
A Consistent Protocol Reveals a Large Heterogeneity in the Biological Effectiveness of Proton and Carbon-Ion Beams for Various Sarcoma and Normal-Tissue-Derived Cell Lines

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
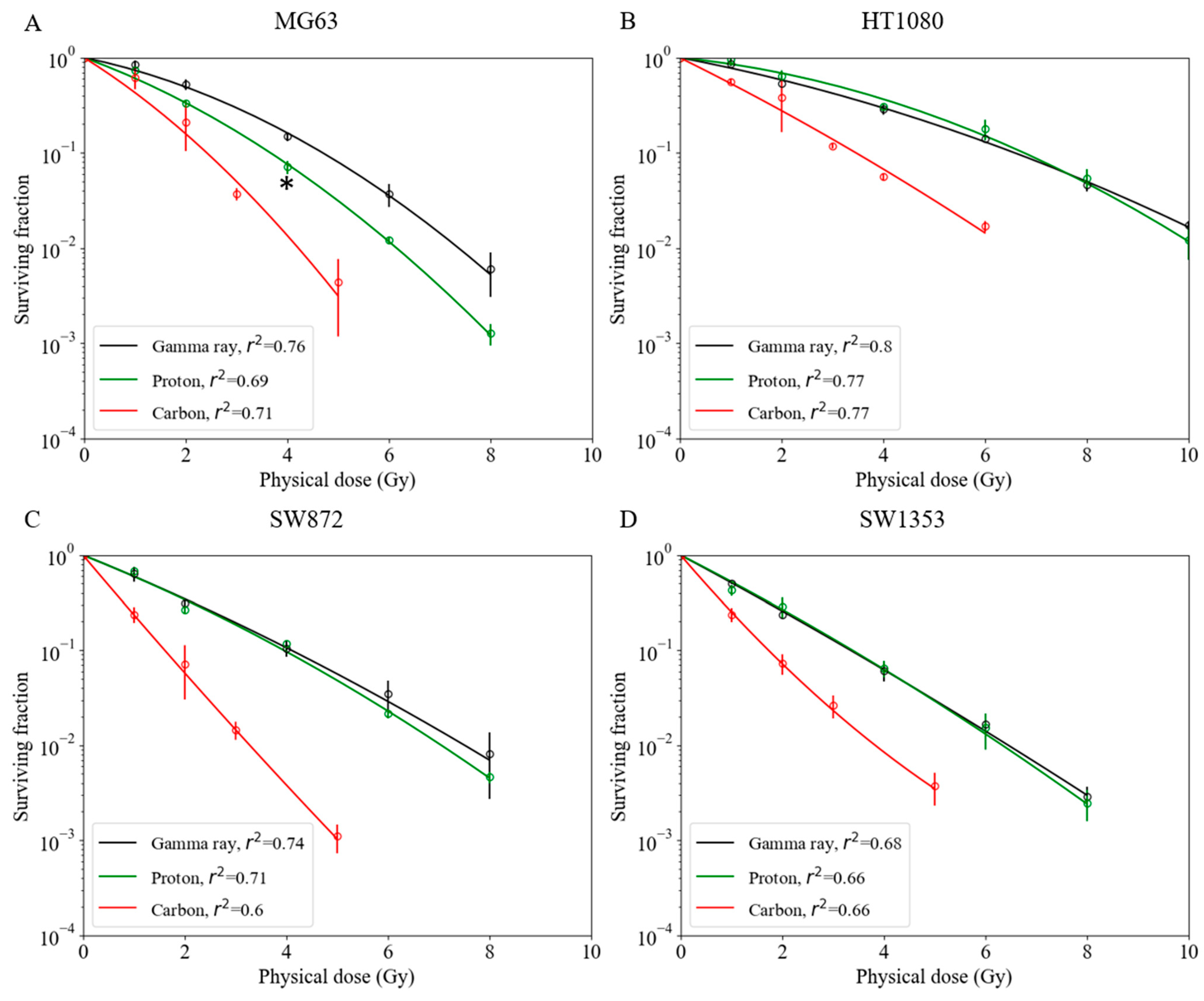
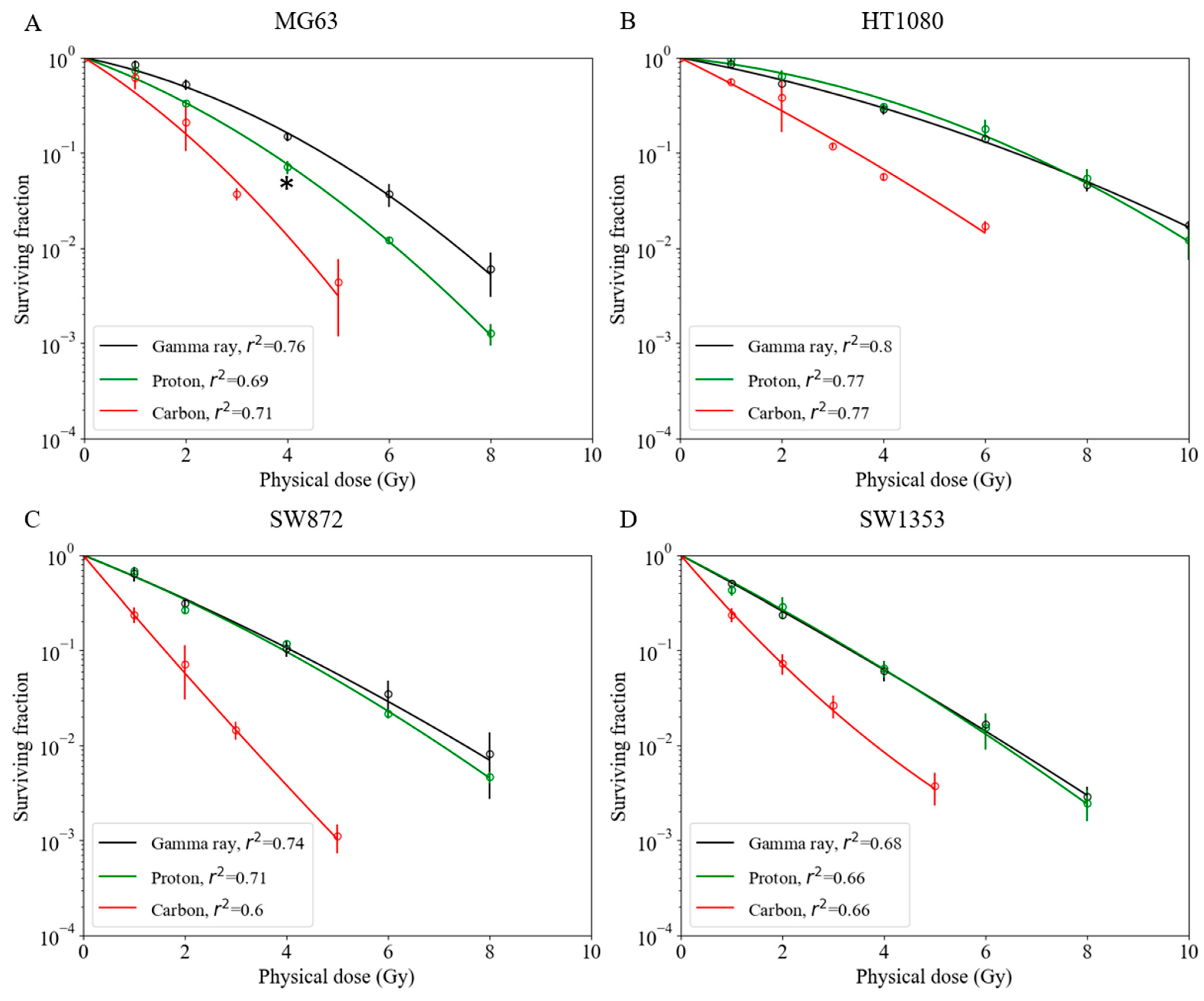
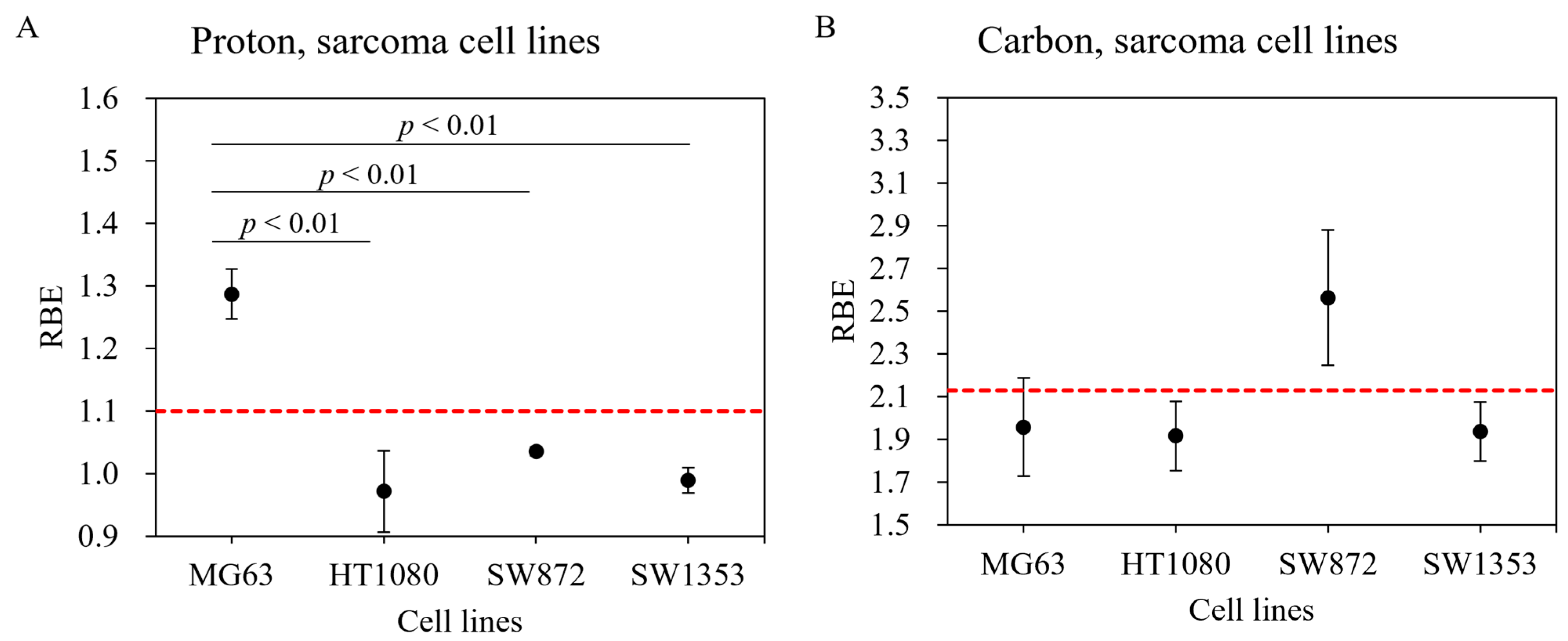
2.1. Survival Fractions for Various Sarcoma Cell Lines for Gamma Ray, Proton Beam, and Carbon-Ion Irradiation
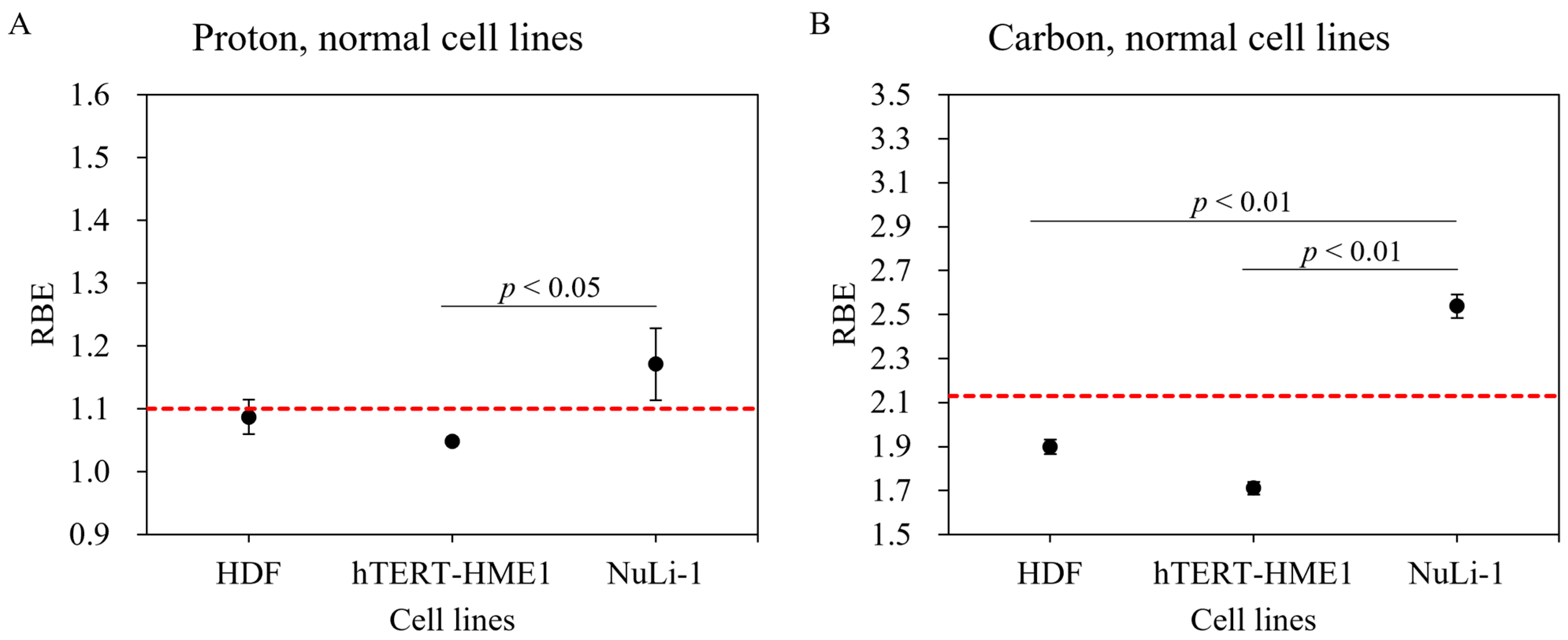
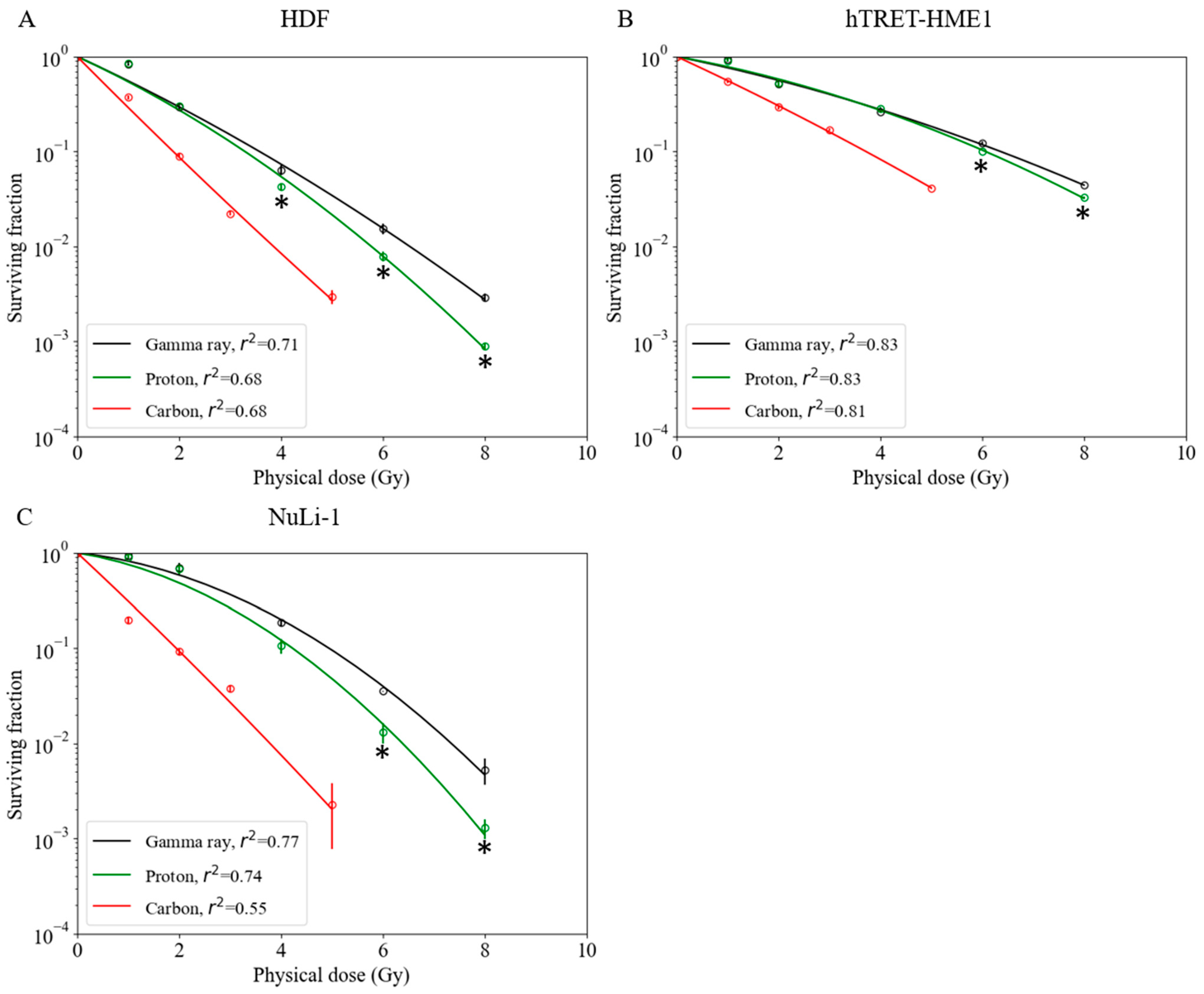
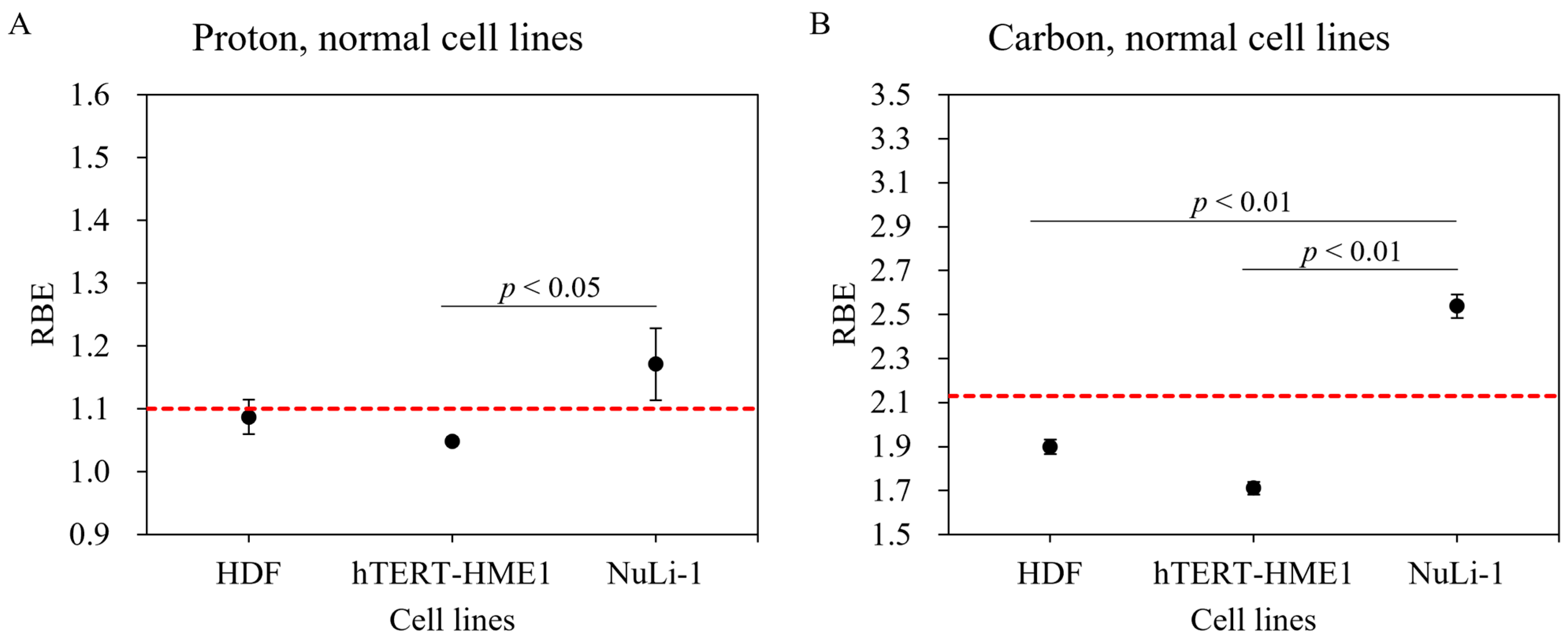
2.2. Survival Fractions for Various Normal Cell Lines for Gamma Ray, Proton Beam, and Carbon-Ion Irradiations
3. Discussion
4. Materials and Methods
4.1. Cell Lines
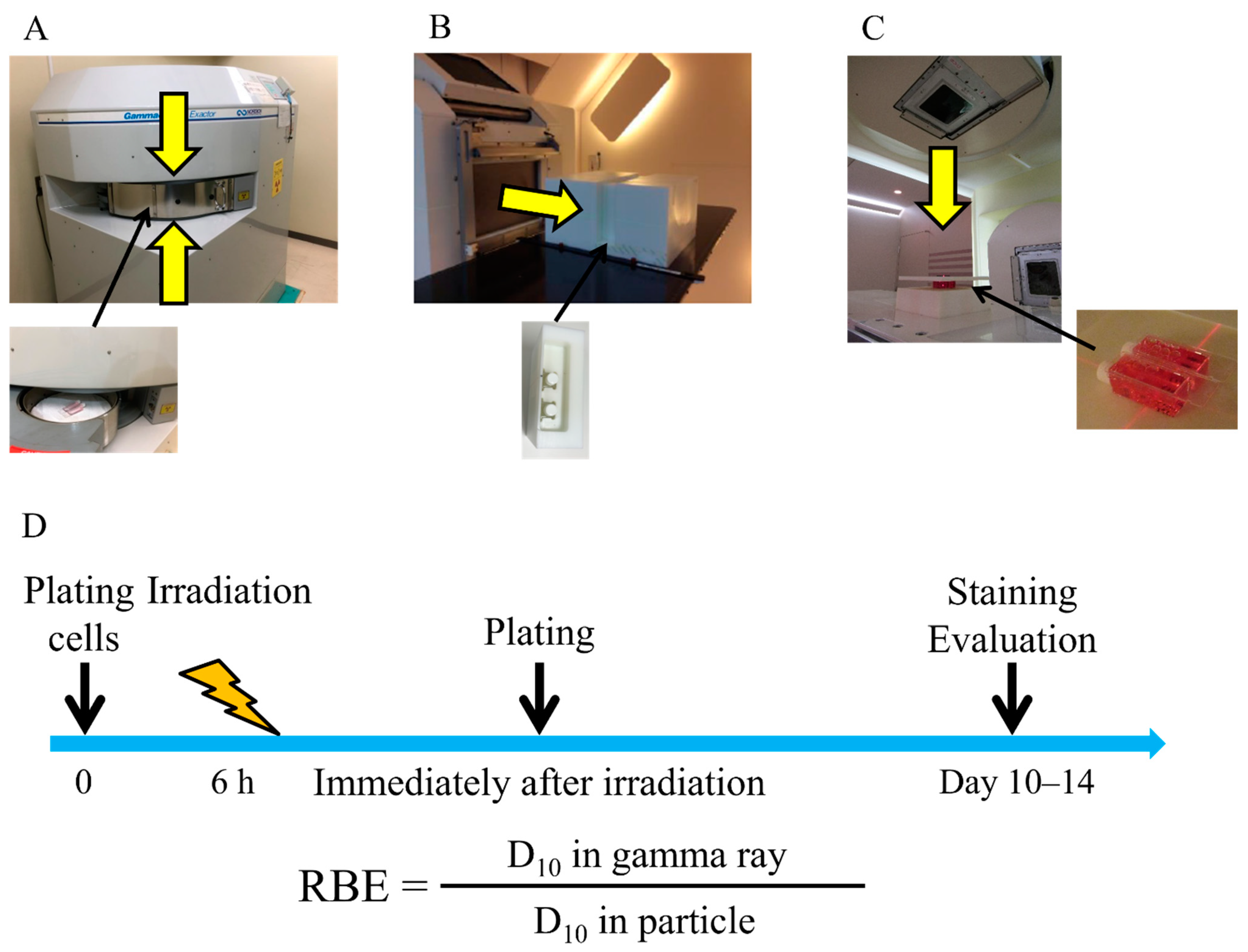
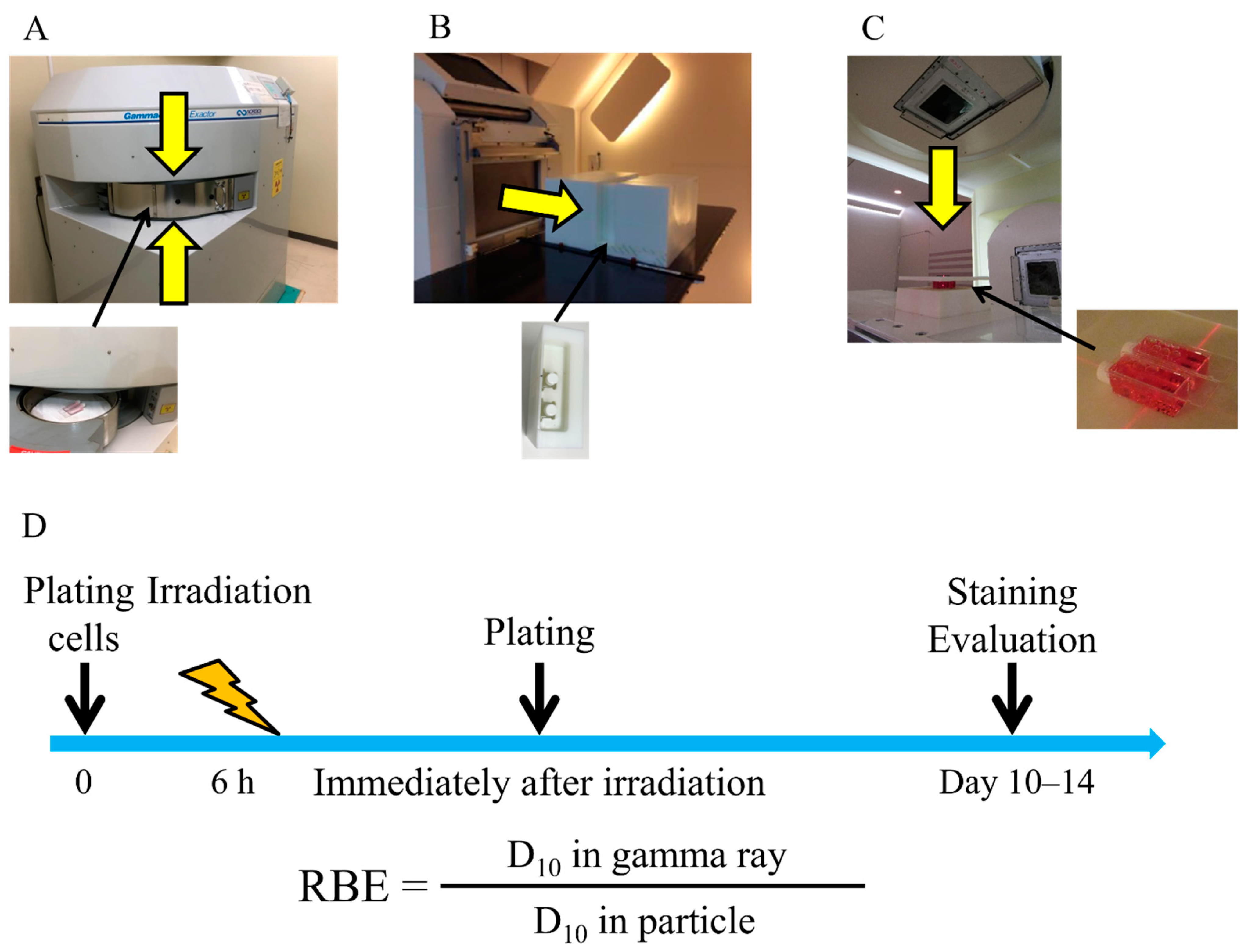
4.2. Irradiation
4.3. Colony Formation Assay
4.4. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamada, T. Clinical evidence of particle beam therapy (carbon). Int. J. Clin. Oncol. 2012, 17, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Kamada, T.; Tsujii, H.; Blakely, E.A.; Debus, J.; De Neve, W.; Durante, M.; Jäkel, O.; Mayer, R.; Orecchia, R.; Pötter, R.; et al. Carbon ion radiotherapy in Japan: An assessment of 20 years of clinical experience. Lancet Oncol. 2015, 16, e93–e100. [Google Scholar] [CrossRef] [Green Version]
- Suit, H.; DeLaney, T.; Goldberg, S.; Paganetti, H.; Clasie, B.; Gerweck, L.; Niemierko, A.; Hall, E.; Flanz, J.; Hallman, J.; et al. Proton vs carbon ion beams in the definitive radiation treatment of cancer patients. Radiother. Oncol. 2010, 95, 3–22. [Google Scholar] [CrossRef] [PubMed]
- Ogata, T.; Teshima, T.; Kagawa, K.; Hishikawa, Y.; Takahashi, Y.; Kawaguchi, A.; Suzumoto, Y.; Nojima, K.; Furusawa, Y.; Matsuura, N. Particle irradiation suppresses metastatic potential of cancer cells. Cancer Res. 2005, 65, 113–120. [Google Scholar]
- Takahashi, Y.; Teshima, T.; Kawaguchi, N.; Hamada, Y.; Mori, S.; Madachi, A.; Ikeda, S.; Mizuno, H.; Ogata, T.; Nojima, K.; et al. Heavy ion irradiation inhibits in vitro angiogenesis even at sublethal dose. Cancer Res. 2003, 63, 4253–4257. [Google Scholar]
- Ogata, T.; Teshima, T.; Inaoka, M.; Minami, K.; Tsuchiya, T.; Isono, M.; Furusawa, Y.; Matsuura, N. Carbon ion irradiation suppresses metastatic potential of human non-small cell lung cancer A549 cells through the phosphatidylinositol-3-kinase/Akt signaling pathway. J. Radiat. Res. 2011, 52, 374–379. [Google Scholar] [CrossRef] [Green Version]
- Fujita, M.; Imadome, K.; Shoji, Y.; Isozaki, T.; Endo, S.; Yamada, S.; Imai, T. Carbon-Ion Irradiation Suppresses Migration and Invasiveness of Human Pancreatic Carcinoma Cells MIAPaCa-2 via Rac1 and RhoA Degradation. Int. J. Radiat. Oncol. 2015, 93, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Tinganelli, W.; Durante, M. Carbon Ion Radiobiology. Cancers 2020, 12, 3022. [Google Scholar] [CrossRef]
- Takahashi, Y.; Yasui, T.; Minami, K.; Tamari, K.; Hayashi, K.; Otani, K.; Seo, Y.; Isohashi, F.; Koizumi, M.; Ogawa, K. Carbon ion irradiation enhances the antitumor efficacy of dual immune checkpoint blockade therapy both for local and distant sites in murine osteosarcoma. Oncotarget 2019, 10, 633–646. [Google Scholar] [CrossRef] [Green Version]
- Marcus, D.; Lieverse, R.; Klein, C.; Abdollahi, A.; Lambin, P.; Dubois, L.; Yaromina, A. Charged Particle and Conventional Radiotherapy: Current Implications as Partner for Immunotherapy. Cancers 2021, 13, 1468. [Google Scholar] [CrossRef]
- Onishi, M.; Okonogi, N.; Oike, T.; Yoshimoto, Y.; Sato, H.; Suzuki, Y.; Kamada, T.; Nakano, T. High linear energy transfer carbon-ion irradiation increases the release of the immune mediator high mobility group box 1 from human cancer cells. J. Radiat. Res. 2018, 59, 541–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helm, A.; Tinganelli, W.; Simoniello, P.; Kurosawa, F.; Fournier, C.; Shimokawa, T.; Durante, M. Reduction of Lung Metastases in a Mouse Osteosarcoma Model Treated With Carbon Ions and Immune Checkpoint Inhibitors. Int. J. Radiat. Oncol. 2021, 109, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Matsunobu, A.; Imai, R.; Kamada, T.; Imaizumi, T.; Tsuji, H.; Tsujii, H.; Shioyama, Y.; Honda, H.; Tatezaki, S.-I.; for the Working Group for Bone and Soft Tissue Sarcomas. Impact of carbon ion radiotherapy for unresectable osteosarcoma of the trunk. Cancer 2012, 118, 4555–4563. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Tanaka, M.; Sugimoto, Y.; Takigawa, T.; Ozaki, T. Carbon-ion radiotherapy of spinal osteosarcoma with long-term follow. Eur. Spine J. 2015, 25, 113–117. [Google Scholar] [CrossRef]
- Karasawa, K.; Wakatsuki, M.; Kato, S.; Kiyohara, H.; Kamada, T.; the Working Group for Gynecological Tumors. Clinical trial of carbon ion radiotherapy for gynecological melanoma. J. Radiat. Res. 2014, 55, 343–350. [Google Scholar] [CrossRef] [Green Version]
- Calipel, A.; Lux, A.-L.; Guerin, S.L.; Lefaix, J.-L.; Laurent, C.; Bernaudin, M.; Mouriaux, F. Differential Radiosensitivity of Uveal Melanoma Cell Lines After X-rays or Carbon Ions Radiation. Investig. Opthalmol. Vis. Sci. 2015, 56, 3085–3094. [Google Scholar] [CrossRef]
- Karger, C.P.; Peschke, P. RBE and related modeling in carbon-ion therapy. Phys. Med. Biol. 2017, 63, 01TR02. [Google Scholar] [CrossRef]
- Fujitaka, S.; Fujii, Y.; Nihongi, H.; Nakayama, S.; Takashina, M.; Hamatani, N.; Tsubouchi, T.; Yagi, M.; Minami, K.; Ogawa, K.; et al. Physical and biological beam modeling for carbon beam scanning at Osaka Heavy Ion Therapy Center. J. Appl. Clin. Med. Phys. 2021, 22, 77–92. [Google Scholar] [CrossRef]
- Kanai, T.; Furusawa, Y.; Fukutsu, K.; Itsukaichi, H.; Eguchi-Kasai, K.; Ohara, H. Irradiation of Mixed Beam and Design of Spread-Out Bragg Peak for Heavy-Ion Radiotherapy. Radiat. Res. 1997, 147, 78. [Google Scholar] [CrossRef]
- Inaniwa, T.; Furukawa, T.; Kase, Y.; Matsufuji, N.; Toshito, T.; Matsumoto, Y.; Furusawa, Y.; Noda, K. Treatment planning for a scanned carbon beam with a modified microdosimetric kinetic model. Phys. Med. Biol. 2010, 55, 6721–6737. [Google Scholar] [CrossRef]
- Fowler, J.F. The linear-quadratic formula and progress in fractionated radiotherapy. Br. J. Radiol. 1989, 62, 679–694. [Google Scholar] [CrossRef] [PubMed]
- Kanai, T.; Endo, M.; Minohara, S.; Miyahara, N.; Koyama-Ito, H.; Tomura, H.; Matsufuji, N.; Futami, Y.; Fukumura, A.; Hiraoka, T.; et al. Biophysical characteristics of HIMAC clinical irradiation system for heavy-ion radiation therapy. Int. J. Radiat. Oncol. 1999, 44, 201–210. [Google Scholar] [CrossRef]
- Suzuki, M.; Kase, Y.; Yamaguchi, H.; Kanai, T.; Ando, K. Relative biological effectiveness for cell-killing effect on various human cell lines irradiated with heavy-ion medical accelerator in Chiba (HIMAC) carbon-ion beams. Int. J. Radiat. Oncol. 2000, 48, 241–250. [Google Scholar] [CrossRef]
- Belli, M.; Bettega, D.; Calzolari, P.; Cherubini, R.; Cuttone, G.; Durante, M.; Esposito, G.; Furusawa, Y.; Gerardi, S.; Gialanella, G.; et al. Effectiveness of Monoenergetic and Spread-Out Bragg Peak Carbon-Ions for Inactivation of Various Normal and Tumour Human Cell Lines. J. Radiat. Res. 2008, 49, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, T.; Scholz, U.; Elsässer, T.; Durante, M.; Scholz, M. Systematic analysis of RBE and related quantities using a database of cell survival experiments with ion beam irradiation. J. Radiat. Res. 2013, 54, 494–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, K.; Kase, Y. Biological characteristics of carbon-ion therapy. Int. J. Radiat. Biol. 2009, 85, 715–728. [Google Scholar] [CrossRef]
- Maeda, K.; Yasui, H.; Matsuura, T.; Yamamori, T.; Suzuki, M.; Nagane, M.; Nam, J.-M.; Inanami, O.; Shirato, H. Evaluation of the relative biological effectiveness of spot-scanning proton irradiation in vitro. J. Radiat. Res. 2016, 57, 307–311. [Google Scholar] [CrossRef] [Green Version]
- Gridley, D.S.; Pecaut, M.; Mao, X.W.; Wroe, A.J.; Luo-Owen, X. Biological Effects of Passive Versus Active Scanning Proton Beams on Human Lung Epithelial Cells. Technol. Cancer Res. Treat. 2015, 14, 81–98. [Google Scholar] [CrossRef] [Green Version]
- Mara, E.; Clausen, M.; Khachonkham, S.; Deycmar, S.; Pessy, C.; Dörr, W.; Kuess, P.; Georg, D.; Gruber, S. Investigating the impact of alpha/beta and LETd on relative biological effectiveness in scanned proton beams: An in vitro study based on human cell lines. Med. Phys. 2020, 47, 3691–3702. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Matsuura, T.; Wada, M.; Egashira, Y.; Nishio, T.; Furusawa, Y. Enhanced radiobiological effects at the distal end of a clinical proton beam: In vitro study. J. Radiat. Res. 2014, 55, 816–822. [Google Scholar] [CrossRef] [Green Version]
- Kagawa, K.; Murakami, M.; Hishikawa, Y.; Abe, M.; Akagi, T.; Yanou, T.; Kagiya, G.; Furusawa, Y.; Ando, K.; Nojima, K.; et al. Preclinical biological assessment of proton and carbon ion beams at Hyogo Ion Beam Medical Center. Int. J. Radiat. Oncol. 2002, 54, 928–938. [Google Scholar] [CrossRef]
- Chevalier, F.; Hamdi, D.H.; Lepleux, C.; Temelie, M.; Nicol, A.; Austry, J.B.; Lesueur, P.; Vares, G.; Savu, D.; Nakajima, T.; et al. High LET Radiation Overcomes In Vitro Resistance to X-rays of Chondrosarcoma Cell Lines. Technol. Cancer Res. Treat. 2019, 18, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toratani, M.; Konno, M.; Asai, A.; Koseki, J.; Kawamoto, K.; Tamari, K.; Li, Z.; Sakai, D.; Kudo, T.; Satoh, T.; et al. A Convolutional Neural Network Uses Microscopic Images to Differentiate between Mouse and Human Cell Lines and Their Radioresistant Clones. Cancer Res. 2018, 78, 6703–6707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paganetti, H. Relative biological effectiveness (RBE) values for proton beam therapy. Variations as a function of biological endpoint, dose, and linear energy transfer. Phys. Med. Biol. 2014, 59, R419–R472. [Google Scholar] [CrossRef] [PubMed]
- Furusawa, Y.; Fukutsu, K.; Aoki, M.; Itsukaichi, H.; Eguchikasai, K.; Ohara, H.; Yatagai, F.; Kanai, T.; Ando, K. Inactivation of Aerobic and Hypoxic Cells from Three Different Cell Lines by Accelerated 3He-, 12C- and 20Ne-Ion Beams. Radiat. Res. 2000, 154, 485–496. [Google Scholar] [CrossRef]
- Held, K.D.; Kawamura, H.; Kaminuma, T.; Paz, A.E.S.; Yoshida, Y.; Liu, Q.; Willers, H.; Takahashi, A. Effects of charged particles on human tumor cells. Front. Oncol. 2016, 6, 23. [Google Scholar] [CrossRef] [Green Version]
- Hauswald, H.; Rieken, S.; Dienemann, H.C.; Thomas, M.; Kieser, M.; Debus, J.; Herfarth, K. Ion therapy within the trimodal management of superior sulcus tumors: The INKA trial. BMC Cancer 2015, 15, 192. [Google Scholar] [CrossRef] [Green Version]
- Oliphant, T.E. Python for Scientific Computing. Comput. Sci. Eng. 2007, 9, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Terpilowski, M. scikit-posthocs: Pairwise multiple comparison tests in Python. J. Open Source Softw. 2019, 4, 1169. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radiation | Sarcoma Cell Lines | Normal Cell Lines | ||||||
|---|---|---|---|---|---|---|---|---|
| MG63 | HT1080 | SW872 | SW1353 | HDF | hTERT-HME1 | NuLi-1 | ||
| α-value | Gamma ray | 0.253 ± 0.0113 | 0.234 ± 0.0458 | 0.498 ± 0.115 | 0.660 ± 0.0448 | 0.568 ± 0.0506 | 0.254 ± 0.00973 | 0.133 ± 0.0750 |
| Proton | 0.448 ± 0.0519 | 0.122 ± 0.0265 | 0.492 ± 0.0190 | 0.627 ± 0.0231 | 0.568 ± 0.0370 | 0.221 ± 0.0264 | 0.199 ± 0.0641 | |
| Carbon | 0.765 ± 0.149 | 0.607 ± 0.142 | 1.46 ± 0.272 | 1.43 ± 0.133 | 1.25 ± 0.0435 | 0.569 ± 0.0306 | 1.15 ± 0.0709 | |
| p-value | Gamma ray vs. Proton | <0.05 | 0.46 | 0.90 | 0.90 | 0.90 | 0.42 | 0.63 |
| Gamma ray vs. Carbon | <0.01 | <0.05 | 0.12 | <0.01 | <0.01 | <0.01 | <0.01 | |
| Proton vs. Carbon | <0.05 | <0.01 | 0.12 | <0.01 | <0.01 | <0.01 | <0.01 | |
| β-value | Gamma ray | 0.0503 ± 0.00598 | 0.0176 ± 0.00480 | 0.0153 ± 0.0242 | 0.00831 ± 0.00723 | 0.0211 ± 0.00749 | 0.0170 ± 0.00116 | 0.0672 ± 0.0130 |
| Proton | 0.0488 ± 0.00852 | 0.0322 ± 0.00303 | 0.0228 ± 0.00376 | 0.0157 ± 0.00879 | 0.0396 ± 0.00499 | 0.0261 ± 0.00380 | 0.0817 ± 0.00457 | |
| Carbon | 0.0774 ± 0.0151 | 0.0165 ± 0.0219 | −0.0165 ± 0.0587 | −0.0606 ± 0.0323 | −0.0134 ± 0.0143 | 0.0134 ± 0.00524 | 0.0184 ± 0.0369 | |
| p-value | Gamma ray vs. Proton | 0.90 | 0.12 | 0.90 | 0.90 | 0.22 | 0.12 | 0.52 |
| Gamma ray vs. Carbon | 0.12 | 0.77 | 0.77 | <0.05 | <0.05 | 0.64 | 0.28 | |
| Proton vs. Carbon | 0.28 | 0.77 | 0.77 | <0.05 | <0.01 | <0.05 | 0.12 | |
| D10(Gy) | Gamma ray | 4.72 ± 0.259 | 6.58 ± 0.230 | 4.10 ± 0.145 | 3.35 ± 0.128 | 3.58 ± 0.124 | 6.36 ± 0.0321 | 4.94 ± 0.0975 |
| Proton | 3.67 ± 0.114 | 6.80 ± 0.437 | 3.96 ± 0.0258 | 3.39 ± 0.0696 | 3.29 ± 0.0824 | 6.06 ± 0.0371 | 4.23 ± 0.214 | |
| Carbon | 2.44 ± 0.298 | 3.46 ± 0.310 | 1.62 ± 0.204 | 1.74 ± 0.129 | 1.89 ± 0.0321 | 3.72 ± 0.0614 | 1.95 ± 0.0402 | |
| p-value | Gamma ray vs. Proton | <0.05 | 0.78 | 0.62 | 0.90 | <0.05 | <0.01 | <0.01 |
| Gamma ray vs. Carbon | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | |
| Proton vs. Carbon | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | |
| RBE | Proton | 1.29 ± 0.0396 | 0.972 ± 0.0652 | 1.04 ± 0.00674 | 0.989 ± 0.0202 | 1.09 ± 0.0271 | 1.05 ± 0.00640 | 1.17 ± 0.0572 |
| Carbon | 1.96 ± 0.229 | 1.92 ± 0.162 | 2.56 ± 0.318 | 1.94 ± 0.138 | 1.90 ± 0.0327 | 1.71 ± 0.0280 | 2.54 ± 0.0531 | |
| p-value | Proton vs. Carbon | 0.05 | <0.01 | <0.05 | <0.01 | <0.01 | <0.01 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yagi, M.; Takahashi, Y.; Minami, K.; Matsuura, T.; Nam, J.-M.; Onodera, Y.; Akagi, T.; Maeda, T.; Okimoto, T.; Shirato, H.; et al. A Consistent Protocol Reveals a Large Heterogeneity in the Biological Effectiveness of Proton and Carbon-Ion Beams for Various Sarcoma and Normal-Tissue-Derived Cell Lines. Cancers 2022, 14, 2009. https://doi.org/10.3390/cancers14082009
Yagi M, Takahashi Y, Minami K, Matsuura T, Nam J-M, Onodera Y, Akagi T, Maeda T, Okimoto T, Shirato H, et al. A Consistent Protocol Reveals a Large Heterogeneity in the Biological Effectiveness of Proton and Carbon-Ion Beams for Various Sarcoma and Normal-Tissue-Derived Cell Lines. Cancers. 2022; 14(8):2009. https://doi.org/10.3390/cancers14082009
Chicago/Turabian StyleYagi, Masashi, Yutaka Takahashi, Kazumasa Minami, Taeko Matsuura, Jin-Min Nam, Yasuhito Onodera, Takashi Akagi, Takuya Maeda, Tomoaki Okimoto, Hiroki Shirato, and et al. 2022. "A Consistent Protocol Reveals a Large Heterogeneity in the Biological Effectiveness of Proton and Carbon-Ion Beams for Various Sarcoma and Normal-Tissue-Derived Cell Lines" Cancers 14, no. 8: 2009. https://doi.org/10.3390/cancers14082009
APA StyleYagi, M., Takahashi, Y., Minami, K., Matsuura, T., Nam, J.-M., Onodera, Y., Akagi, T., Maeda, T., Okimoto, T., Shirato, H., & Ogawa, K. (2022). A Consistent Protocol Reveals a Large Heterogeneity in the Biological Effectiveness of Proton and Carbon-Ion Beams for Various Sarcoma and Normal-Tissue-Derived Cell Lines. Cancers, 14(8), 2009. https://doi.org/10.3390/cancers14082009