

Accuracy of Delirium Screening Tools in Older People with Cancer—A Systematic Review



Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
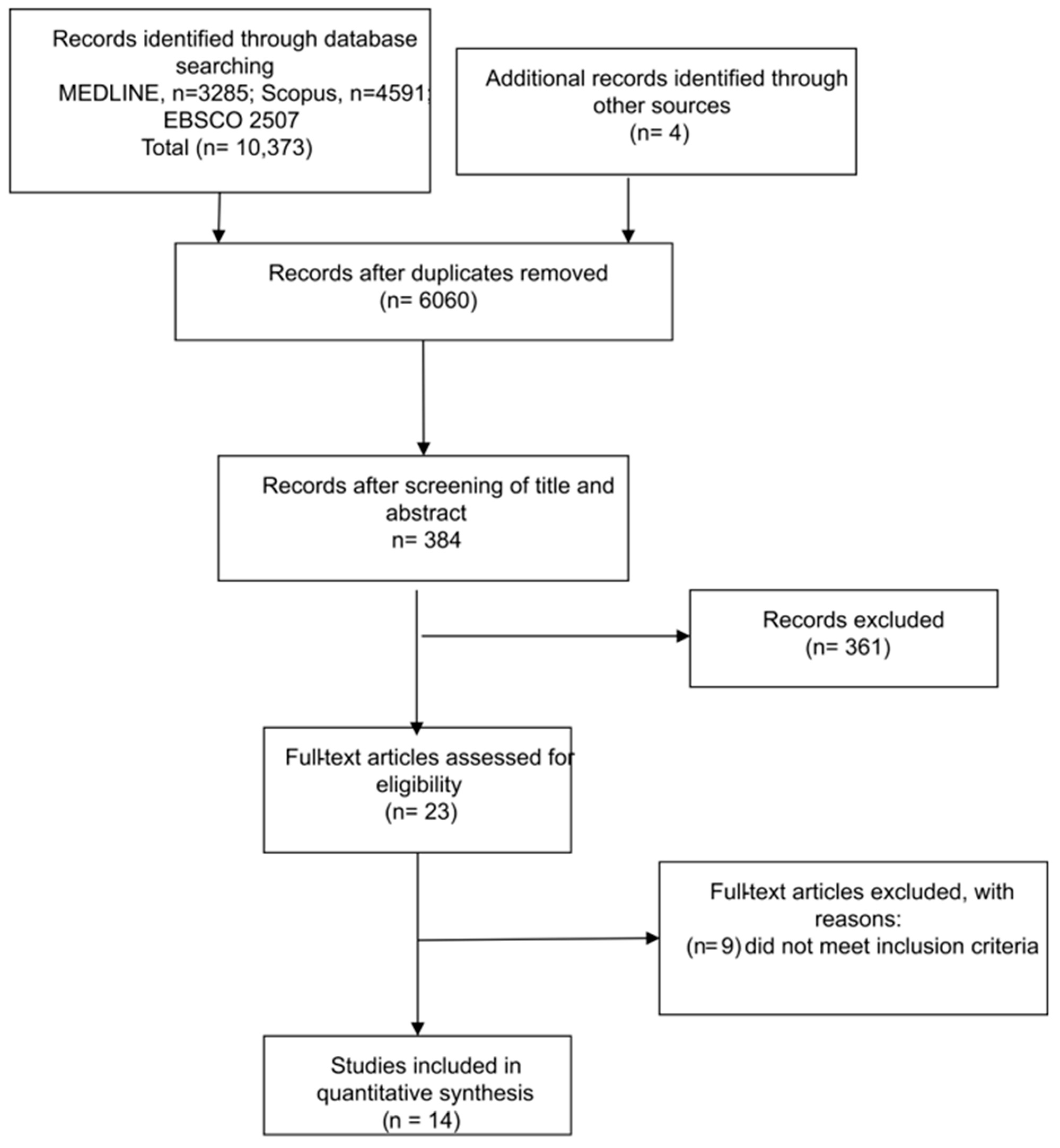
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Analysis
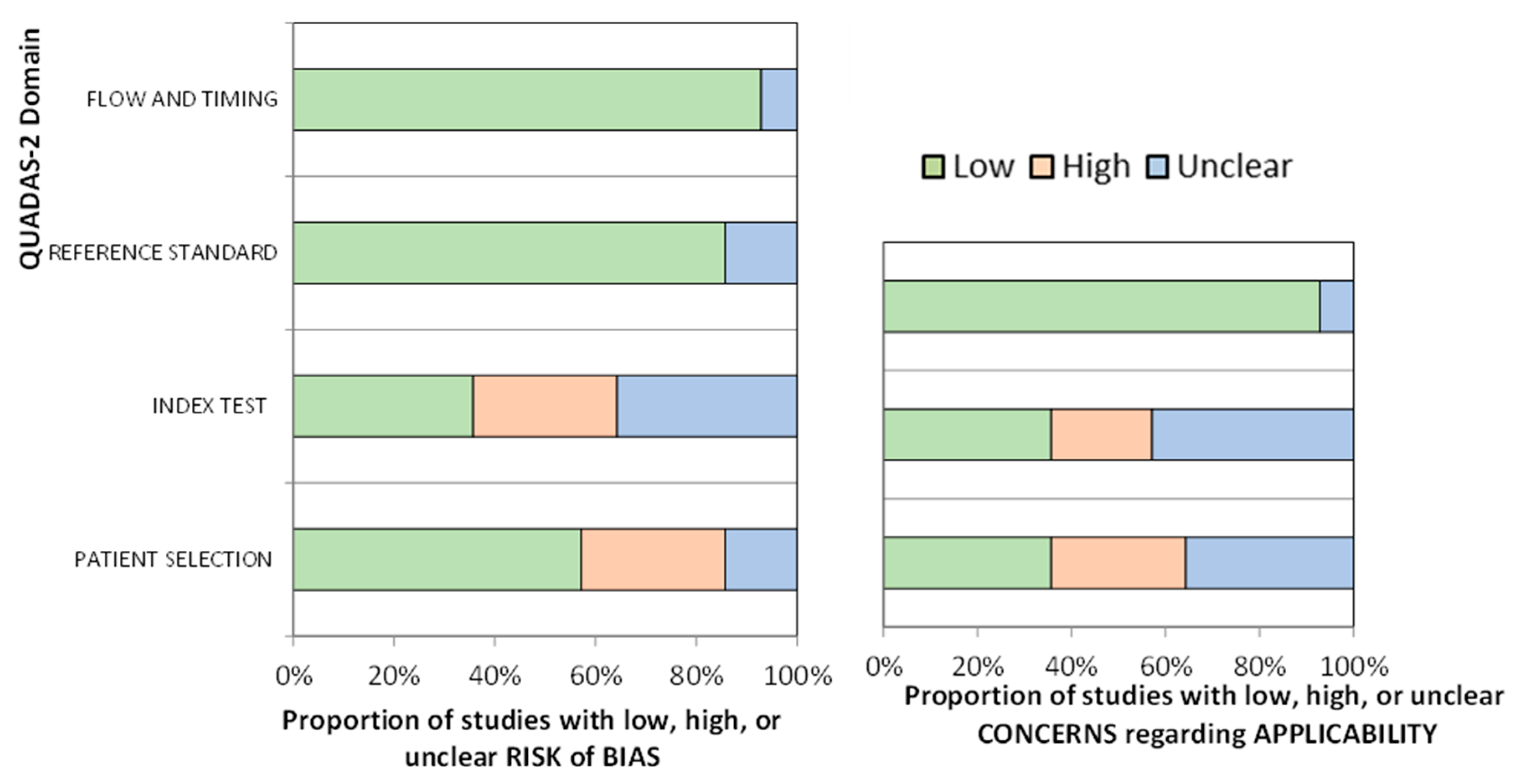
2.4. Assessment of Risk of Bias in the Selected Studies
3. Results
3.1. Characteristics of Studies

{kind=link}
{kind=link}
| Study | Country | Type of Cancer | Setting | n | Mean Age (SD or Range)/% Men | Prevalence (%) |
| Barahona et al., 2018 [21] | Spain | All, advanced cancer | Hospice and general hospital | 60 | 76 (69–83)/48 | 41.8 |
| De la Cruz et al., 2015 [31] | USA | All, advanced cancer | Home, receiving hospice care | 78 | 69 (49–91)/55 | 44, MDAS 42, Nu–DESC Nurse 24, Nu–DESC Caregiver evening 15, Nu–DESC Caregiver night |
| Detroyer et al., 2014 [22] | Belgium | All, palliative care | PCU and MOW | 48 | 72 (67.25–78)/62.5 | 22.9 |
| Gaudreau et al., 2005 [28] | Canada | All, palliative care | Hemato–oncology/Internal medicine hospital unit | 59 | 61 (15–92)/NA | 35.59 |
| Grandahl et al., 2016 [23] | Danish | All, oncology inpatient | MOW | 81 | 68.5 (7.8)/42 | 33 |
| Grassi et al., 2001 [24] | Italy | All, derived from psychiatrist consultation | PCU and MOW | 105 | 67.7 (13.2)/52.4 | 62.8 |
| Hamamo et al., 2015 [33] | Japan | All, palliative care | PCU and MOW | 2343 | 69.1 (12.8) | 19.9 |
| Kang et al., 2018 [30] | Korea | All, advanced cancer | PCU | 123 | 66.92 (12.09)/42.28 | 23.52 |
| Klankluang et al., 2019 [29] | Thailand | All | PCU | 194 | 63.9 (13.3)/51.5 | 51 (8.1 hyperactive; 38.4 hypoactive; 53.5 mixed) |
| Lawlor et al., 2000 [27] | Canada | All, advanced cancer | PCU | 104 | 64.4 (10)/NA | 68.3 |
| Nefjees et al., 2019 [25] | Netherlands | All, advanced cancer | MOW | 187 | 64 (12)/66.3 | 50.26 |
| Ryan et al., 2009 [26] | Ireland | All, advanced cancer | PCU | 52 | 69.19 (36–93)/46.15 | 29.41 |
| Sancho–Espinosa et al., 2018 [20] | Spain | Patients with solid tumors | MOW | 42 | 60.9 (1.9)/71.4 | 14.3 |
| Sands et al., 2021 [32] | Australia | All | MOW | 73 | 68 (60.5–78)/42 | 38 (14.8 hyperactive; 59.3 hypoactive; 22.2 mixed) |
3.2. Risk of Bias
4. Discussion
4.1. Incidence
4.2. Assessment Tools
4.3. Strengths and Limitations
4.4. Implications for Practice
- Studies should include only older people with oncological disease in order to determine the specific predictive capacity of test(s) in this population and to analyze the results by age group.
- Comorbidities, hospital unit, and type of cancer should be analyzed in addition to possible risk factors derived from cytostatic treatment, radiotherapy, or other healthcare interventions.
- Only validated scales, such as the DOSS, CAM or Nu-DESC, should be used whenever possible, respecting the validated cutoff points.
- Whenever possible, the metric properties of the instrument should be measured in the population analyzed.
- Details of the assessment should be described, including the time when it is performed, the person carrying it out, and their previous training or experience in the use of the instrument.
- Studies should be designed to minimize the risk of bias in order to enable extrapolation of the data to the entire older population with oncological disease.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mattiuzzi, C.; Lippi, G. Worldwide Disease Epidemiology in the Older Persons. Eur. Geriatr. Med. 2020, 11, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Word Health Organization. Mortality Rate in Older People—Top 20 Causes (Global and Regions). Available online: https://platform.who.int/data/maternal-newborn-child-adolescent-ageing/static-visualizations/mca (accessed on 27 June 2022).
- Lawlor, P.G.; Bush, S.H. Delirium in Patients with Cancer: Assessment, Impact, Mechanisms and Management. Nat. Rev. Clin. Oncol. 2015, 12, 77–92. [Google Scholar] [CrossRef] [PubMed]
- Bush, S.H.; Lawlor, P.G.; Ryan, K.; Centeno, C.; Lucchesi, M.; Kanji, S.; Siddiqi, N.; Morandi, A.; Davis, D.H.J.; Laurent, M.; et al. Delirium in Adult Cancer Patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv143–iv165. [Google Scholar] [CrossRef] [PubMed]
- Nolan, C.; DeAngelis, L.M. The Confused Oncologic Patient: A Rational Clinical Approach. Curr. Opin. Neurol. 2016, 29, 789–796. [Google Scholar] [CrossRef]
- Meehan, A.M.; Kassab, L.; Qin, H. Cancer and Older Adult Patient Care. Hosp. Pract. 2020, 48, 17–25. [Google Scholar] [CrossRef]
- Oh, E.S.; Fong, T.G.; Hshieh, T.T.; Inouye, S.K. Delirium in Older Persons: Advances in Diagnosis and Treatment. JAMA 2017, 318, 1161–1174. [Google Scholar] [CrossRef]
- Sands, M.B.; Wee, I.; Agar, M.; Vardy, J.L. The Detection of Delirium in Admitted Oncology Patients: A Scoping Review. Eur. Geriatr. Med. 2022, 13, 33–51. [Google Scholar] [CrossRef]
- Boettger, S.; Zipser, C.M.; Bode, L.; Spiller, T.; Deuel, J.; Osterhoff, G.; Ernst, J.; Petry, H.; Volbracht, J.; von Känel, R. The Prevalence Rates and Adversities of Delirium: Too Common and Disadvantageous. Palliat. Support. Care 2021, 19, 161–169. [Google Scholar] [CrossRef]
- Carter, M.J. Diagnostic and Statistical Manual of Mental Disorders; Sagamore Publishing LLC: Urbana, IL, USA, 2014; Volume 48, pp. 275–277. [Google Scholar]
- Network for Investigation of Delirium: Unifying Scientists (NIDUS). 2018. Delirium Measurement Info Cards. Available online: https://deliriumnetwork.org/measurement/delirium-info-cards/ (accessed on 9 April 2023).
- Pérez-Ros, P.; Martínez-Arnau, F.M. Delirium Assessment in Older People in Emergency Departments. A Literature Review. Diseases 2019, 7, 14. [Google Scholar] [CrossRef]
- Bellelli, G.; Morandi, A.; Davis, D.H.J.; Mazzola, P.; Turco, R.; Gentile, S.; Ryan, T.; Cash, H.; Guerini, F.; Torpilliesi, T.; et al. Validation of the 4AT, a New Instrument for Rapid Delirium Screening: A Study in 234 Hospitalised Older People. Age Ageing 2014, 43, 496–502. [Google Scholar] [CrossRef]
- O’Sullivan, R.; Meagher, D.; Leonard, M.; Watne, L.O.; Hall, R.J.; Maclullich, A.M.J.; Trzepacz, P.; Adamis, D. A Comparison of the Revised Delirium Rating Scale (DRS-R98) and the Memorial Delirium Assessment Scale (MDAS) in a Palliative Care Cohort with DSM-IV Delirium. Palliat. Support. Care 2015, 13, 937–944. [Google Scholar] [CrossRef]
- Van Velthuijsen, E.L.; Zwakhalen, S.M.G.; Warnier, R.M.J.; Mulder, W.J.; Verhey, F.R.J.; Kempen, G.I.J.M. Psychometric Properties and Feasibility of Instruments for the Detection of Delirium in Older Hospitalized Patients: A Systematic Review. Int. J. Geriatr. Psychiatry 2016, 31, 974–989. [Google Scholar] [CrossRef]
- Bramati, P.; Bruera, E. Delirium in Palliative Care. Cancers 2021, 13, 5893. [Google Scholar] [CrossRef]
- Watt, C.L.; Scott, M.; Webber, C.; Sikora, L.; Bush, S.H.; Kabir, M.; Boland, J.W.; Woodhouse, R.; Sands, M.B.; Lawlor, P.G. Delirium Screening Tools Validated in the Context of Palliative Care: A Systematic Review. Palliat. Med. 2021, 35, 683–696. [Google Scholar] [CrossRef]
- Yang, E.J.; Hahm, B.-J.; Shim, E.-J. Screening and Assessment Tools for Measuring Delirium in Patients with Cancer in Hospice and Palliative Care: A Systematic Review. J. Hosp. Palliat. Care 2021, 24, 214–225. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Sancho-Espinosa, I.; Calvo-Espinós, C.; Arasanz Esteban, H.; Lacalle Emboroujo, A.; de Gaona Lana, E. Value of a Single-Question Screening Tool for Delirium Screening by a Nurse Team in Cancer Patients at an Oncology Service. Med. Paliativa 2018, 25, 214–221. [Google Scholar] [CrossRef]
- Barahona, E.; Pinhao, R.; Galindo, V.; Noguera, A. The Diagnostic Sensitivity of the Memorial Delirium Assessment Scale-Spanish Version. J. Pain Symptom Manag. 2018, 55, 968–972. [Google Scholar] [CrossRef]
- Detroyer, E.; Clement, P.M.; Baeten, N.; Pennemans, M.; Decruyenaere, M.; Vandenberghe, J.; Menten, J.; Joosten, E.; Milisen, K. Detection of Delirium in Palliative Care Unit Patients: A Prospective Descriptive Study of the Delirium Observation Screening Scale Administered by Bedside Nurses. Palliat. Med. 2014, 28, 79–86. [Google Scholar] [CrossRef]
- Grandahl, M.G.; Nielsen, S.E.; Koerner, E.A.; Schultz, H.H.; Arnfred, S.M. Prevalence of Delirium among Patients at a Cancer Ward: Clinical Risk Factors and Prediction by Bedside Cognitive Tests. Nord. J. Psychiatry 2016, 70, 413–417. [Google Scholar] [CrossRef]
- Grassi, L.; Caraceni, A.; Beltrami, E.; Borreani, C.; Zamorani, M.; Maltoni, M.; Monti, M.; Luzzani, M.; Mercadante, S.; De Conno, F. Assessing Delirium in Cancer Patients: The Italian Versions of the Delirium Rating Scale and the Memorial Delirium Assessment Scale. J. Pain Symptom Manag. 2001, 21, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Neefjes, E.C.W.; Van Der Vorst, M.J.D.L.; Boddaert, M.S.A.; Verdegaal, B.A.T.T.; Beeker, A.; Teunissen, S.C.C.; Beekman, A.T.F.; Zuurmond, W.W.A.; Berkhof, J.; Verheul, H.M.W. Accuracy of the Delirium Observational Screening Scale (DOS) as a Screening Tool for Delirium in Patients with Advanced Cancer. BMC Cancer 2019, 19, 160. [Google Scholar] [CrossRef] [PubMed]
- Ryan, K.; Leonard, M.; Guerin, S.; Donnelly, S.; Conroy, M.; Meagher, D. Validation of the Confusion Assessment Method in the Palliative Care Setting. Palliat. Med. 2009, 23, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, P.G.; Nekolaichuk, C.; Gagnon, B.; Mancini, I.L.; Pereira, J.L.; Bruera, E.D. Clinical Utility, Factor Analysis, and Further Validation of the Memorial Delirium Assessment Scale in Patients with Advanced Cancer: Assessing Delirium in Advanced Cancer. Cancer 2000, 88, 2859–2867. [Google Scholar] [CrossRef] [PubMed]
- Gaudreau, J.-D.; Gagnon, P.; Harel, F.; Tremblay, A.; Roy, M.-A. Fast, Systematic, and Continuous Delirium Assessment in Hospitalized Patients: The Nursing Delirium Screening Scale. J. Pain Symptom Manag. 2005, 29, 368–375. [Google Scholar] [CrossRef]
- Klankluang, W.; Pukrittayakamee, P.; Atsariyasing, W.; Siriussawakul, A.; Chanthong, P.; Tongsai, S.; Tayjasanant, S. Validity and Reliability of the Memorial Delirium Assessment Scale-Thai Version (MDAS-T) for Assessment of Delirium in Palliative Care Patients. Oncologist 2020, 25, e335–e340. [Google Scholar] [CrossRef]
- Kang, B.; Kim, Y.J.; Suh, S.W.; Son, K.-L.; Ahn, G.S.; Park, H.Y. Delirium and Its Consequences in the Specialized Palliative Care Unit: Validation of the Korean Version of Memorial Delirium Assessment Scale. Psycho-Oncology 2019, 28, 160–166. [Google Scholar] [CrossRef]
- De la Cruz, M.; Noguera, A.; San Miguel-Arregui, M.T.; Williams, J.; Chisholm, G.; Bruera, E. Delirium, Agitation, and Symptom Distress within the Final Seven Days of Life among Cancer Patients Receiving Hospice Care. Palliat. Support. Care 2015, 13, 211–216. [Google Scholar] [CrossRef]
- Sands, M.B.; Sharma, S.; Carpenter, L.; Hartshorn, A.; Lee, J.T.; Lujic, S.; Congdon, M.E.; Buchanan, A.M.; Agar, M.; Vardy, J.L. “SQiD, the Single Question in Delirium; Can a Single Question Help Clinicians to Detect Delirium in Hospitalised Cancer Patients?” Running Heading Single Question in Delirium” (Bcan-D-20-01665). BMC Cancer 2021, 21, 75. [Google Scholar] [CrossRef]
- Hamano, J.; Morita, T.; Ozawa, T.; Shishido, H.; Kawahara, M.; Aoki, S.; Demizu, A.; Goshima, M.; Goto, K.; Gyoda, Y.; et al. Validation of the Simplified Palliative Prognostic Index Using a Single Item from the Communication Capacity Scale. J. Pain Symptom Manag. 2015, 50, 542–547.e4. [Google Scholar] [CrossRef]
- León-Salas, B.; Trujillo-Martín, M.M.; Martínez del Castillo, L.P.; García-García, J.; Pérez-Ros, P.; Rivas-Ruiz, F.; Serrano-Aguilar, P. Multicomponent Interventions for the Prevention of Delirium in Hospitalized Older People: A Meta-Analysis. J. Am. Geriatr. Soc. 2020, 68, 2947–2954. [Google Scholar] [CrossRef]
- Breitbart, W.; Rosenfeld, B.; Roth, A.; Smith, M.J.; Cohen, K.; Passik, S. The Memorial Delirium Assessment Scale. J. Pain Symptom Manag. 1997, 13, 128–137. [Google Scholar] [CrossRef]
- Gélinas, C.; Bérubé, M.; Chevrier, A.; Pun, B.T.; Ely, E.W.; Skrobik, Y.; Barr, J. Delirium Assessment Tools for Use in Critically Ill Adults: A Psychometric Analysis and Systematic Review. Crit. Care Nurse 2018, 38, 38–49. [Google Scholar] [CrossRef]
- Gnatta, J.R.; Cavassana, T.M.; Nascimento, A.S.d.; Poveda, V.d.B. Instruments to Identify Delirium in Patients Recovering from Anesthesia: A Scoping Review. J. Perianesth. Nurs. 2022, 37, 961–965.e7. [Google Scholar] [CrossRef]
- Inouye, S.K.; van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying Confusion: The Confusion Assessment Method. A New Method for Detection of Delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Trzepacz, P.T.; Mittal, D.; Torres, R.; Kanary, K.; Norton, J.; Jimerson, N. Validation of the Delirium Rating Scale-Revised-98: Comparison with the Delirium Rating Scale and the Cognitive Test for Delirium. J. Neuropsychiatry Clin. Neurosci. 2001, 13, 229–242. [Google Scholar] [CrossRef]
- Sands, M.B.; Dantoc, B.P.; Hartshorn, A.; Ryan, C.J.; Lujic, S. Single Question in Delirium (SQiD): Testing Its Efficacy against Psychiatrist Interview, the Confusion Assessment Method and the Memorial Delirium Assessment Scale. Palliat. Med. 2010, 24, 561–565. [Google Scholar] [CrossRef]


| Study Characteristics | Validity | Reliability | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | AUC (95% CI) | Accuracy % (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|
| Barahona et al., 2018 [21] | |||||||||
| Diagnostic instrument/cutoff | MDAS–S/ ≥ 7 | NA | NA | 92.9 | 71.8 | 70.2 | 93.3 | 0.93 | NA |
| Assessor | Physicians | ||||||||
| Gold standard | CAM | ||||||||
| Assessor | Physicians | ||||||||
| De la Cruz et al., 2015 [31] | |||||||||
| Diagnostic instrument/cutoff | Nu–DESC/ ≥ 2 | NA | NA | NA | NA | ||||
| Assessor | Nurse | 63 | 67 | 61 | 68 | ||||
| Caregiver evening | 35 | 80 | 58 | 61 | |||||
| Caregiver night | 21 | 85 | 50 | 59 | |||||
| Gold standard | MDAS | ||||||||
| Assessor | Trained nurse | ||||||||
| Detroyer et al., 2014 [22] | |||||||||
| Diagnostic instrument/cutoff | DOSS/ ≥ 3 | DOSS α = 0.772 DOSS and DI ρ = 0.53 | NA | 81.8 (52–95) | 96.1 (90–98) | 69.2 (42–87) | 98 (93–99) | 0.93 (0.82–1) | 94.7 (89–98) |
| Assessor | Nurses | ||||||||
| Gold standard | CAM/DI | ||||||||
| Assessor | Nurses/researchers | ||||||||
| Gaudreau et al., 2005 [28] | K = 0.89 (0.75–1) a | ||||||||
| Diagnostic instrument/cutoffs | NuDESC/ > 1 | NA | 85.7 (65.4–95) | 86.8 (72.7–94.3) | NA | NA | 0.90 | NA | |
| CRS/ > 0 | 76.2 (54.9–89.4) | 81.6 (66.6–90.8) | 0.83 | ||||||
| CRS/ > 1 | 47.6 (28.3–67.6) | 97.4 (86.5–99.5) | |||||||
| DSM–IV/ > 0 | 90.5 (71.1–97.4) | 100 (90.8–100) | 0.95 | ||||||
| MDAS/ ≥ 7 | 95.2 (77.3–95.8) | 89.5 (75.9–99.2) | 0.97 | ||||||
| Assessor | Nurses | ||||||||
| Gold standard | CAM | ||||||||
| Assessor | Nurses and a Psychiatrist | ||||||||
| Grandahl et al., 2016 [23] | |||||||||
| Diagnostic instrument/cutoff | CDT/ = 1 b | NA | NA | 81 | 46 | NA | NA | NA | NA |
| MiniCog/ < 3 | 67 | 85 | |||||||
| DST/ ≤ 6 | 85 | 60 | |||||||
| MiniCog and DST | 93 | 60 | |||||||
| CDT and DST | 82 | 67 | |||||||
| Assessor | Nurses and physicians | ||||||||
| Gold standard | CAM | ||||||||
| Assessor | Psychiatrist | ||||||||
| Grassi et al., 2001 [24] | |||||||||
| Diagnostic instrument/cutoff | DRS–I/ ≥ 10; ≥12 | DRS α = 0.7 | ρ = 0.76 c, DRS & MDAS ρ = 0.88, MMSE & MDAS ρ = 0.67, MMSE & DRS | 95; 81 | 61; 76 | 80; 85 | 89; 70 | NA | NA |
| MDAS–I/ ≥ 13 | α = 0.89 | 68 | 94 | 95 | 63 | ||||
| MMSE < 24 | 96 | 38 | 88 | 72 | |||||
| Assessor | Psychologist | ||||||||
| Gold standard | DSM–III | ||||||||
| Assessor | Neurologist or psychiatrist | ||||||||
| Hamano et al., 2015 [33] | |||||||||
| Diagnostic instrument/cutoff | CCS 0/123 | NA | NA | 93.2 (90.6–95.1) | 70.5 (69.9–71.0) | 43.9 (42.7–44.8) | 97.7 (96.8–98.3) | NA | 75.0 (74.0–75.7) |
| CCS 01/23 | 76.7 (73.4–79.7) | 89.3 (88.5–90.0) | 64.0 (61.–66.5) | 93.9 (93.1–94.7) | 86.8 (85.5–88.0) | ||||
| Assessor | Physician | ||||||||
| Gold standard | DSM–IV | ||||||||
| Assessor | Physician | ||||||||
| Kang et al., 2018 [30] | |||||||||
| Diagnostic instrument/cutoff | MDAS–K/ ≥ 9 | α = 0.942 | MDAS–K and DRS r = 0.95; ICC = 0.98 | 95.8 | 92.1 | 79.3 | 98.6 | 0.98 (0.96–1.00) | NA |
| Assessor | Palliative care staff | ||||||||
| Gold standard | CAM and DSM–IV | ||||||||
| Assessor | Psychiatrist | ||||||||
| Klankluang et al., 2019 [29] | |||||||||
| Diagnostic instrument/cutoff | MDAS–T/ ≥ 9 | α = 0.96 Content validity = 0.97 Content item validity from 0.67 to 1 | ICC 0.98 (0.96–0.99) | 92 (85–96) | 90 (82–94) | 90 | 91 | 0.91 (0.86–0.94) | Mild 42.6 Moderate 44.8 Severe 78.9 Profound 92.6 |
| Assessor | Clinical psychologist | ||||||||
| Gold standard | CAM–ICU–T/DSM–V | ||||||||
| Assessor | Research assistant/psychiatrist | ||||||||
| Lawlor et al., 2000 [27] | |||||||||
| Diagnostic instrument/cutoff | MDAS/ ≥ 7 d | NA | ICC from 0.69 to 1 | 97 | 95 | NA | NA | NA | NA |
| Assessor | Physician resident Medical staff Family interviewers | ||||||||
| Gold standard | DSM–IV | ||||||||
| Assessor | Physician resident | ||||||||
| Nefjees et al., 2019 [25] | |||||||||
| Diagnostic instrument/cutoff | DOSS/ ≥ 3 | NA | NA | >99.9 (95.8–100) | 99.5 (95.5–99.9) | 94.6 (88–97.7) | >99.9 (96.1–100) | NA | NA |
| Assessor | Bedside nurses | ||||||||
| Gold standard | DRS–R–98 | ||||||||
| Assessor | Trained independent assessor | ||||||||
| Ryan et al., 2009 [26] | |||||||||
| Diagnostic instrument/cutoff | CAM/(1 and 2) and (3 or 4) | NA | NA | 96 (78–100) | 93 (77–99) | NA | NA | NA | NA |
| Assessor | NCHDs | ||||||||
| Gold standard | DSM–IV | ||||||||
| Assessor | Psychiatrist | ||||||||
| Sancho–Espinosa et al., 2018 [20] | |||||||||
| Diagnostic instrument/cutoff | Spanish SQiD/yes | Accordance of 95.2%; K = 0.88 | NA | 83.4 (43.6–97) | 83.4 (68.1–92.1) | 45.5 (21.3–72) | 96.8 (83.8–99.4) | NA | 83.4 (69.4–91.7) |
| Assessor | Nurse | ||||||||
| Gold standard | CAM and DSM–IV | ||||||||
| Assessor | Consultor team | ||||||||
| Sands et al., 2021 [32] | |||||||||
| Diagnostic instrument/cutoff | SQiD/yes | K = 0.34 (0.01–0.56), SQID vs. DSM | NA | 44.4 (25.2–64.7) | 87 (73.7–95.1), | 66.7 (45.9–82.5) | 72.7(65.1–79.2) | NA | NA |
| CAM | K = 0.32 (0.11–0.52), CAM vs. DSM | 26.1 (10.2–48.4) | 100 (92–100) | 100 (100) | 72.1 (67–76.7) | ||||
| Assessor | Clinical staff | ||||||||
| Gold standard | Psychiatrist interview | ||||||||
| Assessor | |||||||||
| Study | Risk of Bias | Applicability Concerns | ||||||
|---|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | Overall Risk of Bias | |
| Barahona et al., 2018 [21] | ☺ | ☺ | ☺ | ☺ | ? | ☺ | ☺ | Acceptable |
| De la Cruz et al., 2015 [31] | ☺ | ☺ | ☺ | ☺ | ? | ☺ | ☺ | Acceptable |
| Detroyer et al., 2014 [22] | ☺ | ☺ | ☺ | ☺ | ? | ☺ | ☺ | Acceptable |
| Gaudreau et al., 2005 [28] | ☺ | ? | ☺ | ☺ | ☺ | ? | ☺ | Acceptable |
| Grandahl et al., 2016 [23] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Excellent |
| Grassi et al., 2001 [24] | ☹ | ? | ☺ | ☺ | ☹ | ? | ☺ | Unsatisfactory |
| Humamo et al., 2015 [33] | ☺ | ☹ | ☺ | ? | ☺ | ? | ☺ | Unsatisfactory |
| Kang et al., 2018 [30] | ? | ☺ | ☺ | ☺ | ? | ☺ | ☺ | Acceptable |
| Klankluang et al., 2019 [29] | ☹ | ? | ☺ | ☺ | ☹ | ? | ☺ | Unsatisfactory |
| Lawlor et al., 2000 [27] | ☺ | ☹ | ☹ | ☹ | ☺ | ? | ? | Unsatisfactory |
| Nefjees et al., 2019 [25] | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | ☺ | Excellent |
| Ryan et al., 2009 [26] | ☹ | ? | ? | ☺ | ☹ | ? | ? | Unsatisfactory |
| Sancho-Espinosa et al., 2018 [20] | ☹ | ? | ☺ | ☺ | ☹ | ? | ☺ | Unsatisfactory |
| Sands et al., 2021 [32] | ☺ | ? | ☺ | ☺ | ☺ | ? | ☺ | Acceptable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Arnau, F.M.; Puchades-García, A.; Pérez-Ros, P. Accuracy of Delirium Screening Tools in Older People with Cancer—A Systematic Review. Cancers 2023, 15, 2807. https://doi.org/10.3390/cancers15102807
Martínez-Arnau FM, Puchades-García A, Pérez-Ros P. Accuracy of Delirium Screening Tools in Older People with Cancer—A Systematic Review. Cancers. 2023; 15(10):2807. https://doi.org/10.3390/cancers15102807
Chicago/Turabian StyleMartínez-Arnau, Francisco Miguel, Andrea Puchades-García, and Pilar Pérez-Ros. 2023. "Accuracy of Delirium Screening Tools in Older People with Cancer—A Systematic Review" Cancers 15, no. 10: 2807. https://doi.org/10.3390/cancers15102807
APA StyleMartínez-Arnau, F. M., Puchades-García, A., & Pérez-Ros, P. (2023). Accuracy of Delirium Screening Tools in Older People with Cancer—A Systematic Review. Cancers, 15(10), 2807. https://doi.org/10.3390/cancers15102807