
Comparative Effectiveness of Bevacizumab versus Cetuximab in Metastatic Colorectal Cancer Patients without Primary Tumor Resection

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
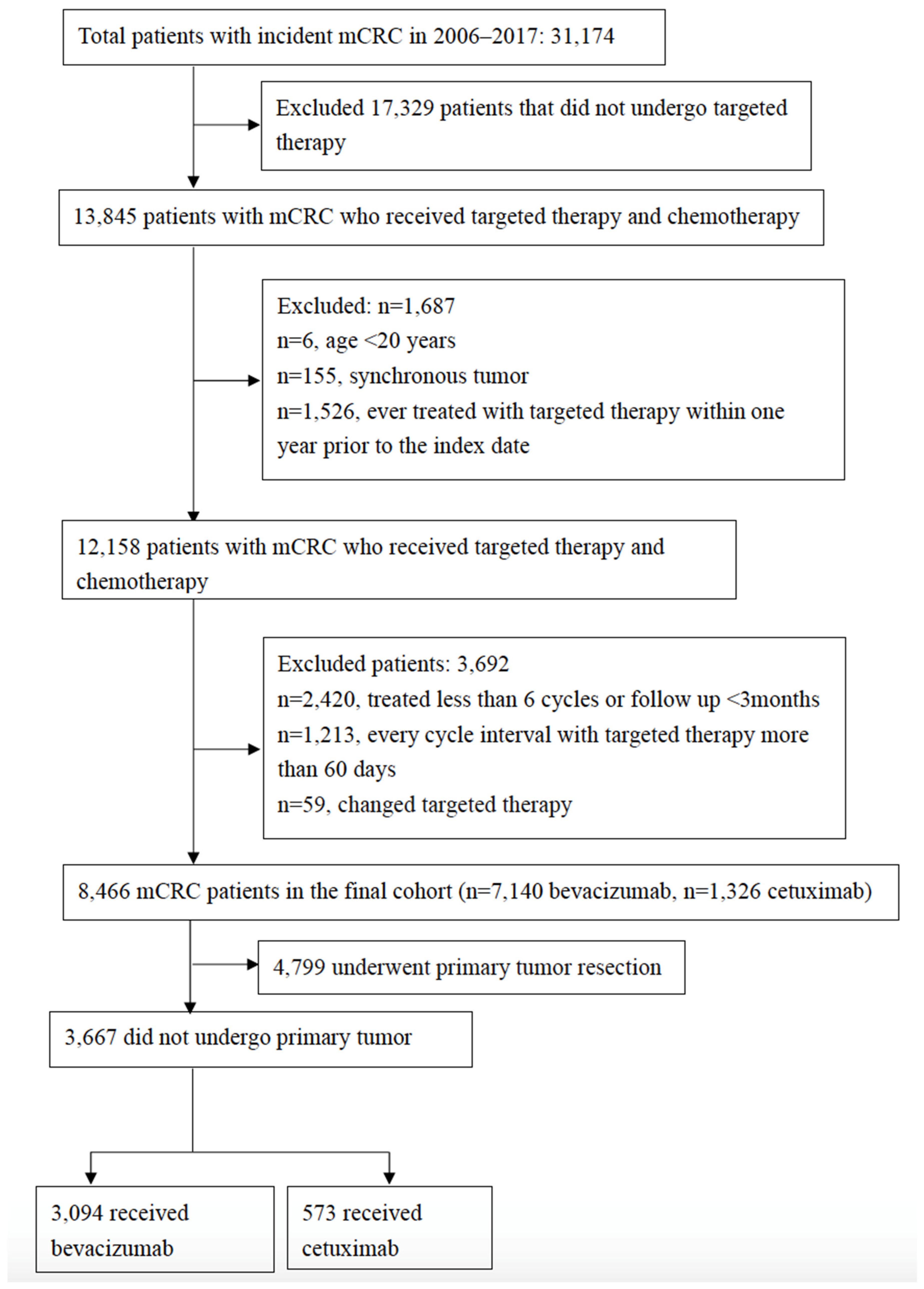
2.2. Study Population
2.3. Study Variables and Targeted Therapy Exposure
2.4. Statistical Analysis
2.5. Sensitivity Analyses
3. Results
3.1. Cohort Characteristics
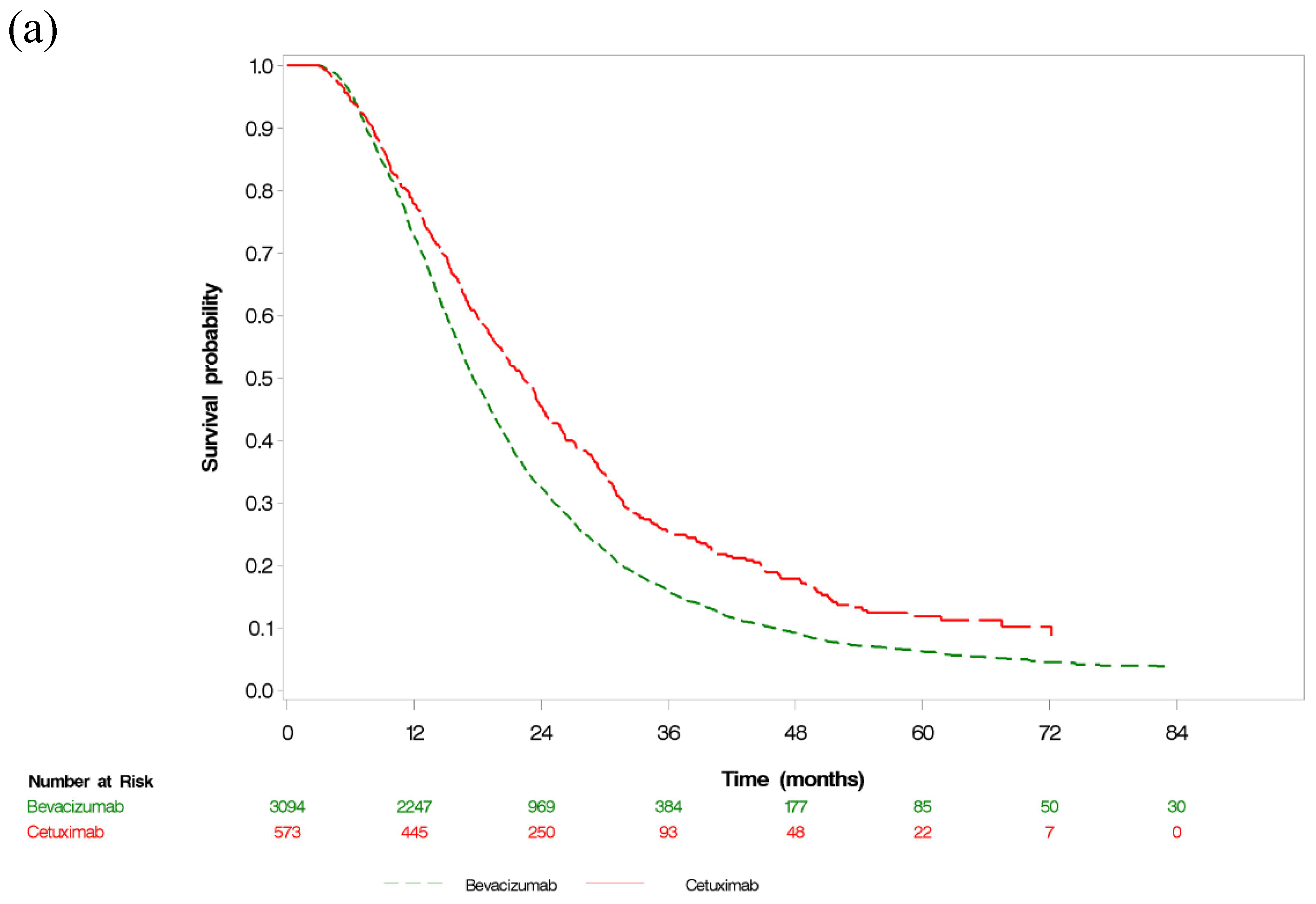
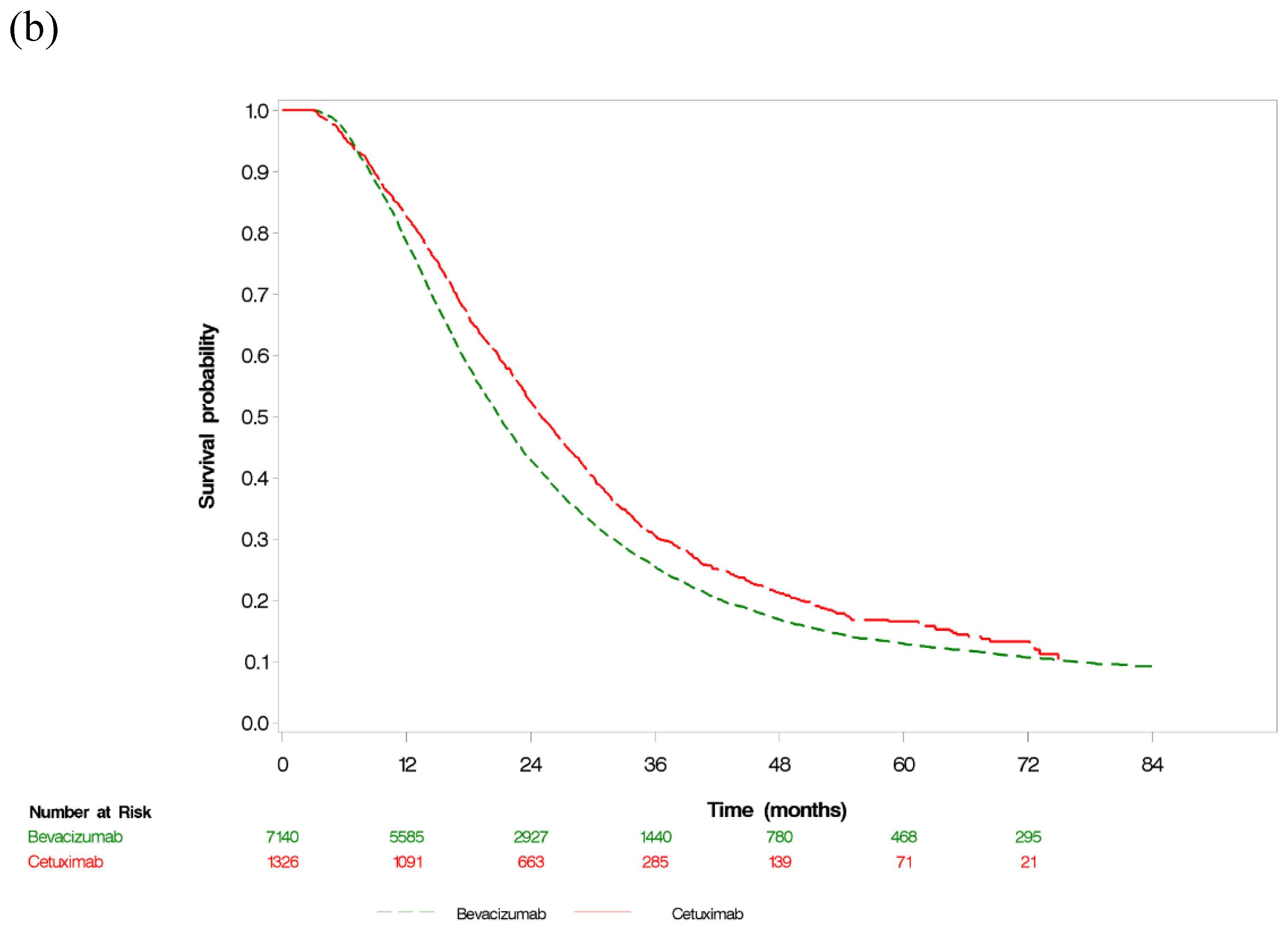
3.2. Overall Survival
3.3. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vatandoust, S.; Price, T.J.; Karapetis, C.S. Colorectal Cancer: Metastases to a Single Organ. World J. Gastroenterol. 2015, 21, 11767–11776. [Google Scholar] [CrossRef] [PubMed]
- Botrel, T.E.A.; Clark, L.G.O.; Paladini, L.; Clark, O.A.C. Efficacy and Safety of Bevacizumab plus Chemotherapy Compared to Chemotherapy Alone in Previously Untreated Advanced or Metastatic Colorectal Cancer: A Systematic Review and Meta-Analysis. BMC Cancer 2016, 16, 677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.C.; Wang, J.H.; Lin, P.C.; Liang, C.A.; Huang, C.Y.; Lien, H.C.; Chen, C.Y.; Chou, K.J.; Su, Y.C. Tumor Sidedness and Efficacy of First-Line Therapy in Patients with RAS/BRAF Wild-Type Metastatic Colorectal Cancer: A Network Meta-Analysis. Crit. Rev. Oncol. Hematol. 2020, 145, 102823. [Google Scholar] [CrossRef]
- Kemeny, N. Management of Liver Metastases from Colorectal Cancer. Oncology 2006, 20, 1161–1176. [Google Scholar] [PubMed]
- Onaitis, M.W.; Petersen, R.P.; Haney, J.C.; Saltz, L.; Park, B.; Flores, R.; Rizk, N.; Bains, M.S.; Dycoco, J.; D’Amico, T.A.; et al. Prognostic Factors for Recurrence After Pulmonary Resection of Colorectal Cancer Metastases. Ann. Thorac. Surg. 2009, 87, 1684–1688. [Google Scholar] [CrossRef] [PubMed]
- Faron, M.; Pignon, J.P.; Malka, D.; Bourredjem, A.; Douillard, J.Y.; Adenis, A.; Elias, D.; Bouché, O.; Ducreux, M. Is Primary Tumour Resection Associated with Survival Improvement in Patients with Colorectal Cancer and Unresectable Synchronous Metastases? A Pooled Analysis of Individual Data from Four Randomised Trials. Eur. J. Cancer 2015, 51, 166–176. [Google Scholar] [CrossRef]
- Shida, D.; Boku, N.; Tanabe, T.; Yoshida, T.; Tsukamoto, S.; Takashima, A.; Kanemitsu, Y. Primary Tumor Resection for Stage IV Colorectal Cancer in the Era of Targeted Chemotherapy. J. Gastrointest. Surg. 2019, 23, 2144–2150. [Google Scholar] [CrossRef]
- Venook, A.P.; Niedzwiecki, D.; Lenz, H.J.; Innocenti, F.; Fruth, B.; Meyerhardt, J.A.; Schrag, D.; Greene, C.; O’Neil, B.H.; Atkins, J.N.; et al. Effect of First-Line Chemotherapy Combined with Cetuximab or Bevacizumab on Overall Survival in Patients with KRAS Wild-Type Advanced or Metastatic Colorectal Cancer: A Randomized Clinical Trial. JAMA 2017, 317, 2392–2401. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, V.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.E.; Heintges, T.; Lerchenmüller, C.; Kahl, C.; Seipelt, G.; et al. FOLFIRI plus Cetuximab Versus FOLFIRI plus Bevacizumab as First-Line Treatment for Patients with Metastatic Colorectal Cancer (FIRE-3): A Randomised, Open-Label, phase 3 Trial. Lancet Oncol. 2014, 15, 1065–1075. [Google Scholar] [CrossRef]
- Bureau of National Health Insurance in Taiwan. The Drugs Payment Guideline for Anti-Neoplastic Agents. Available online: https://www.nhi.gov.tw/DL.aspx?sitessn=292&u=LzAwMS9VcGxvYWQvMjkyL3JlbGZpbGUvMC82MTM3L2NoYXA5XzEwOTEyLnBkZg%3d%3d&n=Y2hhcDlfMTA5MTIucGRm&ico%20=.pdf (accessed on 24 December 2020).
- Arnold, D.; Lueza, B.; Douillard, J.Y.; Peeters, M.; Lenz, H.J.; Venook, A.; Heinemann, V.; Van Cutsem, E.; Pignon, J.P.; Tabernero, J.; et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef] [PubMed]
- Modest, D.P.; Denecke, T.; Pratschke, J.; Ricard, I.; Lang, H.; Bemelmans, M.; Becker, T.; Rentsch, M.; Seehofer, D.; Bruns, C.J.; et al. Surgical Treatment Options Following Chemotherapy plus Cetuximab or Bevacizumab in Metastatic Colorectal Cancer-Central Evaluation of FIRE-3. Eur. J. Cancer 2018, 88, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shitara, K.; Mizusawa, J.; Hamaguchi, T.; Shida, D.; Komori, K.; Ikeda, S.; Ojima, H.; Ike, H.; Shiomi, A.; et al. Primary Tumor Resection Plus Chemotherapy Versus Chemotherapy Alone for Colorectal Cancer Patients with Asymptomatic, Synchronous Unresectable Metastases (JCOG1007; iPACS): A Randomized Clinical Trial. J Clin. Oncol. 2021, 39, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- van der Kruijssen, D.; Elias, S.G.; Vink, G.R.; van Rooijen, K.L.; Lam-Boer, J.; Mol, L.; Punt, C.; de Wilt, J.; Koopman, M.; CAIRO4 Working Group. Sixty-Day Mortality of Patients with Metastatic Colorectal Cancer Randomized to Systemic Treatment vs Primary Tumor Resection Followed by Systemic Treatment: The CAIRO4 Phase 3 Randomized Clinical Trial. JAMA Surg. 2021, 156, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Health and Welfare Data Science Center; Ministry of Health and Welfare Taiwan. National Health Insurance Research Database. Available online: http://nhird.nhri.org.tw/en/index.htm (accessed on 20 August 2021).
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and Future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Chiang, C.J.; You, S.L.; Chen, C.J.; Yang, Y.W.; Lo, W.C.; Lai, M.S. Quality Assessment and Improvement of Nationwide Cancer Registration System in Taiwan: A Review. Jpn J. Clin. Oncol. 2015, 45, 291–296. [Google Scholar] [CrossRef]
- Charlson, M.E.; Charlson, R.E.; Peterson, J.C.; Marinopoulos, S.S.; Briggs, W.M.; Hollenberg, J.P. The Charlson Comorbidity Index Is Adapted to Predict Costs of Chronic Disease in Primary Care Patients. J. Clin. Epidemiol. 2008, 61, 1234–1240. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a Clinical Comorbidity Index for Use with ICD-9-CM Administrative Databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef]
- Knol, M.J.; VanderWeele, T.J.; Groenwold, R.H.; Klungel, O.H.; Rovers, M.M.; Grobbee, D.E. Estimating measures of interaction on an additive scale for preventive exposures. Eur. J. Epidemiol. 2011, 26, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.A.; Kim, J.W.; Suh, K.J.; Chang, W.; Kim, J.W.; Oh, H.K.; Cho, J.Y.; Kim, D.W.; Cho, S.; Kim, J.H.; et al. Conversion Surgery After Cetuximab or Bevacizumab plus FOLFIRI Chemotherapy in Colorectal Cancer Patients with Liver- and/or Lung-Limited Metastases. J. Cancer Res. Clin. Oncol. 2020, 146, 2399–2410. [Google Scholar] [CrossRef] [PubMed]
- Modest, D.P.; Heinemann, V.; Folprecht, G.; Denecke, T.; Pratschke, J.; Lang, H.; Bemelmans, M.; Becker, T.; Rentsch, M.; Seehofer, D.; et al. Factors That Influence Conversion to Resectability and Survival After Resection of Metastases in RAS WT Metastatic Colorectal Cancer (mCRC): Analysis of FIRE-3- AIOKRK0306. Ann. Surg. Oncol. 2020, 27, 2389–2401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartzberg, L.S.; Rivera, F.; Karthaus, M.; Fasola, G.; Canon, J.L.; Hecht, J.R.; Yu, H.; Oliner, K.S.; Go, W.Y. PEAK: A Randomized, Multicenter phase II Study of Panitumumab plus Modified Fluorouracil, Leucovorin, and Oxaliplatin (mFOLFOX6) or Bevacizumab plus mFOLFOX6 in Patients with Previously Untreated, Unresectable, Wild-Type KRAS exon 2 Metastatic Colorectal Cancer. J. Clin. Oncol. 2014, 32, 2240–2247. [Google Scholar] [PubMed]
- Cao, D.; Zheng, Y.; Xu, H.; Ge, W.; Xu, X. Bevacizumab Improves Survival in Metastatic Colorectal Cancer Patients with Primary Tumor Resection: A Meta-Analysis. Sci. Rep. 2019, 9, 20326. [Google Scholar] [CrossRef] [Green Version]
- Shida, D.; Hamaguchi, T.; Ochiai, H.; Tsukamoto, S.; Takashima, A.; Boku, N.; Kanemitsu, Y. Prognostic Impact of Palliative Primary Tumor Resection for Unresectable stage 4 Colorectal Cancer: Using a Propensity Score Analysis. Ann. Surg. Oncol. 2016, 23, 3602–3608. [Google Scholar] [CrossRef]
- Korkmaz, L.; Coşkun, H.Ş.; Dane, F.; Karabulut, B.; Karaağaç, M.; Çabuk, D.; Karabulut, S.; Aykan, N.F.; Doruk, H.; Avcı, N.; et al. Kras-Mutation Influences Outcomes for Palliative Primary Tumor Resection in Advanced Colorectal Cancer-A Turkish Oncology Group Study. Surg. Oncol. 2018, 27, 485–489. [Google Scholar] [CrossRef]
- Cabart, M.; Frénel, J.S.; Campion, L.; Ramée, J.F.; Dupuis, O.; Senellart, H.; Hiret, S.; Douillard, J.Y.; Bennouna, J. Bevacizumab Efficacy Is Influenced by Primary Tumor Resection in First-Line Treatment of Metastatic Colorectal Cancer in a Retrospective Multicenter Study. Clin. Colorectal Cancer 2016, 15, e165–e174. [Google Scholar] [CrossRef]
- Ghiringhelli, F.; Bichard, D.; Limat, S.; Lorgis, V.; Vincent, J.; Borg, C.; Berthou, J.; Orry, D.; Ortega-Deballon, P.; Lakkis, Z.; et al. Bevacizumab Efficacy in Metastatic Colorectal Cancer Is Dependent on Primary Tumor Resection. Ann. Surg. Oncol. 2014, 21, 1632–1640. [Google Scholar] [CrossRef] [Green Version]
- Bozkurt Duman, B.; Çil, T. Do the Survival Data of Primary Tumor Resection Provide Sufficient Data Without Considering the Tumor Sidedness, Predictive Biomarkers, and Biologic Agents? J. Clin. Oncol. 2021, 39, 2970. [Google Scholar] [CrossRef]
- Kanemitsu, Y. Reply to B. Bozkurt Duman et al. J. Clin. Oncol. 2021, 39, 2970–2971. [Google Scholar] [CrossRef]
- Shitara, K.; Yonesaka, K.; Denda, T.; Yamazaki, K.; Moriwaki, T.; Tsuda, M.; Takano, T.; Okuda, H.; Nishina, T.; Sakai, K.; et al. Randomized Study of FOLFIRI plus Either Panitumumab or Bevacizumab for Wild-Type KRAS Colorectal Cancer-WJOG 6210G. Cancer Sci. 2016, 107, 1843–1850. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Without Primary Tumor Resection (n = 3667) | Overall mCRC (n = 8466) | ||||
|---|---|---|---|---|---|---|
| Targeted therapy | B (n = 3094), n (%) | C (n = 573), n (%) | SMD | B (n = 7140), n (%) | C (n = 1326), n (%) | SMD |
| Sex | 0.08 | 0.1 | ||||
| Male | 1805 (58.34) | 356 (62.13) | 4014 (56.22) | 809 (61.01) | ||
| Female | 1289 (41.66) | 217 (37.87) | 3126 (43.78) | 517 (38.99) | ||
| Age, y | −0.08 | −0.06 | ||||
| <50 | 580 (18.75) | 125 (21.82) | 1387 (19.43) | 287 (21.64) | ||
| 50–59 | 865 (27.69) | 162 (28.27) | 1999 (28) | 376 (28.36) | ||
| 60–69 | 862 (27.86) | 154 (26.88) | 2012 (28.18) | 370 (27.9) | ||
| ≥70 | 787 (25.44) | 132 (23.04) | 1742 (24.4) | 293 (22.1) | ||
| Year of mCRC diagnosis | 0.63 | 0.67 | ||||
| 2006–2009 | 45 (1.45) | 11 (1.92) | 93 (1.3) | 28 (2.1) | ||
| 2010 | 43 (1.39) | 3 (0.52) | 199 (2.79) | 25 (1.89) | ||
| 2011 | 317 (10.25) | 5 (0.87) | 900 (12.61) | 19 (1.43) | ||
| 2012 | 439 (14.19) | 20 (3.49) | 1042 (14.59) | 60 (4.52) | ||
| 2013 | 432 (13.96) | 89 (15.53) | 997 (13.96) | 211 (15.91) | ||
| 2014 | 423 (13.67) | 125 (21.82) | 917 (12.84) | 261 (19.68) | ||
| 2015 | 405 (13.09) | 92 (16.06) | 880 (12.32) | 225 (16.97) | ||
| 2016 | 467 (15.09) | 95 (16.58) | 1040 (14.57) | 239 (18.02) | ||
| 2017 | 523 (16.9) | 133 (23.21) | 1072 (15.01) | 258 (19.46) | ||
| Year of targeted therapy | 0.79 | 0.88 | ||||
| 2011 | 290 (9.37) | 0 (0) | 752 (10.53) | 0 (0.00) | ||
| 2012 | 467 (15.09) | 0 (0) | 1151 (16.12) | 0 (0.00) | ||
| 2013 | 430 (13.9) | 97 (16.93) | 996 (13.95) | 233 (17.57) | ||
| 2014 | 418 (13.51) | 131 (22.86) | 956 (13.39) | 285 (21.49) | ||
| 2015 | 429 (13.87) | 94 (16.4) | 905 (12.68) | 227 (17.12) | ||
| 2016 | 451 (14.58) | 99 (17.28) | 997 (13.96) | 255 (19.23) | ||
| 2017 | 514 (16.61) | 124(21.64) | 1085 (15.2) | 260 (19.61) | ||
| 2018–2019 | 95 (3.07) | 28 (4.89) | 298 (4.17) | 66 (4.98) | ||
| Radiotherapy | 533 (17.23) | 106 (18.5) | 0.03 | 911 (12.76) | 182 (13.73) | 0.03 |
| Charlson comorbidity index | 2.70 ± 1.01 | 2.66 ± 1.05 | −0.03 | 2.651 ± 0.98 | 2.62 ± 1.00 | −0.03 |
| Intra-abdominal infection | 87 (2.81) | 16 (2.79) | 0 | 230 (3.22) | 43 (3.24) | 0 |
| Surgery before index date | ||||||
| Primary tumor resection | 0 (0) | 0(0) | 4046 (56.67) | 753 (56.79) | 0 | |
| Liver resection | 22 (0.71) | 11 (1.92) | 0.11 | 759 (10.63) | 166 (12.52) | 0.06 |
| Lung resection | 31 (1) | 10 (1.75) | 0.06 | 191 (2.68) | 33 (2.49) | −0.01 |
| Tumor sidedness | 0.25 | 0.26 | ||||
| Right | 810 (26.18) | 89 (15.53) | 2154 (30.17) | 249 (18.77) | ||
| Left | 2284 (73.82) | 484 (84.47) | 4986 (69.83) | 1077 (81.22) | ||
| Tumor differentiation grade | 0.16 | 0.09 | ||||
| Well differentiated | 134 (4.33) | 23 (4.01) | 233 (3.26) | 33 (2.49) | ||
| Moderately differentiated | 1565 (50.58) | 309 (53.93) | 4701 (65.84) | 912 (68.78) | ||
| Poorly differentiated | 260 (8.4) | 51 (8.9) | 828 (11.6) | 153 (11.54) | ||
| Undifferentiated; anaplastic | 16 (0.52) | 3 (0.52) | 85 (1.19) | 15 (1.13) | ||
| Missing | 1119 (36.17) | 187 (32.64) | 1293 (18.11) | 213 (16.06) | ||
| Histologic type | 0.19 | 0.2 | ||||
| Adenocarcinoma | 2935 (94.86) | 559 (97.56) | 6586 (92.24) | 1256 (94.72) | ||
| Mucinous | 122 (3.94) | 10 (1.75) | 463 (6.48) | 48 (3.62) | ||
| Signet ring cell carcinoma | 37 (1.2) | 4 (0.7) | 91 (1.27) | 22 (1.66) | ||
| Tumor stage | 0.47 | 0.36 | ||||
| T0 | 18 (0.58) | 4 (0.7) | 25 (0.35) | 4 (0.3) | ||
| T1 | 7 (0.23) | 3 (0.52) | 28 (0.39) | 8 (0.6) | ||
| T2 | 41 (1.33) | 14 (2.44) | 130 (1.82) | 36 (2.71) | ||
| T3 | 500 (16.16) | 143 (24.96) | 2538 (35.55) | 533 (40.2) | ||
| T4 | 342 (11.05) | 66 (11.52) | 2013 (28.19) | 351 (26.47) | ||
| TX | 2154 (69.62) | 335 (58.46) | 2346 (32.86) | 380 (28.66) | ||
| Nodal stage | 0.47 | 0.36 | ||||
| N0 | 198 (6.4) | 51 (8.9) | 690 (9.66) | 137 (10.33) | ||
| N1 | 307 (9.92) | 85 (14.83) | 1595 (22.34) | 294 (22.17) | ||
| N2 | 384 (12.41) | 91 (15.88) | 2420 (33.89) | 498 (37.56) | ||
| NX | 2174 (70.27) | 338 (58.99) | 2380 (33.33) | 384 (28.96) | ||
| Tumor size | 0.09 | 0.04 | ||||
| <4 cm | 569 (18.39) | 104 (18.15) | 1633 (22.87) | 313 (23.6) | ||
| 4–5 cm | 373 (12.06) | 74 (12.91) | 1193 (16.71) | 218 (16.44) | ||
| >5 cm | 966 (31.22) | 197 (34.38) | 2756 (38.6) | 525 (39.59) | ||
| Missing | 1186 (38.33) | 198 (34.55) | 1558 (21.82) | 270 (20.36) | ||
| Stage | 0.14 | 0.16 | ||||
| 4A | 1487 (48.06) | 316 (55.15) | 3761 (52.68) | 786 (59.28) | ||
| 4B | 1560 (50.42) | 246 (42.93) | 3284 (45.99) | 512 (38.61) | ||
| Missing | 47 (1.52) | 11 (1.92) | 95 (1.33) | 28 (2.11) | ||
| Positive lymph nodes, number (mean ± SD) | 4.80 ± 6.70 | 4.17 ± 5.36 | −0.1 | 5.68 ± 6.89 | 5.89 ± 6.83 | 0.03 |
| Chemotherapy type | 0.10 | 0.12 | ||||
| No chemotherapy | 3 (0.1) | 4 (0.7) | 16 (22) | 4 (0.3) | ||
| 5-FU | 121 (3.91) | 11 (1.92) | 281 (3.94) | 26 (1.96) | ||
| Irinotecan | 8 (0.26) | 3 (0.52) | 16 (0.22) | 11 (0.83) | ||
| Oxaplatin | 0 (0) | 0 (0) | 0 (0) | 0 (0) | ||
| 5-FU + irinotecan | 2769 (89.5) | 497 (86.74) | 6424 (89.97) | 1169 (88.16) | ||
| 5-FU + oxaplatin | 102 (3.3) | 39 (6.81) | 223 (3.12) | 72 (5.43) | ||
| 5-FU + oxaplatin + irinotecan | 91 (2.94) | 19 (3.32) | 180 (2.52) | 44 (3.32) | ||
| Co-medication | ||||||
| Cardiac glucosides | 32 (1.03) | 8 (1.4) | 0.03 | 76 (1.06) | 15 (1.13) | 0.01 |
| Anti-dyslipidemia agents | 531 (17.16) | 107 (18.67) | 0.04 | 1132 (15.85) | 223 (16.82) | 0.03 |
| Beta blocker | 681 (22.01) | 153 (26.7) | 0.11 | 1854 (25.97) | 356 (26.58) | 0.02 |
| Calcium channel blockers | 1031 (33.32) | 187 (32.64) | −0.01 | 2587 (36.23) | 443 (33.41) | −0.06 |
| Diuretic agents | 886 (28.64) | 182 (31.76) | 0.07 | 2489 (34.86) | 465 (35.07) | 0 |
| ACEI or ARB | 856 (27.67) | 159 (27.75) | 0 | 1921 (26.9) | 346 (26.09) | −0.02 |
| Anti-diabetes agents | 629 (20.33) | 114 (19.9) | −0.01 | 1577 (22.09) | 304 (22.93) | 0.02 |
| Anti-hemorrhage agents | 1204 (38.91) | 238 (41.54) | 0.05 | 3041 (42.59) | 578 (43.59) | 0.02 |
| Anti-arrhythmic agents | 405 (13.09) | 91 (496) | 0.08 | 1317 (18.45) | 240 (18.1) | −0.01 |
| Anti-fungal agents | 60 (1.94) | 14 (2.44) | 0.03 | 150 (2.1) | 35 (2.64) | 0.04 |
| Anti-bacterial agents | 2677 (86.52) | 503 (87.78) | 0.04 | 6636 (92.94) | 1225 (92.38) | −0.02 |
| Non-selective NSAID | 2119 (68.49) | 366 (63.87) | −0.1 | 5078 (71.12) | 919 (69.31) | −0.04 |
| Selective NSAID | 267 (8.63) | 45 (7.85) | −0.03 | 578 (8.22) | 109 (8.22) | 0 |
| Operation | Bevacizumab | Cetuximab | Treatment Type within Strata of Patients with/without Operation |
|---|---|---|---|
| Un-matched | |||
| Primary tumor resection | 0.60 (0.57–0.63) | 0.55 (0.41–0.73) | 0.91 (0.72–1.16) |
| Without primary tumor resection | 1 (reference) | 0.73 (0.66–0.81) | 0.73 (0.66–0.81) |
| Primary tumor resection within strata of treatment type | 0.60 (0.57–0.63) | 0.75 (0.62–0.91) | |
| PS matched a | |||
| Primary tumor resection | 0.56 (0.50–0.64) | 0.56 (0.37–0.87) | 1.00 (0.74–1.36) |
| Without primary tumor resection | 1 (reference) | 0.76 (0.66–0.86) | 0.76 (0.66–0.86) |
| Primary tumor resection within strata of treatment type | 0.56 (0.50–0.64) | 0.75 (0.55–1.01) | |
| SIPTW a | |||
| Primary tumor resection | 0.60 (0.57–0.63) | 0.57 (0.42–0.75) | 0.95 (0.75–1.20) |
| Without primary tumor resection | 1 (reference) | 0.75 (0.68–0.83) | 0.75 (0.68–0.83) |
| Primary tumor resection within strata of treatment type | 0.60 (0.57–0.63) | 0.75 (0.62–0.91) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Y.-C.; Wu, C.-C.; Su, C.-C.; Hsieh, M.-C.; Cheng, C.-L.; Kao Yang, Y.-H. Comparative Effectiveness of Bevacizumab versus Cetuximab in Metastatic Colorectal Cancer Patients without Primary Tumor Resection. Cancers 2022, 14, 2118. https://doi.org/10.3390/cancers14092118
Su Y-C, Wu C-C, Su C-C, Hsieh M-C, Cheng C-L, Kao Yang Y-H. Comparative Effectiveness of Bevacizumab versus Cetuximab in Metastatic Colorectal Cancer Patients without Primary Tumor Resection. Cancers. 2022; 14(9):2118. https://doi.org/10.3390/cancers14092118
Chicago/Turabian StyleSu, Yi-Chia, Chih-Chien Wu, Chien-Chou Su, Meng-Che Hsieh, Ching-Lan Cheng, and Yea-Huei Kao Yang. 2022. "Comparative Effectiveness of Bevacizumab versus Cetuximab in Metastatic Colorectal Cancer Patients without Primary Tumor Resection" Cancers 14, no. 9: 2118. https://doi.org/10.3390/cancers14092118
APA StyleSu, Y.-C., Wu, C.-C., Su, C.-C., Hsieh, M.-C., Cheng, C.-L., & Kao Yang, Y.-H. (2022). Comparative Effectiveness of Bevacizumab versus Cetuximab in Metastatic Colorectal Cancer Patients without Primary Tumor Resection. Cancers, 14(9), 2118. https://doi.org/10.3390/cancers14092118