
Optimization of Radiolabeling of a [90Y]Y-Anti-CD66-Antibody for Radioimmunotherapy before Allogeneic Hematopoietic Cell Transplantation

 ,
,  , ,
, , 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
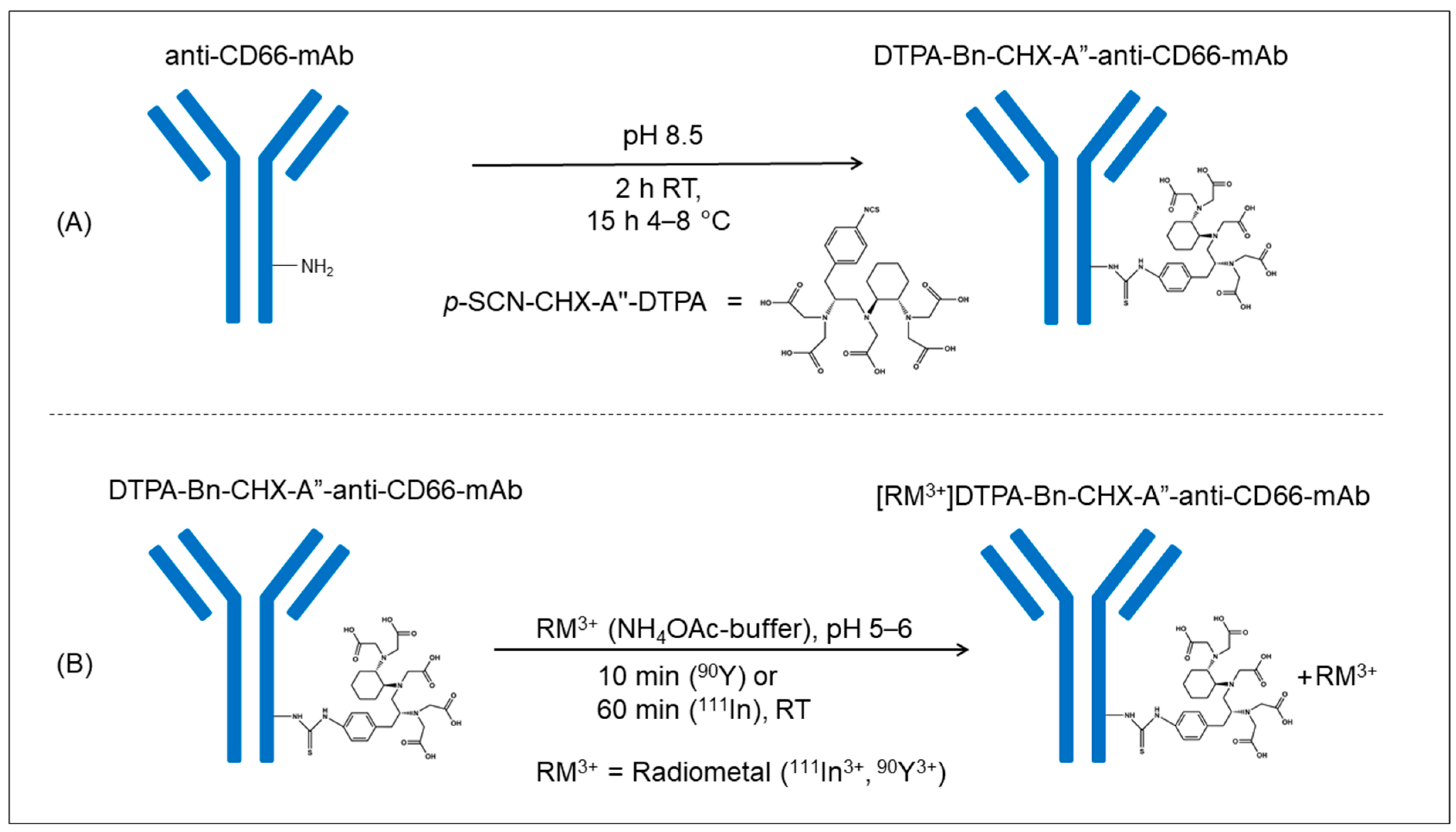
2.1. Conjugation of Anti-CD66-mAb with p-SCN-CHX-A″-DTPA
2.2. Labeling, Purification, and Serum Stability of [111In]In-DTPA-Bn-CHX-A″-Anti-CD66
2.3. Labeling, Purification, and Serum Stability of [90Y]Y-DTPA-Bn-CHX-A″-Anti-CD66
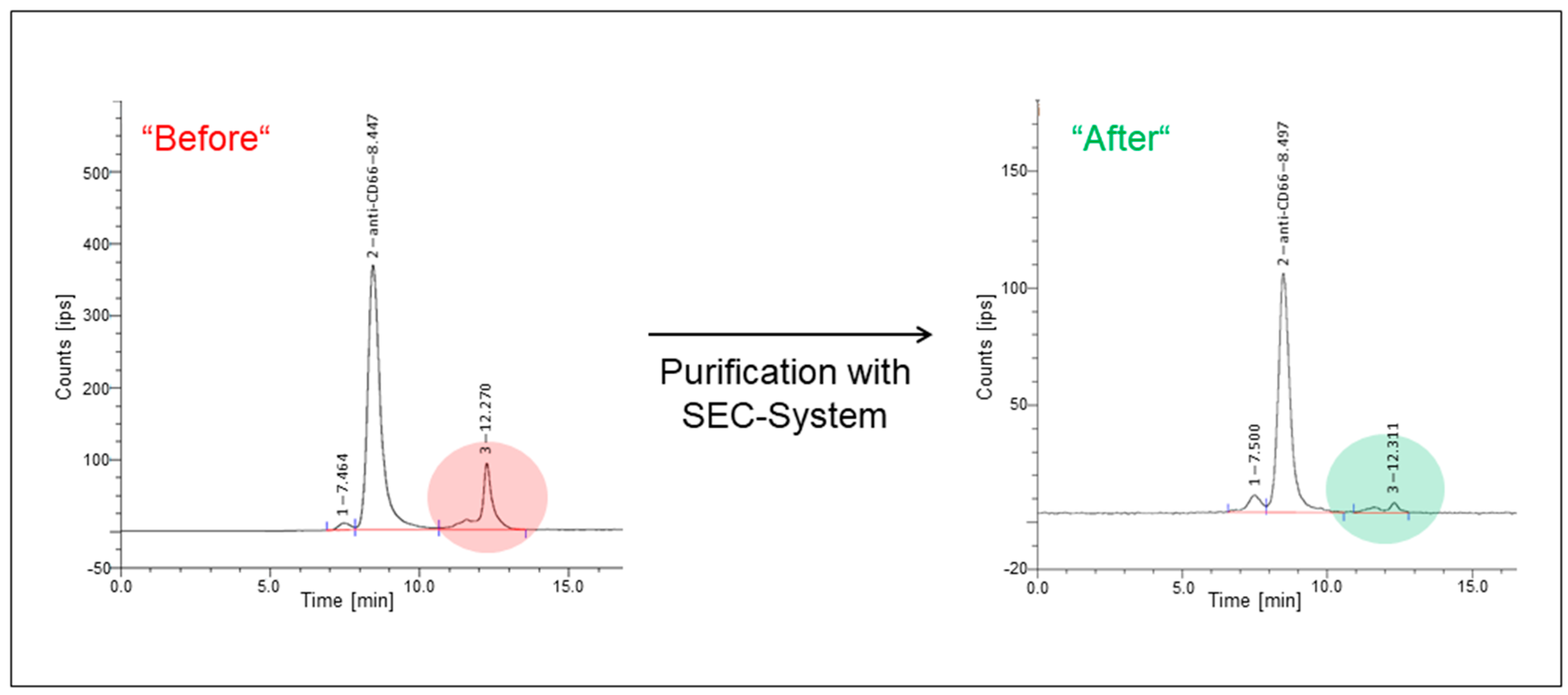
2.4. Determination of Radiochemical Purity of [90Y]Y-DTPA-Bn-CHX-A″-Anti-CD66-mAb
2.5. Determination of Radioimmunoreactivity (RIR)
2.6. Dosimetry
2.7. Radioimmunotherapy
3. Results
3.1. Conjugation of the Chelator
3.2. Radiolabeling, Purification, and Stability of [111In]In-DTPA-Bn-CHX-A″-Anti-CD66
3.3. Radiolabeling, Purification, and Stability of [90Y]Y-DTPA-Bn-CHX-A″-Anti-CD66
3.4. Dosimetry and RIT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carreras, E.; Dufour, C.; Mohty, M.; Kröger, N. (Eds.) The EBMT Handbook: Hematopoietic Stem Cell Transplantation and Cellular Therapies, 7th ed.; Springer: Cham, Switzerland, 2019. [Google Scholar]
- Bunjes, D.; Buchmann, I.; Duncker, C.; Seitz, U.; Kotzerke, J.; Wiesneth, M.; Dohr, D.; Stefanic, M.; Buck, A.; Harsdorf, S.V.; et al. Rhenium 188-labeled anti-CD66 (a, b, c, e) monoclonal antibody to intensify the conditioning regimen prior to stem cell transplantation for patients with high-risk acute myeloid leukemia or myelodysplastic syndrome: Results of a phase I–II study. Blood 2001, 98, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.S.; Glatting, G.; Hoenig, M.; Schuetz, C.; Gatz, S.A.; Grewendorf, S.; Sparber-Sauer, M.; Muche, R.; Blumstein, N.; Kropshofer, G.; et al. Radioimmunotherapy-based conditioning for hematopoietic cell transplantation in children with malignant and nonmalignant diseases. Blood 2011, 117, 4642–4650. [Google Scholar] [CrossRef] [PubMed]
- Audette, M.; Buchegger, F.; Schreyer, M.; Mach, J.P. Monoclonal antibody against carcinoembryonic antigen (CEA) identifies two new forms of crossreacting antigens of molecular weight 90,000 and 160,000 in normal granulocytes. Mol. Immunol. 1987, 24, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Kuijpers, T.W.; Hoogerwerf, M.; van der Laan, L.J.; Nagel, G.; van der Schoot, C.E.; Grunert, F.; Roos, D. CD66 nonspecific cross-reacting antigens are involved in neutrophil adherence to cytokine-activated endothelial cells. J. Cell Biol. 1992, 118, 457–466. [Google Scholar] [CrossRef]
- Kuroki, M.; Abe, H.; Imakiirei, T.; Liao, S.; Uchida, H.; Yamauchi, Y.; Oikawa, S.; Kuroki, M. Identification and comparison of residues critical for cell-adhesion activities of two neutrophil CD66 antigens, CEACAM6 and CEACAM8. J. Leukoc. Biol. 2001, 70, 543–550. [Google Scholar] [CrossRef]
- Bosslet, K.; Luben, G.; Schwarz, A.; Hundt, E.; Harthus, H.P.; Seiler, F.R.; Muhrer, C.; Kloppel, G.; Kayser, K.; Sedlacek, H.H. Immunohistochemical localization and molecular characteristics of three monoclonal antibody-defined epitopes detectable on carcinoembryonic antigen (CEA). Int. J. Cancer 1985, 36, 75–84. [Google Scholar] [CrossRef]
- Bunjes, D. 188Re-labeled anti-CD66 monoclonal antibody in stem cell transplantation for patients with high-risk acute myeloid leukemia. Leuk. Lymphoma 2002, 43, 2125–2131. [Google Scholar] [CrossRef]
- Buchmann, I.; Bunjes, D.; Kotzerke, J.; Martin, H.; Glatting, G.; Seitz, U.; Rattat, D.; Buck, A.; Döhner, H.; Reske, S.N. Myeloablative radioimmunotherapy with Re-188-anti-CD66-antibody for conditioning of high-risk leukemia patients prior to stem cell transplantation: Biodistribution, biokinetics and immediate toxicities. Cancer Biother. Radiopharm. 2002, 17, 151–163. [Google Scholar] [CrossRef]
- Zenz, T.; Glatting, G.; Schlenk, R.F.; Buchmann, I.; Dohner, H.; Reske, S.N.; Bunjes, D. Targeted marrow irradiation with radioactively labeled anti-CD66 monoclonal antibody prior to allogeneic stem cell transplantation for patients with leukemia: Results of a phase I–II study. Haematologica 2006, 91, 285–286. [Google Scholar]
- Fasslrinner, F.; Stolzel, F.; Kramer, M.; Teipel, R.; Brogsitter, C.; Morgner, A.; Arndt, C.; Bachmann, M.; Hanel, M.; Rollig, C.; et al. Radioimmunotherapy in Combination with Reduced-Intensity Conditioning for Allogeneic Hematopoietic Cell Transplantation in Patients with Advanced Multiple Myeloma. Biol. Blood Marrow Transplant. 2020, 26, 691–697. [Google Scholar] [CrossRef]
- Ringhoffer, M.; Blumstein, N.; Neumaier, B.; Glatting, G.; von Harsdorf, S.; Buchmann, I.; Wiesneth, M.; Kotzerke, J.; Zenz, T.; Buck, A.K.; et al. 188Re or 90Y-labelled anti-CD66 antibody as part of a dose-reduced conditioning regimen for patients with acute leukaemia or myelodysplastic syndrome over the age of 55: Results of a phase I–II study. Br. J. Haematol. 2005, 130, 604–613. [Google Scholar] [CrossRef]
- Chiesa, R.; Orchard, K.; Chan, P.-S.; Rao, K.; Amrolia, P.; Lucchini, G.; Silva, J.; Lazareva, A.; Mullanfiroze, K.; Mirci-Danicar, O.; et al. Radio-immunotherapy with 90Yttrium labelled anti-CD66 monoclonal antibody in children with relapsed/refractory acute leukemia: A UK phase 1 study. In Proceedings of the 48th Annual Meeting of the European Society for Blood and Marrow Transplantation, Virtual Meeting, 19–23 March 2022; Volume 57, pp. 16–99. [Google Scholar] [CrossRef]
- Orchard, K.H.; Langford, J.; Lloyd-Evans, P.; Phillips, D.; Guy, M.; Michopoulou, S.; Lewis, G.; Williams, J.; Zvavamwe, C.; Hutchison, C.; et al. Autologous Stem Cell Transplantation in AL-Amyloidosis Following Yttrium-90 Labelled Anti-CD66 Monoclonal Antibody As Sole Conditioning Is Associated with Low Toxicity and Demonstrable Disease Responses. Blood 2021, 138, 3819. [Google Scholar] [CrossRef]
- Baur, B.; Solbach, C.; Andreolli, E.; Winter, G.; Machulla, H.J.; Reske, S.N. Synthesis, Radiolabelling and In Vitro Characterization of the Gallium-68-, Yttrium-90- and Lutetium-177-Labelled PSMA Ligand, CHX-A”-DTPA-DUPA-Pep. Pharmaceuticals 2014, 7, 517–529. [Google Scholar] [CrossRef]
- Price, E.W.; Edwards, K.J.; Carnazza, K.E.; Carlin, S.D.; Zeglis, B.M.; Adam, M.J.; Orvig, C.; Lewis, J.S. A comparative evaluation of the chelators H4octapa and CHX-A”-DTPA with the therapeutic radiometal 90Y. Nucl. Med. Biol. 2016, 43, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Pippin, C.G.; Parker, T.A.; McMurry, T.J.; Brechbiel, M.W. Spectrophotometric method for the determination of a bifunctional DTPA ligand in DTPA-monoclonal antibody conjugates. Bioconjug. Chem. 1992, 3, 342–345. [Google Scholar] [CrossRef]
- Glatting, G.; Reske, S.N. Determination of the immunoreactivity of radiolabeled monoclonal antibodies: A theoretical analysis. Cancer Biother. Radiopharm. 2006, 21, 15–21. [Google Scholar] [CrossRef]
- Kletting, P.; Kull, T.; Bunjes, D.; Mahren, B.; Luster, M.; Reske, S.N.; Glatting, G. Radioimmunotherapy with anti-CD66 antibody: Improving the biodistribution using a physiologically based pharmacokinetic model. J. Nucl. Med. 2010, 51, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Kletting, P.; Maaß, C.; Reske, S.N.; Beer, A.; Glatting, G. Physiologically Based Pharmacokinetic Modeling is Essential in 90Y-labeled Anti-CD66 Radioimmunotherapy. PLoS ONE 2015, 10, e1027934. [Google Scholar] [CrossRef]
- Maaß, C.; Kletting, P.; Bunjes, D.; Mahren, B.; Beer, A.J.; Glatting, G. Population-Based Modeling Improves Treatment Planning Before 90Y-Labeled Anti-CD66 Antibody Radioimmunotherapy. Cancer Biother. Radiopharm. 2015, 30, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Seitz, U.; Neumaier, B.; Glatting, G.; Kotzerke, J.; Bunjes, D.; Reske, S.N. Preparation and evaluation of the rhenium-188-labelled anti-NCA antigen monoclonal antibody BW 250/183 for radioimmunotherapy of leukaemia. Eur. J. Nucl. Med. 1999, 26, 1265–1273. [Google Scholar] [CrossRef]
- Palmer, J.L.; Nisonoff, A. Reduction and Reoxidation of a Critical Disulfide Bond in the Rabbit Antibody Molecule. J. Biol. Chem. 1963, 238, 2393–2398. [Google Scholar] [CrossRef]
- Mun, M.; Khoo, S.; Do Minh, A.; Dvornicky, J.; Trexler-Schmidt, M.; Kao, Y.H.; Laird, M.W. Air sparging for prevention of antibody disulfide bond reduction in harvested CHO cell culture fluid. Biotechnol. Bioeng. 2015, 112, 734–742. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Liu, Y.D.; Cai, B.; Huang, G.; Flynn, G.C. Investigation of antibody disulfide reduction and re-oxidation and impact to biological activities. J. Pharm. Biomed. Anal. 2015, 102, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Gurjar, S.A.; Wheeler, J.X.; Wadhwa, M.; Thorpe, R.; Kimber, I.; Derrick, J.P.; Dearman, R.J.; Metcalfe, C. The impact of thioredoxin reduction of allosteric disulfide bonds on the therapeutic potential of monoclonal antibodies. J. Biol. Chem. 2019, 294, 19616–19634. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.; Tan, Z.; Ehamparanathan, V.; Ren, T.; Hoffman, L.; Du, C.; Song, Y.; Tao, L.; Lewandowski, A.; Ghose, S.; et al. Optimization and kinetic modeling of interchain disulfide bond reoxidation of monoclonal antibodies in bioprocesses. mAbs 2020, 12, 1829336. [Google Scholar] [CrossRef]
- Ren, T.; Tan, Z.; Ehamparanathan, V.; Lewandowski, A.; Ghose, S.; Li, Z.J. Antibody disulfide bond reduction and recovery during biopharmaceutical process development—A review. Biotechnol. Bioeng. 2021, 118, 2829–2844. [Google Scholar] [CrossRef]
- Camera, L.; Kinuya, S.; Garmestani, K.; Wu, C.; Brechbiel, M.W.; Pai, L.H.; McMurry, T.J.; Gansow, O.A.; Pastan, I.; Paik, C.H.; et al. Evaluation of the serum stability and in vivo biodistribution of CHX-DTPA and other ligands for yttrium labeling of monoclonal antibodies. J. Nucl. Med. 1994, 35, 882–889. [Google Scholar]
- Wu, C.; Virzi, F.; Hnatowich, D.J. Investigations of N-linked macrocycles for 111In- and 90Y-labeling of proteins. Int. J. Rad. Appl. Instrum. B 1992, 19, 239–244. [Google Scholar] [CrossRef]
- Chakravarty, R.; Chakraborty, S.; Dash, A. A systematic comparative evaluation of 90Y-labeled bifunctional chelators for their use in targeted therapy. J. Label. Compd. Radiopharm. 2014, 57, 65–74. [Google Scholar] [CrossRef]
- Carrasquillo, J.A.; White, J.D.; Paik, C.H.; Raubitschek, A.; Le, N.; Rotman, M.; Brechbiel, M.W.; Gansow, O.A.; Top, L.E.; Perentesis, P.; et al. Similarities and differences in 111In- and 90Y-labeled 1B4M-DTPA antiTac monoclonal antibody distribution. J. Nucl. Med. 1999, 40, 268–276. [Google Scholar]
- Chinn, P.C.; Leonard, J.E.; Rosenberg, J.; Hanna, N.; Anderson, D.R. Preclinical evaluation of 90Y-labeled anti-CD20 monoclonal antibody for treatment of non-Hodgkin’s lymphoma. Int. J. Oncol. 1999, 15, 1017–1025. [Google Scholar] [CrossRef]
- DeNardo, G.L.; Kroger, L.A.; DeNardo, S.J.; Miers, L.A.; Salako, Q.; Kukis, D.L.; Fand, I.; Shen, S.; Renn, O.; Meares, C.F. Comparative toxicity studies of yttrium-90 MX-DTPA and 2-IT-BAD conjugated monoclonal antibody (BrE-3). Cancer 1994, 73, 1012–1022. [Google Scholar] [CrossRef] [PubMed]
- Witzig, T.E. The use of ibritumomab tiuxetan radioimmunotherapy for patients with relapsed B-cell non-Hodgkin’s lymphoma. Semin. Oncol. 2000, 27, 74–78. [Google Scholar]
- Witzig, T.E. Radioimmunotherapy for patients with relapsed B-cell non-Hodgkin lymphoma. Cancer Chemother. Pharmacol. 2001, 48 (Suppl. 1), S91–S95. [Google Scholar] [CrossRef] [PubMed]
- Morschhauser, F.; Illidge, T.; Huglo, D.; Martinelli, G.; Paganelli, G.; Zinzani, P.L.; Rule, S.; Liberati, A.M.; Milpied, N.; Hess, G.; et al. Efficacy and safety of yttrium-90 ibritumomab tiuxetan in patients with relapsed or refractory diffuse large B-cell lymphoma not appropriate for autologous stem-cell transplantation. Blood 2007, 110, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Adams, G.P.; Shaller, C.C.; Dadachova, E.; Simmons, H.H.; Horak, E.M.; Tesfaye, A.; Klein-Szanto, A.J.; Marks, J.D.; Brechbiel, M.W.; Weiner, L.M. A single treatment of yttrium-90-labeled CHX-A”-C6.5 diabody inhibits the growth of established human tumor xenografts in immunodeficient mice. Cancer Res. 2004, 64, 6200–6206. [Google Scholar] [CrossRef]
- Blend, M.J.; Stastny, J.J.; Swanson, S.M.; Brechbiel, M.W. Labeling anti-HER2/neu monoclonal antibodies with 111In and 90Y using a bifunctional DTPA chelating agent. Cancer Biother. Radiopharm. 2003, 18, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, R.; Chakraborty, S.; Sarma, H.D.; Nair, K.V.; Rajeswari, A.; Dash, A. 90Y/177Lu-labelled Cetuximab immunoconjugates: Radiochemistry optimization to clinical dose formulation. J. Label. Compd. Radiopharm. 2016, 59, 354–363. [Google Scholar] [CrossRef]
- Kennel, S.J.; Stabin, M.; Yoriyaz, H.; Brechbiel, M.; Mirzadeh, S. Treatment of lung tumor colonies with 90Y-targeted to blood vessels: Comparison with the alpha-particle emitter 213Bi. Nucl. Med. Biol. 1999, 26, 149–157. [Google Scholar] [CrossRef]
- Lee, F.T.; Mountain, A.J.; Kelly, M.P.; Hall, C.; Rigopoulos, A.; Johns, T.G.; Smyth, F.E.; Brechbiel, M.W.; Nice, E.C.; Burgess, A.W.; et al. Enhanced efficacy of radioimmunotherapy with 90Y-CHX-A’‘-DTPA-hu3S193 by inhibition of epidermal growth factor receptor (EGFR) signaling with EGFR tyrosine kinase inhibitor AG1478. Clin. Cancer Res. 2005, 11, 7080s–7086s. [Google Scholar] [CrossRef]
- Ma, D.; McDevitt, M.R.; Barendswaard, E.; Lai, L.; Curcio, M.J.; Pellegrini, V.; Brechbiel, M.W.; Scheinberg, D.A. Radioimmunotherapy for model B cell malignancies using Y-90-labeled anti-CD19 and anti-CD20 monoclonal antibodies. Leukemia 2002, 16, 60–66. [Google Scholar] [CrossRef][Green Version]
- Saker, J.; Kriegs, M.; Zenker, M.; Heldt, J.M.; Eke, I.; Pietzsch, H.J.; Grenman, R.; Cordes, N.; Petersen, C.; Baumann, M.; et al. Inactivation of HNSCC cells by 90Y-labeled cetuximab strictly depends on the number of induced DNA double-strand breaks. J. Nucl. Med. 2013, 54, 416–423. [Google Scholar] [CrossRef]
- Thompson, S.; Ballard, B.; Jiang, Z.; Revskaya, E.; Sisay, N.; Miller, W.H.; Cutler, C.S.; Dadachova, E.; Francesconi, L.C. 166Ho and 90Y labeled 6D2 monoclonal antibody for targeted radiotherapy of melanoma: Comparison with 188Re radiolabel. Nucl. Med. Biol. 2014, 41, 276–281. [Google Scholar] [CrossRef]
- Kobayashi, H.; Wu, C.; Yoo, T.M.; Sun, B.F.; Drumm, D.; Pastan, I.; Paik, C.H.; Gansow, O.A.; Carrasquillo, J.A.; Brechbiel, M.W. Evaluation of the in vivo biodistribution of yttrium-labeled isomers of CHX-DTPA-conjugated monoclonal antibodies. J. Nucl. Med. 1998, 39, 829–836. [Google Scholar] [PubMed]
- Scott, P.J.; Hockley, B.G.; Kung, H.F.; Manchanda, R.; Zhang, W.; Kilbourn, M.R. Studies into radiolytic decomposition of fluorine-18 labeled radiopharmaceuticals for positron emission tomography. Appl. Radiat. Isot. 2009, 67, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Skamris, T.; Tian, X.; Thorolfsson, M.; Karkov, H.S.; Rasmussen, H.B.; Langkilde, A.E.; Vestergaard, B. Monoclonal Antibodies Follow Distinct Aggregation Pathways During Production-Relevant Acidic Incubation and Neutralization. Pharm. Res. 2016, 33, 716–728. [Google Scholar] [CrossRef] [PubMed]
- Rouby, G.; Tran, N.T.; Leblanc, Y.; Taverna, M.; Bihoreau, N. Investigation of monoclonal antibody dimers in a final formulated drug by separation techniques coupled to native mass spectrometry. mAbs 2020, 12, e1781743. [Google Scholar] [CrossRef]
- Plath, F.; Ringler, P.; Graff-Meyer, A.; Stahlberg, H.; Lauer, M.E.; Rufer, A.C.; Graewert, M.A.; Svergun, D.; Gellermann, G.; Finkler, C.; et al. Characterization of mAb dimers reveals predominant dimer forms common in therapeutic mAbs. mAbs 2016, 8, 928–940. [Google Scholar] [CrossRef]
- Elmore, S.A. Enhanced histopathology of the spleen. Toxicol. Pathol. 2006, 34, 648–655. [Google Scholar] [CrossRef]
- Cesta, M.F. Normal structure, function, and histology of the spleen. Toxicol. Pathol. 2006, 34, 455–465. [Google Scholar] [CrossRef]
- Polák, Š.; Gálfiová, P.; Varga, I. Ultrastructure of human spleen in transmission and scanning electron microscope. Biologia 2009, 64, 402–408. [Google Scholar] [CrossRef]
- Gätjen, M.; Brand, F.; Grau, M.; Gerlach, K.; Kettritz, R.; Westermann, J.; Anagnostopoulos, I.; Lenz, P.; Lenz, G.; Höpken, U.E.; et al. Splenic Marginal Zone Granulocytes Acquire an Accentuated Neutrophil B-Cell Helper Phenotype in Chronic Lymphocytic Leukemia. Cancer Res. 2016, 76, 5253–5265. [Google Scholar] [CrossRef] [PubMed]
- Bronte, V.; Pittet, M.J. The spleen in local and systemic regulation of immunity. Immunity 2013, 39, 806–818. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L. A study of the structure of splenic sinuses in man and in the albino rat with the light microscope and the electron microscope. J. Biophys. Biochem. Cytol. 1957, 3, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.M.; DeAngelo, D.J.; Stelljes, M.; Martinelli, G.; Liedtke, M.; Stock, W.; Gokbuget, N.; O’Brien, S.; Wang, K.; Wang, T.; et al. Inotuzumab Ozogamicin versus Standard Therapy for Acute Lymphoblastic Leukemia. N. Engl. J. Med. 2016, 375, 740–753. [Google Scholar] [CrossRef] [PubMed]
- Varma, A.; Abraham, S.C.; Mehta, R.S.; Saini, N.Y.; Honhar, M.; Rashid, M.; Chen, J.; Srour, S.A.; Bashir, Q.; Rondon, G.; et al. Idiopathic refractory ascites after allogeneic stem cell transplantation: A previously unrecognized entity. Blood Adv. 2020, 4, 1296–1306. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | |
|---|---|
| Number | 5 |
| Age at the time of HCT | |
| Median | 63 |
| Range | 48–65 |
| Sex (m:f) | 4:1 |
| Diagnosis (n, %) | |
| AML | 2 (40%) |
| MDS | 2 (40%) |
| ALL | 1 (20%) |
| Disease stage at HCT (n, %) | |
| Upfront/early | 2 (40%) |
| CR | 3 (60%) |
| Donor type (n, %) | |
| MUD | 5/5 (100%) |
| Conditioning regimen (n, %) | |
| Fludarabin, treosulfan + ATG | 2 (40%) |
| Fludarabin, melphalan, carmustin + ATG | 2 (40%) |
| Fludarabin, thiotepa, carmustin + ATG | 1 (20%) |
| GvHD prophylaxis (n, %) | |
| Tacrolimus + MMF | 5/5 (100%) |
| Number of HCT (n, %) | |
| 1st HCT | 3/5 (60%) |
| 2nd HCT | 2/5 (40%) |
| Organ Dose [Gy] | P1 a | P2 | P3 | P4 | P5 |
|---|---|---|---|---|---|
| Bone marrow | 9.4 | 21.7 | 24.5 | 26.3 | 24.3 |
| Liver | 3.5 | 7.0 | 6.3 | 5.3 | 6.0 |
| Spleen | 10.8 | 16.1 | 33.4 | 23.1 | 42.2 |
| Kidneys | 0.9 | 2.4 | 2.2 | 2.1 | 1.8 |
| Whole body | 0.5 | 1.1 | 1.0 | 1.4 | 1.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winter, G.; Hamp-Goldstein, C.; Fischer, G.; Kletting, P.; Glatting, G.; Solbach, C.; Herrmann, H.; Sala, E.; Feuring, M.; Döhner, H.; et al. Optimization of Radiolabeling of a [90Y]Y-Anti-CD66-Antibody for Radioimmunotherapy before Allogeneic Hematopoietic Cell Transplantation. Cancers 2023, 15, 3660. https://doi.org/10.3390/cancers15143660
Winter G, Hamp-Goldstein C, Fischer G, Kletting P, Glatting G, Solbach C, Herrmann H, Sala E, Feuring M, Döhner H, et al. Optimization of Radiolabeling of a [90Y]Y-Anti-CD66-Antibody for Radioimmunotherapy before Allogeneic Hematopoietic Cell Transplantation. Cancers. 2023; 15(14):3660. https://doi.org/10.3390/cancers15143660
Chicago/Turabian StyleWinter, Gordon, Carmen Hamp-Goldstein, Gabriel Fischer, Peter Kletting, Gerhard Glatting, Christoph Solbach, Hendrik Herrmann, Elisa Sala, Michaela Feuring, Hartmut Döhner, and et al. 2023. "Optimization of Radiolabeling of a [90Y]Y-Anti-CD66-Antibody for Radioimmunotherapy before Allogeneic Hematopoietic Cell Transplantation" Cancers 15, no. 14: 3660. https://doi.org/10.3390/cancers15143660
APA StyleWinter, G., Hamp-Goldstein, C., Fischer, G., Kletting, P., Glatting, G., Solbach, C., Herrmann, H., Sala, E., Feuring, M., Döhner, H., Beer, A. J., Bunjes, D., & Prasad, V. (2023). Optimization of Radiolabeling of a [90Y]Y-Anti-CD66-Antibody for Radioimmunotherapy before Allogeneic Hematopoietic Cell Transplantation. Cancers, 15(14), 3660. https://doi.org/10.3390/cancers15143660