
Analysis of Molecular Biomarkers in Resected Early-Stage Non-Small Cells Lung Cancer: A Narrative Review

 ,
,  , , ,
, , ,  , ,
, , 

Abstract
:Simple Summary
Abstract
1. Introduction
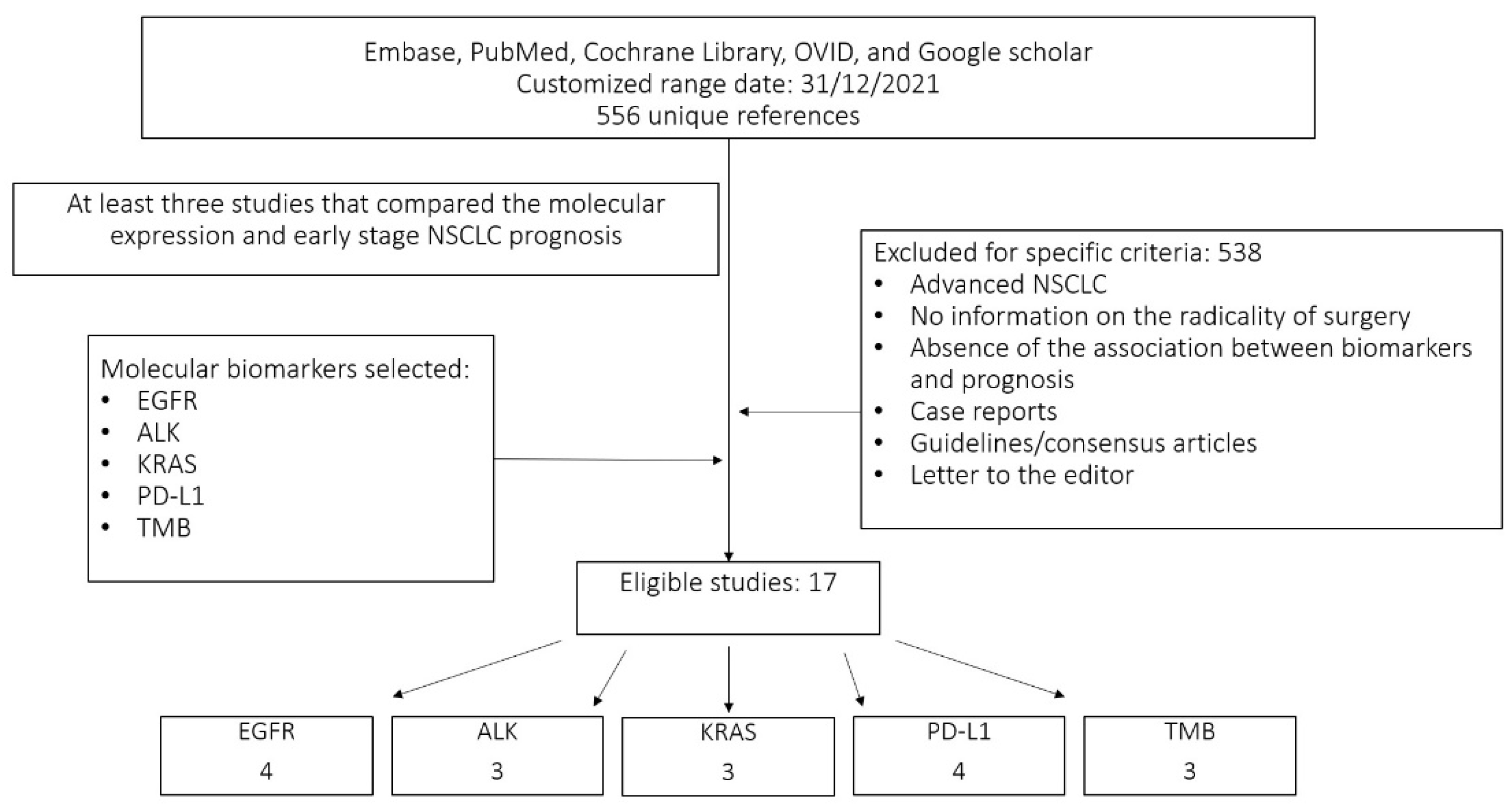
2. Materials and Methods
- (1)
- At least three studies associating the prognosis of early-stage NSCLC with specific molecular expression;
- (2)
- The study was a randomised control trial, prospective study, retrospective study or review article;
- (3)
- Presence of molecular analysis using NGS or PCR methods;
- (4)
- Patients underwent radical surgery for early-stage NSCLC;
- (5)
- An association between molecular expression and overall or disease-free survival.
- (1)
- No information regarding the radicality of the surgery;
- (2)
- Advanced NSCLC;
- (3)
- Absence of a specific association between biomarkers and prognosis;
- (4)
- Case reports;
- (5)
- Guidelines/consensus articles;
- (6)
- Letters to editors.
3. Results
3.1. Epidermal Growth Factor Receptor (EGFR)
3.2. Anaplastic Lymphoma Kinase (ALK)
3.3. Kirsten Rat Sarcoma (K-RAS)
3.4. Programmed Cell Death-Ligand 1 (PD-L1)
Tumour Mutational Burden (TMB)
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef] [PubMed]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; ESMO Guidelines Committee. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Paez, J.G.; Jänne, P.A.; Lee, J.C.; Tracy, S.; Greulich, H.; Gabriel, S.; Herman, P.; Kaye, F.J.; Lindeman, N.; Boggon, T.J.; et al. EGFR Mutations in Lung Cancer: Correlation with Clinical Response to Gefitinib Therapy. Science 2004, 304, 1497–1500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cagle, P.T.; Allen, T.C.; Olsen, R.J. Lung Cancer Biomarkers: Present Status and Future Developments. Arch. Pathol. Lab. Med. 2013, 137, 1191–1198. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.; Barlesi, F.; Lolkema, M.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: A report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- da Cunha Santos, G.; Shepherd, F.A.; Tsao, M.S. EGFR Mutations and Lung Cancer. Annu. Rev. Pathol. 2011, 6, 49–69. [Google Scholar] [CrossRef] [Green Version]
- Mitsudomi, T.; Kosaka, T.; Yatabe, Y. Biological and clinical implications of EGFR mutations in lung cancer. Int. J. Clin. Oncol. 2006, 11, 190–198. [Google Scholar] [CrossRef]
- Shigematsu, H.; Lin, L.; Takahashi, T.; Nomura, M.; Suzuki, M.; Wistuba, I.I.; Fong, K.; Lee, H.; Toyooka, S.; Shimizu, N.; et al. Clinical and Biological Features Associated with Epidermal Growth Factor Receptor Gene Mutations in Lung Cancers. JNCI J. Natl. Cancer Inst. 2005, 97, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Harrison, P.T.; Vyse, S.; Huang, P.H. Rare epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer. Semin. Cancer Biol. 2019, 61, 167–179. [Google Scholar] [CrossRef]
- Gristina, V.; Malapelle, U.; Galvano, A.; Pisapia, P.; Pepe, F.; Rolfo, C.; Tortorici, S.; Bazan, V.; Troncone, G.; Russo, A. The significance of epidermal growth factor receptor uncommon mutations in non-small cell lung cancer: A systematic review and critical appraisal. Cancer Treat. Rev. 2020, 85, 101994. [Google Scholar] [CrossRef]
- Wu, Y.L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef]
- Zhong, W.Z.; Wang, Q.; Mao, W.M.; Xu, S.T.; Wu, L.; Wei, Y.C.; Liu, Y.Y.; Chen, C.; Cheng, Y.; Yin, R.; et al. Gefitinib Versus Vinorelbine Plus Cisplatin as Adjuvant Treatment for Stage II-IIIA (N1-N2) EGFR-Mutant NSCLC: Final Overall Survival Analysis of CTONG1104 Phase III Trial. J. Clin. Oncol. 2021, 39, 713–722. [Google Scholar] [CrossRef]
- Kelly, K.; Altorki, N.K.; Eberhardt, W.E.E.; O’Brien, M.E.; Spigel, D.R.; Crinò, L.; Tsai, C.M.; Kim, J.H.; Cho, E.K.; Hoffman, P.C.; et al. Adjuvant Erlotinib Versus Placebo in Patients with Stage IB-IIIA Non–Small-Cell Lung Cancer (RADIANT): A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2015, 33, 4007–4014. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, T.; Zhang, J.; Cai, X.; Pan, C.; Long, Y.; Chen, J.; Zhou, C.; Yin, X. Prognostic Value of Epidermal Growth Factor Receptor Mutations in Resected Non-Small Cell Lung Cancer: A Systematic Review with Meta-Analysis. PLoS ONE 2014, 9, e106053. [Google Scholar] [CrossRef]
- Yang, X.N.; Yan, H.H.; Wang, J.; Chu, X.Y.; Liu, Z.D.; Shen, Y.; Ma, H.T.; Fu, X.N.; Hu, J.; Zhou, N.K.; et al. Real-World Survival Outcomes Based on EGFR Mutation Status in Chinese Patients with Lung Adenocarcinoma After Complete Resection: Results from the ICAN Study. JTO Clin. Res. Rep. 2021, 3, 100257. [Google Scholar] [CrossRef]
- Chen, S.; Yang, S.; Zhang, Y.; Xiang, J.; Zhang, Y.; Hu, H.; Sun, Y.; Fu, F.; Deng, C.; Wang, S.; et al. Clinicopathologic features and prognostic value of epidermal growth factor receptor mutation in patients with pT1a and pT1b invasive lung adenocarcinoma after surgical resection. J. Thorac. Dis. 2021, 13, 5496–5507. [Google Scholar] [CrossRef]
- Jao, K.; Tomasini, P.; Kamel-Reid, S.; Korpanty, G.J.; Mascaux, C.; Sakashita, S.; Labbé, C.; Leighl, N.B.; Liu, G.; Feld, R.; et al. The prognostic effect of single and multiple cancer-related somatic mutations in resected non-small-cell lung cancer. Lung Cancer 2018, 123, 22–29. [Google Scholar] [CrossRef]
- Saw, S.P.L.; Zhou, S.; Chen, J.; Lai, G.; Ang, M.K.; Chua, K.; Kanesvaran, R.; Ng, Q.S.; Jain, A.; Tan, W.L.; et al. Association of Clinicopathologic and Molecular Tumor Features with Recurrence in Resected Early-Stage Epidermal Growth Factor Receptor–Positive Non–Small Cell Lung Cancer. JAMA Netw. Open 2021, 4, e2131892. [Google Scholar] [CrossRef]
- Dagogo-Jack, I.; Gainor, J.F.; Porter, R.L.; Schultz, K.R.; Solomon, B.J.; Stevens, S.; Azzoli, C.G.; Sequist, L.V.; Lennes, I.T.; Shaw, A.T. Clinicopathologic Features of NSCLC Diagnosed During Pregnancy or the Peripartum Period in the Era of Molecular Genotyping. J. Thorac. Oncol. 2016, 11, 1522–1528. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.J.; Shaw, A.T. Recent Advances in Targeting ROS1 in Lung Cancer. J. Thorac. Oncol. 2017, 12, 1611–1625. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.A.; Hur, J.Y.; Kim, H.J.; Park, J.H.; Hwang, J.J.; Lee, S.A.; Lee, S.E.; Kim, W.S.; Lee, K.Y. Targeted Next-Generation Sequencing Analysis for Recurrence in Early-Stage Lung Adenocarcinoma. Ann. Surg. Oncol. 2020, 28, 3983–3993. [Google Scholar] [CrossRef]
- Dou, Y.; Duan, Q.; Qi, C.; Hou, L.; Wang, H. An intergenic region ALK fusion identified by DNA sequencing and validated by IHC in an early-stage lung adenocarcinoma. J. Cancer Res. Clin. Oncol. 2021, 147, 1865–1867. [Google Scholar] [CrossRef] [PubMed]
- Chaft, J.E.; Dagogo-Jack, I.; Santini, F.C.; Eng, J.; Yeap, B.Y.; Izar, B.; Chin, E.; Jones, D.R.; Kris, M.G.; Shaw, A.T.; et al. Clinical outcomes of patients with resected, early-stage ALK-positive lung cancer. Lung Cancer 2018, 122, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Lee, H.; Jeong, B.H.; Choi, Y.S.; Shin, M.H.; Kim, S.; Han, J.; Lee, K.S.; Shim, Y.M.; Kwon, O.J.; et al. Anaplastic lymphoma kinase rearrangement in surgically resected stage IA lung adenocarcinoma. J. Thorac. Dis. 2018, 10, 3460–3467. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Ahn, J.S.; Barlesi, F.; Dziadziuszko, R.; Nishio, M.; Shaw, A.T.; Bordogna, W.; Meyenberg, C.; Wu, Y.L. ALINA: A phase III study of alectinib versus chemotherapy as adjuvant therapy in patients with stage IB–IIIA anaplastic lymphoma kinase-positive (ALK+) non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2019, 37, TPS8569. [Google Scholar] [CrossRef]
- Govindan, R.; Mandrekar, S.J.; Gerber, D.; Oxnard, G.R.; Dahlberg, S.; Chaft, J.; Malik, S.; Mooney, M.; Abrams, J.S.; Jänne, P.A.; et al. ALCHEMIST Trials: A Golden Opportunity to Transform Outcomes in Early-Stage Non–Small Cell Lung Cancer. Clin. Cancer Res. 2015, 21, 5439–5444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabbò, F.; Novello, S. Expanding anaplastic lymphoma kinase therapeutic indication to early stage non-small cell lung cancer. Transl. Lung Cancer Res. 2019, 8, S290–S297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, H.; Christiani, D.C.; Mark, E.J.; Wiencke, J.K.; Wain, J.C.; Kelsey, K.T. Implications and Prognostic Value of K-ras Mutation for Early-Stage Lung Cancer in Women. JNCI J. Natl. Cancer Inst. 1999, 91, 2032–2038. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.; Soria, J.C.; Tang, X.; Xu, X.C.; Wang, L.; Mao, L.; Lotan, R.; Kemp, B.; Bekele, B.N.; Feng, L.; et al. Prognostic Factors in Resected Stage I Non–Small-Cell Lung Cancer: A Multivariate Analysis of Six Molecular Markers. J. Clin. Oncol. 2004, 22, 4575–4583. [Google Scholar] [CrossRef]
- Lin, M.W.; Wu, C.T.; Kuo, S.W.; Chang, Y.L.; Yang, P.C. Clinicopathology and Genetic Profile of Synchronous Multiple Small Adenocarcinomas: Implication for Surgical Treatment of an Uncommon Lung Malignancy. Ann. Surg. Oncol. 2014, 21, 2555–2562. [Google Scholar] [CrossRef]
- Azzoli, C.G. Practical Value of Molecular Pathology in Stage I–III Lung Cancer: Implications for the Clinical Surgeon. Ann. Surg. Oncol. 2015, 22, 3459–3465. [Google Scholar] [CrossRef]
- Meng, D.; Yuan, M.; Li, X.; Chen, L.; Yang, J.; Zhao, X.; Ma, W.; Xin, J. Prognostic value of K-RAS mutations in patients with non-small cell lung cancer: A systematic review with meta-analysis. Lung Cancer 2013, 81, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, Activity, and Immune Correlates of Anti-PD-1 Antibody in Cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef]
- Gettinger, S.N.; Horn, L.; Gandhi, L.; Spigel, D.R.; Antonia, S.J.; Rizvi, N.A.; Powderly, J.D.; Heist, R.S.; Carvajal, R.D.; Jackman, D.M.; et al. Overall Survival and Long-Term Safety of Nivolumab (Anti–Programmed Death 1 Antibody, BMS-936558, ONO-4538) in Patients with Previously Treated Advanced Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2015, 33, 2004–2012. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [Green Version]
- E Reuss, J.; Anagnostou, V.; Cottrell, T.R.; Smith, K.N.; Verde, F.; Zahurak, M.; Lanis, M.; Murray, J.C.; Chan, H.Y.; McCarthy, C.; et al. Neoadjuvant nivolumab plus ipilimumab in resectable non-small cell lung cancer. J. Immunother. Cancer 2020, 8, e001282. [Google Scholar] [CrossRef]
- Okuma, Y.; Hosomi, Y.; Nakahara, Y.; Watanabe, K.; Sagawa, Y.; Homma, S. High plasma levels of soluble programmed cell death ligand 1 are prognostic for reduced survival in advanced lung cancer. Lung Cancer 2017, 104, 1–6. [Google Scholar] [CrossRef]
- Cooper, W.A.; Tran, T.; Vilain, R.E.; Madore, J.; Selinger, C.I.; Kohonen-Corish, M.; Yip, P.; Yu, B.; O’Toole, S.A.; McCaughan, B.C.; et al. PD-L1 expression is a favorable prognostic factor in early stage non-small cell carcinoma. Lung Cancer 2015, 89, 181–188. [Google Scholar] [CrossRef]
- Shi, T.; Zhu, S.; Guo, H.; Li, X.; Zhao, S.; Wang, Y.; Lei, X.; Huang, D.; Peng, L.; Li, Z.; et al. The Impact of Programmed Death-Ligand 1 Expression on the Prognosis of Early Stage Resected Non-Small Cell Lung Cancer: A Meta-Analysis of Literatures. Front. Oncol. 2021, 11, 567978. [Google Scholar] [CrossRef]
- D’Arcangelo, M.; D’Incecco, A.; Ligorio, C.; Damiani, S.; Puccetti, M.; Bravaccini, S.; Terracciano, L.; Bennati, C.; Minuti, G.; Vecchiarelli, S.; et al. Programmed death ligand 1 expression in early stage, resectable non-small cell lung cancer. Oncotarget 2019, 10, 561–572. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.M.; Zhou, W.; Choi, Y.L.; Choi, S.J.; Kim, S.E.; Wang, Z.; Dolled-Filhart, M.; Emancipator, K.; Wu, D.; Weiner, R.; et al. Prognostic Significance of PD-L1 in Patients with Non–Small Cell Lung Cancer: A Large Cohort Study of Surgically Resected Cases. J. Thorac. Oncol. 2016, 11, 1003–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, B.; Schneidau, J. A serological comparison ofPhialophora verrucosa, Fonsecaea pedrosoiandCladosporium carrioniiusing immunodiffusion and immunoelectrophoresis. Med Mycol. 1970, 8, 217–226. [Google Scholar] [CrossRef]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non–small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Kris, M.G.; Gaspar, L.E.; Chaft, J.E.; Kennedy, E.B.; Azzoli, C.G.; Ellis, P.M.; Lin, S.H.; Pass, H.; Seth, R.; Shepherd, F.A.; et al. Adjuvant Systemic Therapy and Adjuvant Radiation Therapy for Stage I to IIIA Completely Resected Non–Small-Cell Lung Cancers: American Society of Clinical Oncology/Cancer Care Ontario Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 2960–2974. [Google Scholar] [CrossRef] [Green Version]
- Devarakonda, S.; Rotolo, F.; Tsao, M.; Lanc, I.; Brambilla, E.; Masood, A.; Olaussen, K.A.; Fulton, R.; Sakashita, S.; McLeer-Florin, A.; et al. Tumor Mutation Burden as a Biomarker in Resected Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 2995–3006. [Google Scholar] [CrossRef]
- Tian, Y.; Xu, J.; Chu, Q.; Duan, J.; Zhang, J.; Bai, H.; Yang, Z.; Fang, W.; Cai, L.; Wan, R.; et al. A novel tumor mutational burden estimation model as a predictive and prognostic biomarker in NSCLC patients. BMC Med. 2020, 18, 232. [Google Scholar] [CrossRef]
- Owada-Ozaki, Y.; Muto, S.; Takagi, H.; Inoue, T.; Watanabe, Y.; Fukuhara, M.; Yamaura, T.; Okabe, N.; Matsumura, Y.; Hasegawa, T.; et al. Prognostic Impact of Tumor Mutation Burden in Patients with Completely Resected Non–Small Cell Lung Cancer: Brief Report. J. Thorac. Oncol. 2018, 13, 1217–1221. [Google Scholar] [CrossRef] [Green Version]
- Qiu, B.; Guo, W.; Zhang, F.; Lv, F.; Ji, Y.; Peng, Y.; Chen, X.; Bao, H.; Xu, Y.; Shao, Y.; et al. Dynamic recurrence risk and adjuvant chemotherapy benefit prediction by ctDNA in resected NSCLC. Nat. Commun. 2021, 12, 6770. [Google Scholar] [CrossRef]
- Waldeck, S.; Mitschke, J.; Wiesemann, S.; Rassner, M.; Andrieux, G.; Deuter, M.; Mutter, J.; Lüchtenborg, A.; Kottmann, D.; Titze, L.; et al. Early assessment of circulating tumor DNA after curative-intent resection predicts tumor recurrence in early-stage and locally advanced non-small-cell lung cancer. Mol. Oncol. 2021, 16, 527–537. [Google Scholar] [CrossRef]
- Li, N.; Wang, B.; Li, J.; Shao, Y.; Li, M.; Kuang, P.; Liu, Z.; Sun, T.; Wu, H.; Ou, W.; et al. Perioperative circulating tumor DNA as a potential prognostic marker for operable stage I to IIIA non–small cell lung cancer. Cancer 2021, 128, 708–718. [Google Scholar] [CrossRef]


{kind=link}
| Study | Year | Kind of Study | Patients (Total/EGFR) | Stage | DFS | OS |
|---|---|---|---|---|---|---|
| Zhang et al. | 2014 | Meta-analysis | 3337 (n.r.) | I–III | n.s. 1 | n.s. |
| Yang et al. | 2021 | Retrospective | 476 (260) | I–III | n.s. | n.s. |
| Chen et al. | 2021 | Retrospective | 338 (216) | I | n.s. | positive |
| Jao et al. | 2018 | Retrospective | 214 (46) | I–III | Negative | n.s. |
| Study | Year | Kind of Study | Patients (Total/ALK) | Stage | DFS | OS |
|---|---|---|---|---|---|---|
| Kim et al. | 2021 | Retrospective | 203 (12) | I–II | negative | n.s. 1 |
| Chaft et al. | 2018 | Retrospective | 764 (29) | I–III | negative | n.s. |
| Shin et al. | 2018 | Retrospective | 309 (23) | I | negative | n.s. |
| Study | Year | Kind of Study | Patients (Total/K-Ras) | Stage | DFS | OS |
|---|---|---|---|---|---|---|
| Nelson et al. | 1999 | Prospective | 365 (44) | I–IV | n.r.* | negative |
| Lu et al. | 2004 | Retrospective | 94 (34) | I | n.s. | n.s. |
| Lin M-W et al. | 2014 | Retrospective | 64 (4) | I (syn) | n.s. | n.s. |
| Study | Year | Kind of Study | Patients | Cut-Off | Stage | DFS | OS |
|---|---|---|---|---|---|---|---|
| Cooper et al. | 2015 | Retrospective | 678 | ≥50% | I–III | n.r. 1 | positive |
| Shi et al. | 2021 | Retrospective | 3790 | variable | I–III | negative | negative |
| D’Arcangelo et al. | 2019 | Retrospective | 289 | ≥50% | I–III | n.s. | n.s. |
| Sum JM et al. | 2016 | Retrospective | 520 | 1–95%/≥96% | I–III | negative | n.s. |
| Study | Year | Kind of Study | Nr of Patients | DFS | OS |
|---|---|---|---|---|---|
| Devarakonda et al. | 2018 | Prospective | 908 | n.r.* | positive |
| Tian et al. | 2020 | Retrospective | 1026 | positive | n.s. |
| Owada-Ozaki et al. | 2018 | Retrospective | 90 | n.s. | negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallina, F.T.; Bertolaccini, L.; Forcella, D.; Mohamed, S.; Ceddia, S.; Melis, E.; Fusco, F.; Bardoni, C.; Marinelli, D.; Buglioni, S.; et al. Analysis of Molecular Biomarkers in Resected Early-Stage Non-Small Cells Lung Cancer: A Narrative Review. Cancers 2022, 14, 1949. https://doi.org/10.3390/cancers14081949
Gallina FT, Bertolaccini L, Forcella D, Mohamed S, Ceddia S, Melis E, Fusco F, Bardoni C, Marinelli D, Buglioni S, et al. Analysis of Molecular Biomarkers in Resected Early-Stage Non-Small Cells Lung Cancer: A Narrative Review. Cancers. 2022; 14(8):1949. https://doi.org/10.3390/cancers14081949
Chicago/Turabian StyleGallina, Filippo Tommaso, Luca Bertolaccini, Daniele Forcella, Shehab Mohamed, Serena Ceddia, Enrico Melis, Francesca Fusco, Claudia Bardoni, Daniele Marinelli, Simonetta Buglioni, and et al. 2022. "Analysis of Molecular Biomarkers in Resected Early-Stage Non-Small Cells Lung Cancer: A Narrative Review" Cancers 14, no. 8: 1949. https://doi.org/10.3390/cancers14081949
APA StyleGallina, F. T., Bertolaccini, L., Forcella, D., Mohamed, S., Ceddia, S., Melis, E., Fusco, F., Bardoni, C., Marinelli, D., Buglioni, S., Visca, P., Cappuzzo, F., Spaggiari, L., & Facciolo, F. (2022). Analysis of Molecular Biomarkers in Resected Early-Stage Non-Small Cells Lung Cancer: A Narrative Review. Cancers, 14(8), 1949. https://doi.org/10.3390/cancers14081949