
Type of Recurrence, Cause of Death and Second Neoplasms among 737 Patients with Ductal Carcinoma In Situ of the Breast—15-Year Follow-Up

Abstract
:Simple Summary
Abstract
1. Introduction
2. Aim
3. Patients and Methods
3.1. Patients
3.2. Methods
3.3. Statistical Analysis
4. Results
4.1. Frequency and Type of Recurrence
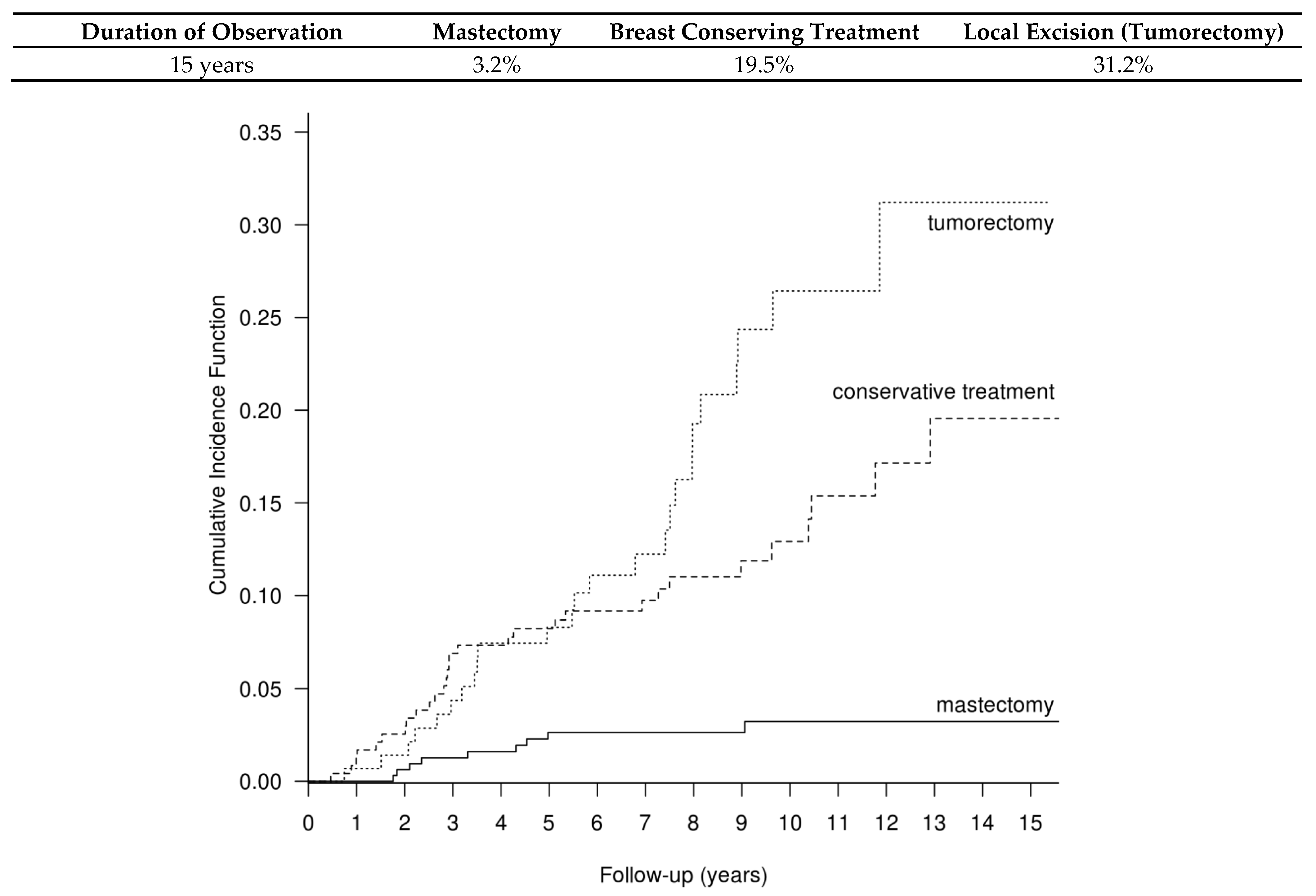
4.2. Cumulative Recurrence Risk
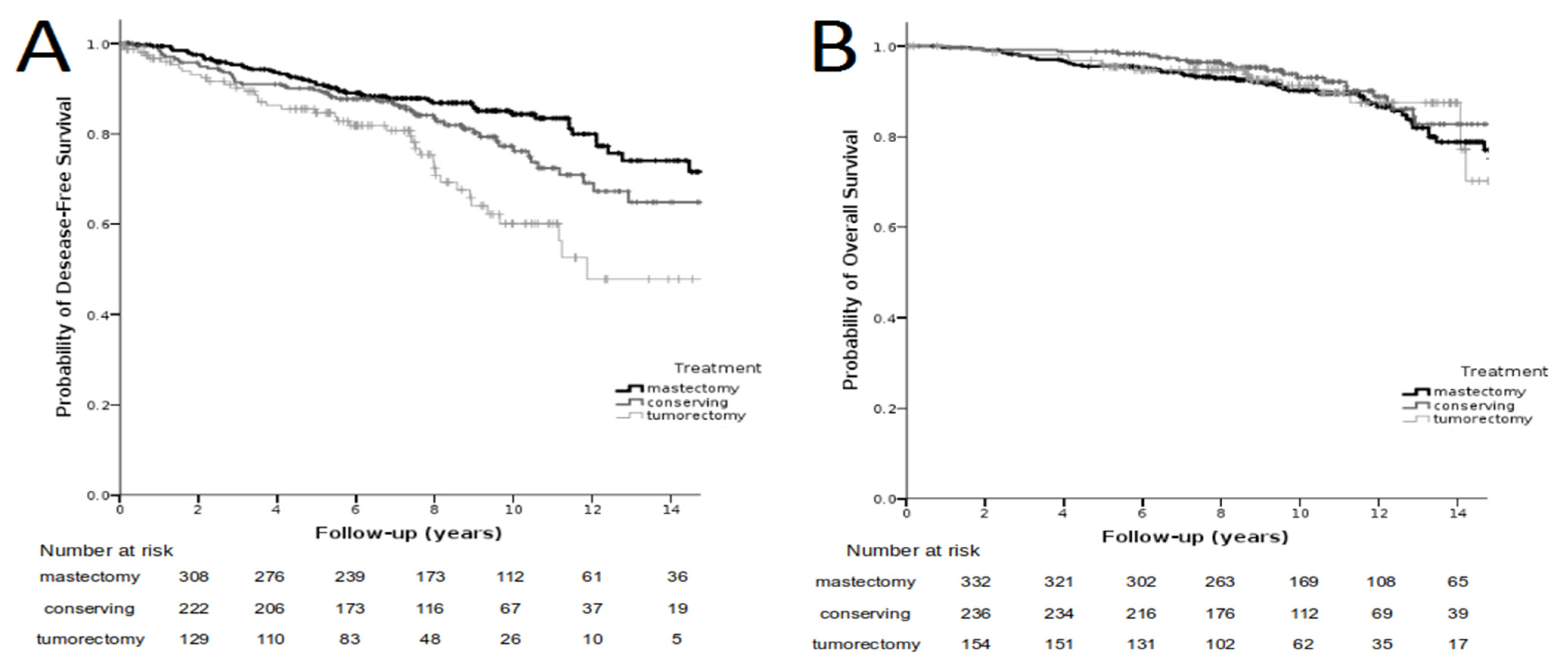
4.3. Disease-Free Survival (DFS)
4.4. Overall Survival (OS)
4.5. Cox Analysis
4.6. Other Neoplastic Lesions
4.7. Causes of Deaths
4.8. Characteristics of Four Patients Who Died Due to DCIS Recurrence
5. Discussion
5.1. Type of Recurrence
5.2. Relationship between Type of Treatment and Risk of DCIS Recurrence
5.3. Cause of Deaths: Does Recurrence Mean Death?
5.4. Other Neoplastic Lesions
5.5. Strengths and Limitations of the Study
6. Conclusions
- The highest recurrence rate was observed in low-risk patients treated with BCS without radiation therapy (31% during 15 years of observation). However, those patients were treated effectively irrespective of the type of the local recurrence (invasive or non-invasive), without influence on survival. No death due to breast cancer was detected in this group.
- The majority (79%) of local recurrences were true recurrences, localized in the tumor bed or up to 5 cm in the same quadrant. They did not differ from the initial DCIS in terms of the biological subtype. Of the recurrences, 58% were in the form of an invasive breast cancer or an invasive breast cancer with a DCIS component. Additionally, 10.5% (4/38) of patients with invasive breast cancer died.
- The rate of death in the whole treated group was 0.5%. Local recurrences (in the breast) detected in the form of DCIS and in the form of an invasive breast cancer were treated effectively without an impact on the overall survival. Invasive recurrences in the form of lymph node metastases or distant metastases (four cases, 10.5% of invasive recurrences) led to death, despite intensive salvage treatment. In those four cases, the time from the initial diagnosis of DCIS to the detection of an invasive recurrence depended on the biological subtype of DCIS.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kerlikowske, K. Epidemiology of ductal carcinoma in situ. J. Natl. Cancer Inst. Monogr. 2010, 41, 139–141. [Google Scholar] [CrossRef] [Green Version]
- Glover, J.A.; Bannon, F.J.; Hughes, C.M.; Cantwell, M.M.; Comber, H.; Gavin, A.; Deady, S.; Murray, L.J. Increased diagnosis and detection rates of carcinoma in situ of the breast. Breast Cancer Res. Treat. 2012, 133, 779–784. [Google Scholar] [CrossRef]
- Martínez-Pérez, C.; Turnbull, A.K.; Ekatah, G.E.; Arthur, L.M.; Sims, A.; Thomas, J.S.; Dixon, J.M. Current treatment trends and the need for better predictive tools in the management of ductal carcinoma in situ of the breast. Cancer Treat. Rev. 2017, 55, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Leonard, G.D.; Swain, S.M. Ductal carcinoma in situ, complexities and challenges. J. Natl. Cancer Inst. 2004, 96, 906–920. [Google Scholar] [CrossRef] [Green Version]
- Erbas, B.; Provenzano, E.; Armes, J.; Gertig, D. The natural history of ductal carcinoma in situ of the breast: A review. Breast Cancer Res. Treat. 2005, 97, 135–144. [Google Scholar] [CrossRef]
- Gorringe, K.; Fox, S.B. Ductal Carcinoma In Situ Biology, Biomarkers, and Diagnosis. Front. Oncol. 2017, 7, 248. [Google Scholar] [CrossRef] [Green Version]
- McCormick, B.; Winter, K.; Hudis, C.; Kuerer, H.M.; Rakovitch, E.; Smith, B.L.; Sneige, N.; Moughan, J.; Shah, A.; Germain, I.; et al. RTOG 9804, A Prospective Randomized Trial for Good-Risk Ductal Carcinoma In Situ Comparing Radiotherapy With Observation. J. Clin. Oncol. 2015, 33, 709–715. [Google Scholar] [CrossRef] [Green Version]
- Solin, L.J.; Gray, R.; Hughes, L.L.; Wood, W.C.; Lowen, M.A.; Badve, S.; Baehner, F.L.; Ingle, J.N.; Perez, E.A.; Recht, A.; et al. Surgical Excision Without Radiation for Ductal Carcinoma in Situ of the Breast: 12-Year Results From the ECOG-ACRIN E5194 Study. J. Clin. Oncol. 2015, 33, 3938–3944. [Google Scholar] [CrossRef] [Green Version]
- Silverstein, M.J.; Lagios, M.D. Treatment selection for patients with ductal carcinoma in situ (DCIS) of the breast using the University of Southern California/Van Nuys (USC/VNPI) Prognostic Index. Breast J. 2015, 21, 127–132. [Google Scholar] [CrossRef]
- Ben Wilkinson, J.; Vicini, F.A.; Shah, C.; Shaitelman, S.; Jawad, M.S.; Ye, H.; Kestin, L.L.; Goldstein, N.S.; Martinez, A.A.; Benitez, P.; et al. Twenty-Year Outcomes after Breast-Conserving Surgery and Definitive Radiotherapy for Mammographically Detected Ductal Carcinoma In Situ. Ann. Surg. Oncol. 2012, 19, 3785–3791. [Google Scholar] [CrossRef]
- Wapnir, I.L.; Dignam, J.J.; Fisher, B.; Mamounas, E.P.; Anderson, S.J.; Julian, T.B.; Land, S.R.; Margolese, R.G.; Swain, S.M.; Costantino, J.P. Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trias for DCIS. J. Natl. Cancer Inst. 2011, 103, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Donker, M.; Litière, S.; Werutsky, G.; Julien, J.P.; Fentiman, I.S.; Agresti, R.; Rouanet, P.; de Lara, C.T.; Bartelink, H.; Duez, N. Breast-conserving treatment with or without radiotherapy in ductal carcinoma in situ: 15-year recurrence rates and outcome after recurrence, from EORTC 10853 randomized chase III trial. J. Clin. Oncol. 2013, 31, 4054–4059. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, M.J. The University of Southern California/VanNuys Prognostic Index for ductal carcinoma in situ of the breast. Am. J. Surg 2003, 186, 337–343. [Google Scholar] [CrossRef]
- Goldstein, N.S.; Kestin, L.; Vicini, F. Intraductal Carcinoma of the Breast. Am. J. Surg. Pathol. 2000, 24, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Cutuli, B.; Bernier, J.; Poortmans, P. Radiotherapy in DCIS, an underestimated benefit? Radiother. Oncol. 2014, 112, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerlikowske, K.; Molinaro, A.M.; Gauthier, M.L.; Berman, H.K.; Waldman, F.; Bennington, J.; Sanchez, H.; Jimenez, C.; Stewart, K.; Chew, K.; et al. Biomarker expression and risk of subsequent tumors after initial ductal carcinoma in situ diagnosis. J. Natl. Cancer Inst. 2010, 102, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Rakovitch, E.; Nofech-Mozes, S.; Narod, S.A.; Hanna, W.; Thiruchelvam, D.; Saskin, R.; Taylor, C.; Tuck, A.; Sengupta, S.; Elavathil, L.; et al. Can we select individuals with low risk ductal carcinoma in situ (DCIS)? A population-based outcomes analysis. Breast Cancer Res. Treat. 2013, 138, 581–590. [Google Scholar] [CrossRef]
- Mamtani, A.; Nakhlis, F.; Downs-Canner, S.; Zabor, E.C.; Morrow, M.; King, T.A.; Ms, K.J.V.Z. Impact of Age on Locoregional and Distant Recurrence After Mastectomy for Ductal Carcinoma In Situ With or Without Microinvasion. Ann. Surg. Oncol. 2019, 26, 4264–4271. [Google Scholar] [CrossRef]
- Stuart, K.E.; Houssami, N.; Taylor, R.; Hayen, A.; Boyages, J. Long-term outcomes of ductal carcinoma in situ of the breast: A systematic review, meta-analysis and meta-regression analysis. BMC Cancer 2015, 15, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Shah, C.; Vicini, F.A.; Berry, S.; Julian, T.B.; Wilkinson, J.B.; Shaitelman, S.F.; Khan, A.; Finkelstein, S.E. Ductal carcinoma in situ of the breast: Evaluating the role of radiation therapy in the management and attempts to identify low-risk patients. Am. J. Clin. Oncol. 2015, 38, 526–533. [Google Scholar] [CrossRef] [Green Version]
- Kelley, L.; Silverstein, M.; Guerra, L. Analyzing the Risk of Recurrence after Mastectomy for DCIS: A New Use for the USC/Van Nuys Prognostic Index. Ann. Surg. Oncol. 2010, 18, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Bijker, N.; Peterse, J.L.; Duchateau, L.; Julien, J.-P.; Fentiman, I.S.; Duval, C.; Di Palma, S.; Simony-Lafontaine, J.; De Mascarel, I.; Van De Vijver, M.J. Risk Factors for Recurrence and Metastasis After Breast-Conserving Therapy for Ductal Carcinoma-In-Situ: Analysis of European Organization for Research and Treatment of Cancer Trial 10853. J. Clin. Oncol. 2001, 19, 2263–2271. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Burstein, H.; Winer, E.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.; Piccart-Gebhart, M.; Senn, H.-J.; et al. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann. Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Wärnberg, F.; Garmo, H.; Emdin, S.; Hedberg, V.; Adwall, L.; Sandelin, K.; Ringberg, A.; Karlsson, P.; Arnesson, L.-G.; Anderson, H.; et al. Effect of Radiotherapy After Breast-Conserving Surgery for Ductal Carcinoma in Situ: 20 Years Follow-Up in the Randomized SweDCIS Trial. J. Clin. Oncol. 2014, 32, 3613–3618. [Google Scholar] [CrossRef]
- Cuzick, J.; Sestak, I.; Pinder, S.E.; Ellis, I.O.; Forsyth, S.; Bundred, N.J.; Forbes, J.F.; Bishop, H.; Fentiman, I.S.; George, W.D. Effect of tamoxifen and radiotherapy in women with locally excised ductal carcinoma in situ: Long-term results from the UK/ANZ DCIS trial. Lancet Oncol. 2011, 12, 21–29. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG); Correa, C.; McGale, P.; Taylor, C.; Wang, Y.; Clarke, M.; Davies, C.; Peto, R.; Bijker, N.; Solin, L.; et al. Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast. J. Natl. Cancer Inst. Monogr. 2010, 41, 162–177. [Google Scholar]
- Goodwin, A.; Parker, S.; Ghersi, D.; Wilcken, N. Post-operative radiotherapy for ductal carcinoma in situ of the breast. Cochrane Database Syst. Rev. 2013, CD000563. [Google Scholar] [CrossRef] [Green Version]
- Garg, P.K.; Jakhetiya, A.; Pandey, R.; Chishi, N.; Pandey, D. Adjuvant radiotherapy versus observation following lumpectomy in ductal carcinoma in-situ: A meta-analysis of randomized controlled trials. Breast J. 2017, 233–239. [Google Scholar] [CrossRef]
- Warren, L.E.G.; Chen, Y.-H.; Halasz, L.M.; Brock, J.E.; Capuco, A.; Punglia, R.S.; Wong, J.S.; Golshan, M.; Bellon, J.R. Long-term outcomes of breast-conserving therapy for women with ductal carcinoma in situ. Breast Cancer Res. Treat. 2019, 178, 607–615. [Google Scholar] [CrossRef]
- Boyages, J.; Delaney, G.; Taylor, R. Predictors of local recurrence after treatment of ductal carcinoma in situ: A meta-analysis. Cancer 1999, 85, 616–628. [Google Scholar] [CrossRef]
- Giannakeas, V.; Sopik, V.; Narod, S.A. Association of a Diagnosis of Ductal Carcinoma In Situ With Death From Breast Can-cer. JAMA Network Open. 2020, 3, e2017124. [Google Scholar] [CrossRef] [PubMed]
- Narod, S.A.; Iqbal, J.; Giannakeas, V.; Sopik, V.; Sun, P. Breast Cancer Mortality After a Diagnosis of Ductal Carcinoma In Situ. JAMA Oncol. 2015, 1, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Worni, M.; Akushevich, I.; Greenup, R.; Sarma, D.; Ryser, M.D.; Myers, E.R.; Hwang, E.S. Trends in Treatment Patterns and Outcomes for Ductal Carcinoma In Situ. JNCI: J. Natl. Cancer Inst. 2015, 107, djv263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, W.; Sofie Lindström, L.; Hall, P.; Czene, K. Cause-specific mortality in women with breast cancer in situ. Int. J. Cancer 2017, 140, 2414–2421. [Google Scholar] [CrossRef]
- Sagara, Y.; Freedman, R.A.; Vaz-Luis, I.; Mallory, M.A.; Wong, S.M.; Aydogan, F.; DeSantis, S.; Barry, W.T.; Golshan, M. Patient Prognostic Score and Associations With Survival Improvement Offered by Radiotherapy After Breast-Conserving Surgery for Ductal Carcinoma In Situ: A Population-Based Longitudinal Cohort Study. J. Clin. Oncol. 2016, 34, 1190–1196. [Google Scholar] [CrossRef]
- Elshof, L.E.; Schmidt, M.; Rutgers, E.J.; van Leeuwen, F.E.; Wesseling, J.; Schaapveld, M. Cause-specific Mortality in a Population-based Cohort of 9799 Women Treated for Ductal Carcinoma In Situ. Ann. Surg. 2018, 267, 952–958. [Google Scholar] [CrossRef] [Green Version]
- Viani, G.A.; Stefano, E.J.; Afonso, S.L.; De Fendi, L.I.; Soares, F.V.; Leon, P.G.; Guimarães, F.S. Breast-conserving surgery with or without radiotherapy in women with ductal carcinoma in situ: A meta-analysis of randomized trials. Radiat. Oncol. 2007, 2, 28–39. [Google Scholar] [CrossRef] [Green Version]
- Shaaban, A.M.; Hilton, B.; Clements, K.; Provenzano, E.; Cheung, S.; Wallis, M.G.; Sawyer, E.; Thomas, J.S.; Hanby, A.M.; Pinder, S.E.; et al. Pathological features of 11,337 patients with primary ductal carcinoma in situ (DCIS) and subsequent events: Results from the UK Sloane Project. Br. J. Cancer 2020, 124, 1009–1017. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Feature | Total 737 Patients (%) | Mastectomy 337 Patients (%) | BCT * 241 Patients (%) | BCS ** 159 Patients (%) |
|---|---|---|---|---|
| Age (years) | ||||
| <40 | 29 (4) | 19 (6) | 7 (3) | 3 (2) |
| 40–50 | 142 (19) | 64 (19) | 49 (20) | 29 (18) |
| 51–60 | 293 (40) | 123 (36) | 110 (46) | 60 (38) |
| >60 | 273 (37) | 131 (39) | 75 (31) | 67 (42) |
| Method of DCIS diagnosis | ||||
| Mammography alone Clinically explicit | 643 (87) | 275 (82) | 228 (95) | 140 (88) |
| 94 (13) | 62 (18) | 13 (5) | 19 (12) | |
| DCIS size on mammography (cm) | ||||
| <1 | 246 (33) | 73 (22) | 96 (40) | 77 (49) |
| 1.1–2.5 | 249 (34) | 78 (23) | 104 (44) | 67 (42) |
| 2.6–4 | 123 (17) | 84 (25) | 26 (10) | 13 (8) |
| >4 | 119 (16) | 102 (30) | 15 (6) | 2 (1) |
| DCIS size on histopathological examination (cm) | ||||
| <1 | 278 (38) | 58 (17) | 98 (41) | 122 (77) |
| 1.1–2.5 | 238 (32) | 89 (26) | 117 (48) | 32 (20) |
| 2.6–4 | 97 (13) | 70 (21) | 22 (9) | 5 (3) |
| >4 | 124 (17) | 120 (36) | 4 (2) | 0 |
| The narrowest margin (mm) | ||||
| <1 | 0 | 0 | 0 | 0 |
| 1–2 | 232 (32) | 143 (43) | 30 (12) | 59 (37) |
| 3–9 | 129 (17) | 110 (33) | 2 (1) | 17 (11) |
| ≥10 | 376 (51) | 84 (25) | 209 (87) | 83 (52) |
| Histological malignancy grade | ||||
| NG1 | 151 (20) | 40 (12) | 33 (14) | 78 (49) |
| NG2 | 296 (40) | 155 (46) | 89 (36) | 53 (33) |
| NG3 | 290 (40) | 142 (42) | 119 (50) | 28 (18) |
| Comedo necrosis | ||||
| Present | 271 (37) | 119 (35) | 119 (49) | 33 (21) |
| Absent | 466 (63) | 218 (65) | 122 (51) | 126 (79) |
| Feature | Number of Patients with Recurrence (%) | ||
|---|---|---|---|
| Character of recurrence | |||
| Local recurrence | 61/737 (8) | ||
| Metastases to lymph nodes | 4/737 (0.5) | ||
| Distant metastases (liver and bones) | 1/737 (0.1) | ||
| Location of local recurrence | |||
| Recurrence in the tumor bed | 32/61 (53) | 79% true recurrences | |
| Recurrence in the same quadrant | 16/61 (26) | ||
| Recurrence in another breast quadrant | 13/61 (21) | 21% likely another primary breast cancer | |
| Histological type of the recurrence | |||
| DCIS | 28/66 (42) | ||
| DCIS + invasive cancer | 31/66 (47) | 58% recurrences in the form of invasive cancer | |
| Invasive cancer | 7/66 (11) | ||
| Biological type of the recurrence * | |||
| ER−PR−HER2− | 5/66 (8) | ||
| ER−PR−HER2+ | 12/66 (18) | 29% HER2+ cancers | |
| ER/PR+HER2+ | 7/66 (11) | 74% luminal cancers | |
| Luminal A | 30/66 (45) | 63% luminal HER2-negative cancers | |
| Luminal B | 12/66 (18) | ||
| Feature | Mastectomy Number of pts (%) | BCT Number of pts (%) | BCS Number of pts (%) |
|---|---|---|---|
| Number of patients | 337 | 241 | 159 |
| Recurrences | |||
| Yes | 9 (2.6) | 32 (13.2) | 25 (15.7) |
| No | 328 (97) | 209 (87) | 134 (84) |
| Histological type of the recurrence | |||
| DCIS | 0 | 15/32 (47) | 11/25 (44) |
| DCIS + inv. cancer * | 0 | 11/32 (34) | 13/25 (52) |
| Invasive cancer | 9/9 (100) | 6/32 (19) | 1/25 (4) |
| Biological type of the recurrence ** | |||
| ER−PR−HER2− | 0 | 4/66 (6) | 1/66 (2) |
| ER/PR-HER2+ | 4/66 (6) | 6/66 (9) | 2/66 (3) |
| ER/PR+HER2+ | 3/66 (4.5) | 2/66 (3) | 2/66 (3) |
| Luminal A | 2/66 (3) | 12/66 (18) | 16/66 (24) |
| Luminal B | 0 | 8/66 (12) | 4/66 (6) |
| Recurrence location | |||
| Tumor bed | 5/9 (55) | 16/32 (50) | 14/25 (56) |
| The same quadrant | - | 8/32 (25) | 6/25 (24) |
| Another quadrant | - | 7/32 (22) | 5/25 (20) |
| Metastases to lymph nodes | 3/9 (34) | 1/32 (3) | 0 |
| Distant metastases | 1/9 (11) | 0 | 0 |
| Cause of Deaths | Number of Deaths | Initial Method of DCIS Treatment | ||
|---|---|---|---|---|
| Mastectomy | Breast-Conserving Treatment | Breast-Conserving Surgery | ||
| Total number of deaths | 86 | 47 | 22 | 17 |
| Deaths due to DCIS recurrence | 4/737 (0.5%) | 3 | 1 | 0 |
| Deaths due to other neoplastic lesions | 26 | 11 | 7 | 8 |
| Endometrial cancer | 5 | 2 | 2 | 1 |
| Lung cancer | 4 | 1 | 1 | 2 |
| Ovarian cancer | 3 | 2 | 1 | 0 |
| Contralateral breast cancer | 3 | 2 | 0 | 1 |
| Gallbladder/liver hilum cancer | 3 | 1 | 1 | 1 |
| Pancreatic cancer | 2 | 1 | 1 | 0 |
| Colon cancer | 2 | 1 | 1 | 0 |
| Gastric cancer | 1 | 0 | 0 | 1 |
| Cervical cancer | 1 | 0 | 0 | 1 |
| Melanoma | 1 | 0 | 0 | 1 |
| Glioblastoma multiforme | 1 | 1 | 0 | 0 |
| Deaths due to other causes | 48 | 29 | 12 | 7 |
| Missing data | 8 | 4 | 2 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niwińska, A.; Kunkiel, M. Type of Recurrence, Cause of Death and Second Neoplasms among 737 Patients with Ductal Carcinoma In Situ of the Breast—15-Year Follow-Up. Cancers 2022, 14, 669. https://doi.org/10.3390/cancers14030669
Niwińska A, Kunkiel M. Type of Recurrence, Cause of Death and Second Neoplasms among 737 Patients with Ductal Carcinoma In Situ of the Breast—15-Year Follow-Up. Cancers. 2022; 14(3):669. https://doi.org/10.3390/cancers14030669
Chicago/Turabian StyleNiwińska, Anna, and Michał Kunkiel. 2022. "Type of Recurrence, Cause of Death and Second Neoplasms among 737 Patients with Ductal Carcinoma In Situ of the Breast—15-Year Follow-Up" Cancers 14, no. 3: 669. https://doi.org/10.3390/cancers14030669
APA StyleNiwińska, A., & Kunkiel, M. (2022). Type of Recurrence, Cause of Death and Second Neoplasms among 737 Patients with Ductal Carcinoma In Situ of the Breast—15-Year Follow-Up. Cancers, 14(3), 669. https://doi.org/10.3390/cancers14030669