
Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma

 , , , add
Show full author list
, , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection, Sample Collection, and Data Collection
2.2. Microbiome Analyses
2.3. Statistical Analyses
3. Results
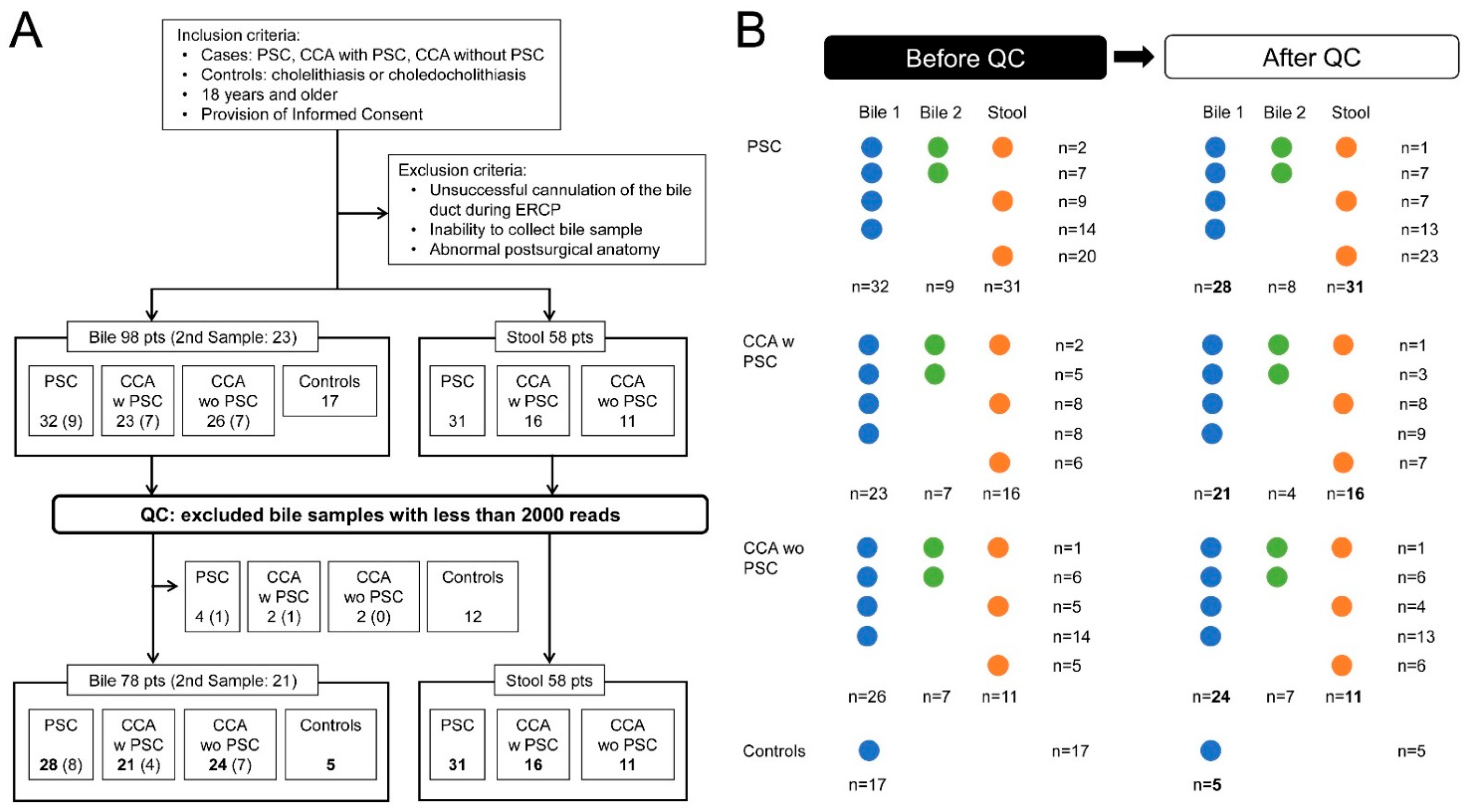
3.1. Sample Collection and Patient Characteristics
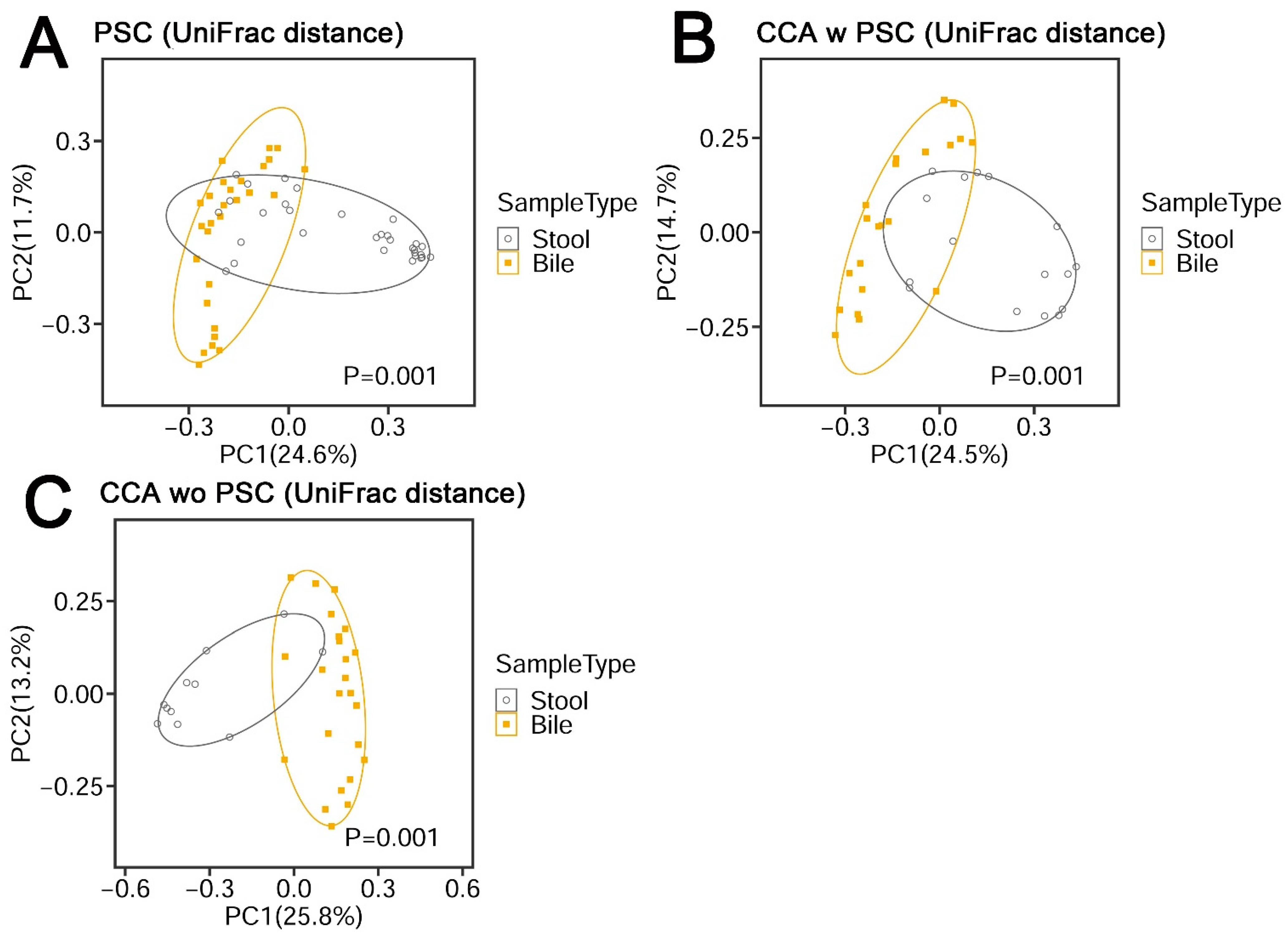
3.2. Bile Has a Unique Microbiota Distinguished from the Negative DNA Controls
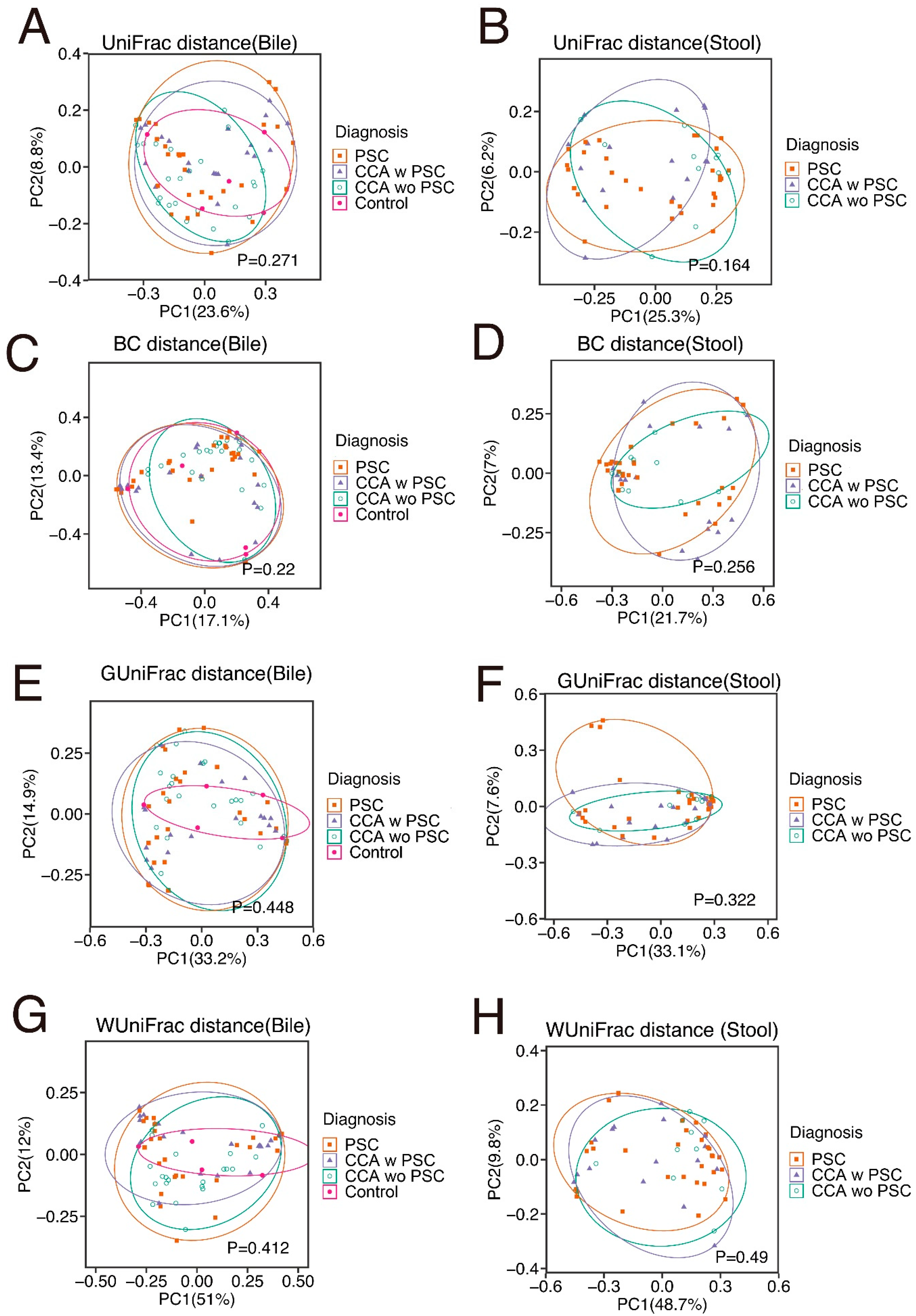
3.3. Demographic and Clinical Factors Influencing the Biliary and Stool Microbiota in PSC and CCA Patients
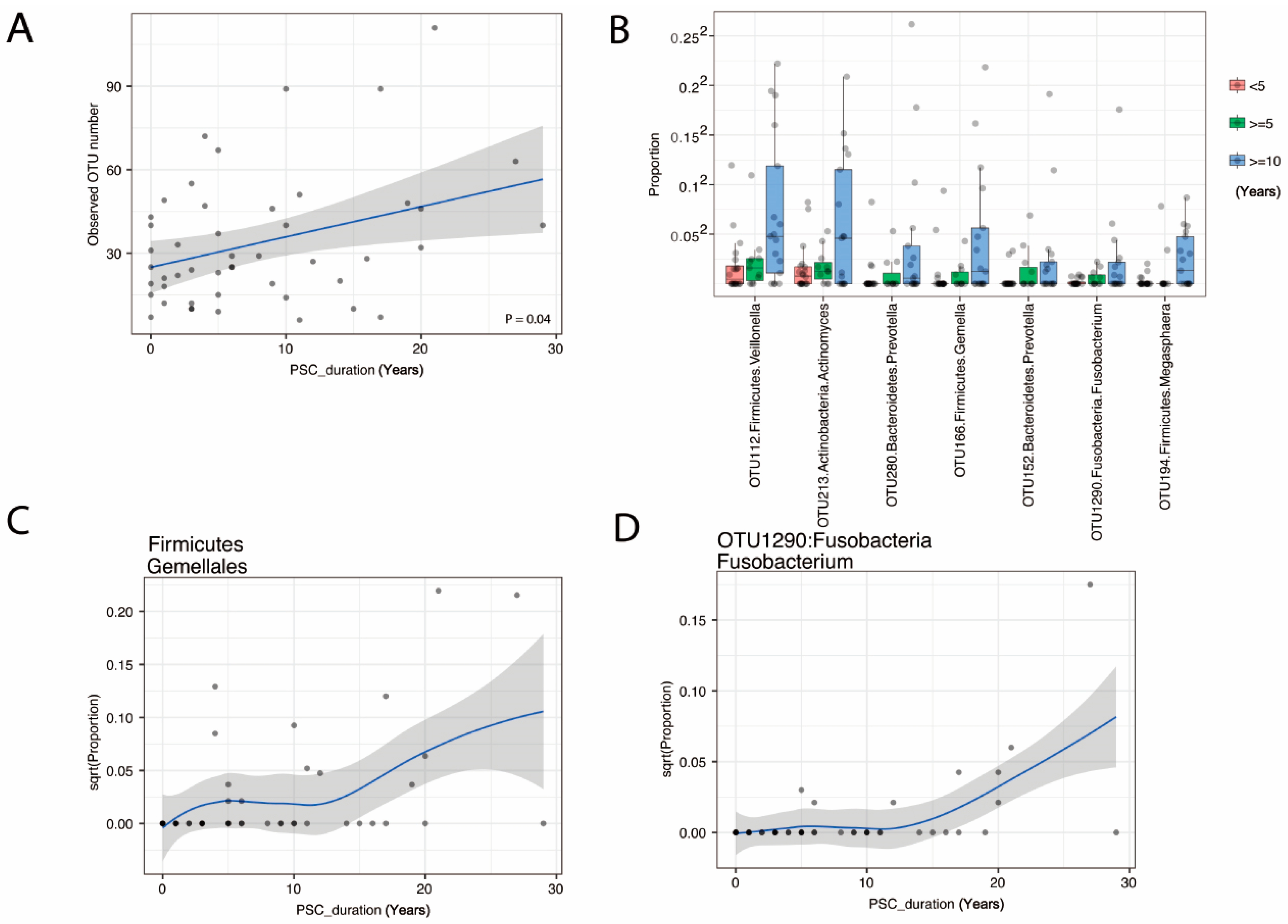
3.4. The Duration of PSC Is Correlated with Increased Species Richness and Abundance of Fusobacteria
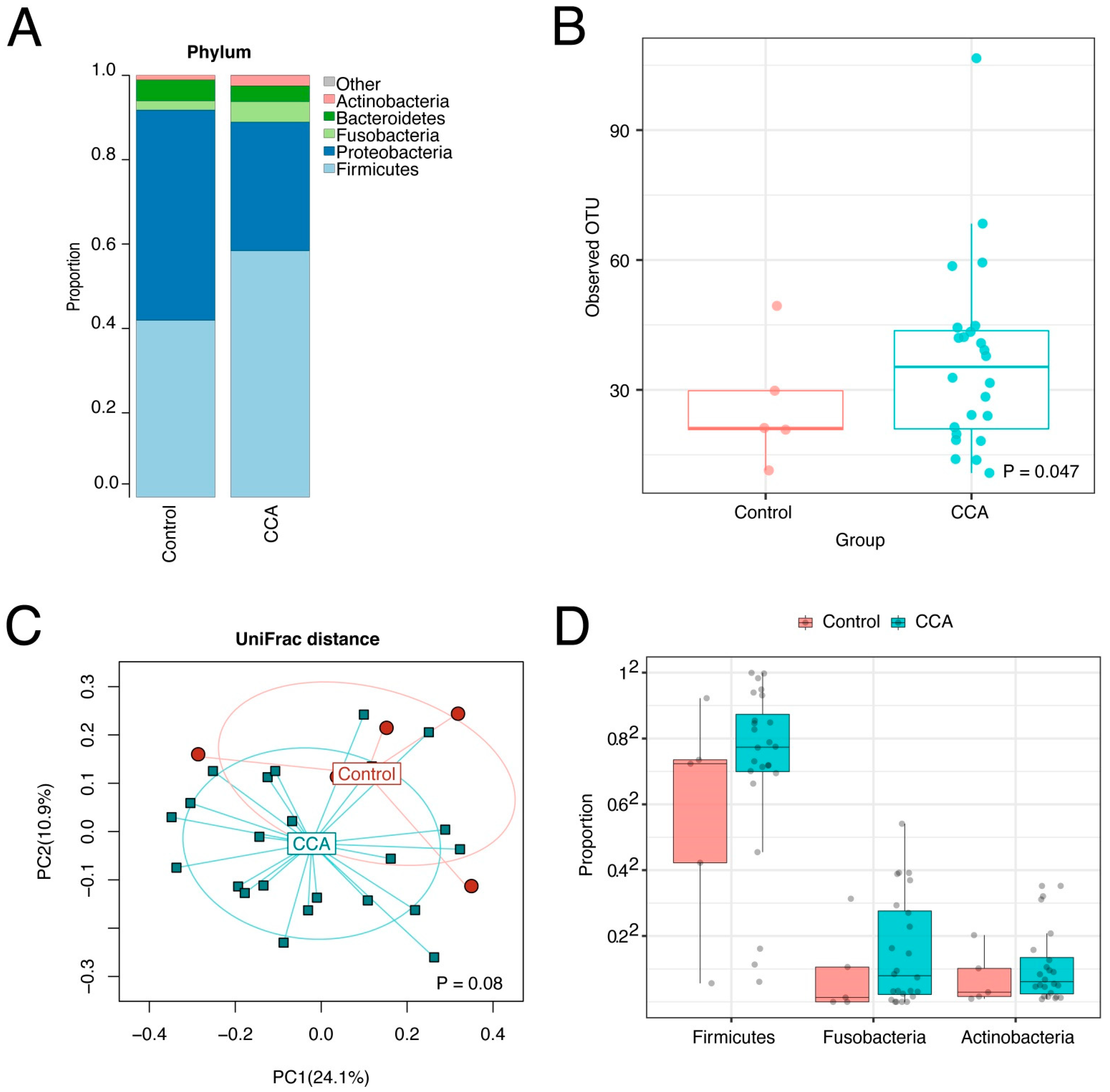
3.5. The CCA Biliary Microbiota Is also Characterized by Increased Species Richness and Abundance of Fusobacteria
3.6. The Stool Microbiota Was Not Statistically Different between PSC, CCA w PSC, or CCA wo PSC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tabibian, J.H.; Lindor, K.D. Primary sclerosing cholangitis: A review and update on therapeutic developments. Expert Rev. Gastroenterol. Hepatol. 2013, 7, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Bowlus, C.L. Primary sclerosing cholangitis: Etiopathogenesis and clinical management. Front. Biosci. 2012, 4, 1683–1705. [Google Scholar] [CrossRef]
- Dyson, J.K.; Beuers, U.; Jones, D.E.J.; Lohse, A.W.; Hudson, M. Primary sclerosing cholangitis. Lancet 2018, 391, 2547–2559. [Google Scholar] [CrossRef]
- Rizvi, S.; Gores, G.J. Pathogenesis, diagnosis, and management of cholangiocarcinoma. Gastroenterology 2013, 145, 1215–1229. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Kim, B.; Sanderson, S.O.; Sauver, J.S.; Yawn, B.P.; Larson, J.J.; Therneau, T.M.; Roberts, L.; Gores, G.J.; Kim, R.W. Biliary Tract Cancers in Olmsted County, Minnesota, 1976–2008. Am. J. Gastroenterol. 2012, 107, 1256–1262. [Google Scholar] [CrossRef]
- Bertuccio, P.; Bosetti, C.; Levi, F.; Decarli, A.; Negri, E.; La Vecchia, C. A comparison of trends in mortality from primary liver cancer and intrahepatic cholangiocarcinoma in Europe. Ann. Oncol. 2013, 24, 1667–1674. [Google Scholar] [CrossRef]
- Chen, B.; Fu, S.W.; Lu, L.; Zhao, H. A Preliminary Study of Biliary Microbiota in Patients with Bile Duct Stones or Distal Cholangiocarcinoma. Biomed. Res. Int. 2019, 2019, 1092563. [Google Scholar] [CrossRef]
- Saab, M.; Mestivier, D.; Sohrabi, M.; Rodriguez, C.; Khonsari, M.R.; Faraji, A.; Sobhani, I. Characterization of biliary microbiota dysbiosis in extrahepatic cholangiocarcinoma. PLoS ONE 2021, 16, e0247798. [Google Scholar] [CrossRef]
- Lazaridis, K.N.; LaRusso, N.F. Primary Sclerosing Cholangitis. N. Engl. J. Med. 2016, 375, 1161–1170. [Google Scholar] [CrossRef]
- Chen, X.; Johnson, S.; Jeraldo, P.; Wang, J.; Chia, N.; Kocher, J.A.; Chen, J. Hybrid-denovo: A de novo OTU-picking pipeline integrating single-end and paired-end 16S sequence tags. Gigascience. 2018, 7, 1–7. [Google Scholar] [CrossRef]
- Price, M.N.; Dehal, P.S.; Arkin, A.P. FastTree 2—Approximately maximum-likelihood trees for large alignments. PLoS ONE 2010, 5, e9490. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Bittinger, K.; Charlson, E.S.; Hoffmann, C.; Lewis, J.; Wu, G.D.; Collman, R.G.; Bushman, F.D.; Li, H. Associating microbiome composition with environmental covariates using generalized UniFrac distances. Bioinformatics 2012, 28, 2106–2113. [Google Scholar] [CrossRef]
- Kummen, M.; Holm, K.; Anmarkrud, J.A.; Nygård, S.; Vesterhus, M.; Høivik, M.L.; Trøseid, M.; Marschall, H.-U.; Schrumpf, E.; Moum, B.; et al. The gut microbial profile in patients with primary sclerosing cholangitis is distinct from patients with ulcerative colitis without biliary disease and healthy controls. Gut 2017, 66, 611–619. [Google Scholar] [CrossRef]
- Quraishi, M.N.; Sergeant, M.; Kay, G.; Iqbal, T.; Chan, J.; Constantinidou, C.; Trivedi, P.; Ferguson, J.; Adams, D.H.; Pallen, M.; et al. The gut-adherent microbiota of PSC–IBD is distinct to that of IBD. Gut 2017, 66, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Lu, S.; Zeng, Z.; Liu, Q.; Dong, Z.; Chen, Y.; Zhu, Z.; Hong, Z.; Zhang, T.; Du, G.; et al. Characterization of Gut Microbiota, Bile Acid Metabolism, and Cytokines in Intrahepatic Cholangiocarcinoma. Hepatology 2020, 71, 893–906. [Google Scholar] [CrossRef]
- Pereira, P.; Aho, V.; Arola, J.; Boyd, S.; Jokelainen, K.; Paulin, L.; Auvinen, P.; Färkkilä, M. Bile microbiota in primary sclerosing cholangitis: Impact on disease progression and development of biliary dysplasia. PLoS ONE 2017, 12, e0182924. [Google Scholar] [CrossRef]
- Jimenez, E.; Sanchez, B.; Farina, A.; Margolles, A.; Rodriguez, J.M. Characterization of the bile and gall bladder microbiota of healthy pigs. Microbiologyopen 2014, 3, 937–949. [Google Scholar] [CrossRef]
- Liwinski, T.; Zenouzi, R.; John, C.; Ehlken, H.; Rühlemann, M.C.; Bang, C.; Groth, S.; Lieb, W.; Kantowski, M.; Andersen, N.; et al. Alterations of the bile microbiome in primary sclerosing cholangitis. Gut 2020, 69, 665–672. [Google Scholar] [CrossRef]
- Gaiser, R.A.; Halimi, A.; Alkharaan, H.; Lu, L.; Davanian, H.; Healy, K.; Hugerth, L.W.; Ateeb, Z.; Valente, R.; Moro, C.F.; et al. Enrichment of oral microbiota in early cystic precursors to invasive pancreatic cancer. Gut 2019, 68, 2186–2194. [Google Scholar] [CrossRef]
- Sabino, J.; Vieira-Silva, S.; Machiels, K.; Joossens, M.; Falony, G.; Ballet, V.; Ferrante, M.; Van Assche, G.; Van der Merwe, S.; Vermeire, S.; et al. Primary sclerosing cholangitis is characterised by intestinal dysbiosis independent from IBD. Gut 2016, 65, 1681–1689. [Google Scholar] [CrossRef] [PubMed]
- Ruhlemann, M.C.; Heinsen, F.A.; Zenouzi, R.; Lieb, W.; Franke, A.; Schramm, C. Faecal microbiota profiles as diagnostic biomarkers in primary sclerosing cholangitis. Gut 2017, 66, 753–754. [Google Scholar] [CrossRef] [PubMed]
- Gulamhusein, A.F.; Eaton, J.E.; Tabibian, J.H.; Atkinson, E.J.; Juran, B.D.; Lazaridis, K.N. Duration of Inflammatory Bowel Disease Is Associated with Increased Risk of Cholangiocarcinoma in Patients With Primary Sclerosing Cholangitis and IBD. Am. J. Gastroenterol. 2016, 111, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Engevik, M.A.; Danhof, H.A.; Ruan, W.; Engevik, A.C.; Chang-Graham, A.L.; Engevik, K.A.; Shi, Z.; Zhao, Y.; Brand, C.K.; Krystofiak, E.S.; et al. Fusobacterium nucleatum Secretes Outer Membrane Vesicles and Promotes Intestinal Inflammation. MBio 2021, 12, e02706-20. [Google Scholar] [CrossRef]
- Levy, M.J.; Norton, I.D.; Clain, J.E.; Enders, F.B.; Gleeson, F.; Limburg, P.J.; Nelson, H.; Rajan, E.; Topazian, M.; Wang, K.K.; et al. Prospective Study of Bacteremia and Complications with EUS FNA of Rectal and Perirectal Lesions. Clin. Gastroenterol. Hepatol. 2007, 5, 684–689. [Google Scholar] [CrossRef]
- Purcell, L.K.; Finley, J.P.; Chen, R.; Lovgren, M.; Halperin, S.A. Gemella species endocarditis in a child. Can. J. Infect. Dis. 2001, 12, 317–320. [Google Scholar]
- Thurnheer, T.; Karygianni, L.; Flury, M.; Belibasakis, G.N. Fusobacterium Species and Subspecies Differentially Affect the Composition and Architecture of Supra- and Subgingival Biofilms Models. Front. Microbiol. 2019, 10, 1716. [Google Scholar] [CrossRef]
- Cheng, C.; Wei, H.; Yu, H.; Xu, C.; Jiang, S.; Peng, J. Metabolic Syndrome During Perinatal Period in Sows and the Link with Gut Microbiota and Metabolites. Front. Microbiol. 2018, 9, 1989. [Google Scholar] [CrossRef]
- Qin, N.; Yang, F.; Li, A.; Prifti, E.; Chen, Y.; Shao, L.; Guo, J.; Le Chatelier, E.; Yao, J.; Wu, L.; et al. Alterations of the human gut microbiome in liver cirrhosis. Nature 2014, 513, 59–64. [Google Scholar] [CrossRef]
- Strauss, J.; Kaplan, G.; Beck, P.L.; Rioux, K.; Panaccione, R.; DeVinney, R.; Lynch, T.; Allen-Vercoe, E. Invasive potential of gut mucosa-derived fusobacterium nucleatum positively correlates with IBD status of the host. Inflamm. Bowel Dis. 2011, 17, 1971–1978. [Google Scholar] [CrossRef]
- Gevers, D.; Kugathasan, S.; Denson, L.A.; Vázquez-Baeza, Y.; Van Treuren, W.; Ren, B.; Schwager, E.; Knights, D.; Song, S.J.; Yassour, M.; et al. The Treatment-Naive Microbiome in New-Onset Crohn’s Disease. Cell Host Microbe 2014, 15, 382–392. [Google Scholar] [CrossRef] [PubMed]
- Kostic, A.D.; Gevers, D.; Pedamallu, C.S.; Michaud, M.; Duke, F.; Earl, A.M.; Ojesina, A.I.; Jung, J.; Bass, A.J.; Tabernero, J.; et al. Genomic analysis identifies association of Fusobacterium with colorectal carcinoma. Genome Res. 2012, 22, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Wehbe, H.; Henson, R.; Meng, F.; Mize-Berge, J.; Patel, T. Interleukin-6 contributes to growth in cholangiocarcinoma cells by aberrant promoter methylation and gene expression. Cancer Res. 2006, 66, 10517–10524. [Google Scholar] [CrossRef]
- Pinto, C.; Giordano, D.M.; Maroni, L.; Marzioni, M. Role of inflammation and proinflammatory cytokines in cholangiocyte pathophysiology. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 1270–1278. [Google Scholar] [CrossRef]
- Tilg, H.; Cani, P.D.; Mayer, E.A. Gut microbiome and liver diseases. Gut 2016, 65, 2035–2044. [Google Scholar] [CrossRef] [PubMed]
- Syal, G.; Fausther, M.; Dranoff, J.A. Advances in cholangiocyte immunobiology. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 303, G1077–G1086. [Google Scholar] [CrossRef]
- Choi, J.; Ghoz, H.M.; Peeraphatdit, T.; Baichoo, E.; Addissie, B.D.; Harmsen, W.S.; Therneau, T.M.; Olson, J.E.; Chaiteerakij, R.; Roberts, L.R. Aspirin use and the risk of cholangiocarcinoma. Hepatology 2016, 64, 785–796. [Google Scholar] [CrossRef]
- Lavu, S.; Therneau, T.M.; Harmsen, W.S.; Mara, K.C.; Wongjarupong, N.; Hassan, M.; Ali, H.A.; Antwi, S.; Giama, N.H.; Miyabe, K.; et al. Effect of Statins on the Risk of Extrahepatic Cholangiocarcinoma. Hepatology 2020, 72, 1298–1309. [Google Scholar] [CrossRef]
- Jeraldo, P.; Kalari, K.; Chen, X.; Bhavsar, J.; Mangalam, A.; White, B.; Nelson, H.; Kocher, J.; Chia, N. IM-TORNADO: A tool for comparison of 16S reads from paired-end libraries. PLoS ONE 2014, 9, e114804. [Google Scholar] [CrossRef]
- Chen, L.; Reeve, J.; Zhang, L.; Huang, S.; Wang, X.; Chen, J. GMPR: A robust normalization method for zero-inflated count data with application to microbiome sequencing data. PeerJ 2018, 6, e4600. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis (# with Bile 1/# with Bile 2) | PSC (n = 28/8) | CCA w PSC (n = 21/4) | CCA wo PSC (n = 24/7) | Controls (n = 5) | p |
|---|---|---|---|---|---|
| Female, n (%) | 10 (36) | 3 (14) | 6 (25) | 3 (60) | NS |
| Race, white, n (%) | 28 (100) | 19 (91) | 22 (92) | 5 (100) | NS |
| Age (years), Median (IQR) | 60 (47–66) | 45 (37–52) | 62 (51–73) | 69 (59–69) | <0.001 |
| BMI (kg/m2), Median (IQR) | 26 (23–28) | 24 (21–29) | 27 (22–32) | 34 (29–39) | NS |
| PSC duration (years), Median (IQR) | 5 (3–13) | 6 (1–10) | NA | NA | NS |
| CCA site, perihilar, n (%) | NA | 20 (95) | 23 (96) | NA | NS |
| Cholelithiasis, n (%) | 3 (11) | 8 (38) | 1 (4) | 3 (60) | 0.006 |
| Choledocholithiasis, n (%) | 3 (11) | 0 (0) | 4 (17) | 4 (80) | <0.001 |
| Leukocytosis, n (%) | |||||
| Bile 1 | 2 (7) | 6 (29) | 4 (17) | 0 (0) | NS |
| Bile 2 | 0 (0) | 1 (25) | 0 (0) | NA | NS |
| Antibiotic use, n (%) | 10 (36) | 9 (43) | 8 (33) | 0 (0) | NS |
| Use for more than a month | 3(11) | 4(19) | 2(8) | 0(0) | NS |
| MELD score, Median (IQR) | 10 (8–14) | 18 (10–22) | 11 (8–18) | 12 (9–12) | NS |
| Surgical Procedures | NS | ||||
| Ileal pouch, n (%) | 2 (7) | 6 (29) | 1 (4) | 0 (0) | 0.038 |
| Ileostomy, n (%) | 1 (4) | 2 (10) | 1 (4) | 0 (0) | NS |
| Cholecystectomy, n (%) | 5 (18) | 4 (19) | 5 (21) | 2 (40) | NS |
| Treatments | |||||
| Chemotherapy, n (%) | 0 (0) | 11 (52) | 14 (58) | 0 (0) | <0.001 |
| Radiotherapy, n (%) | 0 (0) | 11 (52) | 11 (46) | 0 (0) | <0.001 |
| Stent Placement, n (%) | 9 (32) | 11 (52) | 21 (88) | 2 (40) | <0.001 |
| Plastic stent *, n (%) | 9 (32) | 10 (48) | 19 (79) | 2 (40) | 0.008 |
| Metallic stent *, n (%) | 0 (0) | 1 (5) | 5 (21) | 0 (0) | 0.031 |
| Steroid use (for IBD), n (%) | 4 (14) | 3 (14) | 4 (17) | 1 (20) | NS |
| Immunosuppressant, n (%) | 5 (18) | 5 (24) | 1 (4) | 0 (0) | NS |
| Lifestyle Factors | |||||
| Alcohol use, n (%) | 14 (50) | 11 (52) | 15 (63) | 2 (40) | NS |
| Current smoker, n (%) | 6 (21) | 5 (24) | 14 (58) | 2 (40) | 0.026 |
| Comorbidities | |||||
| IBD, n (%) | 20 (71) | 16 (76) | 0 (0) | 0 (0) | <0.001 |
| Hypertension, n (%) | 15 (54) | 5 (24) | 14 (58) | 3 (60) | NS |
| Hypercholesterolemia, n (%) | 8 (29) | 5 (24) | 9 (38) | 2 (40) | NS |
| Diabetes mellitus, n (%) | 2 (7) | 5 (24) | 5 (21) | 0 (0) | NS |
| Diagnosis | PSC (n = 31) | CCA w PSC (n = 16) | CCA wo PSC (n = 11) | p |
|---|---|---|---|---|
| Female, n (%) | 12 (39) | 5 (31) | 3 (27) | NS |
| Race, white, n (%) | 30 (97) | 14 (88) | 10 (91) | NS |
| Age (years), Median (IQR) | 51 (43–60) | 52 (45–55) | 60 (51–64) | NS |
| BMI (kg/m2), Median (IQR) | 26 (23–28) | 25 (23–28) | 26 (23–29) | NS |
| PSC duration (years), Median (IQR) | 10 (4–18) | 7 (3–12) | NA | NS |
| CCA site, perihilar, n (%) | NA | 12 (75) | 9 (82) | NS |
| Cholelithiasis, n (%) | 2 (6) | 1 (6) | 1 (9) | NS |
| Choledocholithiasis, n (%) | 3 (10) | 1 (6) | 3 (27) | NS |
| Leukocytosis, n (%) | 2 (7) | 5 (31) | 0 (0) | 0.019 |
| Antibiotic use, n (%) | 11 (36) | 4 (25) | 2 (18) | NS |
| Use for more than a month | 8 (26) | 3 (19) | 0 (0) | NS |
| MELD score, Median (IQR) | 9 (7–15) | 16 (9–22) | 11 (8–18) | NS |
| Surgical Procedures | NS | |||
| Ileal pouch, n (%) | 8 (26) | 5 (31) | 2 (18) | NS |
| Ileostomy, n (%) | 5 (16) | 2 (14) | 2 (18) | NS |
| Cholecystectomy, n (%) | 10 (32) | 6 (38) | 3 (27) | NS |
| Treatments | ||||
| Chemotherapy, n (%) | 0 (0) | 6 (38) | 2 (18) | 0.002 |
| Radiotherapy, n (%) | 0 (0) | 4 (25) | 2 (18) | 0.018 |
| Stent Placement, n (%) | 3 (10) | 5 (31) | 9 (82) | <0.001 |
| Plastic stent *, n (%) | 3 (10) | 5 (31) | 7 (64) | 0.002 |
| Metallic stent *, n (%) | 1 (3) | 0 (0) | 3 (27) | 0.011 |
| Steroid use (for IBD), n (%) | 4 (13) | 5 (31) | 1 (9) | NS |
| Immunosuppressant, n (%) | 3 (10) | 2 (13) | 1 (9) | NS |
| Lifestyle Factors | NS | |||
| Alcohol use, n (%) | 17 (55) | 9 (56) | 7 (64) | NS |
| Current smoker, n (%) | 1 (3) | 4 (25) | 3 (27) | 0.043 |
| Comorbidities | NS | |||
| IBD, n (%) | 24 (77) | 12 (75) | 1 (9) | <0.001 |
| Hypertension, n (%) | 8 (26) | 3 (19) | 4 (36) | NS |
| Hypercholesterolemia, n (%) | 12 (39) | 6 (38) | 3 (27) | NS |
| Diabetes mellitus, n (%) | 4 (13) | 4 (25) | 4 (36) | NS |
| Sample | Bile | Stool | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| UniFrac | WUniFrac | GUniFrac | Bray-Curtis | Omnibus | UniFrac | WUniFrac | GUniFrac | Bray-Curtis | Omnibus | |
| Diagnosis * | 0.154 | 0.414 | 0.409 | 0.201 | 0.347 | 0.18 | 0.494 | 0.339 | 0.287 | 0.309 |
| Gender | 0.01 | 0.334 | 0.107 | 0.728 | 0.026 | 0.869 | 0.9 | 0.886 | 0.814 | 0.963 |
| Age | 0.183 | 0.154 | 0.123 | 0.261 | 0.291 | 0.052 | 0.087 | 0.075 | 0.195 | 0.09 |
| BMI | 0.581 | 0.759 | 0.866 | 0.671 | 0.865 | 0.509 | 0.206 | 0.304 | 0.507 | 0.338 |
| IBD | 0.555 | 0.305 | 0.298 | 0.046 | 0.117 | 0.001 | 0.035 | 0.021 | 0.015 | 0.001 |
| Cholelithiasis | 0.254 | 0.057 | 0.053 | 0.147 | 0.13 | 0.903 | 0.722 | 0.812 | 0.344 | 0.517 |
| Hypertension | 0.578 | 0.24 | 0.246 | 0.135 | 0.312 | 0.636 | 0.278 | 0.261 | 0.400 | 0.415 |
| Hypercholesterolemia | 0.569 | 0.81 | 0.796 | 0.770 | 0.861 | 0.995 | 0.896 | 0.928 | 0.850 | 0.975 |
| Diabetes mellitus | 0.840 | 0.42 | 0.629 | 0.716 | 0.738 | 0.455 | 0.804 | 0.778 | 0.708 | 0.667 |
| Ileal Pouch | 0.127 | 0.015 | 0.011 | 0.017 | 0.029 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 |
| Ileostomy | 0.213 | 0.274 | 0.279 | 0.421 | 0.435 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 |
| Cholecystectomy | 0.192 | 0.031 | 0.03 | 0.352 | 0.076 | 0.918 | 0.615 | 0.704 | 0.226 | 0.36 |
| Chemotherapy | 0.223 | 0.043 | 0.044 | 0.105 | 0.116 | 0.161 | 0.256 | 0.132 | 0.051 | 0.085 |
| Radiotherapy | 0.095 | 0.36 | 0.303 | 0.304 | 0.231 | 0.406 | 0.575 | 0.429 | 0.189 | 0.301 |
| Antibiotics use | 0.017 | 0.165 | 0.05 | 0.311 | 0.045 | 0.002 | 0.019 | 0.005 | 0.007 | 0.004 |
| Steroid intake | 0.689 | 0.61 | 0.596 | 0.281 | 0.565 | 0.074 | 0.429 | 0.279 | 0.374 | 0.125 |
| Immunosuppressant intake | 0.582 | 0.298 | 0.332 | 0.06 | 0.151 | 0.278 | 0.35 | 0.349 | 0.574 | 0.438 |
| Stent placement | 0.037 | 0.18 | 0.078 | 0.001 | 0.001 | 0.463 | 0.197 | 0.289 | 0.335 | 0.335 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyabe, K.; Chandrasekhara, V.; Wongjarupong, N.; Chen, J.; Yang, L.; Johnson, S.; Chia, N.; Walther-Antonio, M.; Yao, J.Z.; Harrington, S.C.; et al. Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma. Cancers 2022, 14, 2120. https://doi.org/10.3390/cancers14092120
Miyabe K, Chandrasekhara V, Wongjarupong N, Chen J, Yang L, Johnson S, Chia N, Walther-Antonio M, Yao JZ, Harrington SC, et al. Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma. Cancers. 2022; 14(9):2120. https://doi.org/10.3390/cancers14092120
Chicago/Turabian StyleMiyabe, Katsuyuki, Vinay Chandrasekhara, Nicha Wongjarupong, Jun Chen, Lu Yang, Stephen Johnson, Nicholas Chia, Marina Walther-Antonio, Janet Z. Yao, Sean C. Harrington, and et al. 2022. "Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma" Cancers 14, no. 9: 2120. https://doi.org/10.3390/cancers14092120
APA StyleMiyabe, K., Chandrasekhara, V., Wongjarupong, N., Chen, J., Yang, L., Johnson, S., Chia, N., Walther-Antonio, M., Yao, J. Z., Harrington, S. C., Nordyke, C. K., Eaton, J. E., Gossard, A. A., Oli, S., Ali, H. A., Lavu, S., Giama, N. H., Hassan, F. A., Ali, H. M., ... Roberts, L. R. (2022). Potential Role of Inflammation-Promoting Biliary Microbiome in Primary Sclerosing Cholangitis and Cholangiocarcinoma. Cancers, 14(9), 2120. https://doi.org/10.3390/cancers14092120