
Phase 2 Trial (POLA Study) of Lurbinectedin plus Olaparib in Patients with Advanced Solid Tumors: Results of Efficacy, Tolerability, and the Translational Study

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Treatment
2.3. Outcomes
2.4. Translational Studies
2.4.1. DNA Extraction
2.4.2. Next-Generation Sequencing (NGS) Panel
2.4.3. Multiplex Ligation-Dependent Probe Amplification (MLPA) Analysis
2.5. Statistical Analysis
3. Results
3.1. Efficacy
3.2. Safety and Tolerability
3.3. Translational Studies
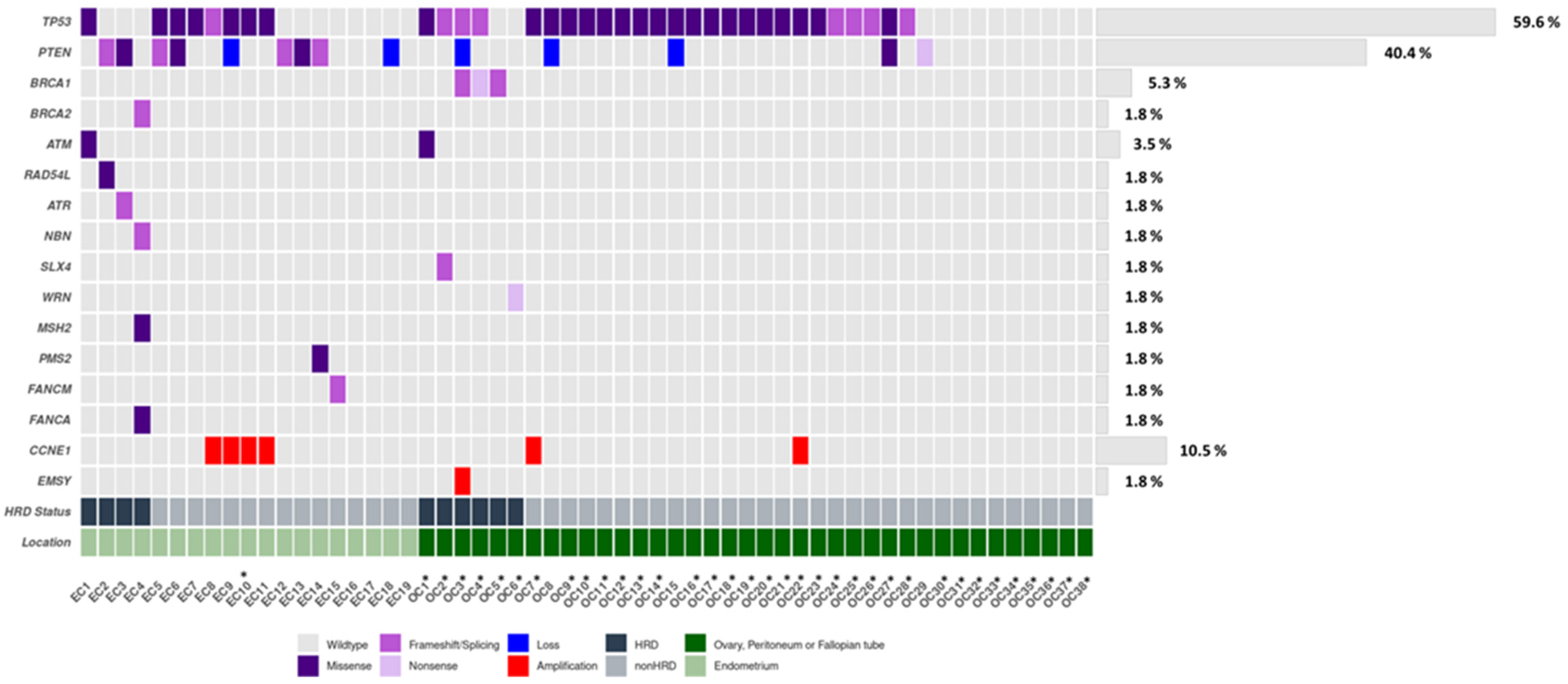
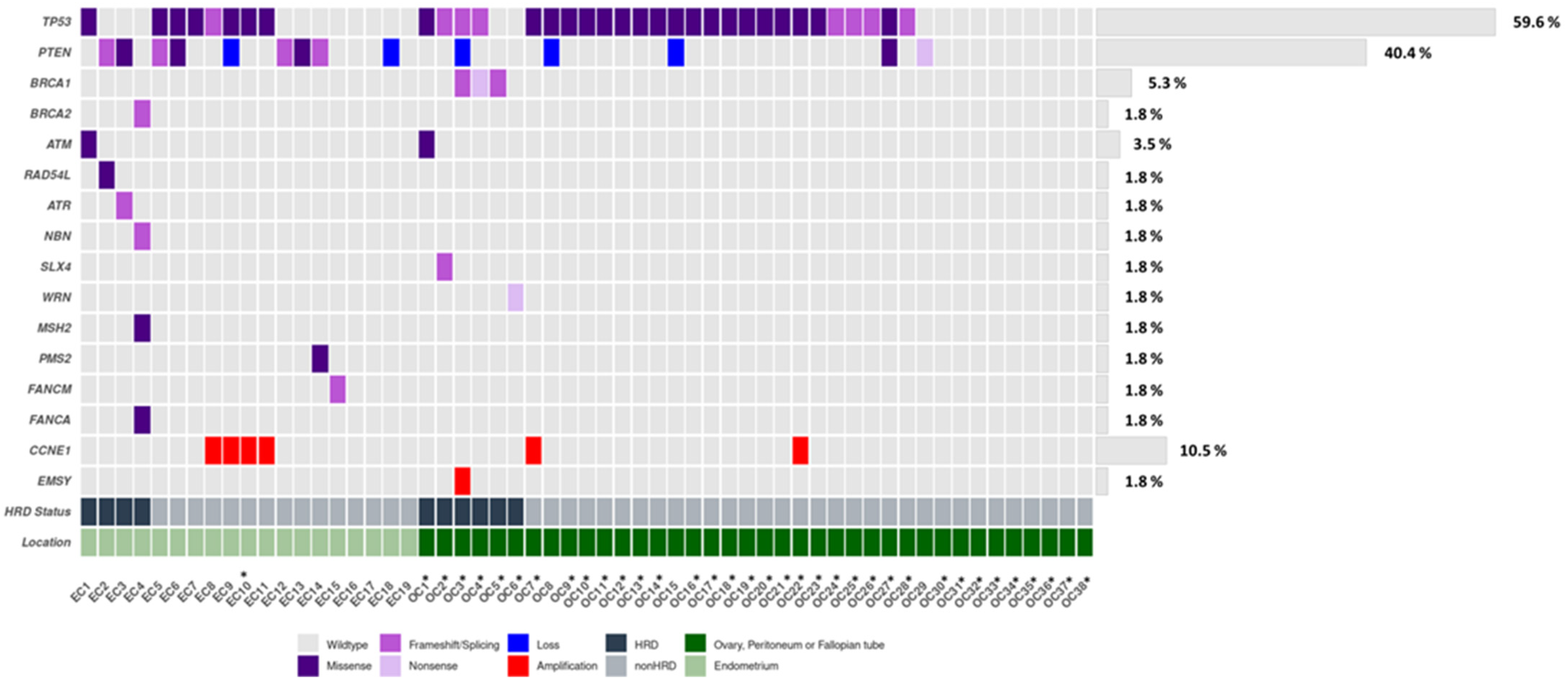
3.3.1. Distribution of Genetic Alterations and Clinical Impact
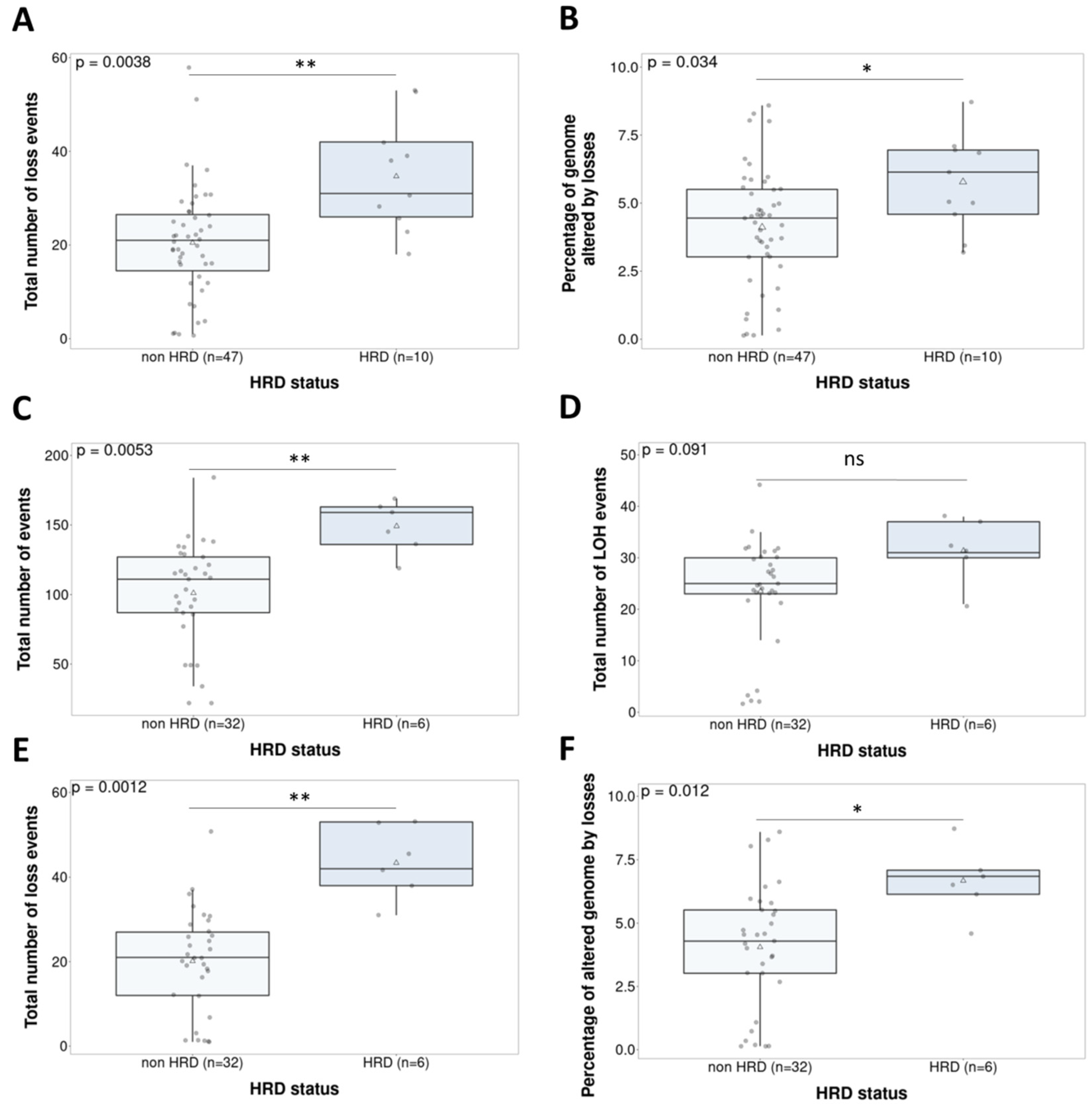
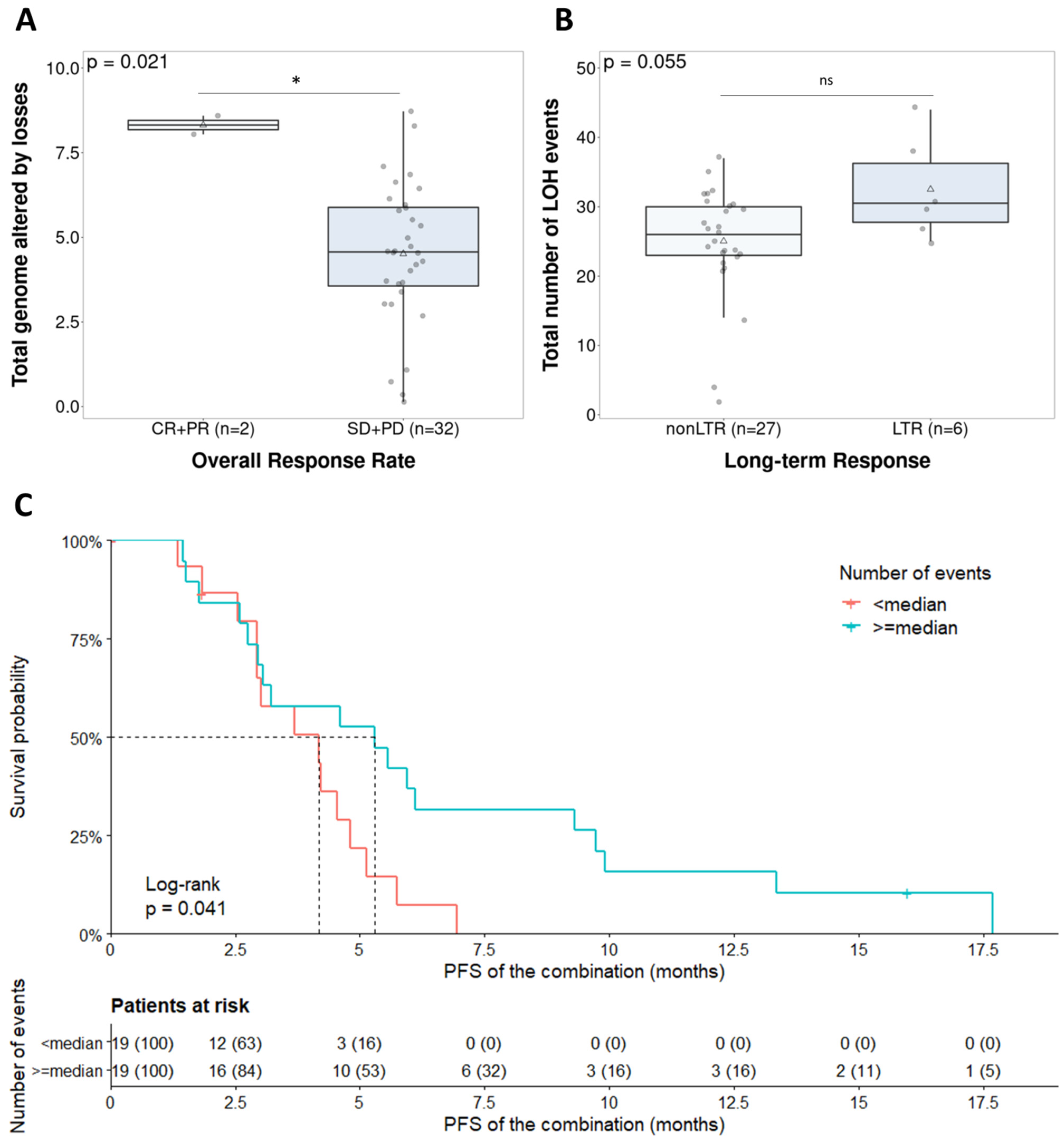
3.3.2. Characterization of Copy Number Patterns across the Clinical Trial Population: Clinical Impact of Genomic Instability-Based Classification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Fong, P.C.; Boss, D.S.; Yap, T.A.; Tutt, A.; Wu, P.; Mergui-Roelvink, M.; Mortimer, P.; Swaisland, H.; Lau, A.; O’Connor, M.J.; et al. Inhibition of Poly(ADP-Ribose) Polymerase in Tumors from BRCA Mutation Carriers. N. Engl. J. Med. 2009, 361, 123–134. [Google Scholar] [CrossRef] [Green Version]
- Gelmon, K.A.; Tischkowitz, M.; Mackay, H.; Swenerton, K.; Robidoux, A.; Tonkin, K.; Hirte, H.; Huntsman, D.; Clemons, M.; Gilks, B.; et al. Olaparib in patients with recurrent high-grade serous or poorly differentiated ovarian carcinoma or triple-negative breast cancer: A phase 2, multicentre, open-label, non-randomised study. Lancet Oncol. 2011, 12, 852–861. [Google Scholar] [CrossRef]
- Franzese, E.; Centonze, S.; Diana, A.; Carlino, F.; Guerrera, L.P.; Di Napoli, M.; De Vita, F.; Pignata, S.; Ciardiello, F.; Orditura, M. PARP inhibitors in ovarian cancer. Cancer Treat. Rev. 2019, 73, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujade-Lauraine, E.; Ledermann, J.A.; Selle, F.; Gebski, V.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Poveda, A.; Pignata, S.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1274–1284. [Google Scholar] [CrossRef] [Green Version]
- Mirza, M.R.; Monk, B.J.; Herrstedt, J.; Oza, A.M.; Mahner, S.; Redondo, A.; Fabbro, M.; Ledermann, J.A.; Lorusso, D.; Vergote, I.; et al. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N. Engl. J. Med. 2016, 375, 2154–2164. [Google Scholar] [CrossRef]
- Coleman, R.L.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.; Scambia, G.; et al. Rucaparib maintenance treatment for recurrent ovarian carcinoma after response to platinum therapy (ARIEL3): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 1949–1961. [Google Scholar] [CrossRef] [Green Version]
- Ledermann, J.A.; Pujade-Lauraine, E. Olaparib as maintenance treatment for patients with platinum-sensitive relapsed ovarian cancer. Ther. Adv. Med. Oncol. 2019, 11. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- Matulonis, U.A.; Monk, B.J. PARP inhibitor and chemotherapy combination trials for the treatment of advanced malignancies: Does a development pathway forward exist? Ann. Oncol. 2017, 28, 443–447. [Google Scholar] [CrossRef]
- Oza, A.M.; Cibula, D.; Benzaquen, A.O.; Poole, C.; Mathijssen, R.H.J.; Sonke, G.S.; Colombo, N.; Špaček, J.; Vuylsteke, P.; Hirte, H.; et al. Olaparib combined with chemotherapy for recurrent platinum-sensitive ovarian cancer: A randomised phase 2 trial. Lancet Oncol. 2015, 16, 87–97. [Google Scholar] [CrossRef]
- van der Noll, R.; Jager, A.; Ang, J.E.; Marchetti, S.; Mergui-Roelvink, M.W.J.; de Bono, J.S.; Lolkema, M.P.; de Jonge, M.J.A.; van der Biessen, D.A.; Brunetto, A.T.; et al. Phase I study of intermittent olaparib capsule or tablet dosing in combination with carboplatin and paclitaxel (part 2). Investig. New Drugs 2019, 38, 1096–1107. [Google Scholar] [CrossRef]
- Lampert, E.J.; Hays, J.L.; Kohn, E.C.; Annunziata, C.M.; Minasian, L.; Yu, M.; Gordon, N.; Sissung, T.M.; Chiou, V.L.; Figg, W.D.; et al. Phase I/Ib study of olaparib and carboplatin in heavily pretreated recurrent high-grade serous ovarian cancer at low genetic risk. Oncotarget 2019, 10, 2855–2868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Conte, G.; Sessa, C.; Von Moos, R.; Viganò, L.; Digena, T.; Locatelli, A.; Gallerani, E.; Fasolo, A.; Tessari, A.; Cathomas, R.; et al. Phase i study of olaparib in combination with liposomal doxorubicin in patients with advanced solid tumours. Br. J. Cancer 2014, 111, 651–659. [Google Scholar] [CrossRef] [Green Version]
- Gray, H.J.; Bell-McGuinn, K.; Fleming, G.F.; Cristea, M.; Xiong, H.; Sullivan, D.; Luo, Y.; McKee, M.D.; Munasinghe, W.; Martin, L.P. Phase I combination study of the PARP inhibitor veliparib plus carboplatin and gemcitabine in patients with advanced ovarian cancer and other solid malignancies. Gynecol. Oncol. 2018, 148, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.L.; Fleming, G.F.; Brady, M.F.; Swisher, E.M.; Steffensen, K.D.; Friedlander, M.; Okamoto, A.; Moore, K.N.; Efrat Ben-Baruch, N.; Werner, T.L.; et al. Veliparib with First-Line Chemotherapy and as Maintenance Therapy in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2403–2415. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.F.M.M.; Martínez-Díez, M.; García-Hernández, V.; Moneo, V.; Domingo, A.; Bueren-Calabuig, J.A.; Negri, A.; Gago, F.; Guillén-Navarro, M.J.; Avilés, P.; et al. PM01183, a new DNA minor groove covalent binder with potent in vitro and in vivo anti-tumour activity. Br. J. Pharmacol. 2010, 161, 1099–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belgiovine, C.; Bello, E.; Liguori, M.; Craparotta, I.; Mannarino, L.; Paracchini, L.; Beltrame, L.; Marchini, S.; Galmarini, C.M.; Mantovani, A.; et al. Lurbinectedin reduces tumour-associated macrophages and the inflammatory tumour microenvironment in preclinical models. Br. J. Cancer 2017, 117, 628–638. [Google Scholar] [CrossRef]
- Trigo, J.; Subbiah, V.; Besse, B.; Moreno, V.; López, R.; Sala, M.A.; Peters, S.; Ponce, S.; Fernández, C.; Alfaro, V.; et al. Lurbinectedin as second-line treatment for patients with small-cell lung cancer: A single-arm, open-label, phase 2 basket trial. Lancet Oncol. 2020, 21, 645–654. [Google Scholar] [CrossRef]
- Poveda, A.; Del Campo, J.M.; Ray-Coquard, I.; Alexandre, J.; Provansal, M.; Guerra Alía, E.M.; Casado, A.; Gonzalez-Martin, A.; Fernández, C.; Rodriguez, I.; et al. Phase II randomized study of PM01183 versus topotecan in patients with platinum-resistant/refractory advanced ovarian cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 1280–1287. [Google Scholar] [CrossRef]
- Gaillard, S.; Oaknin, A.; Ray-Coquard, I.; Vergote, I.; Scambia, G.; Colombo, N.; Fernandez, C.; Alfaro, V.; Kahatt, C.; Nieto, A.; et al. Lurbinectedin versus pegylated liposomal doxorubicin or topotecan in patients with platinum-resistant ovarian cancer: A multicenter, randomized, controlled, open-label phase 3 study (CORAIL). Gynecol. Oncol. 2021, 163, 237–245. [Google Scholar] [CrossRef]
- Ordóñez, J.L.; Amaral, A.T.; Carcaboso, A.M.; Herrero-Martín, D.; Del Carmen García-Macías, M.; Sevillano, V.; Alonso, D.; Pascual-Pasto, G.; San-Segundo, L.; Vila-Ubach, M.; et al. The PARP inhibitor olaparib enhances the sensitivity of Ewing sarcoma to trabectedin. Oncotarget 2015, 6, 18875–18890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ávila-Arroyo, S.; Nuñez, G.S.; García-Fernández, L.F.; Galmarini, C.M. Synergistic Effect of Trabectedin and Olaparib Combination Regimen in Breast Cancer Cell Lines. J. Breast Cancer 2015, 18, 329–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz, C.; Llop-Guevara, A.; Garber, J.E.; Arun, B.K.; Perez Fidalgo, J.A.; Lluch, A.; Telli, M.L.; Ferńandez, C.; Kahatt, C.; Galmarini, C.M.; et al. Multicenter phase II study of lurbinectedin in BRCAMutated and unselected metastatic advanced breast cancer and biomarker assessment substudy. J. Clin. Oncol. 2018, 36, 3134–3143. [Google Scholar] [CrossRef] [PubMed]
- Poveda, A.; Oaknin, A.; Romero, I.; Guerrero-Zotano, A.; Fariñas-Madrid, L.; Rodriguez-Freixinos, V.; Mallol, P.; Lopez-Reig, R.; Lopez-Guerrero, J.A. A phase I dose-finding, pharmacokinetics and genotyping study of olaparib and lurbinectedin in patients with advanced solid tumors. Sci. Rep. 2021, 11, 4433. [Google Scholar] [CrossRef] [PubMed]
- Povysil, G.; Tzika, A.; Vogt, J.; Haunschmid, V.; Messiaen, L.; Zschocke, J.; Klambauer, G.; Hochreiter, S.; Wimmer, K. panelcn.MOPS: Copy-number detection in targeted NGS panel data for clinical diagnostics. Hum. Mutat. 2017, 38, 889–897. [Google Scholar] [CrossRef]
- Talevich, E.; Shain, A.H.; Botton, T.; Bastian, B.C. CNVkit: Genome-Wide Copy Number Detection and Visualization from Targeted DNA Sequencing. PLoS Comput. Biol. 2016, 12, e1004873. [Google Scholar] [CrossRef]
- Telli, M.L.; Timms, K.M.; Tedi, J.; Hennessy, B.; Mills, G.B.; Jensen, K.C.; Szallasi, Z.; Barry, W.T.; Winer, E.P.; Tung, N.M.; et al. Homologous recombination deficiency (hrd) score predicts response to platinum-containing neoadjuvant chemotherapy in patients with triple-negative breast cancer. Clin. Cancer Res. 2016, 22, 3764–3773. [Google Scholar] [CrossRef] [Green Version]
- Davis, A.; Tinker, A.V.; Friedlander, M. “Platinum resistant” ovarian cancer: What is it, who to treat and how to measure benefit? Gynecol. Oncol. 2014, 133, 624–631. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: The AURELIA open-label randomized phase III trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef]
- Kaufman, B.; Shapira-Frommer, R.; Schmutzler, R.K.; Audeh, M.W.; Friedlander, M.; Balmaña, J.; Mitchell, G.; Fried, G.; Stemmer, S.M.; Hubert, A.; et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J. Clin. Oncol. 2015, 33, 244–250. [Google Scholar] [CrossRef]
- Perez-Fidalgo, J.A.; Cortés, A.; Guerra, E.; García, Y.; Iglesias, M.; Bohn Sarmiento, U.; Calvo García, E.; Manso Sánchez, L.; Santaballa, A.; Oaknin, A.; et al. Olaparib in combination with pegylated liposomal doxorubicin for platinum-resistant ovarian cancer regardless of BRCA status: A GEICO phase II trial (ROLANDO study). ESMO Open 2021, 6, 100212. [Google Scholar] [CrossRef] [PubMed]
- Madariaga, A.; Garg, S.; Tchrakian, N.; Dhani, N.C.; Jimenez, W.; Welch, S.; Mackay, H.; Ethier, J.-L.; Gilbert, L.; Rodriguez, A.; et al. Phase II trial assessing niraparib with or without dostarlimab (anti-PD-1) in recurrent endometrial carcinoma. J. Clin. Oncol. 2021, 39, 5574. [Google Scholar] [CrossRef]
- Tate Thigpen, J.; Brady, M.F.; Homesley, H.D.; Malfetano, J.; Dubeshter, B.; Burger, R.A.; Liao, S.; Mackey, D. Phase III trial of doxorubicin with or without cisplatin in advanced endometrial carcinoma: A gynecologic oncology group study. J. Clin. Oncol. 2004, 22, 3902–3908. [Google Scholar] [CrossRef]
- McMeekin, S.; Dizon, D.; Barter, J.; Scambia, G.; Manzyuk, L.; Lisyanskaya, A.; Oaknin, A.; Ringuette, S.; Mukhopadhyay, P.; Rosenberg, J.; et al. Phase III randomized trial of second-line ixabepilone versus paclitaxel or doxorubicin in women with advanced endometrial cancer. Gynecol. Oncol. 2015, 138, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Makker, V.; Colombo, N.; Herráez, A.C.; Santin, A.; Colomba, E.; Miller, D.; Fujiwara, K.; Pignata, S.; Baron-Hay, S.; Ray-Coquard, I.; et al. A multicenter, open-label, randomized, phase III study to compare the efficacy and safety of lenvatinib in combination with pembrolizumab versus treatment of physician’s choice in patients with advanced endometrial cancer. Gynecol. Oncol. 2021, 162, S4. [Google Scholar] [CrossRef]
- Moore, K.N.; Oza, A.M.; Colombo, N.; Oaknin, A.; Scambia, G.; Lorusso, D.; Konecny, G.E.; Banerjee, S.; Murphy, C.G.; Tanyi, J.L.; et al. Phase III, randomized trial of mirvetuximab soravtansine versus chemotherapy in patients with platinum-resistant ovarian cancer: Primary analysis of FORWARD I. Ann. Oncol. 2021, 32, 757–765. [Google Scholar] [CrossRef]
- Kristeleit, R.; Moreno, V.; Boni, V.; Guerra, E.M.; Kahatt, C.; Romero, I.; Calvo, E.; Basté, N.; López-Vilariño, J.A.; Siguero, M.; et al. Doxorubicin plus lurbinectedin in patients with advanced endometrial cancer: Results from an expanded phase I study. Int. J. Gynecol. Cancer 2021, 31, 1428–1436. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Lurbinectedin plus Olaparib, n = 73 Patients |
|---|---|
| Age, median (range), years | 65 (22–80) |
| Gender | |
| Females, n (%) | 73 (100) |
| ECOG PS, n (%) | |
| 0 | 40 (54.8) |
| 1 | 33 (45.2) |
| Primary tumor type, n (%) | |
| Ovarian carcinoma | 46 (63) |
| High-grade serous | 44 (60.3) |
| High-grade endometroid | 2 (2.7) |
| Endometrial carcinoma | 23 (31.5) |
| Endometrial carcinosarcoma | 3 (4.1) |
| Triple negative breast cancer | 1 (1.4) |
| Metastasis at baseline, n (%) | 27 (37) |
| Lung | 10 (37) |
| Liver | 5 (18.5) |
| Lymph nodes | 16 (59.3) |
| Bone | 1 (3.7) |
| Others | 12 (44.4) |
| Number of previous treatment regimens | |
| <3 treatments, n (%) | 28 (38.4) |
| ≥3 treatments, n (%) | 45 (61.6) |
| TEAE | Grade 1 | Grade 2 | Grade 3 | Grade 4 | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | |
| Anemia | 8 | (10.9) | 7 | (9.5) | 6 | (8.2) | 0 | (0) | 21 | (27.3) |
| Leukopenia | 3 | (4.1) | 5 | (6.8) | 3 | (4.1) | 0 | (0) | 11 | (15) |
| Neutropenia | 0 | (0) | 10 | (13.6) | 19 | (26) | 9 | (12.3) | 38 | (52) |
| Trombocytopenia | 4 | (5.4) | 2 | (2.7) | 2 | (2.7) | 1 | (1.3) | 9 | (12.3) |
| Abdominal pain | 14 | (19.0) | 10 | (13.6) | 2 | (2.7) | 0 | (0) | 26 | (35.3) |
| Constipation | 18 | (24.6) | 6 | (8.2) | 0 | (0) | 0 | (0) | 24 | (32.8) |
| Diarrhea | 15 | (20.5) | 4 | (5.4) | 1 | (1.3) | 0 | (0) | 20 | (27.3) |
| Dyspepsia | 3 | (4.1) | 2 | (2.7) | 0 | (0) | 0 | (0) | 5 | (6.8) |
| Nausea | 30 | (41) | 11 | (15) | 0 | (0) | 0 | (0) | 41 | (56.1) |
| Vomiting | 12 | (16.4) | 7 | (9.5) | 1 | (1.3) | 0 | (0) | 20 | (27.3) |
| Asthenia | 15 | (20.5) | 29 | (39.7) | 6 | (8.2) | 0 | (0.0) | 50 | (68.4) |
| Fatigue | 2 | (2.7) | 3 | (4.1) | 0 | (0) | 0 | (0) | 5 | (6.8) |
| Mucosal inflammation | 3 | (4.1) | 1 | (1.3) | 0 | (0) | 0 | (0) | 4 | (5.4) |
| Pyrexia | 9 | (12.3) | 1 | (1.3) | 0 | (0) | 0 | (0) | 10 | (13.6) |
| Bronchitis | 3 | (4.1) | 2 | (2.7) | 0 | (0) | 0 | (0) | 5 | (6.8) |
| Urinary tract infection | 1 | (1.3) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (1.3) |
| ALT/GPT increased | 4 | (5.4) | 1 | (1.3) | 1 | (1.3) | 0 | (0) | 6 | (8.1) |
| AST/GOT increased | 5 | (6.8) | 2 | (2.7) | 0 | (0) | 1 | (1.3) | 8 | (10.9) |
| GGT increased | 0 | (0) | 1 | (1.3) | 0 | (0) | 3 | (4.1) | 4 | (5.4) |
| Decreased appetite | 8 | (10.9) | 4 | (5.4) | 0 | (0) | 0 | (0) | 12 | (16.4) |
| Hypoalbuminaemia | 2 | (2.7) | 4 | (5.4) | 0 | (0) | 0 | (0) | 6 | (8.2) |
| Hypogamnesaemia | 7 | (9.5) | 0 | (0) | 0 | (0) | 0 | (0) | 7 | (9.5) |
| Artralgia | 4 | (5.4) | 1 | (1.3) | 0 | (0) | 0 | (0) | 5 | (6.8) |
| Back pain | 7 | (9.5) | 3 | (4.1) | 0 | (0) | 0 | (0) | 10 | (13.6) |
| Dizziness | 3 | (4.1) | 0 | (0) | 0 | (0) | 0 | (0) | 3 | (4.1) |
| Dysgeusia | 16 | (21.9) | 1 | (1.3) | 0 | (0) | 0 | (0) | 17 | (23.2) |
| Cough | 4 | (5.4) | 0 | (0) | 0 | (0) | 0 | (0) | 4 | (5.4) |
| Dyspnea | 6 | (8.2) | 4 | (5.4) | 1 | (1.3) | 0 | (0) | 11 | (15) |
| Pulmonary embolism | 1 | (1.3) | 1 | (1.3) | 4 | (4.5) | 0 | (0) | 6 | (8.2) |
| Lymphedema | 3 | (4.1) | 1 | (1.3) | 0 | (0) | 0 | (0) | 4 | (5.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poveda, A.; Lopez-Reig, R.; Oaknin, A.; Redondo, A.; Rubio, M.J.; Guerra, E.; Fariñas-Madrid, L.; Gallego, A.; Rodriguez-Freixinos, V.; Fernandez-Serra, A.; et al. Phase 2 Trial (POLA Study) of Lurbinectedin plus Olaparib in Patients with Advanced Solid Tumors: Results of Efficacy, Tolerability, and the Translational Study. Cancers 2022, 14, 915. https://doi.org/10.3390/cancers14040915
Poveda A, Lopez-Reig R, Oaknin A, Redondo A, Rubio MJ, Guerra E, Fariñas-Madrid L, Gallego A, Rodriguez-Freixinos V, Fernandez-Serra A, et al. Phase 2 Trial (POLA Study) of Lurbinectedin plus Olaparib in Patients with Advanced Solid Tumors: Results of Efficacy, Tolerability, and the Translational Study. Cancers. 2022; 14(4):915. https://doi.org/10.3390/cancers14040915
Chicago/Turabian StylePoveda, Andres, Raquel Lopez-Reig, Ana Oaknin, Andres Redondo, Maria Jesus Rubio, Eva Guerra, Lorena Fariñas-Madrid, Alejandro Gallego, Victor Rodriguez-Freixinos, Antonio Fernandez-Serra, and et al. 2022. "Phase 2 Trial (POLA Study) of Lurbinectedin plus Olaparib in Patients with Advanced Solid Tumors: Results of Efficacy, Tolerability, and the Translational Study" Cancers 14, no. 4: 915. https://doi.org/10.3390/cancers14040915
APA StylePoveda, A., Lopez-Reig, R., Oaknin, A., Redondo, A., Rubio, M. J., Guerra, E., Fariñas-Madrid, L., Gallego, A., Rodriguez-Freixinos, V., Fernandez-Serra, A., Juan, O., Romero, I., & Lopez-Guerrero, J. A. (2022). Phase 2 Trial (POLA Study) of Lurbinectedin plus Olaparib in Patients with Advanced Solid Tumors: Results of Efficacy, Tolerability, and the Translational Study. Cancers, 14(4), 915. https://doi.org/10.3390/cancers14040915