

The Impact of NUTRItional Status at First Medical Oncology Visit on Clinical Outcomes: The NUTRIONCO Study

 , , ,
, , ,  , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design and Objective
2.3. Database Set-Up and Data Collection
2.4. Malnutrition- and Anorexia-Related Scores
2.5. Pre-Cachexia and Cachexia Determination at Baseline
2.6. Statistical Analysis
3. Results
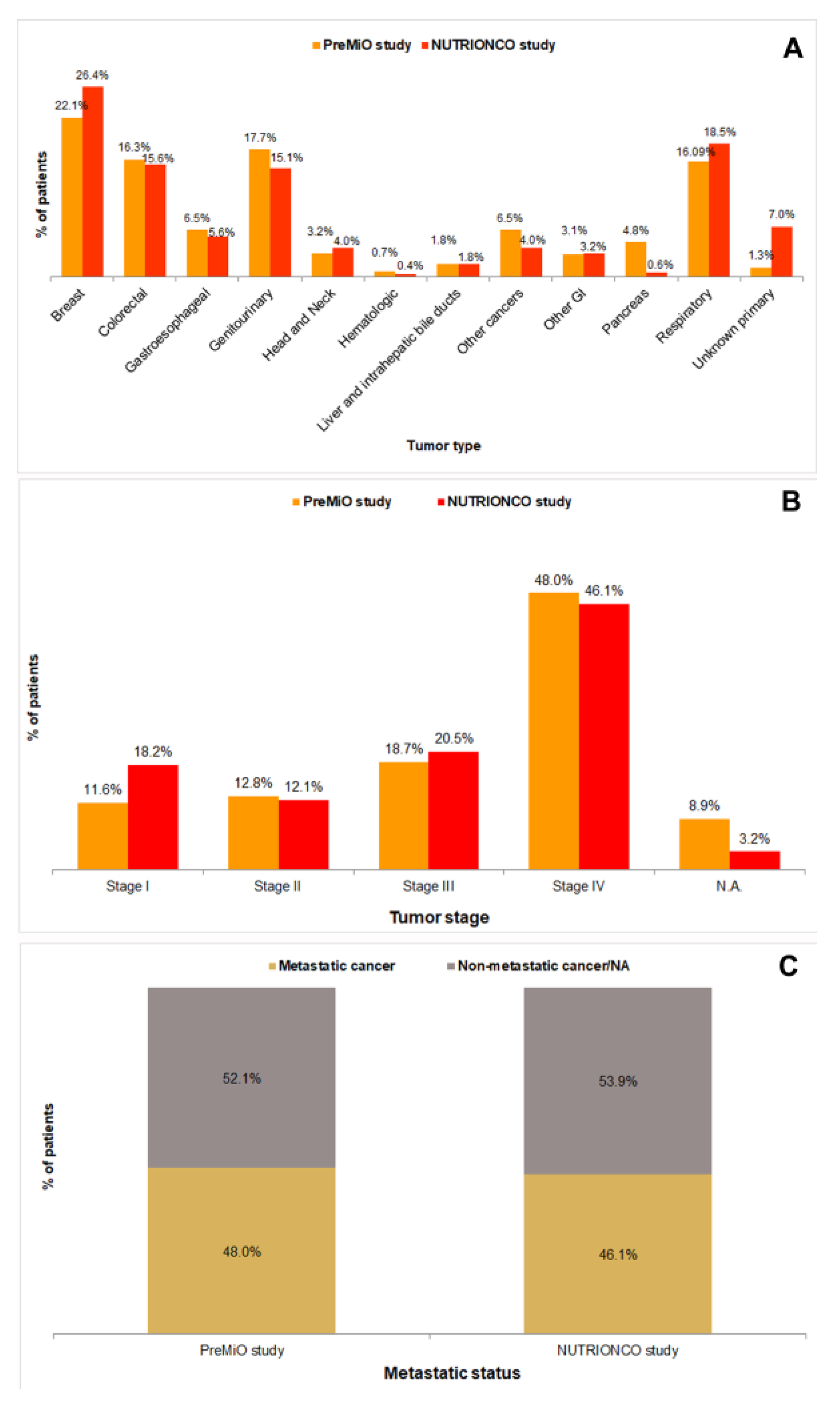
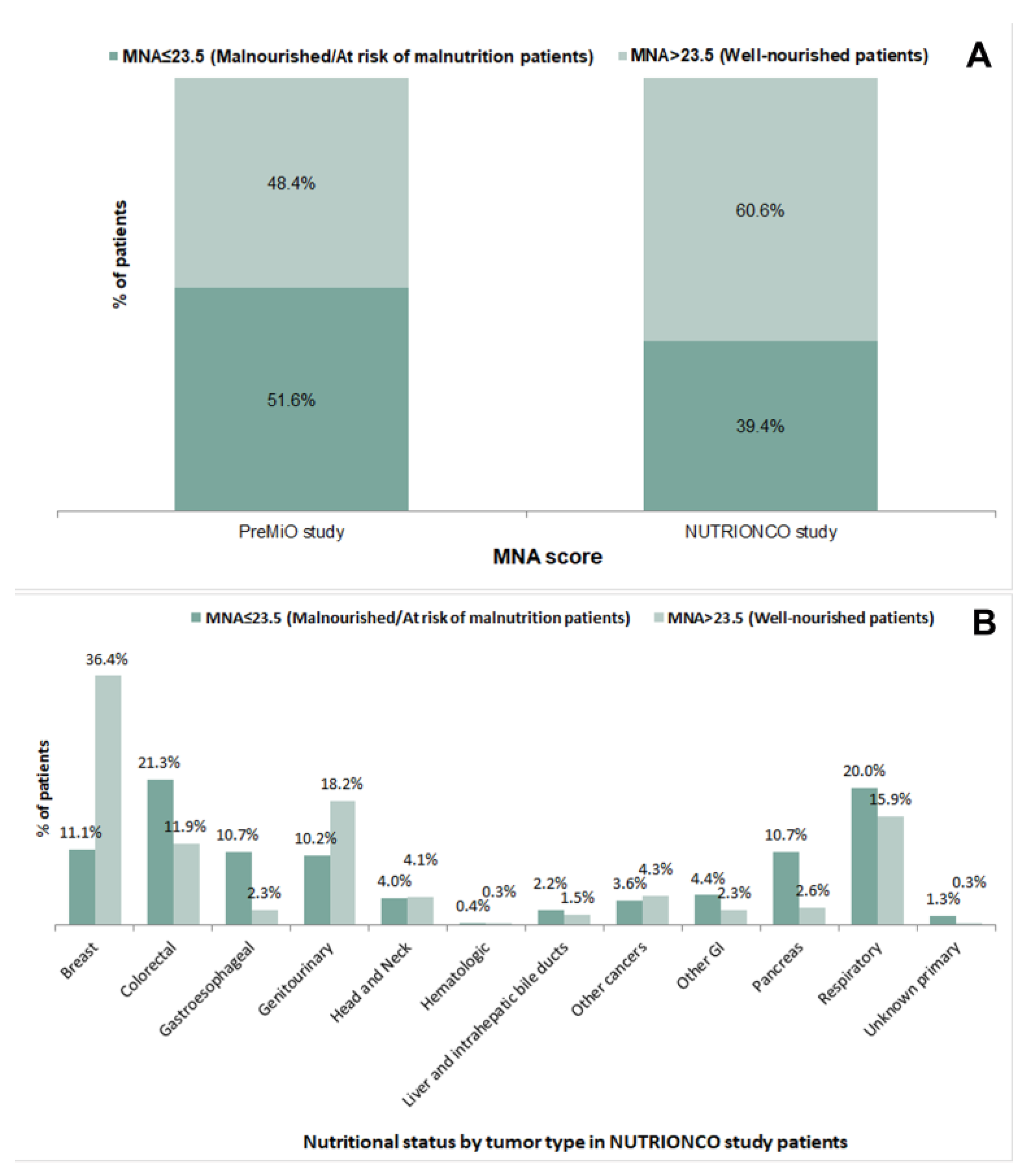
3.1. Patients’ Demographics and Baseline Characteristics: A Comparison between the PreMiO and the NUTRIONCO Study Populations
3.2. Baseline Characteristics and Clinical Outcomes: An Association Analysis in the NUTRIONCO Study Population
3.2.1. Outcome: Disease Progression
3.2.2. Outcome: Patient’s Death
3.2.3. Outcome: Patients’ Rehospitalization
3.2.4. Outcome: Treatment-Related Toxicity
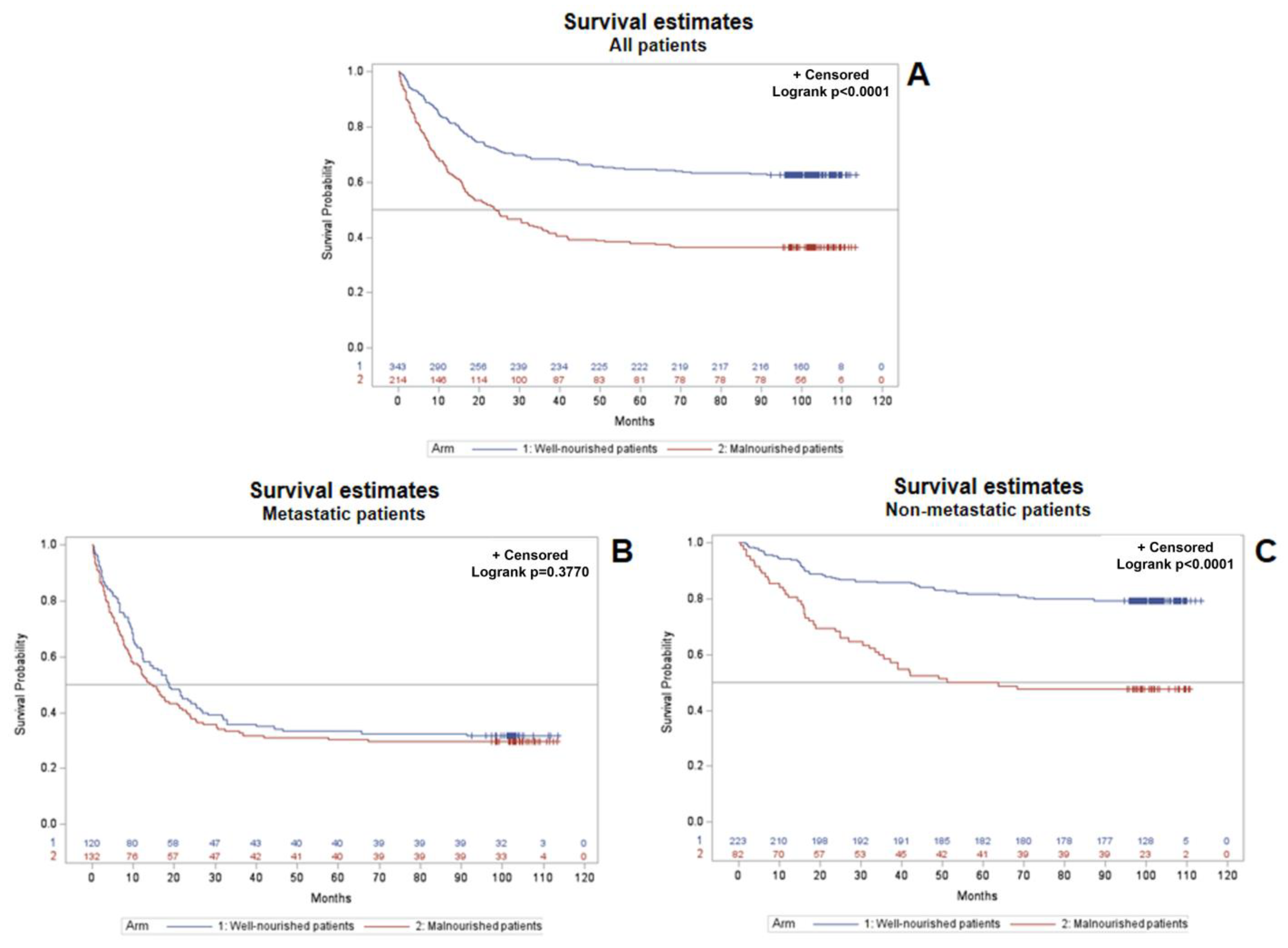
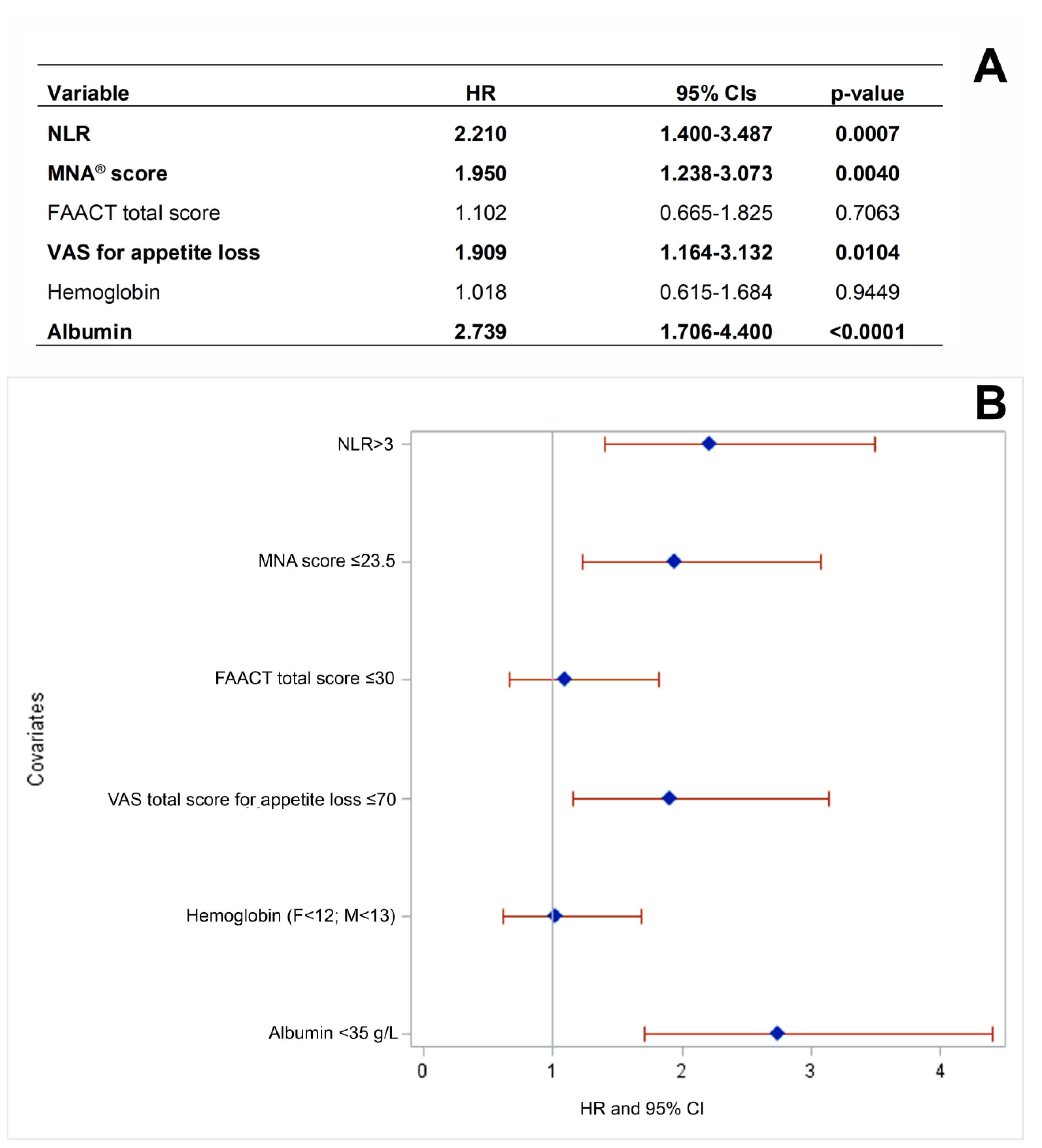
3.3. Baseline Characteristics and Patients’ Survival: A Multivariate Analysis in the NUTRIONCO Study Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 20 February 2023).
- Zimta, A.A.; Tigu, A.B.; Muntean, M.; Cenariu, D.; Slaby, O.; Berindan-Neagoe, I. Molecular Links between Central Obesity and Breast Cancer. Int. J. Mol. Sci. 2019, 20, 5364. [Google Scholar] [CrossRef]
- Saunders, J.; Smith, T. Malnutrition: Causes and consequences. Clin. Med. 2010, 10, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Bossi, P.; Delrio, P.; Mascheroni, A.; Zanetti, M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology According to Different Cancer Types and Settings: A Narrative Review. Nutrients 2021, 13, 1980. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Lucia, S.; Farcomeni, A.; Lorusso, V.; Saracino, V.; Barone, C.; Plastino, F.; Gori, S.; Magarotto, R.; Carteni, G.; et al. Prevalence of malnutrition in patients at first medical oncology visit: The PreMiO study. Oncotarget 2017, 8, 79884–79896. [Google Scholar] [CrossRef]
- Martin, L.; Muscaritoli, M.; Bourdel-Marchasson, I.; Kubrak, C.; Laird, B.; Gagnon, B.; Chasen, M.; Gioulbasanis, I.; Wallengren, O.; Voss, A.C.; et al. Diagnostic criteria for cancer cachexia: Reduced food intake and inflammation predict weight loss and survival in an international, multi-cohort analysis. J. Cachexia Sarcopenia Muscle 2021, 12, 1189–1202. [Google Scholar] [CrossRef] [PubMed]
- Marceca, G.P.; Londhe, P.; Calore, F. Management of Cancer Cachexia: Attempting to Develop New Pharmacological Agents for New Effective Therapeutic Options. Front. Oncol. 2020, 10, 298. [Google Scholar] [CrossRef] [PubMed]
- van der Meij, B.S.; Teleni, L.; McCarthy, A.L.; Isenring, E.A. Cancer Cachexia: An Overview of Diagnostic Criteria and Therapeutic Approaches for the Accredited Practicing Dietitian. J. Hum. Nutr. Diet. 2020, 34, 243–254. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Molfino, A.; Gioia, G.; Laviano, A.; Rossi Fanelli, F. The “parallel pathway”: A novel nutritional and metabolic approach to cancer patients. Intern. Emerg. Med. 2011, 6, 105–112. [Google Scholar] [CrossRef]
- Ni, J.; Zhang, L. Cancer Cachexia: Definition, Staging, and Emerging Treatments. Cancer Manag. Res. 2020, 12, 5597–5605. [Google Scholar] [CrossRef]
- O’Connell, T.M.; Golzarri-Arroyo, L.; Pin, F.; Barreto, R.; Dickinson, S.L.; Couch, M.E.; Bonetto, A. Metabolic Biomarkers for the Early Detection of Cancer Cachexia. Front. Cell. Dev. Biol. 2021, 9, 720096. [Google Scholar] [CrossRef]
- Ryan, A.M.; Prado, C.M.; Sullivan, E.S.; Power, D.G.; Daly, L.E. Effects of weight loss and sarcopenia on response to chemotherapy, quality of life, and survival. Nutrition 2019, 67–68, 110539. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A.M.; Power, D.G.; Daly, L.; Cushen, S.J.; Ní Bhuachalla, Ē.; Prado, C.M. Cancer-associated malnutrition, cachexia and sarcopenia: The skeleton in the hospital closet 40 years later. Proc. Nutr. Soc. 2016, 75, 199–211. [Google Scholar] [CrossRef]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and Classification of Cancer Cachexia: An International Consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Meyer, F.; Valentini, L. Disease-Related Malnutrition and Sarcopenia as Determinants of Clinical Outcome. Visc. Med. 2019, 35, 282–291. [Google Scholar] [CrossRef]
- Molfino, A.; Emerenziani, S.; Tonini, G.; Santini, D.; Gigante, A.; Guarino, M.P.L.; Nuglio, C.; Imbimbo, G.; La Cesa, A.; Cicala, M.; et al. Early impairment of food intake in patients newly diagnosed with cancer. Front. Nutr. 2023, 9, 997813. [Google Scholar] [CrossRef]
- Reber, E.; Schönenberger, K.A.; Vasiloglou, M.F.; Stanga, Z. Nutritional Risk Screening in Cancer Patients: The First Step Toward Better Clinical Outcome. Front. Nutr. 2021, 8, 603936. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Anker, S.D.; Argilés, J.; Aversa, Z.; Bauer, J.M.; Biolo, G.; Boirie, Y.; Bosaeus, I.; Cederholm, T.; Costelli, P.; et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: Joint document elaborated by Special Interest Groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin. Nutr. 2010, 29, 154–159. [Google Scholar] [CrossRef]
- Blauwhoff-Buskermolen, S.; Ruijgrok, C.; Ostelo, R.W.; de Vet, H.C.W.; Verheul, H.M.W.; de van der Schueren, M.A.E.; Langius, J.A.E. The assessment of anorexia in patients with cancer: Cut-off values for the FAACT-A/CS and the VAS for appetite. Support. Care Cancer 2016, 24, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Grenader, T.; Waddell, T.; Peckitt, C.; Oates, J.; Starling, N.; Cunningham, D.; Bridgewater, J. Prognostic value of neutrophil-to-lymphocyte ratio in advanced oesophago-gastric cancer: Exploratory analysis of the REAL-2 trial. Ann. Oncol. 2016, 27, 687–692. [Google Scholar] [CrossRef]
- McGovern, J.; Dolan, R.D.; Skipworth, R.J.; Laird, B.J.; McMillan, D.C. Cancer cachexia: A nutritional or a systemic inflammatory syndrome? Br. J. Cancer 2022, 127, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Gellrich, N.C.; Handschel, J.; Holtmann, H.; Krüskemper, G. Oral cancer malnutrition impacts weight and quality of life. Nutrients 2015, 7, 2145–2160. [Google Scholar] [CrossRef]
- Bolte, F.J.; McTavish, S.; Wakefield, N.; Shantzer, L.; Hubbard, C.; Krishnaraj, A.; Novicoff, W.; Gentzler, R.D.; Hall, R.D. Association of sarcopenia with survival in advanced NSCLC patients receiving concurrent immunotherapy and chemotherapy. Front. Oncol. 2022, 12, 986236. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Qi, Y.; Kong, X.; Su, Z.; Wang, Z.; Wang, X.; Du, Y.; Fang, Y.; Li, X.; Wang, J. Nutritional Risk Index Predicts Survival in Patients with Breast Cancer Treated with Neoadjuvant Chemotherapy. Front. Nutr. 2022, 8, 786742. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.E.; Coats, A.J.; Anker, S.D.; Sherman, L.; Klompenhouwer, T.; International Advisory Board, and Regional Advisory Boards for North America, Europe, and Japan. Identification and management of cancer cachexia in patients: Assessment of healthcare providers’ knowledge and practice gaps. J. Cachexia Sarcopenia Muscle 2022, 13, 2683–2696. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Corsaro, E.; Molfino, A. Awareness of Cancer-Related Malnutrition and Its Management: Analysis of the Results from a Survey Conducted Among Medical Oncologists. Front. Oncol. 2021, 11, 682999. [Google Scholar] [CrossRef]
- Durán-Poveda, M.; Suárez-de-la-Rica, A.; Cancer Minchot, E.; Ocón-Bretón, J.; Sánchez-Pernaute, A.; Rodríguez-Caravaca, G. Knowledge and Practices of Digestive Surgeons concerning Specialized Nutritional Support in Cancer Patients: A Survey Study. Nutrients 2022, 14, 4764. [Google Scholar] [CrossRef]
- Clamon, G.; Byrne, M.M.; Talbert, E.E. Inflammation as a Therapeutic Target in Cancer Cachexia. Cancers 2022, 14, 5262. [Google Scholar] [CrossRef]
- de Matos-Neto, E.M.; Lima, J.D.; de Pereira, W.O.; Figuerêdo, R.G.; Riccardi, D.M.; Radloff, K.; das Neves, R.X.; Camargo, R.G.; Maximiano, L.F.; Tokeshi, F.; et al. Systemic Inflammation in Cachexia-Is Tumor Cytokine Expression Profile the Culprit? Front. Immunol. 2015, 6, 629. [Google Scholar] [CrossRef]
- Kaya, T.; Açıkgöz, S.B.; Yıldırım, M.; Nalbant, A.; Altaş, A.E.; Cinemre, H. Association between neutrophil-to-lymphocyte ratio and nutritional status in geriatric patients. J. Clin. Lab. Anal. 2019, 33, e22636. [Google Scholar] [CrossRef]
- Hsueh, W.H.; Hsueh, S.W.; Yeh, K.Y.; Hung, Y.S.; Ho, M.M.; Lin, S.Y.; Tseng, C.K.; Hung, C.Y.; Chou, W.C. Albumin and Neutrophil-to-Lymphocyte Ratio Score in Neoadjuvant Concurrent Chemoradiotherapy for Esophageal Cancer: Comparison with Prognostic Nutritional Index. In Vivo 2022, 36, 2400–2408. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.M.; Soares, J.D.P.; Borges, T.C.; Gomes, T.L.N.; Pimentel, G.D. High neutrophil to lymphocytes ratio is associated with nutritional risk in hospitalised, unselected cancer patients: A cross-sectional study. Sci. Rep. 2021, 11, 17120. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, G.J.; Charles, K.A.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil-lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [PubMed]
- Corbeau, I.; Jacot, W.; Guiu, S. Neutrophil to Lymphocyte Ratio as Prognostic and Predictive Factor in Breast Cancer Patients: A Systematic Review. Cancers 2020, 12, 958. [Google Scholar] [CrossRef]
- Nunno, V.D.; Mollica, V.; Gatto, L.; Santoni, M.; Cosmai, L.; Porta, C.; Massari, F. Prognostic impact of neutrophil-to-lymphocyte ratio in renal cell carcinoma: A systematic review and meta-analysis. Immunotherapy 2019, 11, 631–643. [Google Scholar] [CrossRef]
- Allenet, C.; Klein, C.; Rouget, B.; Margue, G.; Capon, G.; Alezra, E.; Blanc, P.; Estrade, V.; Bladou, F.; Robert, G.; et al. Can Pre-Operative Neutrophil-to-Lymphocyte Ratio (NLR) Help Predict Non-Metastatic Renal Carcinoma Recurrence after Nephrectomy? (UroCCR-61 Study). Cancers 2022, 14, 5692. [Google Scholar] [CrossRef]
- Bland, K.A.; Zopf, E.M.; Harrison, M.; Ely, M.; Cormie, P.; Liu, E.; Dowd, A.; Martin, P. Prognostic Markers of Overall Survival in Cancer Patients Attending a Cachexia Support Service: An Evaluation of Clinically Assessed Physical Function, Malnutrition and Inflammatory Status. Nutr. Cancer 2021, 73, 1400–1410. [Google Scholar] [CrossRef] [PubMed]
- Dolan, R.D.; McSorley, S.T.; Horgan, P.G.; Laird, B.; McMillan, D.C. The role of the systemic inflammatory response in predicting outcomes in patients with advanced inoperable cancer: Systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2017, 116, 134–146. [Google Scholar] [CrossRef]
- Ludwig, H.; Van Belle, S.; Barrett-Lee, P.; Birgegård, G.; Bokemeyer, C.; Gascón, P.; Kosmidis, P.; Krzakowski, M.; Nortier, J.; Olmi, P.; et al. The European Cancer Anaemia Survey (ECAS): A large, multinational, prospective survey defining the prevalence, incidence, and treatment of anaemia in cancer patients. Eur. J. Cancer 2004, 40, 2293–2306. [Google Scholar] [CrossRef]
- Zhang, X.W.; Zhang, Q.; Song, M.M.; Zhang, K.P.; Zhang, X.; Ruan, G.T.; Yang, M.; Ge, Y.Z.; Tang, M.; Li, X.R.; et al. The prognostic effect of hemoglobin on patients with cancer cachexia: A multicenter retrospective cohort study. Support. Care Cancer 2022, 30, 875–885. [Google Scholar] [CrossRef] [PubMed]
- Molfino, A.; de van der Schueren, M.A.E.; Sánchez-Lara, K.; Milke, P.; Amabile, M.I.; Imbimbo, G.; Di Lazzaro, L.; Cavuto, S.; Ronzani, G.; Snegovoy, A.; et al. Cancer-associated anorexia: Validity and performance overtime of different appetite tools among patients at their first cancer diagnosis. Clin. Nutr. 2021, 40, 4037–4042. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Watanabe, S.; Fainsinger, R.; Lau, F.; Ghosh, S.; Quan, H.; Atkins, M.; Fassbender, K.; Downing, G.M.; Baracos, V. Prognostic factors in patients with advanced cancer: Use of the patient-generated subjective global assessment in survival prediction. J. Clin. Oncol. 2010, 28, 4376–4383. [Google Scholar] [CrossRef] [PubMed]
- Torbahn, G.; Strauss, T.; Sieber, C.C.; Kiesswetter, E.; Volkert, D. Nutritional status according to the mini nutritional assessment (MNA)® as potential prognostic factor for health and treatment outcomes in patients with cancer-a systematic review. BMC Cancer 2020, 20, 594. [Google Scholar] [CrossRef] [PubMed]
- de van der Schueren, M.A.E.; Laviano, A.; Blanchard, H.; Jourdan, M.; Arends, J.; Baracos, V.E. Systematic review and meta-analysis of the evidence for oral nutritional intervention on nutritional and clinical outcomes during chemo(radio)therapy: Current evidence and guidance for design of future trials. Ann. Oncol. 2018, 29, 1141–1153. [Google Scholar] [CrossRef]
- Schuetz, P.; Sulo, S.; Walzer, S.; Krenberger, S.; Brunton, C. Nutritional support during the hospital stay is cost-effective for preventing adverse outcomes in patients with cancer. Front. Oncol. 2022, 12, 916073. [Google Scholar] [CrossRef]
- Nishie, K.; Sato, S.; Hanaoka, M. Anamorelin for cancer cachexia. Drugs Today 2022, 58, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.L.; Teoh, S.E.; Yaow, C.Y.L.; Lin, D.J.; Masuda, Y.; Han, M.X.; Yeo, W.S.; Ng, Q.X. A Systematic Review and Meta-Analysis of the Clinical Use of Megestrol Acetate for Cancer-Related Anorexia/Cachexia. J. Clin. Med. 2022, 11, 3756. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Arends, J.; Aapro, M. From guidelines to clinical practice: A roadmap for oncologists for nutrition therapy for cancer patients. Ther. Adv. Med. Oncol. 2019, 11, 1758835919880084. [Google Scholar] [CrossRef]
- Ravasco, P.; Monteiro-Grillo, I.; Marques Vidal, P.; Camilo, M.E. Impact of nutrition on outcome: A prospective randomized controlled trial in patients with head and neck cancer undergoing radiotherapy. Head Neck 2005, 27, 659–668. [Google Scholar] [CrossRef]
- Isenring, E.A.; Capra, S.; Bauer, J.D. Nutrition intervention is beneficial in oncology outpatients receiving radiotherapy to the gastrointestinal or head and neck area. Br. J. Cancer 2004, 2, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Bar-Sela, G.; Battisti, N.M.L.; Belev, B.; Contreras-Martínez, J.; Cortesi, E.; de Brito-Ashurst, I.; Prado, C.M.; Ravasco, P.; Yalcin, S. Oncology-Led Early Identification of Nutritional Risk: A Pragmatic, Evidence-Based Protocol (PRONTO). Cancers 2023, 15, 380. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.D.B.; Pickhardt, P.J. CT-Derived Body Composition Assessment as a Prognostic Tool in Oncologic Patients: From Opportunistic Research to Artificial Intelligence-Based Clinical Implementation. AJR Am. J. Roentgenol. 2022, 219, 671–680. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Statistics | NUTRIONCO Study n = 571 | PreMiO Study n = 1952 |
|---|---|---|---|
| Age (years) | Mean (SD) | 63.7 ± 12.7 | 62.7 ± 12.9 |
| Gender | Male | 262 (45.9%) | 931 (47.7%) |
| Female | 309 (54.1%) | 1021 (52.3%) | |
| Weight (kg) | Mean (SD) | 68.3 ± 13.8 | 68.4 ± 13.2 |
| BMI (kg/m2) | Mean (SD) | 24.8 ± 4.6 | 24.8 ± 4.4 |
| Parameter | Statistics | NUTRIONCO Study n = 571 | PreMiO Study n = 1952 |
|---|---|---|---|
| Albumin (g/L) | Mean (SD) | 36.4 ± 6.0 | 36.3 ± 6.0 |
| Hemoglobin (g/dL) | Mean (SD) | M: 12.7 ± 1.9 | M: 12.4 ± 1.9 |
| F: 12.5 ± 1.6 | F: 12.2 ± 2.0 | ||
| NLR | Mean (SD) | 3.7 ± 3.7 | 3.9 ± 4.7 |
| FAACT total score | Mean (SD) | 31.0 ± 5.6 | 29.9 ± 5.9 |
| VAS anorexia | Mean (SD) | 69.8 ± 21.1 | 67.0 ± 22.6 |
| Tumor Type | FAACT ≤30 | FAACT >30 | VAS ≤70 | VAS >70 |
|---|---|---|---|---|
| Breast | 45 (17.2%) | 106 (34.2%) | 57 (20.1%) | 94 (32.8%) |
| Colorectal | 41 (15.7%) | 48 (15.5%) | 46 (16.2%) | 43 (15.0%) |
| Gastroesophageal | 26 (10.0%) | 6 (1.9%) | 27 (9.5%) | 5 (1.7%) |
| Genitourinary | 31 (11.9%) | 55 (17.7%) | 33 (11.6%) | 53 (18.5%) |
| Head and Neck | 8 (3.1%) | 15 (4.8%) | 10 (3.5%) | 13 (4.5%) |
| Hematologic | 1 (0.4%) | 1 (0.3%) | 1 (0.4%) | 1 (0.4%) |
| Liver and intrahepatic bile ducts | 6 (2.3%) | 4 (1.3%) | 5 (1.8%) | 5 (1.7%) |
| Other cancers | 12 (4.6%) | 11 (3.6%) | 12 (4.2%) | 11 (3.8%) |
| Other GI | 8 (3.1%) | 10 (3.2%) | 15 (5.3%) | 3 (1.1%) |
| Pancreas | 30 (11.5%) | 3 (1.0%) | 24 (8.5%) | 9 (3.1%) |
| Respiratory | 50 (19.2%) | 50 (16.1%) | 51 (18.0%) | 49 (17.1%) |
| Unknown primary | 3 (1.2%) | 1 (0.3%) | 3 (1.1%) | 1 (0.4%) |
| Parameter | Cut-Off Value/Status | Progression | Non-Progression | p-Value |
|---|---|---|---|---|
| Albumin (g/L) | <35 | 95 (78.5%) | 26 (21.5%) | <0.0001 |
| ≥35 | 107 (48.4%) | 114 (51.6%) | ||
| Hemoglobin (g/dL) | F < 12; M < 13 | 122 (69.3%) | 54 (30.7%) | 0.0003 |
| F ≥ 12; M ≥ 13 | 102 (47.0%) | 115 (53.0%) | ||
| NLR | >3 | 111 (71.2%) | 45 (28.8%) | <0.0001 |
| 1–3 | 111 (48.3%) | 119 (51.7%) | ||
| FAACT total score * | ≤30 | 97 (70.3%) | 41 (29.7%) | <0.0001 |
| >30 | 127 (49.4%) | 130 (50.6%) | ||
| VAS for appetite loss * | ≤70 | 124 (60.8%) | 80 (39.2%) | 0.0911 |
| >70 | 100 (52.4%) | 91 (47.6%) | ||
| MNA® * | Malnourished/At risk of malnutrition | 109 (70.8%) | 45 (29.2%) | <0.0001 |
| Well-nourished | 114 (47.5%) | 126 (52.5%) | ||
| Mestastatic status | Metastatic | 138 (82.1%) | 30 (17.9%) | <0.0001 |
| Non-metastatic | 86 (37.9%) | 141 (62.1%) |
| Parameter | Cut-Off Value/Status | Dead | Alive | p-Value |
|---|---|---|---|---|
| Albumin (g/L) | <35 | 139 (72.4%) | 53 (26.6%) | <0.0001 |
| ≥35 | 120 (39.5%) | 184 (60.5%) | ||
| Hemoglobin (g/dL) | F < 12; M < 13 | 162 (62.1%) | 99 (37.9%) | <0.0001 |
| F ≥ 12; M ≥ 13 | 116 (37.9%) | 190 (62.1%) | ||
| NLR | >3 | 156 (64.5%) | 86 (35.5%) | <0.0001 |
| 1–3 | 119 (37.5%) | 198 (62.5%) | ||
| FAACT total score * | ≤30 | 138 (65.7%) | 72 (34.3%) | <0.0001 |
| >30 | 140 (39.0%) | 219 (61.0%) | ||
| VAS for appetite loss * | ≤70 | 167 (59.0%) | 116 (41.0%) | <0.0001 |
| >70 | 111 (38.8%) | 175 (61.2%) | ||
| MNA® * | Malnourished/At risk of malnutrition | 146 (65.2%) | 78 (34.8%) | <0.0001 |
| Well-nourished | 131 (38.1%) | 213 (61.9%) | ||
| Mestastatic status | Metastatic | 186 (71.0%) | 76 (29.0%) | <0.0001 |
| Non-metastatic | 92 (30.0%) | 215 (70.0%) |
| Parameter | Cut-Off Value/Status | Rehospitalization | Non-Rehospitalization | p-Value |
|---|---|---|---|---|
| Albumin (g/L) | <35 | 93 (48.4%) | 99 (51.6%) | 0.1670 |
| ≥35 | 128 (42.1%) | 176 (57.9%) | ||
| Hemoglobin (g/dL) | F < 12; M < 13 | 125 (47.9%) | 136 (52.1%) | 0.0376 |
| F ≥ 12; M ≥ 13 | 120 (39.2%) | 186 (60.8%) | ||
| NLR | >3 | 116 (47.9%) | 126 (52.1%) | 0.0369 |
| 1–3 | 124 (39.1%) | 193 (60.9%) | ||
| FAACT total score * | ≤30 | 99 (47.1%) | 111 (52.9%) | 0.1323 |
| >30 | 146 (40.7%) | 213 (59.3%) | ||
| VAS for appetite loss * | ≤70 | 125 (44.2%) | 158 (55.8%) | 0.5942 |
| >70 | 120 (42.0%) | 166 (58.0%) | ||
| MNA® * | Malnourished/at risk of malnutrition | 103 (46.0%) | 121 (54.0%) | 0.2400 |
| Well-nourished | 141 (41.0%) | 203 (59.0%) | ||
| Mestastatic status | Metastatic | 138 (52.7%) | 124 (47.3%) | <0.0001 |
| Non-metastatic | 107 (34.9%) | 200 (65.1%) |
| Parameter | Cut-Off Value/Status | Toxicity | Non-Toxicity | p-Value |
|---|---|---|---|---|
| Albumin (g/L) | <35 | 65 (33.9%) | 127 (66.2%) | 0.7035 |
| ≥35 | 108 (35.5%) | 196 (64.5%) | ||
| Hemoglobin (g/dL) | F < 12; M < 13 | 82 (31.4%) | 179 (68.6%) | 0.1244 |
| F ≥ 12; M ≥ 13 | 115 (37.6%) | 191 (62.4%) | ||
| NLR | >3 | 85 (35.1%) | 157 (64.9%) | 0.7950 |
| 1–3 | 108 (34.1%) | 209 (65.9%) | ||
| FAACT total score * | ≤30 | 67 (31.9%) | 143 (68.1%) | 0.2974 |
| >30 | 130 (36.2%) | 229 (63.8%) | ||
| VAS for appetite loss * | ≤70 | 97 (34.3%) | 186 (65.7%) | 0.8628 |
| >70 | 100 (35.0%) | 186 (65.0%) | ||
| MNA® * | Malnourished/at risk of malnutrition | 70 (31.2%) | 154 (68.8%) | 0.1654 |
| Well-nourished | 127 (36.9%) | 217 (63.1%) | ||
| Mestastatic status | Metastatic | 93 (35.5%) | 169 (64.5%) | 0.6856 |
| Non-metastatic | 104 (33.9%) | 203 (66.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muscaritoli, M.; Modena, A.; Valerio, M.; Marchetti, P.; Magarotto, R.; Quadrini, S.; Narducci, F.; Tonini, G.; Grassani, T.; Cavanna, L.; et al. The Impact of NUTRItional Status at First Medical Oncology Visit on Clinical Outcomes: The NUTRIONCO Study. Cancers 2023, 15, 3206. https://doi.org/10.3390/cancers15123206
Muscaritoli M, Modena A, Valerio M, Marchetti P, Magarotto R, Quadrini S, Narducci F, Tonini G, Grassani T, Cavanna L, et al. The Impact of NUTRItional Status at First Medical Oncology Visit on Clinical Outcomes: The NUTRIONCO Study. Cancers. 2023; 15(12):3206. https://doi.org/10.3390/cancers15123206
Chicago/Turabian StyleMuscaritoli, Maurizio, Alessandra Modena, Matteo Valerio, Paolo Marchetti, Roberto Magarotto, Silvia Quadrini, Filomena Narducci, Giuseppe Tonini, Teresa Grassani, Luigi Cavanna, and et al. 2023. "The Impact of NUTRItional Status at First Medical Oncology Visit on Clinical Outcomes: The NUTRIONCO Study" Cancers 15, no. 12: 3206. https://doi.org/10.3390/cancers15123206
APA StyleMuscaritoli, M., Modena, A., Valerio, M., Marchetti, P., Magarotto, R., Quadrini, S., Narducci, F., Tonini, G., Grassani, T., Cavanna, L., Di Nunzio, C., Citterio, C., Occelli, M., Strippoli, A., Chiurazzi, B., Frassoldati, A., Altavilla, G., Lucenti, A., Nicolis, F., & Gori, S. (2023). The Impact of NUTRItional Status at First Medical Oncology Visit on Clinical Outcomes: The NUTRIONCO Study. Cancers, 15(12), 3206. https://doi.org/10.3390/cancers15123206