
Efficacy of Liver-Directed Combined Radiotherapy in Locally Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis

 , , , ,
, , , ,  , , , , ,
, , , , ,
Abstract
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
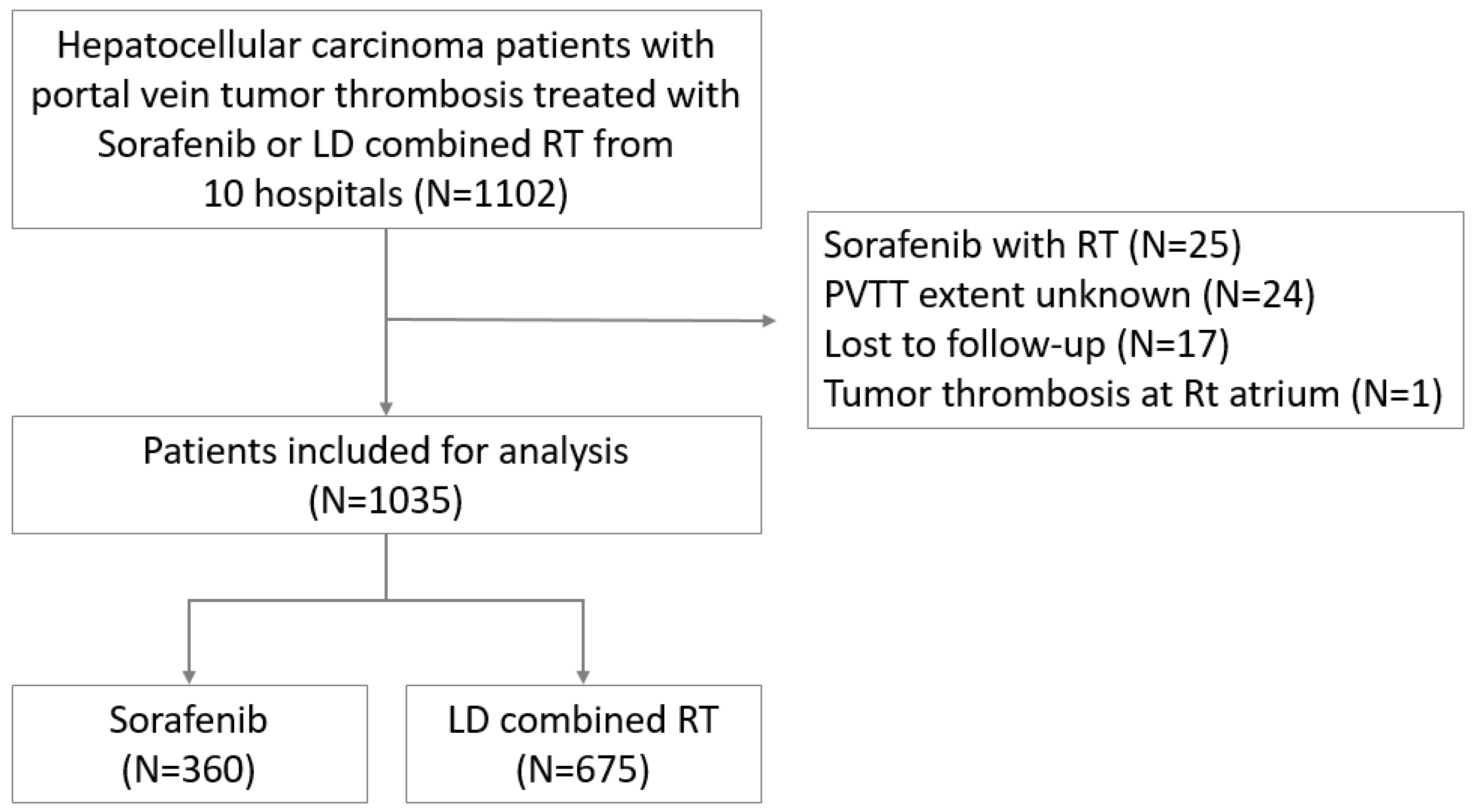
2.1. Study Population
2.2. Treatment
2.3. Response Evaluation and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Lee, D.S.; Seong, J. Radiotherapeutic options for hepatocellular carcinoma with portal vein tumor thrombosis. Liver Cancer 2014, 3, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Hamaoka, M.; Kobayashi, T.; Kuroda, S.; Iwako, H.; Okimoto, S.; Kimura, T.; Aikata, H.; Nagata, Y.; Chayama, K.; Ohdan, H. Hepatectomy after down-staging of hepatocellular carcinoma with portal vein tumor thrombus using chemoradiotherapy: A retrospective cohort study. Int. J. Surg. 2017, 44, 223–228. [Google Scholar] [CrossRef]
- Takizawa, D.; Kakizaki, S.; Sohara, N.; Sato, K.; Takagi, H.; Arai, H.; Katakai, K.; Kojima, A.; Matsuzaki, Y.; Mori, M. Hepatocellular carcinoma with portal vein tumor thrombosis: Clinical characteristics, prognosis, and patient survival analysis. Dig. Dis. Sci. 2007, 52, 3290–3295. [Google Scholar] [CrossRef] [PubMed]
- Qiu, G.; Xie, K.; Jin, Z.; Jiang, C.; Liu, H.; Wan, H.; Huang, J. The multidisciplinary management of hepatocellular carcinoma with portal vein tumor thrombus. Biosci. Trends 2021, 15, 148–154. [Google Scholar] [CrossRef]
- Cheng, S.; Yang, J.; Shen, F.; Zhou, W.; Wang, Y.; Cong, W.; Yang, G.S.; Cheng, H.; Hu, H.; Gao, C. Multidisciplinary management of hepatocellular carcinoma with portal vein tumor thrombus–eastern hepatobiliary surgical hospital consensus statement. Oncotarget 2016, 7, 40816. [Google Scholar] [CrossRef]
- Chan, S.L.; Chong, C.C.; Chan, A.W.; Poon, D.M.; Chok, K.S. Management of hepatocellular carcinoma with portal vein tumor thrombosis: Review and update at 2016. World J. Gastroenterol. 2016, 22, 7289. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R. Bclc strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2021, 76, 681–693. [Google Scholar] [CrossRef]
- Lu, J.; Zhang, X.-P.; Zhong, B.-Y.; Lau, W.Y.; Madoff, D.C.; Davidson, J.C.; Qi, X.; Cheng, S.-Q.; Teng, G.-J. Management of patients with hepatocellular carcinoma and portal vein tumour thrombosis: Comparing east and west. Lancet Gastroenterol. Hepatol. 2019, 4, 721–730. [Google Scholar] [CrossRef]
- Niu, Z.-J.; Ma, Y.-L.; Kang, P.; Ou, S.-Q.; Meng, Z.-B.; Li, Z.-K.; Qi, F.; Zhao, C. Transarterial chemoembolization compared with conservative treatment for advanced hepatocellular carcinoma with portal vein tumor thrombus: Using a new classification. Med. Oncol. 2012, 29, 2992–2997. [Google Scholar] [CrossRef] [PubMed]
- Ikai, I.; Arii, S.; Okazaki, M.; Okita, K.; Omata, M.; Kojiro, M.; Takayasu, K.; Nakanuma, Y.; Makuuchi, M.; Matsuyama, Y. Report of the 17th nationwide follow-up survey of primary liver cancer in japan. Hepatol. Res. 2007, 37, 676–691. [Google Scholar] [CrossRef]
- Choi, J.Y.; Jeong, I.Y.; Park, H.C.; Kwon, C.D.; Kim, J.M.; Joh, J.-W.; Choi, G.-S.; Park, J.B.; Kim, S.J.; Lee, S.H. The possibility of radiotherapy as downstaging to living donor liver transplantation for hepatocellular carcinoma with portal vein tumor thrombus. Liver Transplant. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transplant. Soc. 2017, 23, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.-A.; Chen, Y.-S.; Perng, D.-S. The role of radiotherapy in the treatment of hepatocellular carcinoma with portal vein tumor thrombus. J. Radiat. Res. 2015, 56, 325–331. [Google Scholar] [CrossRef]
- Yu, J.I.; Park, H.C. Radiotherapy as valid modality for hepatocellular carcinoma with portal vein tumor thrombosis. World J. Gastroenterol. 2016, 22, 6851. [Google Scholar] [CrossRef]
- Cho, J.Y.; Paik, Y.H.; Park, H.C.; Yu, J.I.; Sohn, W.; Gwak, G.Y.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W. The feasibility of combined transcatheter arterial chemoembolization and radiotherapy for advanced hepatocellular carcinoma. Liver Int. 2014, 34, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, T.; Hidaka, H.; Shibuya, A.; Okuwaki, Y.; Tanaka, Y.; Takada, J.; Minamino, T.; Watanabe, M.; Kokubu, S.; Koizumi, W. Overall survival in response to sorafenib versus radiotherapy in unresectable hepatocellular carcinoma with major portal vein tumor thrombosis: Propensity score analysis. BMC Gastroenterol. 2014, 14, 84. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.-H.; Li, A.-J.; Yang, G.-M.; Lai, E.C.; Zhou, W.-P.; Jiang, Z.-H.; Lau, W.Y.; Wu, M.-C. Surgical resection versus conformal radiotherapy combined with tace for resectable hepatocellular carcinoma with portal vein tumor thrombus: A comparative study. World J. Surg. 2013, 37, 1362–1370. [Google Scholar] [CrossRef]
- Kim, J.; Byun, H.K.; Kim, T.H.; Kim, S.I.; Kim, B.K.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Seong, J. Liver-directed concurrent chemoradiotherapy versus sorafenib in hepatocellular carcinoma with portal vein tumor thrombosis. Cancers 2022, 14, 2396. [Google Scholar] [CrossRef]
- Granito, A.; Facciorusso, A.; Sacco, R.; Bartalena, L.; Mosconi, C.; Cea, U.V.; Cappelli, A.; Antonino, M.; Modestino, F.; Brandi, N. Trans-tace: Prognostic role of the transient hypertransaminasemia after conventional chemoembolization for hepatocellular carcinoma. J. Pers. Med. 2021, 11, 1041. [Google Scholar] [CrossRef]
- Facciorusso, A.; Abd El Aziz, M.A.; Tartaglia, N.; Ramai, D.; Mohan, B.P.; Cotsoglou, C.; Pusceddu, S.; Giacomelli, L.; Ambrosi, A.; Sacco, R. Microwave ablation versus radiofrequency ablation for treatment of hepatocellular carcinoma: A meta-analysis of randomized controlled trials. Cancers 2020, 12, 3796. [Google Scholar] [CrossRef] [PubMed]
- Horvat, N.; De Oliveira, A.I.; Clemente de Oliveira, B.; Araujo-Filho, J.A.; El Homsi, M.; Elsakka, A.; Bajwa, R.; Martins, G.L.; Elsayes, K.M.; Menezes, M.R. Local-regional treatment of hepatocellular carcinoma: A primer for radiologists. RadioGraphics 2022, 42, 1670–1689. [Google Scholar] [CrossRef]
- Shi, J.; Lai, E.C.; Li, N.; Guo, W.-X.; Xue, J.; Lau, W.-Y.; Wu, M.-C.; Cheng, S.-Q. A new classification for hepatocellular carcinoma with portal vein tumor thrombus. J. Hepato-Biliary-Pancreat. Sci. 2011, 18, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, Y.; Kimura, T.; Kawaoka, T.; Ogawa, Y.; Amioka, K.; Naruto, K.; Yoshikawa, Y.; Kikukawa, C.; Suehiro, Y.; Yamaoka, K. Hepatic arterial infusion chemotherapy combined with radiation therapy for advanced hepatocellular carcinoma with tumor thrombosis of the main trunk or bilobar of the portal vein. Liver Cancer 2021, 10, 151–160. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Raoul, J.-L.; Sherman, M.; Mazzaferro, V.; Bolondi, L.; Craxi, A.; Galle, P.R.; Santoro, A.; Beaugrand, M.; Sangiovanni, A. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma: Subanalyses of a phase iii trial. J. Hepatol. 2012, 57, 821–829. [Google Scholar] [CrossRef]
- Zeng, Z.-C.; Fan, J.; Tang, Z.-Y.; Zhou, J.; Qin, L.-X.; Wang, J.-H.; Sun, H.-C.; Wang, B.-L.; Zhang, J.-Y.; Jiang, G.-L. A comparison of treatment combinations with and without radiotherapy for hepatocellular carcinoma with portal vein and/or inferior vena cava tumor thrombus. Int. J. Radiat. Oncol. * Biol. * Phys. 2005, 61, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Bo, W.-T.; Sun, J.; Xiang, X.; Lang, J.-Y.; Zhong, J.-H.; Li, L.-Q. New evidence and perspectives on the management of hepatocellular carcinoma with portal vein tumor thrombus. J. Clin. Transl. Hepatol. 2017, 5, 169. [Google Scholar]
- Meng, M.-B.; Cui, Y.-L.; Lu, Y.; She, B.; Chen, Y.; Guan, Y.-S.; Zhang, R.-M. Transcatheter arterial chemoembolization in combination with radiotherapy for unresectable hepatocellular carcinoma: A systematic review and meta-analysis. Radiother. Oncol. 2009, 92, 184–194. [Google Scholar] [CrossRef]
- Liao, M.; Huang, J.; Zhang, T.; Wu, H. Transarterial chemoembolization in combination with local therapies for hepatocellular carcinoma: A meta-analysis. PLoS ONE 2013, 8, e68453. [Google Scholar] [CrossRef]
- Huo, Y.R.; Eslick, G.D. Transcatheter arterial chemoembolization plus radiotherapy compared with chemoembolization alone for hepatocellular carcinoma: A systematic review and meta-analysis. JAMA Oncol. 2015, 1, 756–765. [Google Scholar] [CrossRef]
- Yoon, S.M.; Ryoo, B.-Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.H.; Lee, H.C.; Lim, Y.-S. Efficacy and safety of transarterial chemoembolization plus external beam radiotherapy vs sorafenib in hepatocellular carcinoma with macroscopic vascular invasion: A randomized clinical trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef]
- Lin, D.-X.; Zhang, Q.-Y.; Li, X.; Ye, Q.-W.; Lin, F.; Li, L.-L. An aggressive approach leads to improved survival in hepatocellular carcinoma patients with portal vein tumor thrombus. J. Cancer Res. Clin. Oncol. 2011, 137, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Feng, S.; Xue, J.; Wei, X.-B.; Shi, J.; Guo, W.-X.; Lau, W.-Y.; Wu, M.-C.; Cheng, S.-Q.; Meng, Y. Hepatocellular carcinoma with main portal vein tumor thrombus: A comparative study comparing hepatectomy with or without neoadjuvant radiotherapy. Hpb 2016, 18, 549–556. [Google Scholar] [CrossRef]
- Lee, W.H.; Byun, H.K.; Choi, J.S.; Choi, G.H.; Joo, D.J.; Han, K.-H.; Seong, J. Liver-directed combined radiotherapy as a bridge to curative surgery in locally advanced hepatocellular carcinoma beyond the milan criteria. Radiother. Oncol. 2020, 152, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Abulimiti, M.; Li, Z.; Wang, H.; Apiziaji, P.; Abulimiti, Y.; Tan, Y. Combination intensity-modulated radiotherapy and sorafenib improves outcomes in hepatocellular carcinoma with portal vein tumor thrombosis. J. Oncol. 2021, 2021, 9943683. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.H.; Fei, Z.L.; Zhou, J.P.; Hu, Z.T.; Hao, W.S. A comparison between three-dimensional conformal radiotherapy combined with interventional treatment and interventional treatment alone for hepatocellular carcinoma with portal vein tumour thrombosis. J. Med. Imaging Radiat. Oncol. 2015, 59, 109–114. [Google Scholar] [CrossRef]
- Manzar, G.S.; De, B.S.; Abana, C.O.; Lee, S.S.; Javle, M.; Kaseb, A.O.; Vauthey, J.-N.; Tran Cao, H.S.; Koong, A.C.; Smith, G.L. Outcomes and toxicities of modern combined modality therapy with atezolizumab plus bevacizumab and radiation therapy for hepatocellular carcinoma. Cancers 2022, 14, 1901. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|
| Sorafenib | LD Combined RT | Sorafenib | LD Combined RT | |||
| (N = 360) | (N = 675) | p Value | (N = 305) | (N = 305) | p Value | |
| Sex, n (%) | 0.029 | 0.905 | ||||
| Female | 59 (16.4) | 78 (11.6) | 41 (13.4) | 40 (13.1) | ||
| Median age [IQR], years | 60 [52–68] | 55 [49–63] | <0.001 | 59 [51–67] | 57 [50–65] | 0.090 |
| ECOG, PS, n (%) | <0.001 | 0.344 | ||||
| 0 | 86 (23.9) | 179 (26.5) | 82 (26.9) | 67 (22.0) | ||
| 1 | 220 (61.1) | 457 (67.7) | 185 (60.7) | 222 (72.8) | ||
| 2 | 40 (11.1) | 37 (5.5) | 30 (9.8) | 15 (4.9) | ||
| 3 | 14 (3.9) | 2 (0.2) | 8 (2.6) | 1 (0.3) | ||
| Etiology, n (%) | 0.174 | 0.536 | ||||
| HBV | 252 (70.0) | 522 (77.3) | 218 (71.5) | 220 (72.1) | ||
| HCV | 67 (18.6) | 68 (10.1) | 52 (17.0) | 37 (12.1) | ||
| NBNC | 41 (11.4) | 85 (12.6) | 35 (11.5) | 48 (15.7) | ||
| Child–Pugh class, n (%) | 0.123 | 0.777 | ||||
| A | 268 (74.4) | 504 (74.6) | 230 (75.4) | 233 (76.4) | ||
| B | 90 (25.0) | 170 (25.2) | 75 (24.6) | 72 (23.6) | ||
| C | 2 (0.6) | 1 (0.2) | 0 | 0 | ||
| Prior treatment history, n (%) | <0.001 | 0.321 | ||||
| Yes | 170 (47.2) | 138 (20.4) | 126 (41.3) | 114 (37.4) | ||
| Median AFP [IQR], ng/mL | 1040.1 [42.6–17,218.8] | 627.3 [31.0–11,572.2] | 0.446 | 962.3 [45.7–15,769.0] | 443.1 [26.7–9828.0] | 0.602 |
| Median tumor size [IQR], cm | 8.2 [5.4–11.7] | 9.6 [6.2–13.0] | <0.001 | 8.4 [5.5–11.9] | 8.4 [5.3–11.0] | 0.907 |
| Disease extent | <0.001 | 0.257 | ||||
| Bilateral | 220 (61.1) | 248 (36.7) | 170 (55.7) | 156 (51.1) | ||
| Lymph node status | 0.848 | 0.257 | ||||
| Involved | 47 (13.1) | 91 (13.5) | 40 (13.1) | 31 (10.2) | ||
| PVTT type (Cheng’s criteria) | 0.002 | 0.945 | ||||
| I | 24 (6.7) | 15 (2.2) | 16 (5.2) | 12 (3.9) | ||
| II | 193 (53.6) | 357 (52.9) | 164 (53.8) | 168 (55.1) | ||
| III | 138 (38.3) | 297 (44.0) | 121 (39.7) | 124 (40.7) | ||
| IV | 5 (1.4) | 6 (0.9) | 4 (1.3) | 1 (0.3) | ||
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Before PSM | ||||||
| Treatment (LD combined RT vs. Sorafenib) | 0.52 | 0.45–0.59 | <0.001 | 0.43 | 0.37–0.50 | <0.001 |
| Sex (Female vs. Male) | 1.11 | 0.92–1.35 | 0.275 | N.S. | ||
| Age | 1.00 | 1.00–1.01 | 0.456 | N.S. | ||
| ECOG PS (2-3 vs. 0-1) | 1.35 | 1.08–1.70 | 0.009 | N.S. | ||
| Child–Pugh class (B-C vs. A) | 1.98 | 1.71–2.30 | <0.001 | 1.78 | 1.52–2.07 | <0.001 |
| Prior treatment history (Yes vs. No) | 1.13 | 0.98–1.30 | 0.089 | N.S. | ||
| Log(Pretreatment AFP) | 1.22 | 1.16–1.27 | <0.001 | 1.18 | 1.13–1.24 | <0.001 |
| Tumor size | 1.04 | 1.03–1.05 | <0.001 | 1.04 | 1.03–1.06 | <0.001 |
| Disease extent (Bilateral vs. Unilateral) | 1.39 | 1.22–1.58 | <0.001 | N.S. | ||
| LN status (Involved vs. Not involved) | 1.29 | 1.07–1.55 | 0.008 | N.S. | ||
| PVTT type (III, IV vs. I, II) | 1.23 | 1.08–1.40 | 0.002 | N.S. | ||
| After PSM | ||||||
| Treatment (LD combined RT vs. Sorafenib) | 0.52 | 0.44–0.61 | <0.001 | 0.46 | 0.39–0.55 | <0.001 |
| Sex (Female vs. Male) | 0.98 | 0.77–1.26 | 0.887 | N.S. | ||
| Age | 1.00 | 0.99–1.01 | 0.425 | N.S. | ||
| ECOG PS (2-3 vs. 0-1) | 1.60 | 1.19–2.14 | 0.002 | N.S. | ||
| Child–Pugh class (B vs. A) | 1.88 | 1.55–2.28 | <0.001 | 1.69 | 1.38–2.07 | <0.001 |
| Prior treatment history (Yes vs. No) | 0.91 | 0.77–1.09 | 0.308 | N.S. | ||
| Log(Pretreatment AFP) | 1.27 | 1.19–1.35 | <0.001 | 1.23 | 1.15–1.31 | <0.001 |
| Tumor size | 1.05 | 1.04–1.07 | <0.001 | 1.05 | 1.03–1.07 | <0.001 |
| Disease extent (Bilateral vs. Unilateral) | 1.35 | 1.14–1.61 | <0.001 | N.S. | ||
| LN status (Involved vs. Not involved) | 1.39 | 1.08–1.79 | 0.011 | N.S. | ||
| PVTT type (III, IV vs. I, II) | 1.28 | 1.08–1.52 | 0.004 | N.S. | ||
| Sorafenib (N = 360) | LD Combined RT (N = 675) | |||||
|---|---|---|---|---|---|---|
| Grade 1–2 | Grade 3–4 | Total | Grade 1–2 | Grade 3–4 | Total | |
| Acute toxicity (within 3 months) | ||||||
| Fatigue | 21 (5.8%) | 0 (0.0%) | 21 (5.8%) | 13 (1.9%) | 2 (0.3%) | 15 (2.2%) |
| Nausea | 9 (2.5%) | 1 (0.3%) | 10 (2.8%) | 18 (2.7%) | 3 (0.4%) | 21 (3.1%) |
| Vomiting | 9 (2.5%) | 0 (0.0%) | 9 (2.5%) | 19 (2.8%) | 0 (0.0%) | 19 (2.8%) |
| Anorexia | 22 (6.1%) | 0 (0.0%) | 22 (6.1%) | 25 (3.7%) | 2 (0.3%) | 27 (4.0%) |
| Fever | 4 (1.1%) | 2 (0.6%) | 6 (1.7%) | 14 (2.1%) | 0 (0.0%) | 14 (2.1%) |
| Hand–foot syndrome | 26 (7.2%) | 2 (0.6%) | 28 (7.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Skin rash | 35 (9.7%) | 4 (1.1%) | 39 (10.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Leukopenia | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 5 (0.7%) | 0 (0.0%) | 5 (0.7%) |
| Diarrhea | 61 (16.9%) | 4 (1.1%) | 65 (18.1%) | 7 (1.0%) | 0 (0.0%) | 7 (1.0%) |
| AST/ALT elevation | 31 (8.6%) | 16 (4.4%) | 47 (13.0%) | 52 (7.7%) | 21 (3.1%) | 73 (10.8%) |
| Bilirubin elevation | 27 (7.5%) | 15 (4.2%) | 42 (11.7%) | 38 (5.6%) | 26 (3.9%) | 64 (9.5%) |
| Abdominal pain | 25 (6.9%) | 2 (0.6%) | 27 (7.5%) | 38 (5.6%) | 1 (0.2%) | 39 (5.8%) |
| Late toxicity (after 3 months) | ||||||
| Fatigue | 2 (0.6%) | 1 (0.3%) | 3 (0.8%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Hypertension | 2 (0.6%) | 0 (0.0%) | 2 (0.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| GI bleeding | 13 (3.6%) | 10 (2.8%) | 23 (6.4%) | 0 (0.0%) | 5 (0.7%) | 5 (0.7%) |
| Duodenal ulcer | 0 (0.0%) | 1 (0.3%) | 1 (0.3%) | 6 (0.9%) | 0 (0.0%) | 6 (0.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Cheng, J.C.-H.; Nam, T.-K.; Kim, J.H.; Jang, B.K.; Huang, W.-Y.; Aikata, H.; Kim, M.; Kwon, J.H.; Yue, J.; et al. Efficacy of Liver-Directed Combined Radiotherapy in Locally Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis. Cancers 2023, 15, 3164. https://doi.org/10.3390/cancers15123164
Kim J, Cheng JC-H, Nam T-K, Kim JH, Jang BK, Huang W-Y, Aikata H, Kim M, Kwon JH, Yue J, et al. Efficacy of Liver-Directed Combined Radiotherapy in Locally Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis. Cancers. 2023; 15(12):3164. https://doi.org/10.3390/cancers15123164
Chicago/Turabian StyleKim, Jina, Jason Chia-Hsien Cheng, Taek-Keun Nam, Jin Hee Kim, Byoung Kuk Jang, Wen-Yen Huang, Hiroshi Aikata, Myungsoo Kim, Jung Hyun Kwon, Jinbo Yue, and et al. 2023. "Efficacy of Liver-Directed Combined Radiotherapy in Locally Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis" Cancers 15, no. 12: 3164. https://doi.org/10.3390/cancers15123164
APA StyleKim, J., Cheng, J. C.-H., Nam, T.-K., Kim, J. H., Jang, B. K., Huang, W.-Y., Aikata, H., Kim, M., Kwon, J. H., Yue, J., Lee, V. H. F., Zeng, Z., & Seong, J. (2023). Efficacy of Liver-Directed Combined Radiotherapy in Locally Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis. Cancers, 15(12), 3164. https://doi.org/10.3390/cancers15123164