


The Impact of Mindfulness on Functional Brain Connectivity and Peripheral Inflammation in Breast Cancer Survivors with Cognitive Complaints

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design and Study Procedure
2.3. Interventions
2.3.1. Mindfulness-Based Intervention
2.3.2. Physical Training
2.4. Measures
2.4.1. MRI Acquisition
2.4.2. Serum Collection and Cytokine Analysis
2.5. Image Processing and Analysis
2.6. Graph Analysis
2.7. Serum Cytokine Analysis
2.8. Correlation Analysis
3. Results
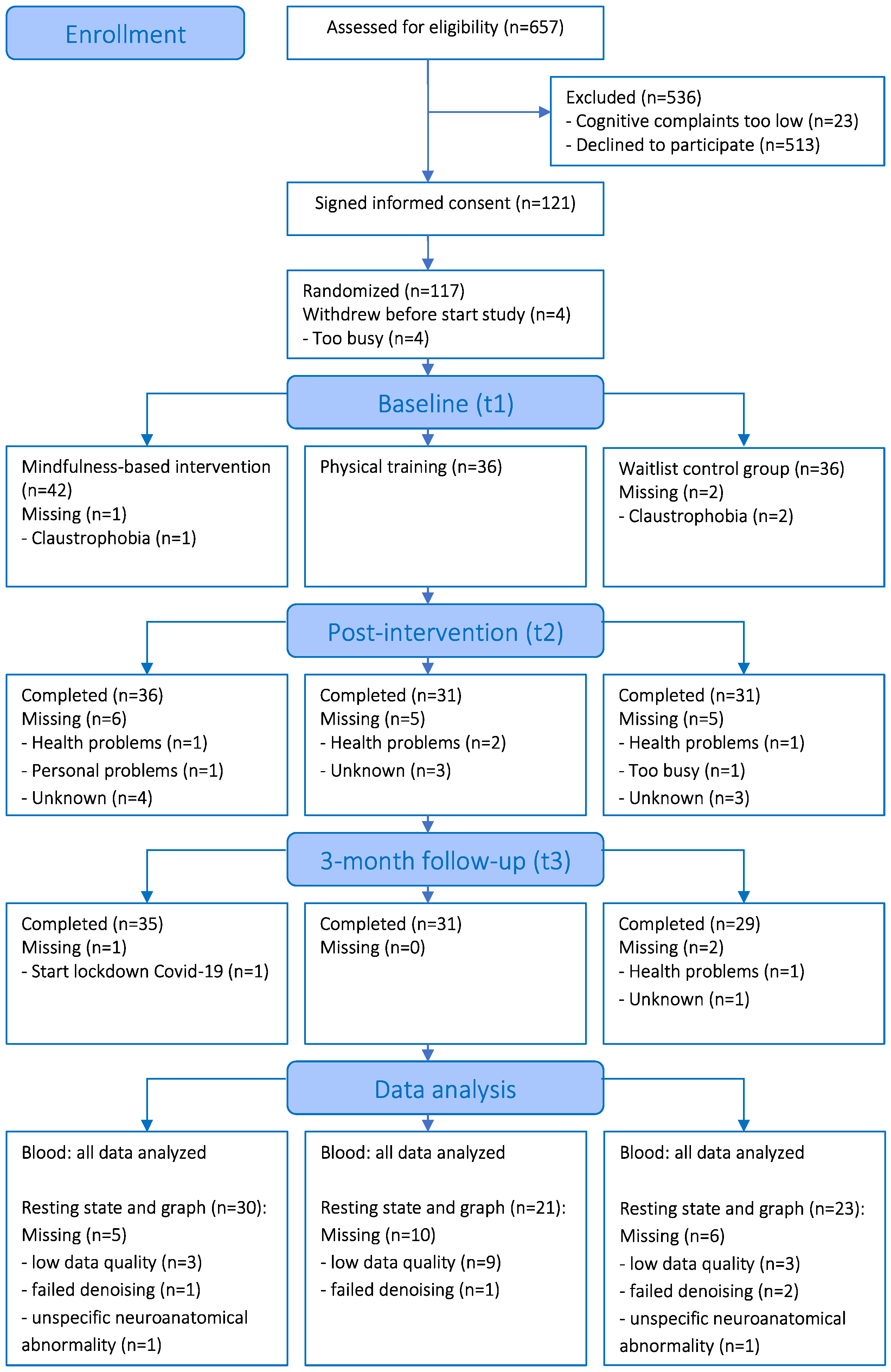
3.1. Enrolment and Attrition
3.2. Participant Characteristics
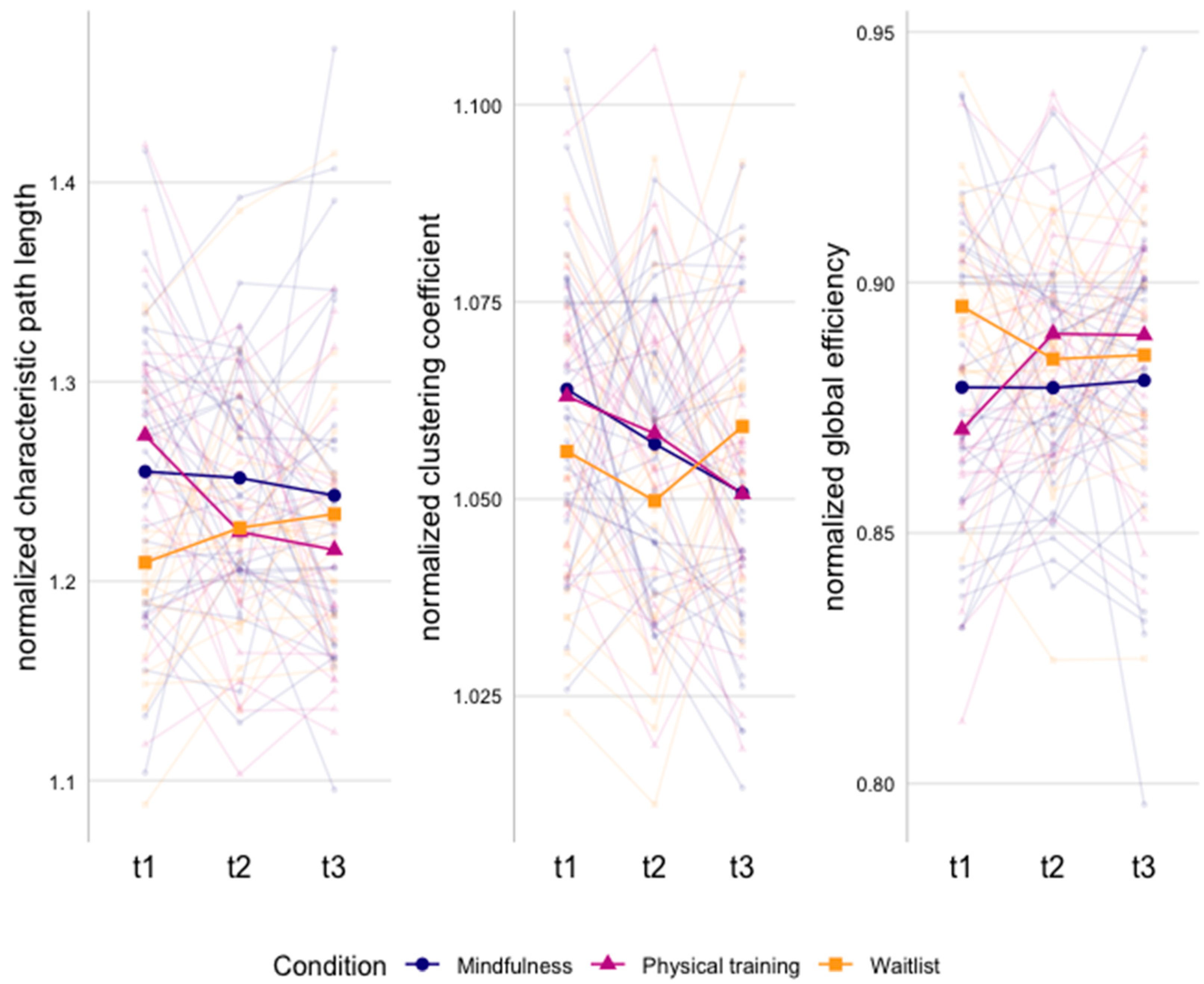
3.3. Resting State Functional Connectivity and Graph Analysis
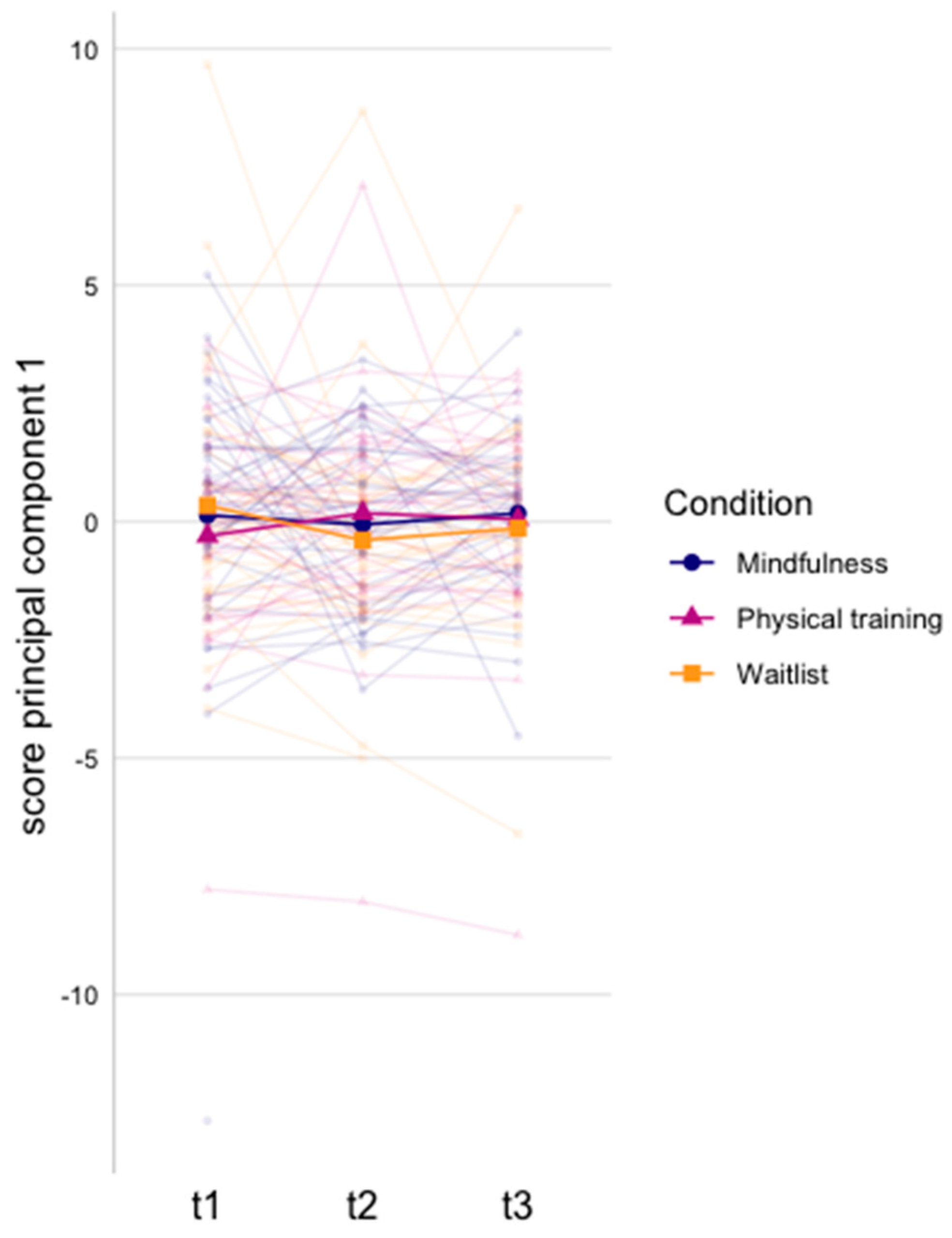
3.4. Serum Cytokine Analysis
3.5. Correlation Analysis
4. Discussion
Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Mokhatri-Hesari, P.; Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual. Life Outcomes 2020, 18, 338. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; De Ruiter, M.B.; Castel, H. Cancer-related cognitive impairment: An update on state of the art, detection, and management strategies in cancer survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, A.L.; George, R.P.; O’Malley, L. Prevalence of cognitive impairment following chemotherapy treatment for breast cancer: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 2135. [Google Scholar] [CrossRef]
- Ahles, T.A.; Root, J.C. Cognitive effects of cancer and cancer treatments. Annu. Rev. Clin. Psychol. 2018, 14, 425–451. [Google Scholar] [CrossRef] [PubMed]
- Lv, H.; Wang, Z.; Tong, E.; Williams, L.M.; Zaharchuk, G.; Zeineh, M.; Goldstein-Piekarski, A.N.; Ball, T.M.; Liao, C.; Wintermark, M. Resting-state functional MRI: Everything that nonexperts have always wanted to know. Am. J. Neuroradiol. 2018, 39, 1390–1399. [Google Scholar] [CrossRef] [PubMed]
- Dumas, J.A.; Makarewicz, J.; Schaubhut, G.J.; Devins, R.; Albert, K.; Dittus, K.; Newhouse, P.A. Chemotherapy altered brain functional connectivity in women with breast cancer: A pilot study. Brain Imaging Behav. 2013, 7, 524–532. [Google Scholar] [CrossRef]
- Miao, H.; Chen, X.; Yan, Y.; He, X.; Hu, S.; Kong, J.; Wu, M.; Wei, Y.; Zhou, Y.; Wang, L.; et al. Functional connectivity change of brain default mode network in breast cancer patients after chemotherapy. Neuroradiology 2016, 58, 921–928. [Google Scholar] [CrossRef]
- Kesler, S.R. Default mode network as a potential biomarker of chemotherapy-related brain injury. Neurobiol. Aging 2014, 35, S11–S19. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, Y.F.; Zheng, L.J.; Shi, Z.; Huang, W.; Zhang, L.J. Network-level functional connectivity alterations in chemotherapy treated breast cancer patients: A longitudinal resting state functional MRI study. Cancer Imaging 2020, 20, 73. [Google Scholar] [CrossRef]
- Shen, C.-Y.; Chen, V.C.-H.; Yeh, D.-C.; Huang, S.-L.; Zhang, X.-R.; Chai, J.-W.; Huang, Y.-H.; Chou, M.-C.; Weng, J.-C. Association of functional dorsal attention network alterations with breast cancer and chemotherapy. Sci. Rep. 2019, 9, 104. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yan, Y.; Wang, X.; Tao, L.; Chen, Q.; Bian, Y.; He, X.; Liu, Y.; Ding, W.; Yu, Y.; et al. Executive function alternations of breast cancer patients after chemotherapy: Evidence from resting-state functional MRI. Acad. Radiol. 2016, 23, 1264–1270. [Google Scholar] [CrossRef]
- Miao, H.; Li, J.; Hu, S.; He, X.; Partridge, S.C.; Ren, J.; Bian, Y.; Yu, Y.; Qiu, B. Long-term cognitive impairment of breast cancer patients after chemotherapy: A functional MRI study. Eur. J. Radiol. 2016, 85, 1053–1057. [Google Scholar] [CrossRef] [PubMed]
- Apple, A.C.; Schroeder, M.P.; Ryals, A.J.; Wagner, L.I.; Cella, D.; Shih, P.A.; Reilly, J.; Penedo, F.J.; Voss, J.L.; Wang, L. Hippocampal functional connectivity is related to self-reported cognitive concerns in breast cancer patients undergoing adjuvant therapy. Neuroimage Clin. 2018, 20, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Tuluhong, D.; Shi, Z.; Zheng, L.J.; Chen, T.; Lu, G.M.; Wang, S.; Zhang, L.J. Postchemotherapy hippocampal functional connectivity patterns in patients with breast cancer: A longitudinal resting state functional MR imaging study. Brain Imaging Behav. 2020, 14, 1456–1467. [Google Scholar] [CrossRef] [PubMed]
- Alves, P.N.; Foulon, C.; Karolis, V.; Bzdok, D.; Margulies, D.S.; Volle, E.; Thiebaut de Schotten, M. An improved neuroanatomical model of the default-mode network reconciles previous neuroimaging and neuropathological findings. Commun. Biol. 2019, 2, 370. [Google Scholar] [CrossRef]
- Bullmore, E.; Sporns, O. Complex brain networks: Graph theoretical analysis of structural and functional systems. Nat. Rev. Neurosci. 2009, 10, 186–198. [Google Scholar] [CrossRef]
- Soares, J.M.; Magalhães, R.; Moreira, P.S.; Sousa, A.; Ganz, E.; Sampaio, A.; Alves, V.; Marques, P.; Sousa, N. A hitchhiker’s guide to functional magnetic resonance imaging. Front. Neurosci. 2016, 10, 515. [Google Scholar] [CrossRef]
- van den Heuvel, M.P.; Hulshoff, P.H.E. Exploring the brain network: A review on resting-state fMRI functional connectivity. Eur. Neuropsychopharmacol. 2010, 20, 519–534. [Google Scholar] [CrossRef]
- Bekele, B.M.; Luijendijk, M.; Schagen, S.B.; de Ruiter, M.; Douw, L. Fatigue and resting-state functional brain networks in breast cancer patients treated with chemotherapy. Breast Cancer Res. Treat. 2021, 189, 787–796. [Google Scholar] [CrossRef]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. Neuroimage 2010, 52, 1059–1069. [Google Scholar] [CrossRef]
- Xuan, H.; Gan, C.; Li, W.; Huang, Z.; Wang, L.; Jia, Q.; Chen, Z.; Cheng, H.; Xuan, H.; Gan, C.; et al. Altered network efficiency of functional brain networks in patients with breast cancer after chemotherapy. Oncotarget 2017, 8, 105648–105661. [Google Scholar] [CrossRef]
- Phillips, N.S.; Rao, V.; Kmetz, L.; Vela, R.; Medick, S.; Krull, K.; Kesler, S.R. Changes in brain functional and effective connectivity after treatment for breast cancer and implications for intervention targets. Brain Connect. 2022, 12, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Bruno, J.; Hosseini, S.M.H.; Kesler, S. Altered resting state functional brain network topology in chemotherapy-treated breast cancer survivors. Neurobiol. Dis. 2012, 48, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Schroyen, G.; Vissers, J.; Smeets, A.; Gillebert, C.R.; Lemiere, J.; Sunaert, S.; Deprez, S.; Sleurs, C. Blood and neuroimaging biomarkers of cognitive sequelae in breast cancer patients throughout chemotherapy: A systematic review. Transl. Oncol. 2022, 16, 101297. [Google Scholar] [CrossRef] [PubMed]
- Ren, X.; St. Clair, D.K.; Butterfield, D.A. Dysregulation of cytokine mediated chemotherapy induced cognitive impairment. Pharmacol. Res. 2017, 117, 267–273. [Google Scholar] [CrossRef]
- Castel, H.; Denouel, A.; Lange, M.; Tonon, M.C.; Dubois, M.; Joly, F. Biomarkers associated with cognitive impairment in treated cancer patients: Potential predisposition and risk factors. Front. Pharmacol. 2017, 8, 138. [Google Scholar] [CrossRef] [PubMed]
- Biegler, K.A.; Alejandro Chaoul, M.; Cohen, L. Cancer, cognitive impairment, and meditation. Acta Oncol. 2009, 48, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Floyd, R.; Dyer, A.H.; Kennelly, S.P. Non-pharmacological interventions for cognitive impairment in women with breast cancer post-chemotherapy: A systematic review. J. Geriatr. Oncol. 2021, 12, 173–181. [Google Scholar] [CrossRef]
- Oldacres, L.; Hegarty, J.; O’Regan, P.; Murphy-Coakley, N.M.; Saab, M.M. Interventions promoting cognitive function in patients experiencing cancer related cognitive impairment: A systematic review. Psychooncology. 2022, 32, 214–228. [Google Scholar] [CrossRef]
- Crane, R.S.; Brewer, J.; Feldman, C.; Kabat-Zinn, J.; Santorelli, S.; Williams, J.M.G.; Kuyken, W. What defines mindfulness-based programs? The warp and the weft. Psychol. Med. 2017, 47, 990–999. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lopes, S.; Lavelle, T.; Jones, K.O.; Chen, L.; Jindal, M.; Zinzow, H.; Shi, L. Economic evaluations of mindfulness-based interventions: A systematic review. Mindfulness 2022, 13, 2359–2378. [Google Scholar] [CrossRef] [PubMed]
- Melis, M.; Schroyen, G.; Pollefeyt, J.; Raes, F.; Smeets, A.; Sunaert, S.; Deprez, S.; Van der Gucht, K. The impact of mindfulness-based interventions on brain functional connectivity: A systematic review. Mindfulness 2022, 13, 1857–1875. [Google Scholar] [CrossRef]
- Smith, A.M.; Leeming, A.; Fang, Z.; Hatchard, T.; Mioduszewski, O.; Schneider, M.A.; Ferdossifard, A.; Shergill, Y.; Khoo, E.L.; Poulin, P. Mindfulness-based stress reduction alters brain activity for breast cancer survivors with chronic neuropathic pain: Preliminary evidence from resting-state fMRI. J. Cancer Surviv. 2021, 15, 518–525. [Google Scholar] [CrossRef]
- Van der Gucht, K.; Ahmadoun, S.; Melis, M.; Cloe, E.; Sleurs, C.; Radwan, A.; Blommaert, J.; Takano, K.; Vandenbulcke, M.; Wildiers, H.; et al. Effects of a mindfulness-based intervention on cancer-related cognitive impairment: Results of a randomized controlled functional magnetic resonance imaging pilot study. Cancer 2020, 126, 4246–4255. [Google Scholar] [CrossRef]
- Qin, K.; Lei, D.; Yang, J.; Li, W.; Tallman, M.J.; Duran, L.R.P.; Blom, T.J.; Bruns, K.M.; Cotton, S.; Sweeney, J.A.; et al. Network-level functional topological changes after mindfulness-based cognitive therapy in mood dysregulated adolescents at familial risk for bipolar disorder: A pilot study. BMC Psychiatry 2021, 21, 213. [Google Scholar] [CrossRef]
- Zimmerman, B.; Finnegan, M.; Paul, S.; Schmidt, S.; Tai, Y.; Roth, K.; Chen, Y.; Husain, F.T. Functional brain changes during mindfulness-based cognitive therapyassociated with tinnitus severity. Front. Neurosci. 2019, 13, 747. [Google Scholar] [CrossRef]
- Cotier, F.A.; Zhang, R.; Lee, T.M.C. A longitudinal study of the effect of short-term meditation training on functional network organization of the aging brain. Sci. Rep. 2017, 7, 598. [Google Scholar] [CrossRef]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef]
- Bower, J.E.; Irwin, M.R. Mind–body therapies and control of inflammatory biology: A descriptive review. Brain. Behav. Immun. 2016, 51, 1–11. [Google Scholar] [CrossRef]
- Sanada, K.; Alda Díez, M.; Salas Valero, M.; Pérez-Yus, M.C.; Demarzo, M.M.P.; Montero-Marín, J.; García-Toro, M.; García-Campayo, J. Effects of mindfulness-based interventions on biomarkers in healthy and cancer populations: A systematic review. BMC Complement. Altern. Med. 2017, 17, 125. [Google Scholar] [CrossRef] [PubMed]
- Cillessen, L.; Johannsen, M.; Speckens, A.E.M.; Zachariae, R. Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and survivors: A systematic review and meta-analysis of randomized controlled trials. Psychooncology 2019, 28, 2257–2269. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.-Y.; Lin, L.-H.; Tzeng, G.-L.; Huang, Y.-H.; Tai, J.-F.; Chen, Y.-L.; Wu, C.-J.; Chen, P.-H.; Lin, P.-C.; Hung, P.-L. Effects of mindfulness-based therapy for cancer patients: A systematic review and meta-analysis. J. Clin. Psychol. Med. Settings 2022, 29, 432–445. [Google Scholar] [CrossRef]
- Zhang, D.; Lee, E.K.P.; Mak, E.C.W.; Ho, C.Y.; Wong, S.Y.S. Mindfulness-based interventions: An overall review. Br. Med. Bull. 2021, 138, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Melis, M.; Schroyen, G.; Leenaerts, N.; Smeets, A.; Sunaert, S.; Van der Gucht, K.; Deprez, S. The impact of mindfulness on cancer-related cognitive impairment in breast cancer survivors with cognitive complaints. Cancer 2023, 129, 1105–1116. [Google Scholar] [CrossRef]
- Bower, J.E. Mindfulness interventions for cancer survivors: Moving beyond wait-list control groups. J. Clin. Oncol. 2016, 34, 3366–3368. [Google Scholar] [CrossRef]
- Zimmer, P.; Baumann, F.T.; Oberste, M.; Wright, P.; Garthe, A.; Schenk, A.; Elter, T.; Galvao, D.A.; Bloch, W.; Hübner, S.T.; et al. Effects of exercise interventions and physical activity behavior on cancer related cognitive impairments: A systematic review. Biomed Res. Int. 2016, 2016, 1820954. [Google Scholar] [CrossRef]
- Campbell, K.L.; Zadravec, K.; Bland, K.A.; Chesley, E.; Wolf, F.; Janelsins, M.C. The effect of exercise on cancer-related cognitive impairment and applications for physical therapy: Systematic review of randomized controlled trials. Phys. Ther. 2020, 100, 523–542. [Google Scholar] [CrossRef]
- Koevoets, E.W.; Schagen, S.B.; de Ruiter, M.B.; Geerlings, M.I.; Witlox, L.; van der Wall, E.; Stuiver, M.M.; Sonke, G.S.; Velthuis, M.J.; Jobsen, J.J.; et al. Effect of physical exercise on cognitive function after chemotherapy in patients with breast cancer: A randomized controlled trial (PAM study). Breast Cancer Res. 2022, 24, 36. [Google Scholar] [CrossRef]
- Ren, X.; Wang, X.; Sun, J.; Hui, Z.; Lei, S.; Wang, C.; Wang, M. Effects of physical exercise on cognitive function of breast cancer survivors receiving chemotherapy: A systematic review of randomized controlled trials. Breast 2022, 63, 113–122. [Google Scholar] [CrossRef]
- Van Der Gucht, K.; Melis, M.; Ahmadoun, S.; Gebruers, A.; Smeets, A.; Vandenbulcke, M.; Wildiers, H.; Neven, P.; Kuppens, P.; Raes, F.; et al. A mindfulness-based intervention for breast cancer patients with cognitive impairment after chemotherapy: Study protocol of a three-group randomized controlled trial. Trials 2020, 21, 290. [Google Scholar] [CrossRef]
- Ponds, R.; van Boxtel, M.; Jolles, J. De “Cognitive Failure Questionnaire” als maat voor subjectief cognitief functioneren. Tijdschr. Voor Neuropsychol. 2006, 2, 37–45. [Google Scholar]
- Van der Gucht, K.; Takano, K.; Van Broeck, N.; Raes, F. A Mindfulness-Based Intervention for Economically Disadvantaged People: Effects on Symptoms of Stress, Anxiety, and Depression and on Cognitive Reactivity and Overgeneralization. Mindfulness 2015, 6, 1042–1052. [Google Scholar] [CrossRef]
- Van Der Gucht, K.; Takano, K.; Labarque, V.; Vandenabeele, K.; Nolf, N.; Kuylen, S.; Cosyns, V.; Van Broeck, N.; Kuppens, P.; Raes, F. A mindfulness-based intervention for adolescents and young adults after cancer treatment: Effects on quality of life, emotional distress, and cognitive vulnerability. J. Adolesc. Young Adult Oncol. 2017, 6, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Melis, M.; Blommaert, J.; Radwan, A.; Smeets, A.; Van der Gucht, K.; Deprez, S.; Sunaert, S. Structural brain changes after a mindfulness-based intervention in breast cancer survivors with cognitive complaints. Mindfulness 2023, 1, 1–16. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: How to Cope with Stress, Pain and Illness Using Mindfulness Meditation, 15th ed.; Delacorte Press: New York, NY, USA, 2001. [Google Scholar]
- Bartley, T. Mindfulness-Based Cognitive Therapy for Cancer: Gently Turning Towards; John Wiley & Sons: Hoboken, NJ, USA, 2012; ISBN 9780470683835. [Google Scholar]
- Stanic, J.; Barth, J.; Danon, N.; Bondolfi, G.; Jermann, F.; Eicher, M. Adherence to standardized 8-week mindfulness-based interventions among women with breast or gynecological cancer: A scoping review. J. Psychosoc. Oncol. Res. Pract. 2021, 3, e048. [Google Scholar] [CrossRef]
- WHO. Physical Activity and Adults; WHO: Geneva, Switzerland, 2015.
- Gorgolewski, K.J.; Auer, T.; Calhoun, V.D.; Craddock, R.C.; Das, S.; Duff, E.P.; Flandin, G.; Ghosh, S.S.; Glatard, T.; Halchenko, Y.O.; et al. The brain imaging data structure, a format for organizing and describing outputs of neuroimaging experiments. Sci. Data 2016, 3, 160044. [Google Scholar] [CrossRef]
- Esteban, O.; Birman, D.; Schaer, M.; Koyejo, O.O.; Poldrack, R.A.; Gorgolewski, K.J. MRIQC: Advancing the automatic prediction of image quality in MRI from unseen sites. PLoS ONE 2017, 12, e0184661. [Google Scholar] [CrossRef]
- Esteban, O.; Markiewicz, C.J.; Blair, R.W.; Moodie, C.A.; Isik, A.I.; Erramuzpe, A.; Kent, J.D.; Goncalves, M.; DuPre, E.; Snyder, M.; et al. fMRIPrep: A robust preprocessing pipeline for functional MRI. Nat. Methods 2018, 16, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Peterson, D.J.; Gatenby, J.C.; Li, W.; Grabowski, T.J.; Madhyastha, T.M. Evaluation of field map and nonlinear registration methods for correction of susceptibility artifacts in diffusion MRI. Front. Neuroinform. 2017, 11, 17. [Google Scholar] [CrossRef]
- Pruim, R.H.R.; Mennes, M.; van Rooij, D.; Llera, A.; Buitelaar, J.K.; Beckmann, C.F. ICA-AROMA: A robust ICA-based strategy for removing motion artifacts from fMRI data. Neuroimage 2015, 112, 267–277. [Google Scholar] [CrossRef]
- Wang, Y.; Ghumare, E.; Vandenberghe, R.; Dupont, P. Comparison of different generalizations of clustering coefficient and local efficiency for weighted undirected graphs. Neural Comput. 2017, 29, 313–331. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 48. [Google Scholar] [CrossRef]
- Lorah, J. Effect size measures for multilevel models: Definition, interpretation, and TIMSS example. Large-Scale Assess. Educ. 2018, 6, 8. [Google Scholar] [CrossRef]
- Henneghan, A.M.; Palesh, O.; Harrison, M.; Kesler, S.R. Identifying cytokine predictors of cognitive functioning in breast cancer survivors up to 10 years post chemotherapy using machine learning. J. Neuroimmunol. 2018, 320, 38–47. [Google Scholar] [CrossRef]
- Schroyen, G.; Blommaert, J.; van Weehaeghe, D.; Sleurs, C.; Vandenbulcke, M.; Dedoncker, N.; Hatse, S.; Goris, A.; Koole, M.; Smeets, A.; et al. Neuroinflammation and its association with cognition, neuronal markers and peripheral inflammation after chemotherapy for breast cancer. Cancers 2021, 13, 4198. [Google Scholar] [CrossRef]
- Ringnér, M. What is principal component analysis? Nat. Biotechnol. 2008, 26, 303–304. [Google Scholar] [CrossRef]
- De Jager, W.; Bourcier, K.; Rijkers, G.T.; Prakken, B.J.; Seyfert-Margolis, V. Prerequisites for cytokine measurements in clinical trials with multiplex immunoassays. BMC Immunol. 2009, 10, 52. [Google Scholar] [CrossRef]
- Nieuwenhuis, R.; te Grotenhuis, M.; Pelzer, B. influence.ME: Tools for detecting influential data in mixed effects models-web of science core collection. R J. 2012, 4, 38–47. [Google Scholar] [CrossRef]
- Sporns, O. Network attributes for segregation and integration in the human brain. Curr. Opin. Neurobiol. 2013, 23, 162–171. [Google Scholar] [CrossRef]
- Bullmore, E.; Sporns, O. The economy of brain network organization. Nat. Rev. Neurosci. 2012, 13, 336–349. [Google Scholar] [CrossRef]
- Haddad, J.J. Cytokines and related receptor-mediated signaling pathways. Biochem. Biophys. Res. Commun. 2002, 297, 700–713. [Google Scholar] [CrossRef] [PubMed]
- Kleckner, I.R.; Kamen, C.; Cole, C.; Fung, C.; Heckler, C.E.; Guido, J.J.; Culakova, E.; Onitilo, A.A.; Conlin, A.; Kuebler, J.P.; et al. Effects of exercise on inflammation in patients receiving chemotherapy: A nationwide NCORP randomized clinical trial. Support. Care Cancer 2019, 27, 4615–4625. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. Proinflammatory Cytokines. Chest 2000, 118, 503–508. [Google Scholar] [CrossRef]
- Zimmer, P.; Baumann, F.T.; Oberste, M.; Schmitt, J.; Joisten, N.; Hartig, P.; Schenk, A.; Kuhn, R.; Bloch, W.; Reuss-Borst, M. Influence of personalized exercise recommendations during rehabilitation on the sustainability of objectively measured physical activity levels, fatigue, and fatigue-related biomarkers in patients with breast cancer. Integr. Cancer Ther. 2017, 17, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Nakagawa, S. Physical activity for cognitive health promotion: An overview of the underlying neurobiological mechanisms. Ageing Res. Rev. 2023, 86, 101868. [Google Scholar] [CrossRef] [PubMed]
- Broadbent, D.E.; Cooper, P.F.; FitzGerald, P.; Parkes, K.R. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br. J. Clin. Psychol. 1982, 21, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, S. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation: London, UK, 1995. [Google Scholar]
- Rizopoulos, D. ltm: An R package for latent variable modeling and item response analysis. J. Stat. Softw. 2007, 17, 1–25. [Google Scholar] [CrossRef]
- Vercoulen, J.H.M.M.; Swanink, C.M.A.; Fennis, J.F.M.; Galama, J.M.D.; van der Meer, J.W.M.; Bleijenberg, G. Dimensional assessment of chronic fatigue syndrome. J. Psychosom. Res. 1994, 38, 383–392. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mindfulness | Physical Training | Waitlist | ||||
|---|---|---|---|---|---|---|
| Mean (SD) [95% CI] or n (%) | blood (n = 43) | rsfMRI (n = 30) | blood (n = 36) | rsfMRI (n = 21) | blood (n = 38) | rsfMRI (n = 23) |
| Age | 47.2 (8.1) [44.7, 49.7] | 48.1 (7.8) [45.1, 51.2] | 48.0 (7.7) [45.4, 50.6] | 50.2 (6.9) [42.4, 58.0] | 50.1 (10.1) [46.8, 53.4] | 50.1 (10.2) [42.4, 57.8] |
| Time since chemo | 24.9 (14.8) [20.4, 29.5] | 26.8 (15.8) [21.2, 32.4] | 24.5 (13.6) [19.9, 29.1] | 25.3 (13.2) [11.0, 39.6] | 26.3 (15.1) [21.3, 31.2] | 25.5 (16.4) [11.4, 39.5] |
| Verbal IQ | 110 (7.2) [108.0, 112.0] | 109.3 (6.2) [107.0, 111.5] | 111 (5.3) [109.0, 113.0] | 110.2 (6.3) [104.4, 116.1] | 107 (5.2) [105.0, 109.0] | 108.5 (6.3) [102.8, 114.2] |
| Chemotherapy | 43 (100) | 30 (100) | 36 (100) | 21 (100) | 38 (100) | 23 (100) |
| Endocrine therapy | 30 (69.8) | 22 (73.3) | 27 (75.0) | 16 (76.2) | 26 (68.4) | 17 (73.9) |
| Radiotherapy | 27 (62.8) | 19 (63.3) | 24 (66.7) | 16 (76.2) | 34 (89.5) | 21 (91.3) |
| Current psychotherapy | 10 (23.3) | 6 (20.0) | 4 (11.1) | 5 (23.8) | 5 (13.2) | 3 (13.0) |
| Education level | ||||||
| Secondary school | 12 (27.9) | 6 (20.0) | 11 (30.6) | 4 (19.0) | 8 (21.1) | 6 (26.1) |
| Higher education | 31 (72.1) | 24 (80.0) | 25 (69.4) | 17 (81.0) | 30 (78.9) | 17 (73.9) |
| Race: Caucasian | 43 (100) | 30 (100) | 36 (100) | 21 (100) | 38 (100) | 23 (100) |
| Home Practice n (%) | Post-Intervention (t2) | Three-Month Follow-Up (t3) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mindfulness | Physical Training | Mindfulness | Physical Training | |||||
| Blood (n = 36) | rsfMRI (n = 30) | Blood (n = 31) | rsfMRI (n = 21) | Blood (n = 35) | rsfMRI (n = 30) | Blood (n = 31) | rsfMRI (n = 21) | |
| Never | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (3.2) | 1 (4.8) |
| Less than once a month | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (5.7) | 2 (6.7) | 0 (0.0) | 0 (0.0) |
| About once a month | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.9) | 1 (3.3) | 0 (0.0) | 0 (0.0) |
| Several times a month | 1 (2.8) | 1 (3.3) | 2 (6.5) | 1 (4.8) | 4 (11.4) | 3 (10.0) | 0 (0.0) | 0 (0.0) |
| About once a week | 6 (16.7) | 5 (16.7) | 2 (6.5) | 1 (4.8) | 8 (22.9) | 8 (26.7) | 3 (9.7) | 3 (14.3) |
| Several times a week | 18 (50.0) | 14 (46.7) | 17 (54.8) | 14 (66.7) | 16 (45.7) | 14 (46.7) | 11 (35.5) | 8 (38.1) |
| Daily | 7 (19.4) | 7 (23.3) | 0 (0.0) | 0 (0.0) | 2 (5.7) | 2 (6.7) | 0 (0.0) | 0 (0.0) |
| Not reported | 4 (11.1) | 3 (10.0) | 10 (32.3) | 5 (23.8) | 2 (5.7) | 0 (0.0) | 16 (51.6) | 9 (42.9) |
| Cytokine | PC1 | PC2 | PC3 | |||
|---|---|---|---|---|---|---|
| Loadings (% contribution to the component) | ||||||
| IL-12p70 | −0.37 | (13) | −0.12 | (1) | −0.27 | (7) |
| IFN-g | −0.35 | (12) | −0.18 | (3) | −0.05 | (0) |
| IL-1b | −0.34 | (12) | −0.20 | (4) | −0.09 | (1) |
| IL-8 | −0.31 | (10) | 0.19 | (4) | 0.03 | (0) |
| MCP-1 | −0.16 | (3) | 0.48 | (23) | 0.08 | (1) |
| MIP-1b | −0.20 | (4) | 0.43 | (19) | 0.29 | (9) |
| BDNF | −0.23 | (5) | 0.37 | (13) | −0.34 | (12) |
| TNF-a | −0.20 | (4) | −0.32 | (10) | 0.07 | (1) |
| IFN-a2 | −0.30 | (9) | −0.31 | (9) | 0.00 | (0) |
| IFN-b | −0.30 | (9) | 0.16 | (3) | −0.50 | (25) |
| IL-18 | −0.22 | (5) | 0.22 | (5) | 0.46 | (21) |
| IL-17A | −0.24 | (6) | −0.24 | (6) | 0.37 | (14) |
| IL-6 | −0.29 | (8) | −0.03 | (0) | 0.31 | (10) |
| Model metrics | ||||||
| Variance (in %) | 41 | 15 | 9 | |||
| Eigenvalue | 5.3 | 1.9 | 1.1 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melis, M.; Schroyen, G.; Blommaert, J.; Leenaerts, N.; Smeets, A.; Van Der Gucht, K.; Sunaert, S.; Deprez, S. The Impact of Mindfulness on Functional Brain Connectivity and Peripheral Inflammation in Breast Cancer Survivors with Cognitive Complaints. Cancers 2023, 15, 3632. https://doi.org/10.3390/cancers15143632
Melis M, Schroyen G, Blommaert J, Leenaerts N, Smeets A, Van Der Gucht K, Sunaert S, Deprez S. The Impact of Mindfulness on Functional Brain Connectivity and Peripheral Inflammation in Breast Cancer Survivors with Cognitive Complaints. Cancers. 2023; 15(14):3632. https://doi.org/10.3390/cancers15143632
Chicago/Turabian StyleMelis, Michelle, Gwen Schroyen, Jeroen Blommaert, Nicolas Leenaerts, Ann Smeets, Katleen Van Der Gucht, Stefan Sunaert, and Sabine Deprez. 2023. "The Impact of Mindfulness on Functional Brain Connectivity and Peripheral Inflammation in Breast Cancer Survivors with Cognitive Complaints" Cancers 15, no. 14: 3632. https://doi.org/10.3390/cancers15143632
APA StyleMelis, M., Schroyen, G., Blommaert, J., Leenaerts, N., Smeets, A., Van Der Gucht, K., Sunaert, S., & Deprez, S. (2023). The Impact of Mindfulness on Functional Brain Connectivity and Peripheral Inflammation in Breast Cancer Survivors with Cognitive Complaints. Cancers, 15(14), 3632. https://doi.org/10.3390/cancers15143632