invasive bladder cancer. J. Clin. Pathol. 2019, 72, 140–144. [Google Scholar] [CrossRef]
- Cancel-Tassin, G.; Roupret, M.; Pinar, U.; Gaffory, C.; Vanie, F.; Ondet, V.; Compérat, E.; Cussenot, O. Assessment of Xpert Bladder Cancer Monitor test performance for the detection of recurrence during non-muscle invasive bladder cancer follow-up. World J. Urol. 2021, 39, 3329–3335. [Google Scholar] [CrossRef]
- Hurle, R.; Casale, P.; Saita, A.; Colombo, P.; Elefante, G.M.; Lughezzani, G.; Fasulo, V.; Paciotti, M.; Domanico, L.; Bevilacqua, G.; et al. Clinical performance of Xpert Bladder Cancer (BC) Monitor, a mRNA-based urine test, in active surveillance (AS) patients with recurrent non-muscle-invasive bladder cancer (NMIBC): Results from the Bladder Cancer Italian Active Surveillance (BIAS) project. World J. Urol. 2020, 38, 2215–2220. [Google Scholar] [CrossRef]
- Pichler, R.; Fritz, J.; Tulchiner, G.; Klinglmair, G.; Soleiman, A.; Horninger, W.; Klocker, H.; Heidegger, I.; Wallace, E.; Higuchi, R.G.; et al. Prospective Validation of an MRNA-Based Urine Test for Surveillance of Patients with Bladder Cancer. Eur. Urol. 2021, 128, 853–860. [Google Scholar]
- Lotan, Y.; Roehrborn, C.G. Sensitivity and specificity of commonly available bladder tumor markers versus cytology: Results of a comprehensive literature review and meta-analyses. Urology 2003, 61, 109–118. [Google Scholar] [CrossRef]
- Benderska-Söder, N.; Hovanec, J.; Pesch, B.; Goebell, P.J.; Roghmann, F.; Noldus, J.; Rabinovich, J.; Wichert, K.; Gleichenhagen, J.; Käfferlein, H.U.; et al. Toward noninvasive follow-up of low-risk bladder cancer—Rationale and concept of the UroFollow trial. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 886–895. [Google Scholar] [CrossRef]
- Kamat, A.M.; Karakiewicz, P.I.; Xylinas, E.; Hegarty, P.K.; Hegarty, N.; Jenkins, L.C.; Droller, M.; van Rhijn, B.W.; Shariat, S.F.; Schmitz-Dräger, B.J.; et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Screening, Diagnosis, and Molecular Markers. Eur. Urol. 2012, 63, 4–15. [Google Scholar] [CrossRef]
- Lotan, Y.; Roehrborn, C.G. Cost-effectiveness of a modified care protocol substituting bladder tumor markers for cystoscopy for the follow up of patients with transitional cell carcinoma of the bladder: A decision analytical approach. J. Urol. 2002, 167, 75–79. [Google Scholar] [CrossRef]
- Nam, R.K.; Redelmeier, D.A.; Spiess, P.E.; Sampson, H.A.; Fradet, Y.; Jewett, M.A.S. Comparison of molecular and conventional strategies for follow up of superficial bladder cancer using decision analysis. J. Urol. 2000, 163, 752–757. [Google Scholar] [CrossRef]
- Van der Aa, M.N.; Steyerberg, E.W.; Sen, E.F.; Zwarthoff, E.C.; Kirkels, W.J.; van der Kwast, T.H.; Essink-Bot, M.-L. Patients’ perceived burden of cystoscopic and urinary surveillance of bladder cancer: A randomized comparison. BJU Int. 2008, 101, 1106–1110. [Google Scholar] [CrossRef]
- Koo, K.; Zubkoff, L.; Sirovich, B.E.; Goodney, P.P.; Robertson, D.J.; Seigne, J.D.; Schroeck, F.R. The Burden of Cystoscopic Bladder Cancer Surveillance: Anxiety, Discomfort, and Patient Preferences for Decision Making. Urology 2017, 108, 122–128. [Google Scholar] [CrossRef]
- Burger, M.; Grossman, H.B.; Droller, M.; Schmidbauer, J.; Hermann, G.; Drăgoescu, O.; Ray, E.; Fradet, Y.; Karl, A.; Burgués, J.P.; et al. Photodynamic Diagnosis of Non–muscle-invasive Bladder Cancer with Hexaminolevulinate Cystoscopy: A Meta-analysis of Detection and Recurrence Based on Raw Data. Eur. Urol. 2013, 64, 846–854. [Google Scholar] [CrossRef]
- Van Osch, F.H.M.; Nekeman, D.; Aaronson, N.K.; Billingham, L.J.; James, N.D.; Cheng, K.K.; Bryan, R.T.; Zeegers, M.P. Patients choose certainty over burden in bladder cancer surveillance. World J. Urol. 2019, 37, 2747–2753. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.S.; Teo, C.H.; Chan, D.; Heinrich, M.; Feber, A.; Sarpong, R.; Allan, J.; Williams, N.; Brew-Graves, C.; Ng, C.J.; et al. Mixed-methods approach to exploring patients’ perspectives on the acceptability of a urinary biomarker test in replacing cystoscopy for bladder cancer surveillance. BJU Int. 2019, 124, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, R.J.; Oosterlinck, W.; Holmang, S.; Sydes, M.R.; Birtle, A.; Gudjonsson, S.; De Nunzio, C.; Okamura, K.; Kaasinen, E.; Solsona, E.; et al. Systematic Review and Individual Patient Data Meta-analysis of Randomized Trials Comparing a Single Immediate Instillation of Chemotherapy After Transurethral Resection with Transurethral Resection Alone in Patients with Stage pTa–pT1 Urothelial Carcinoma of the Bladder: Which Patients Benefit from the Instillation? Eur. Urol. 2016, 69, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Palou, J.; Brausi, M.; Catto, J.W. Management of Patients with Normal Cystoscopy but Positive Cytology or Urine Markers. Eur. Urol. Oncol. 2020, 3, 548–554. [Google Scholar] [CrossRef]
- Cowan, B.; Klein, E.; Jansz, K.; Westenfelder, K.; Bradford, T.; Peterson, C.; Scherr, D.; Karsh, L.I.; Egerdie, R.B.; Witjes, J.A.; et al. Longitudinal follow-up and performance validation of an mRNA-based urine test (Xpert ® Bladder Cancer Monitor) for surveillance in patients with non-muscle-invasive bladder cancer. BJU Int. 2021, 128, 713–721. [Google Scholar] [CrossRef]
- Todenhöfer, T.; Hennenlotter, J.; Guttenberg, P.; Mohrhardt, S.; Kuehs, U.; Esser, M.; Aufderklamm, S.; Bier, S.; Harland, N.; Rausch, S.; et al. Prognostic relevance of positive urine markers in patients with negative cystoscopy during surveillance of bladder cancer. BMC Cancer 2015, 15, 155. [Google Scholar] [CrossRef]
- Gopalakrishna, A.; Fantony, J.J.; Longo, T.A.; Owusu, R.; Foo, W.-C.; Dash, R.; Denton, B.T.; Inman, B.A. Anticipatory Positive Urine Tests for Bladder Cancer. Ann. Surg. Oncol. 2017, 24, 1747–1753. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Median age, years (IQR) | 73 (65–80) |
| Gender, n (%) | |
| Male | 274 (81.1) |
| Female | 64 (18.9) |
| Smoke habit, n (%) | |
| Smoker/former smoker | 261 (77.2) |
| Non- smoker | 77 (22.8) |
| Type of tumour, n (%) | |
| Primary | 231 (68.3) |
| Recurrence within one year follow-up | 64 (18.9) |
| Recurrence later than one year follow-up | 43 (12.7) |
| Previous number of recurrences | |
| One | 63 (58.9) |
| Two or more | 44 (41.1) |
| EORTC * risk of recurrence and progression, n (%) | |
| Low | 84 (24.9) |
| Intermediate | 67 (19.8) |
| High | 187 (55.3) |
| Pathological stage, n (%) | |
| Ta | 156 (47.1) |
| T1 | 115 (34) |
| CIS ** | 12 (3.6) |
| Tx | 55 (16.3) |
| Pathological grade, n (%) | |
| Low | 153 (45.3) |
| High | 185 (54.7) |
| Adjuvant treatment, n (%) | |
| Postoperative Mytomicin C | 128 (38) |
| No | 152 (45) |
| BCG *** | 159 (47) |
| Mytomicin C | 18 (5.3) |
| Systemic immunotherapy | 9 (2.7) |
| Recurrences diagnosed at the time of XBM assessment, n (%) | |
| Any recurrence | 49 (14.5) |
| High-risk recurrence | 22 (6.5) |
| No recurrence | 266 (79) |
| Recurrences diagnosed within one year follow-up, n (%) | |
| Any recurrence | 33 (9.8) |
| High-risk recurrence | 16 (5.6) |
| Variable | Xpert Bladder Monitor | |
|---|---|---|
| Grade | Positive | Negative |
| Low Grade, n (%) | 20/27 (74.1) | 7/27 (25.9) |
| High Grade, n (%) | 14/22 (63.6) | 8/22 (36.4) |
| Pathological stage | ||
| Ta, n (%) | 19/27 (70.4) | 8/27 (29.6) |
| Tx, n (%) | 6/7 (85.7) | 1/7 (14.3) |
| Tis *, n (%) | 4/4 (100) | 0/4 (0) |
| T1, n (%) | 3/9 (33.3) | 6/9 (66.7) |
| T2, n (%) | 2/2 (100) | 0/2 (100) |
| Parameter | All Recurrences | High-Risk Recurrences | ||
|---|---|---|---|---|
| XBM | Cystoscopy and Washing Cytology | XBM | Cystoscopy and Washing Cytology | |
| Sensitivity, n (%) | 34/49 (69.4) | 49/49 (100) | 14/22 (63.6) | 22/22 (100) |
| Specificity, n (%) | 198/288 (68.8) | 278/288 (96.5) | 205/315 (65.1) | 278/315 (88.3) |
| Positive predictive value, n (%) | 34/124 (27.4) | 49/59 (83.1) | 14/124 (11.3) | 22/59 (37.3) |
| Negative predictive value, n (%) | 198/213 (93.0) | 278/278 (100) | 205/213 (96.2) | 278/278 (100) |
| Accuracy, n (%) | 232/337 (68.8) | 327/337 (97.0) | 219/337 (65.0) | 300/337 (89) |
| Avoided diagnostic procedures, n (%) | 213/337 (63.2) | 0 (0) | 213/337 (63.2) | 0 (0) |
| Missed recurrences, n (%) | 15/49 (30.6) | 0 (0) | 8/22 (36.4) | 0 (0) |
| Method of Suspicion | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Odd Ratio (95% CI) | p Value | Odd Ratio (95% CI) | p Value | |
| For any type of recurrence | ||||
| XBM | 4.987 (2.586–9.616) | =0.001 | 3.585 (0.820–15.675) | =0.090 |
| Cystoscopy | 615.524 (153.624–2466.212) | <0.001 | 1517.105 (175.210–13136.239) | <0.001 |
| Washing cytology | 15.975 (4.700–54.296) | <0.001 | 100.409 (7.207–1398.817) | =0.110 |
| For high-risk recurrences | ||||
| XBM | 3.261 (1.327–8.014) | =0.007 | 0.723 (0.226–2.312) | =0.585 |
| Cystoscopy | 52.343 (14.720–186.124) | =0.001 | 53.712 (13.243–217.851) | <0.001 |
| Washing cytology | 24.033 (7.186–80.377) | =0.001 | 22.473 (3.530–143.048) | =0.001 |
| Sensitivity (%) | Specificity (%) | Cutoff |
|---|---|---|
| 100 | 7.1 | 0.1117 |
| 95 | 13.4 | 0.1294 |
| 90 | 15.4 | 0.1459 |
| 85 | 17.1 | 0.6661 |
| 80 | 38.1 | 0.2950 |
| 75 | 51.2 | 0.3950 |
| 63 | 66.6 | 0.5000 |
| Parameter | All Recurrences | High-Risk Recurrences | ||
|---|---|---|---|---|
| XBM | Cystoscopy and Washing Cytology | XBM | Cystoscopy and Washing Cytology | |
| Sensitivity, n (%) | 79/82 (96.3) | 50/82 (61.0) | 37/38 (97.4) | 24/38 (63.2) |
| Specificity, n (%) | 35/255 (13.7) | 246/255 (96.5) | 37/299 (12.4) | 264/299 (88.3) |
| Positive predictive value, n (%) | 79/299 (26.4) | 50/59 (84.7) | 37/299 (12.4) | 24/59 (40.7) |
| Negative predictive value, n (%) | 35/38 (92.1) | 246/278 (88.5) | 37/38 (97.4) | 264/278 (95.0) |
| Accuracy, n (%) | 114/337 (33.8) | 296/337 (87.8) | 74/337 (22.0) | 288/337 (85.5) |
| Avoided diagnostic procedures, n (%) | 38/337 (11.3) | 278/337 (82.5) | 38/337 (11.3) | 278/337 (82.5) |
| Missed recurrences, n (%) | 3/82 (3.7) | 32/482 (39.0) | 1/38 (2.6) | 14/38 (36.8) |
| Method of Suspicion | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Odd Ratio (95% CI) | p Value | Odd Ratio (95% CI) | p Value | |
| For any type of recurrence | ||||
| XBM | 4.189 (1.253–14.004) | =0.090 | 2.178 (0.567–8.369) | =0.257 |
| Cystoscopy | 55.729 (22.200–139.897) | <0.001 | 49.818 (19.623–126.477) | <0.001 |
| Washing cytology | 11.667 (3.127–43.522) | <0.001 | 7.762 (1.597–37.711) | =0.110 |
| For high-risk recurrences | ||||
| XBM | 5.225 (0.96–39.227) | =0.052 | 2.644 (0.337–20.714) | =0.355 |
| Cystoscopy | 10.307 (4.932–21.540) | < 0.001 | 8.182 (3.766–17.773) | <0.001 |
| Washing cytology | 15.680 (4.824–59.968) | < 0.001 | 9.504 (2.515–35.919) | =0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lozano, F.; Raventós, C.X.; Carrion, A.; Dinarés, C.; Hernández, J.; Trilla, E.; Morote, J. Xpert Bladder Cancer Monitor for the Early Detection of Non-Muscle Invasive Bladder Cancer Recurrences: Could Cystoscopy Be Substituted? Cancers 2023, 15, 3683. https://doi.org/10.3390/cancers15143683
Lozano F, Raventós CX, Carrion A, Dinarés C, Hernández J, Trilla E, Morote J. Xpert Bladder Cancer Monitor for the Early Detection of Non-Muscle Invasive Bladder Cancer Recurrences: Could Cystoscopy Be Substituted? Cancers. 2023; 15(14):3683. https://doi.org/10.3390/cancers15143683
Chicago/Turabian StyleLozano, Fernando, Carles X. Raventós, Albert Carrion, Carme Dinarés, Javier Hernández, Enrique Trilla, and Juan Morote. 2023. "Xpert Bladder Cancer Monitor for the Early Detection of Non-Muscle Invasive Bladder Cancer Recurrences: Could Cystoscopy Be Substituted?" Cancers 15, no. 14: 3683. https://doi.org/10.3390/cancers15143683
APA StyleLozano, F., Raventós, C. X., Carrion, A., Dinarés, C., Hernández, J., Trilla, E., & Morote, J. (2023). Xpert Bladder Cancer Monitor for the Early Detection of Non-Muscle Invasive Bladder Cancer Recurrences: Could Cystoscopy Be Substituted? Cancers, 15(14), 3683. https://doi.org/10.3390/cancers15143683