
Factors Predictive of Primary Resistance to Immune Checkpoint Inhibitors in Patients with Advanced Non-Small Cell Lung Cancer
 , ,
, ,  , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methodology
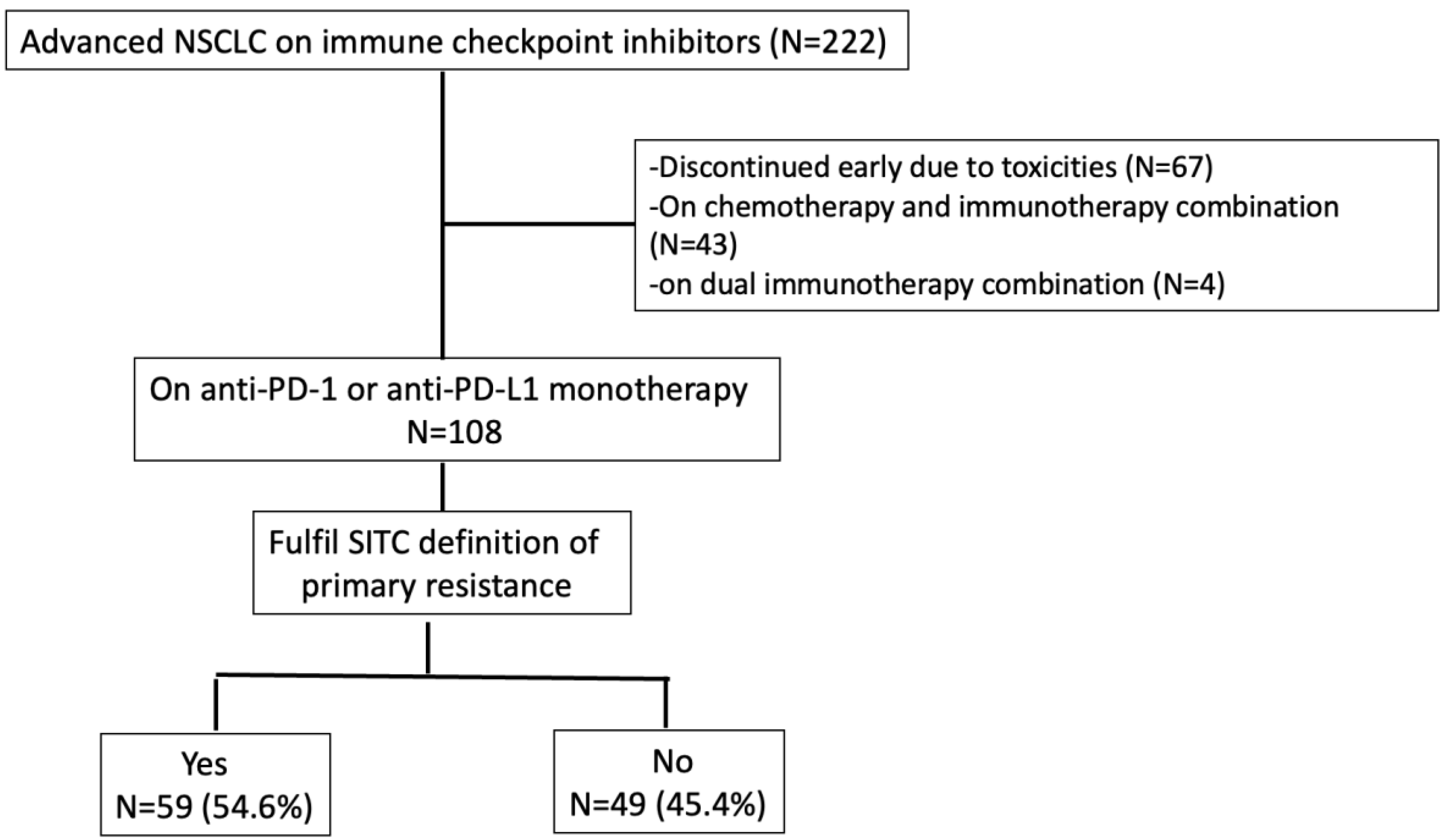
2.1. Study Design and Participants
2.2. Data Collection
2.3. Outcomes
2.4. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.; Kilickap, S.; Gümüş, M.; Bondarenko, I.; Özgüroğlu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab Monotherapy for First-Line Treatment of Advanced Non-Small-Cell Lung Cancer with PD-L1 of at Least 50%: A Multicentre, Open-Label, Global, Phase 3, Randomised, Controlled Trial. Lancet 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Health-Related Quality-of-Life Results for Pembrolizumab versus Chemotherapy in Advanced, PD-L1-Positive NSCLC (KEYNOTE-024): A Multicentre, International, Randomised, Open-Label Phase 3 Trial. Lancet Oncol. 2017, 18, 1600–1609. [Google Scholar] [CrossRef]
- Mok, T.S.K.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus Chemotherapy for Previously Untreated, PD-L1-Expressing, Locally Advanced or Metastatic Non-Small-Cell Lung Cancer (KEYNOTE-042): A Randomised, Open-Label, Controlled, Phase 3 Trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Carbone, D.P.; Reck, M.; Paz-Ares, L.; Creelan, B.; Horn, L.; Steins, M.; Felip, E.; van den Heuvel, M.M.; Ciuleanu, T.-E.; Badin, F.; et al. First-Line Nivolumab in Stage IV or Recurrent Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 376, 2415–2426. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.-G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in Combination with Carboplatin plus Nab-Paclitaxel Chemotherapy Compared with Chemotherapy Alone as First-Line Treatment for Metastatic Non-Squamous Non-Small-Cell Lung Cancer (IMpower130): A Multicentre, Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef] [PubMed]
- Walsh, R.J.; Soo, R.A. Resistance to Immune Checkpoint Inhibitors in Non-Small Cell Lung Cancer: Biomarkers and Therapeutic Strategies. Ther. Adv. Med. Oncol. 2020, 12, 1758835920937902. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus Docetaxel in Patients with Previously Treated Non-Small-Cell Lung Cancer (OAK): A Phase 3, Open-Label, Multicentre Randomised Controlled Trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus Docetaxel for Previously Treated, PD-L1-Positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010): A Randomised Controlled Trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Shah, S.; Wood, K.; Labadie, B.; Won, B.; Brisson, R.; Karrison, T.; Hensing, T.; Kozloff, M.; Bao, R.; Patel, J.D.; et al. Clinical and Molecular Features of Innate and Acquired Resistance to Anti-PD-1/PD-L1 Therapy in Lung Cancer. Oncotarget 2018, 9, 4375–4384. [Google Scholar] [CrossRef]
- Jenkins, R.W.; Barbie, D.A.; Flaherty, K.T. Mechanisms of Resistance to Immune Checkpoint Inhibitors. Br. J. Cancer 2018, 118, 9–16. [Google Scholar] [CrossRef]
- Kluger, H.M.; Tawbi, H.A.; Ascierto, M.L.; Bowden, M.; Callahan, M.K.; Cha, E.; Chen, H.X.; Drake, C.G.; Feltquate, D.M.; Ferris, R.L.; et al. Defining Tumor Resistance to PD-1 Pathway Blockade: Recommendations from the First Meeting of the SITC Immunotherapy Resistance Taskforce. J. Immunother. Cancer 2020, 8, e000398. [Google Scholar] [CrossRef]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef]
- Wang, F.; Wang, S.; Zhou, Q. The Resistance Mechanisms of Lung Cancer Immunotherapy. Front. Oncol. 2020, 10, 568059. [Google Scholar] [CrossRef]
- Pavan, A.; Calvetti, L.; Dal Maso, A.; Attili, I.; Del Bianco, P.; Pasello, G.; Guarneri, V.; Aprile, G.; Conte, P.; Bonanno, L. Peripheral Blood Markers Identify Risk of Immune-Related Toxicity in Advanced Non-Small Cell Lung Cancer Treated with Immune-Checkpoint Inhibitors. Oncologist 2019, 24, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. IRECIST: Guidelines for Response Criteria for Use in Trials Testing Immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152. [Google Scholar] [CrossRef] [PubMed]
- Bernichon, E.; Tissot, C.; Bayle-Bleuez, S.; Rivoirard, R.; Bouleftour, W.; Forest, F.; Tinquaut, F.; Mery, B.; Fournel, P. Predictive Resistance Factors in Lung Cancer Patients Treated with Nivolumab. Retrospective Study. Bull. Cancer 2021, 108, 250–265. [Google Scholar] [CrossRef] [PubMed]
- Li, J.J.N.; Karim, K.; Sung, M.; Le, L.W.; Lau, S.C.M.; Sacher, A.; Leighl, N.B. Tobacco Exposure and Immunotherapy Response in PD-L1 Positive Lung Cancer Patients. Lung Cancer 2020, 150, 159–163. [Google Scholar] [CrossRef]
- Chiu, M.; Lipka, M.B.; Bhateja, P.; Fu, P.; Dowlati, A. A Detailed Smoking History and Determination of MYC Status Predict Response to Checkpoint Inhibitors in Advanced Non-Small Cell Lung Cancer. Transl. Lung Cancer Res. 2020, 9, 55–60. [Google Scholar] [CrossRef]
- Dimitrakopoulos, F.-I.; Nikolakopoulos, A.; Kottorou, A.; Kalofonou, F.; Liolis, E.; Frantzi, T.; Pyrousis, I.; Koutras, A.; Makatsoris, T.; Kalofonos, H. PIOS (Patras Immunotherapy Score) Score Is Associated with Best Overall Response, Progression-Free Survival, and Post-Immunotherapy Overall Survival in Patients with Advanced Non-Small-Cell Lung Cancer (NSCLC) Treated with Anti-Program Cell Death-1 (PD-1) Inhibitors. Cancers 2020, 12, 1257. [Google Scholar] [CrossRef]
- Wu, Y.; Ju, Q.; Jia, K.; Yu, J.; Shi, H.; Wu, H.; Jiang, M. Correlation between Sex and Efficacy of Immune Checkpoint Inhibitors (PD-1 and CTLA-4 Inhibitors). Int. J. Cancer 2018, 143, 45–51. [Google Scholar] [CrossRef]
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer Immunotherapy Efficacy and Patients’ Sex: A Systematic Review and Meta-Analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef]
- Grassadonia, A.; Sperduti, I.; Vici, P.; Iezzi, L.; Brocco, D.; Gamucci, T.; Pizzuti, L.; Maugeri-Saccà, M.; Marchetti, P.; Cognetti, G.; et al. Effect of Gender on the Outcome of Patients Receiving Immune Checkpoint Inhibitors for Advanced Cancer: A Systematic Review and Meta-Analysis of Phase III Randomized Clinical Trials. J. Clin. Med. 2018, 7, 542. [Google Scholar] [CrossRef]
- Conforti, F.; Pala, L.; Pagan, E.; Corti, C.; Bagnardi, V.; Queirolo, P.; Catania, C.; De Pas, T.; Giaccone, G. Sex-Based Differences in Response to Anti-PD-1 or PD-L1 Treatment in Patients with Non-Small-Cell Lung Cancer Expressing High PD-L1 Levels. A Systematic Review and Meta-Analysis of Randomized Clinical Trials. ESMO Open 2021, 6, 100251. [Google Scholar] [CrossRef] [PubMed]
- Madala, S.; Rasul, R.; Singla, K.; Sison, C.P.; Seetharamu, N.; Castellanos, M.R. Gender Differences and Their Effects on Survival Outcomes in Lung Cancer Patients Treated With PD-1/PD-L1 Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Clin. Oncol. 2022, 34, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Bagnardi, V.; Viale, G.; De Pas, T.; Pagan, E.; Pennacchioli, E.; Cocorocchio, E.; Ferrucci, P.F.; De Marinis, F.; et al. Sex-Based Heterogeneity in Response to Lung Cancer Immunotherapy: A Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2019, 111, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex Differences in Immune Responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Dinesh, R.K.; Hahn, B.H.; Singh, R.P. PD-1, Gender, and Autoimmunity. Autoimmun. Rev. 2010, 9, 583–587. [Google Scholar] [CrossRef]
- Polanczyk, M.J.; Hopke, C.; Vandenbark, A.A.; Offner, H. Estrogen-Mediated Immunomodulation Involves Reduced Activation of Effector T Cells, Potentiation of Treg Cells, and Enhanced Expression of the PD-1 Costimulatory Pathway. J. Neurosci. Res. 2006, 84, 370–378. [Google Scholar] [CrossRef]
- Markle, J.G.M.; Frank, D.N.; Mortin-Toth, S.; Robertson, C.E.; Feazel, L.M.; Rolle-Kampczyk, U.; von Bergen, M.; McCoy, K.D.; Macpherson, A.J.; Danska, J.S. Sex Differences in the Gut Microbiome Drive Hormone-Dependent Regulation of Autoimmunity. Science 2013, 339, 1084–1088. [Google Scholar] [CrossRef]
- Fish, E.N. The X-Files in Immunity: Sex-Based Differences Predispose Immune Responses. Nat. Rev. Immunol. 2008, 8, 737–744. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Fouad, Y.A.; Aanei, C. Revisiting the Hallmarks of Cancer. Am. J. Cancer Res. 2017, 7, 1016–1036. [Google Scholar]
- Gibney, G.T.; Weiner, L.M.; Atkins, M.B. Predictive Biomarkers for Checkpoint Inhibitor-Based Immunotherapy. Lancet Oncol. 2016, 17, e542–e551. [Google Scholar] [CrossRef] [PubMed]
- Granot, Z.; Jablonska, J. Distinct Functions of Neutrophil in Cancer and Its Regulation. Mediators Inflamm. 2015, 2015, 701067. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Wang, Y.; Liu, F.; Qiu, X.; Zhang, X.; Fang, C.; Qian, X.; Li, Y. Peripheral Blood Markers Predictive of Outcome and Immune-Related Adverse Events in Advanced Non-Small Cell Lung Cancer Treated with PD-1 Inhibitors. Cancer Immunol. Immunother. 2020, 69, 1813–1822. [Google Scholar] [CrossRef] [PubMed]
- Diem, S.; Schmid, S.; Krapf, M.; Flatz, L.; Born, D.; Jochum, W.; Templeton, A.J.; Früh, M. Neutrophil-to-Lymphocyte Ratio (NLR) and Platelet-to-Lymphocyte Ratio (PLR) as Prognostic Markers in Patients with Non-Small Cell Lung Cancer (NSCLC) Treated with Nivolumab. Lung Cancer 2017, 111, 176–181. [Google Scholar] [CrossRef]
- Lee, P.Y.; Oen, K.Q.X.; Lim, G.R.S.; Hartono, J.L.; Muthiah, M.; Huang, D.Q.; Teo, F.S.W.; Li, A.Y.; Mak, A.; Chandran, N.S.; et al. Neutrophil-to-Lymphocyte Ratio Predicts Development of Immune-Related Adverse Events and Outcomes from Immune Checkpoint Blockade: A Case-Control Study. Cancers 2021, 13, 1308. [Google Scholar] [CrossRef]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the Lung Immune Prognostic Index With Immune Checkpoint Inhibitor Outcomes in Patients With Advanced Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef]
- Zhang, N.; Jiang, J.; Tang, S.; Sun, G. Predictive Value of Neutrophil-Lymphocyte Ratio and Platelet-Lymphocyte Ratio in Non-Small Cell Lung Cancer Patients Treated with Immune Checkpoint Inhibitors: A Meta-Analysis. Int. Immunopharmacol. 2020, 85, 106677. [Google Scholar] [CrossRef]
- Suh, K.J.; Kim, S.H.; Kim, Y.J.; Kim, M.; Keam, B.; Kim, T.M.; Kim, D.-W.; Heo, D.S.; Lee, J.S. Post-Treatment Neutrophil-to-Lymphocyte Ratio at Week 6 Is Prognostic in Patients with Advanced Non-Small Cell Lung Cancers Treated with Anti-PD-1 Antibody. Cancer Immunol. Immunother. 2018, 67, 459–470. [Google Scholar] [CrossRef]
- Xiong, Q.; Huang, Z.; Xin, L.; Qin, B.; Zhao, X.; Zhang, J.; Shi, W.; Yang, B.; Zhang, G.; Hu, Y. Post-Treatment Neutrophil-to-Lymphocyte Ratio (NLR) Predicts Response to Anti-PD-1/PD-L1 Antibody in SCLC Patients at Early Phase. Cancer Immunol. Immunother. 2021, 70, 713–720. [Google Scholar] [CrossRef]
- Ho, W.J.; Yarchoan, M.; Hopkins, A.; Mehra, R.; Grossman, S.; Kang, H. Association between Pretreatment Lymphocyte Count and Response to PD1 Inhibitors in Head and Neck Squamous Cell Carcinomas. J. Immunother. Cancer 2018, 6, 84. [Google Scholar] [CrossRef]
- Syn, N.L.; Teng, M.W.L.; Mok, T.S.K.; Soo, R.A. De-Novo and Acquired Resistance to Immune Checkpoint Targeting. Lancet Oncol. 2017, 18, e731–e741. [Google Scholar] [CrossRef] [PubMed]
- Riaz, N.; Morris, L.; Havel, J.J.; Makarov, V.; Desrichard, A.; Chan, T.A. The Role of Neoantigens in Response to Immune Checkpoint Blockade. Int. Immunol. 2016, 28, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in Cancer Immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Spranger, S.; Bao, R.; Gajewski, T.F. Melanoma-Intrinsic β-Catenin Signalling Prevents Anti-Tumour Immunity. Nature 2015, 523, 231–235. [Google Scholar] [CrossRef]
- Peng, W.; Chen, J.Q.; Liu, C.; Malu, S.; Creasy, C.; Tetzlaff, M.T.; Xu, C.; McKenzie, J.A.; Zhang, C.; Liang, X.; et al. Loss of PTEN Promotes Resistance to T Cell-Mediated Immunotherapy. Cancer Discov. 2016, 6, 202–216. [Google Scholar] [CrossRef]
- Oida, T.; Zhang, X.; Goto, M.; Hachimura, S.; Totsuka, M.; Kaminogawa, S.; Weiner, H.L. CD4+CD25- T Cells That Express Latency-Associated Peptide on the Surface Suppress CD4+CD45RBhigh-Induced Colitis by a TGF-Beta-Dependent Mechanism. J. Immunol. 2003, 170, 2516–2522. [Google Scholar] [CrossRef]
- Sakaguchi, S.; Yamaguchi, T.; Nomura, T.; Ono, M. Regulatory T Cells and Immune Tolerance. Cell 2008, 133, 775–787. [Google Scholar] [CrossRef]
- Meyer, C.; Cagnon, L.; Costa-Nunes, C.M.; Baumgaertner, P.; Montandon, N.; Leyvraz, L.; Michielin, O.; Romano, E.; Speiser, D.E. Frequencies of Circulating MDSC Correlate with Clinical Outcome of Melanoma Patients Treated with Ipilimumab. Cancer Immunol. Immunother. 2014, 63, 247–257. [Google Scholar] [CrossRef]
- Chanmee, T.; Ontong, P.; Konno, K.; Itano, N. Tumor-Associated Macrophages as Major Players in the Tumor Microenvironment. Cancers 2014, 6, 1670–1690. [Google Scholar] [CrossRef]
- Hu, W.; Li, X.; Zhang, C.; Yang, Y.; Jiang, J.; Wu, C. Tumor-Associated Macrophages in Cancers. Clin. Transl. Oncol. 2016, 18, 251–258. [Google Scholar] [CrossRef]
- Joyce, J.A.; Fearon, D.T. T Cell Exclusion, Immune Privilege, and the Tumor Microenvironment. Science 2015, 348, 74–80. [Google Scholar] [CrossRef]
- Zhang, H.; Conrad, D.M.; Butler, J.J.; Zhao, C.; Blay, J.; Hoskin, D.W. Adenosine Acts through A2 Receptors to Inhibit IL-2-Induced Tyrosine Phosphorylation of STAT5 in T Lymphocytes: Role of Cyclic Adenosine 3′,5′-Monophosphate and Phosphatases. J. Immunol. 2004, 173, 932–944. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, H.; Cheng, L.; Wang, Y.; Zhang, Y.-K.; Zhao, M.-F.; Liang, G.-D.; Zhang, M.-C.; Li, Y.-G.; Zhao, J.-B.; Gao, Y.-N.; et al. Dysbiosis of the Gut Microbiome in Lung Cancer. Front. Cell. Infect. Microbiol. 2019, 9, 112. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Cheng, Y.; Zang, D.; Zhang, M.; Li, X.; Liu, D.; Gao, B.; Zhou, H.; Sun, J.; Han, X.; et al. The Role of Gut Microbiota in Lung Cancer: From Carcinogenesis to Immunotherapy. Front. Oncol. 2021, 11, 720842. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.-W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus Ipilimumab in Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Ciuleanu, T.-E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-Line Nivolumab plus Ipilimumab Combined with Two Cycles of Chemotherapy in Patients with Non-Small-Cell Lung Cancer (CheckMate 9LA): An International, Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall | No Primary Resistance | Primary Resistance | p | ||
|---|---|---|---|---|---|
| N | 108 | 49 | 59 | ||
| Age (median (IQR)) | 64.17 (5.44, 71.50) | 66.25 (57.89, 72.82) | 62.00 (53.64, 70.13) | 0.144 | |
| Gender (%) | Female | 37 (34.3) | 11 (22.4) | 26 (44.1) | 0.018 |
| Male | 71 (65.7) | 38 (77.6) | 33 (55.9) | ||
| Ethnicity (%) | Chinese | 86 (79.6) | 39 (79.6) | 47 (79.7) | 0.685 |
| Indian | 4 (3.7) | 3 (6.1) | 1 (1.7) | ||
| Malay | 13 (12.0) | 5 (10.2) | 8 (13.6) | ||
| Others | 5 (4.6) | 2 (4.1) | 3 (5.1) | ||
| Smoking status (%) | No | 35 (33.7) | 12 (24.5) | 23 (41.8) | 0.062 |
| Yes | 69 (66.3) | 37 (75.5) | 32 (58.2) | ||
| Performance status (%) | 0 | 26 (34.2) | 13 (38.2) | 13 (31.0) | 0.506 |
| ≥1 | 50 (65.8) | 21 (61.8) | 29 (69.0) | ||
| Line of treatment (%) | 1 | 42 (38.9) | 26 (53.1) | 16 (27.1) | 0.034 |
| 2 | 31 (28.7) | 12 (24.5) | 19 (32.2) | ||
| 3 | 17 (15.7) | 4 (8.2) | 13 (22.0) | ||
| ≥4 | 18 (16.7) | 7 (14.3) | 11 (18.6) | ||
| Brain metastasis (%) | No | 78 (72.2) | 39 (79.6) | 39 (66.1) | 0.119 |
| Yes | 30 (27.8) | 10 (20.4) | 20 (33.9) | ||
| Histology (%) | Adenocarcinoma | 83 (76.9) | 39 (79.6) | 44 (74.6) | 0.536 |
| Squamous cell carcinoma | 13 (12.0) | 4 (8.2) | 9 (15.3) | ||
| Others | 12 (11.1) | 6 (12.2) | 6 (10.2) | ||
| PDL1 level (%) | <1% | 5 (8.8) | 3 (11.1) | 2 (6.7) | 0.916 |
| 1–49% | 13 (22.8) | 6 (22.2) | 7 (23.3) | ||
| ≥50% | 39 (68.4) | 18 (66.7) | 21 (70.0) | ||
| EGFR mutation (%) | No | 60 (75.9) | 32 (88.9) | 28 (65.1) | 0.018 |
| Yes | 19 (24.1) | 4 (11.1) | 15 (34.9) | ||
| BMI (kg/m2) (median [IQR]) | 21.10 [19.10, 24.16] | 21.12 [20.06, 24.07] | 21.00 [19.00, 24.17] | 0.641 | |
| Best response (%) | CR | 1 (0.9) | 1 (2.0) | 0 (0.0) | <0.001 |
| PD | 49 (45.4) | 4 (8.2) | 45 (76.3) | ||
| PR | 23 (21.3) | 23 (46.9) | 0 (0.0) | ||
| SD | 35 (32.4) | 21 (42.9) | 14 (23.7) | ||
| Immunotherapy agent (%) | Pembrolizumab | 60 (55.6) | 28 (57.1) | 32 (54.2) | |
| Nivolumab | 24 (22.2) | 7 (14.3) | 17 (28.8) | ||
| Durvalumab | 11 (10.2) | 5 (10.2) | 6 (10.2) | ||
| Atezolizumab | 8 (7.4) | 5 (10.2) | 3 (5.1) | 0.203 | |
| Avelumab | 5 (4.6) | 4 (8.2) | 1 (1.7) | ||
| 6th week lymphocyte count (×109 L) (median [IQR]) | 1.21 [0.94, 1.65] | 1.36 [1.09, 2.02] | 1.14 [0.83, 1.50] | 0.007 | |
| Pre-treatment NLR (%) | <3 | 19 (29.2) | 10 (40.0) | 9 (22.5) | 0.131 |
| ≥3 | 46 (70.8) | 15 (60.0) | 31 (77.5) | ||
| <5 | 36 (55.4) | 16 (64.0) | 20 (50.0) | 0.269 | |
| ≥5 | 29 (44.6) | 9 (36.0) | 20 (50.0) | ||
| Pre-treatment PLR (%) | <180 | 33 (35.1) | 16 (40.0) | 17 (31.5) | 0.392 |
| ≥180 | 61 (64.9) | 24 (60.0) | 37 (68.5) | ||
| 6th week NLR (%) | <3 | 31 (31.6) | 20 (48.8) | 11 (19.3) | 0.002 |
| ≥3 | 67 (68.4) | 21 (51.2) | 46 (80.7) | ||
| <5 | 59 (60.2) | 30 (73.2) | 29 (50.9) | 0.026 | |
| ≥5 | 39 (39.8) | 11 (26.8) | 28 (49.1) | ||
| 6th week PLR (%) | <180 | 27 (29.0) | 15 (40.5) | 12 (21.4) | 0.047 |
| ≥180 | 66 (71.0) | 22 (59.5) | 44 (78.6) |
| Variable | Comparison | Reference | OR | p | Adjusted-OR | p |
|---|---|---|---|---|---|---|
| Age | 0.979 (0.946–1.012) | 0.216 | ||||
| Gender | Female (n = 37) | Male (n = 71) | 2.725 (1.192–6.536) | 0.020 | 3.165 (1.078–10.101) | 0.041 |
| Ethnicity | Indian (n = 4) | Chinese (n = 86) | 0.277 (0.013–2.257) | 0.274 | ||
| Malay (n = 13) | Chinese (n = 86) | 1.328 (0.409–4.699) | 0.642 | |||
| Others (n = 5) | Chinese (n = 86) | 1.245 (0.197–9.808) | 0.816 | |||
| Smoking status | Yes (n = 69) | No (n = 35) | 0.451 (0.190–1.034) | 0.064 | 1.046 (0.330–3.389) | 0.939 |
| Alcohol | Yes (n = 27) | No (n = 57) | 0.628 (0.247–1.580) | 0.323 | ||
| Performance status | 0 (n = 26) | ≥1 (n = 50) | 0.724 (0.277–1.882) | 0.506 | ||
| Line of treatment | ≥2 (n = 66) | 1 (n = 42) | 3.040 (1.377–6.897) | 0.007 | 2.676 (1.056–7.008) | 0.040 |
| Brain metastasis | Yes (n = 30) | No (n = 78) | 2.000 (0.845–4.972) | 0.122 | ||
| Histology | Others (n = 12) | Adenocarcinoma (n = 83) | 0.886 (0.257–3.051) | 0.845 | ||
| Squamous cell carcinoma (n = 13) | Adenocarcinoma (n = 83) | 1.994 (0.598–7.831) | 0.281 | |||
| PD-L1 level | ≥50% (n = 39) | <1% (n = 5) | 1.750 (0.262–14.424) | 0.563 | ||
| 1–49% (n = 13) | <1% (n = 5) | 1.750 (0.217–16.980) | 0.601 | |||
| EGFR mutation | Yes (n = 19) | No (n = 60) | 4.286 (1.371–16.413) | 0.019 | ||
| BMI (kg/m2) | 0.995 (0.898–1.102) | 0.920 | ||||
| Pre-treatment lymphocyte count (×109 L) | 0.464 (0.237–0.844) | 0.017 | ||||
| 6th week lymphocyte count (×109 L) | 0.452 (0.222–0.829) | 0.017 | 0.769 (0.321–1.691) | 0.528 | ||
| Pre-treatment NLR ≥ 3 | ≥3 (n = 46) | <3 (n = 19) | 2.296 (0.773–6.988) | 0.135 | ||
| Pre-treatment NLR ≥ 5 | ≥5 (n = 29) | <5 (n = 36) | 1.778 (0.646–5.095) | 0.271 | ||
| 6th week NLR ≥ 3 | ≥3 (n = 67) | <3 (n = 31) | 3.983 (1.651–10.068) | 0.003 | 3.454 (1.102–11.643) | 0.037 |
| 6th week NLR ≥ 5 | ≥5 (n = 39) | <5 (n = 59) | 2.633 (1.130–6.433) | 0.028 | ||
| Pre-treatment PLR ≥ 180 | ≥180 (n = 61) | <180 (n = 33) | 1.451 (0.616–3.430) | 0.393 | ||
| 6th week PLR ≥ 180 | ≥180 (n = 66) | <180 (n = 27) | 2.500 (1.007–6.357) | 0.050 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.; Zhao, J.J.; Soon, Y.Y.; Kee, A.; Tay, S.H.; Aminkeng, F.; Ang, Y.; Wong, A.S.C.; Bharwani, L.D.; Goh, B.C.; et al. Factors Predictive of Primary Resistance to Immune Checkpoint Inhibitors in Patients with Advanced Non-Small Cell Lung Cancer. Cancers 2023, 15, 2733. https://doi.org/10.3390/cancers15102733
Huang Y, Zhao JJ, Soon YY, Kee A, Tay SH, Aminkeng F, Ang Y, Wong ASC, Bharwani LD, Goh BC, et al. Factors Predictive of Primary Resistance to Immune Checkpoint Inhibitors in Patients with Advanced Non-Small Cell Lung Cancer. Cancers. 2023; 15(10):2733. https://doi.org/10.3390/cancers15102733
Chicago/Turabian StyleHuang, Yiqing, Joseph J. Zhao, Yu Yang Soon, Adrian Kee, Sen Hee Tay, Folefac Aminkeng, Yvonne Ang, Alvin S. C. Wong, Lavina D. Bharwani, Boon Cher Goh, and et al. 2023. "Factors Predictive of Primary Resistance to Immune Checkpoint Inhibitors in Patients with Advanced Non-Small Cell Lung Cancer" Cancers 15, no. 10: 2733. https://doi.org/10.3390/cancers15102733
APA StyleHuang, Y., Zhao, J. J., Soon, Y. Y., Kee, A., Tay, S. H., Aminkeng, F., Ang, Y., Wong, A. S. C., Bharwani, L. D., Goh, B. C., & Soo, R. A. (2023). Factors Predictive of Primary Resistance to Immune Checkpoint Inhibitors in Patients with Advanced Non-Small Cell Lung Cancer. Cancers, 15(10), 2733. https://doi.org/10.3390/cancers15102733