
Predictive and Prognostic Role of Pre-Therapy and Interim 68Ga-DOTATOC PET/CT Parameters in Metastatic Advanced Neuroendocrine Tumor Patients Treated with PRRT

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ga-DOTATOC PET/CT
2.3. PRRT
2.4. Assessment of Treatment Response
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. PRRT and PET/CT
3.3. Overall Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Eychenne, R.; Bouvry, C.; Bourgeois, M.; Loyer, P.; Benoist, E.; Lepareur, N. Overview of Radiolabeled Somatostatin Analogs for Cancer Imaging and Therapy. Molecules 2020, 25, 4012. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of 177 Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Bodei, L.; Kidd, M.; Paganelli, G.; Grana, C.M.; Drozdov, I.; Cremonesi, M.; Lepensky, C.; Kwekkeboom, D.J.; Baum, R.P.; Krenning, E.P.; et al. Long-term tolerability of PRRT in 807 patients with neuroendocrine tumours: The value and limitations of clinical factors. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.H.; Goldner, W.S.; Halfdanarson, T.R.; Bergsland, E.; Berlin, J.D.; Halperin, D.; Chan, J.; Kulke, M.H.; Benson, A.B.; Blaszkowsky, L.S.; et al. Neuroendocrine and adrenal tumors, version 2.2018 featured updates to the nccn guidelines. JNCCN J. Natl. Compr. Cancer Netw. 2018, 16, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Filice, A.; Fraternali, A.; Frasoldati, A.; Asti, M.; Grassi, E.; Massi, L.; Sollini, M.; Froio, A.; Erba, P.A.; Versari, A. Radiolabeled Somatostatin Analogues Therapy in Advanced Neuroendocrine Tumors: A Single Centre Experience. J. Oncol. 2012, 2012, 320198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albertelli, M.; Dotto, A.; Di Dato, C.; Malandrino, P.; Modica, R.; Versari, A.; Colao, A.; Ferone, D.; Faggiano, A. PRRT: Identikit of the perfect patient. Rev. Endocr. Metab. Disord. 2021, 22, 563–579. [Google Scholar] [CrossRef] [PubMed]
- Cottereau, A.S.; Versari, A.; Loft, A.; Casasnovas, O.; Bellei, M.; Ricci, R.; Bardet, S.; Castagnoli, A.; Brice, P.; Raemaekers, J.; et al. Prognostic value of baseline metabolic tumor volume in early-stage Hodgkin lymphoma in the standard arm of the H10 trial. Blood 2018, 131, 1456–1463. [Google Scholar] [CrossRef] [PubMed]
- Hofheinz, F.; Li, Y.; Steffen, I.G.; Lin, Q.; Lili, C.; Hua, W.; van den Hoff, J.; Zschaeck, S. Confirmation of the prognostic value of pretherapeutic tumor SUR and MTV in patients with esophageal squamous cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1485–1494. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, F.; Werner, R.A.; Henkenberens, C.; Ross, T.L.; Christiansen, H.; Bengel, F.M.; Derlin, T. Predictive and prognostic impact of blood-based inflammatory biomarkers in patients with gastroenteropancreatic neuroendocrine tumors commencing peptide receptor radionuclide therapy. Diagnostics 2021, 11, 504. [Google Scholar] [CrossRef] [PubMed]
- Ortega, C.; Wong, R.K.S.; Schaefferkoetter, J.; Veit-Haibach, P.; Myrehaug, S.; Juergens, R.; Laidley, D.; Anconina, R.; Liu, A.; Metser, U. Quantitative 68 Ga-DOTATATE PET/CT Parameters for the Prediction of Therapy Response in Patients with Progressive Metastatic Neuroendocrine Tumors Treated with 177 Lu-DOTATATE. J. Nucl. Med. 2021, 62, 1406–1414. [Google Scholar] [CrossRef] [PubMed]
- Zaknun, J.J.; Bodei, L.; Mueller-Brand, J.; Pavel, M.E.; Baum, R.P.; Hörsch, D.; O’Dorisio, M.S.; O’Dorisiol, T.M.; Howe, J.R.; Cremonesi, M.; et al. The joint IAEA, EANM, and SNMMI practical guidance on peptide receptor radionuclide therapy (PRRNT) in neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 800–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CHMP Lutathera, INN-Lutetium (177Lu) Oxodotreotide. Available online: https://www.ema.europa.eu/en/documents/product-information/lutathera-epar-product-information_en.pdf (accessed on 23 January 2022).
- Cives, M.; Strosberg, J. Radionuclide Therapy for Neuroendocrine Tumors. Curr. Oncol. Rep. 2017, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; Wolin, E.; Chasen, B.; Kulke, M.; Bushnell, D.; Caplin, M.; Baum, R.P.; Kunz, P.; Hobday, T.; Hendifar, A.; et al. Health-related quality of life in patients with progressive midgut neuroendocrine tumors treated with 177 lu-dotatate in the phase III netter-1 trial. J. Clin. Oncol. 2018, 36, 2578–2584. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lin, L.; Wang, M.; Li, Y. The therapeutic efficacy of 177Lu-DOTATATE/DOTATOC in advanced neuroendocrine tumors. Medicine 2020, 99, e19304. [Google Scholar] [CrossRef] [PubMed]
- Öksüz, M.Ö.; Winter, L.; Pfannenberg, C.; Reischl, G.; Müssig, K.; Bares, R.; Dittmann, H. Peptide receptor radionuclide therapy of neuroendocrine tumors with 90Y-DOTATOC: Is treatment response predictable by pre-therapeutic uptake of 68Ga-DOTATOC? Diagn. Interv. Imaging 2014, 95, 289–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratochwil, C.; Stefanova, M.; Mavriopoulou, E.; Holland-Letz, T.; Dimitrakopoulou-Strauss, A.; Afshar-Oromieh, A.; Mier, W.; Haberkorn, U.; Giesel, F.L. SUV of [68Ga]DOTATOC-PET/CT Predicts Response Probability of PRRT in Neuroendocrine Tumors. Mol. Imaging Biol. 2014, 17, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.; Oberauer, A.; Dobrozemsky, G.; Decristoforo, C.; Putzer, D.; Kendler, D.; Uprimny, C.; Kovacs, P.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-octreotide PET for assessing response to somatostatin-receptor-mediated radionuclide therapy. J. Nucl. Med. 2009, 50, 1427–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soydal, Ç.; Peker, A.; Özkan, E.; Küçük, Ö.N.; Kir, M.K. The role of baseline Ga-68 DOTATATE positron emission tomography/computed tomography in the prediction of response to fixed-dose peptide receptor radionuclide therapy with lu-177 DOTATATE. Turk. J. Med. Sci. 2016, 46, 409–413. [Google Scholar] [CrossRef]
- Werner, R.A.; Ilhan, H.; Lehner, S.; Papp, L.; Zsótér, N.; Schatka, I.; Muegge, D.O.; Javadi, M.S.; Higuchi, T.; Buck, A.K.; et al. Pre-therapy Somatostatin Receptor-Based Heterogeneity Predicts Overall Survival in Pancreatic Neuroendocrine Tumor Patients Undergoing Peptide Receptor Radionuclide Therapy. Mol. Imaging Biol. 2019, 21, 582–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohlendorf, F.; Henkenberens, C.; Brunkhorst, T.; Ross, T.L.; Christiansen, H.; Bengel, F.M.; Derlin, T. Volumetric 68Ga-DOTA-TATE PET/CT for assessment of whole-body tumor burden as a quantitative imaging biomarker in patients with metastatic gastroenteropancreatic neuroendocrine tumors. Q. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, E.; Van Binnebeek, S.; Vandecaveye, V.; Baete, K.; Vanbilloen, H.; Koole, M.; Mottaghy, F.M.; Haustermans, K.; Clement, P.M.; Nackaerts, K.; et al. Inflammation-based index and 68ga-dotatoc pet-derived uptake and volumetric parameters predict outcome in neuroendocrine tumor patients treated with 90y-dotatoc. J. Nucl. Med. 2020, 61, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Meignan, M.; Sasanelli, M.; Casasnovas, R.O.; Luminari, S.; Fioroni, F.; Coriani, C.; Masset, H.; Itti, E.; Gobbi, P.G.; Merli, F.; et al. Metabolic tumour volumes measured at staging in lymphoma: Methodological evaluation on phantom experiments and patients. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, A.; Papadakis, G.Z.; Millo, C.; Hammoud, D.; Sadowski, S.M.; Herscovitch, P.; Pacak, K.; Marx, S.J.; Yang, L.; Nockel, P.; et al. Prognostic Utility of Total 68Ga-DOTATATE-Avid Tumor Volume in Patients with Neuroendocrine Tumors. Gastroenterology 2018, 154, 998–1008.e1. [Google Scholar] [CrossRef] [PubMed]
- Abdulrezzak, U.; Kurt, Y.K.; Kula, M.; Tutus, A. Combined imaging with 68Ga-DOTA-TATE and 18F-FDG PET/CT on the basis of volumetric parameters in neuroendocrine tumors. Nucl. Med. Commun. 2016, 37, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Haug, A.R.; Auernhammer, C.J.; Wängler, B.; Schmidt, G.P.; Uebleis, C.; Göke, B.; Cumming, P.; Bartenstein, P.; Tiling, R.; Hacker, M. 68Ga-DOTATATE PET/CT for the early prediction of response to somatostatin receptor-mediated radionuclide therapy in patients with well-differentiated neuroendocrine tumors. J. Nucl. Med. 2010, 51, 1349–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binderup, T.; Knigge, U.; Johnbeck, C.B.; Loft, A.; Berthelsen, A.K.; Oturai, P.; Mortensen, J.; Federspiel, B.; Langer, S.W.; Kjaer, A. 18F-FDG PET is Superior to WHO Grading as a Prognostic Tool in Neuroendocrine Neoplasms and Useful in Guiding PRRT: A Prospective 10-Year Follow-up Study. J. Nucl. Med. 2021, 62, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Poeppel, T.D.; Binse, I.; Petersenn, S.; Lahner, H.; Schott, M.; Antoch, G.; Brandau, W.; Bockisch, A.; Boy, C. 68Ga-DOTATOC versus 68Ga-DOTATATE PET/CT in functional imaging of neuroendocrine tumors. J. Nucl. Med. 2011, 52, 1864–1870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnbeck, C.B.; Knigge, U.; Loft, A.; Berthelsen, A.K.; Mortensen, J.; Oturai, P.; Langer, S.W.; Elema, D.R.; Kjaer, A. Head-to-Head Comparison of 64Cu-DOTATATE and 68Ga-DOTATOC PET/CT: A Prospective Study of 59 Patients with Neuroendocrine Tumors. J. Nucl. Med. 2017, 58, 451–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Patients | (n = 46) |
|---|---|
| Age, median (range) in years | 60 (25–85) |
| Gender, n (%) | |
| Male | 25 (54%) |
| Female | 21 (46%) |
| Primary tumour, n (%) | |
| GEP | 36 (78%) |
| Stomach | 3 (8%) |
| Pancreas | 8 (22%) |
| Intestine | 25 (70%) |
| Broncho-Pulmonary | 6 (13%) |
| Unkown | 4 (9%) |
| GEP NETs WHO grade, n (%) | |
| G1 ((Ki-67 0–2%) | 21 (46%) |
| G2 (Ki-67 3–20%) | 19 (41%) |
| G3 (Ki-67 >20%) | 2 (4%) |
| NA | 4 (9%) |
| Metastasis, n | |
| Liver | 21 |
| Lymph nodes | 23 |
| Bone | 15 |
| Lung | 7 |
| Other | 9 |
| Cycles of PRRT, n (%) | |
| 2 | 2 (4%) |
| 3 | 1 (2%) |
| 4 | 5 (11%) |
| 5 | 11 (24%) |
| 6 | 27 (59%) |
| Type of PRRT | |
| Only 177Lu | 5 (11%) |
| 177Lu + 90Y | 41(89%) |
| PET Parameters | All (n = 46) | Responders (n = 35) | Non-Responders (n = 11) | p Value |
|---|---|---|---|---|
| SUVmax | 0.58 | |||
| Mean (SD) | 40 (24.9) | 41.5 (27.1) | 35.5 (35.5) | |
| Median (IQR) | 34 (23.1–55.8) | 34.5 (23.7–56.2) | 33.5 (21.8–53.9) | |
| SUVmean | 0.57 | |||
| Mean (SD) | 11.6 (5.9) | 10.3 (4.1) | 11.9 (6.3) | |
| Median (IQR) | 9.9 (7.6–16.4) | 9.9 (7.2–17.3) | 10(7.8–13.5) | |
| SUVratio T/S | 0.93 | |||
| Mean (SD) | 1.8 (0.9) | 1.4 (0.7) | 1.9 (2.2) | |
| Median (IQR) | 1.1 (0.7–2.3) | 1.2 (0.6–2.3) | 1 (0.8–2.2) | |
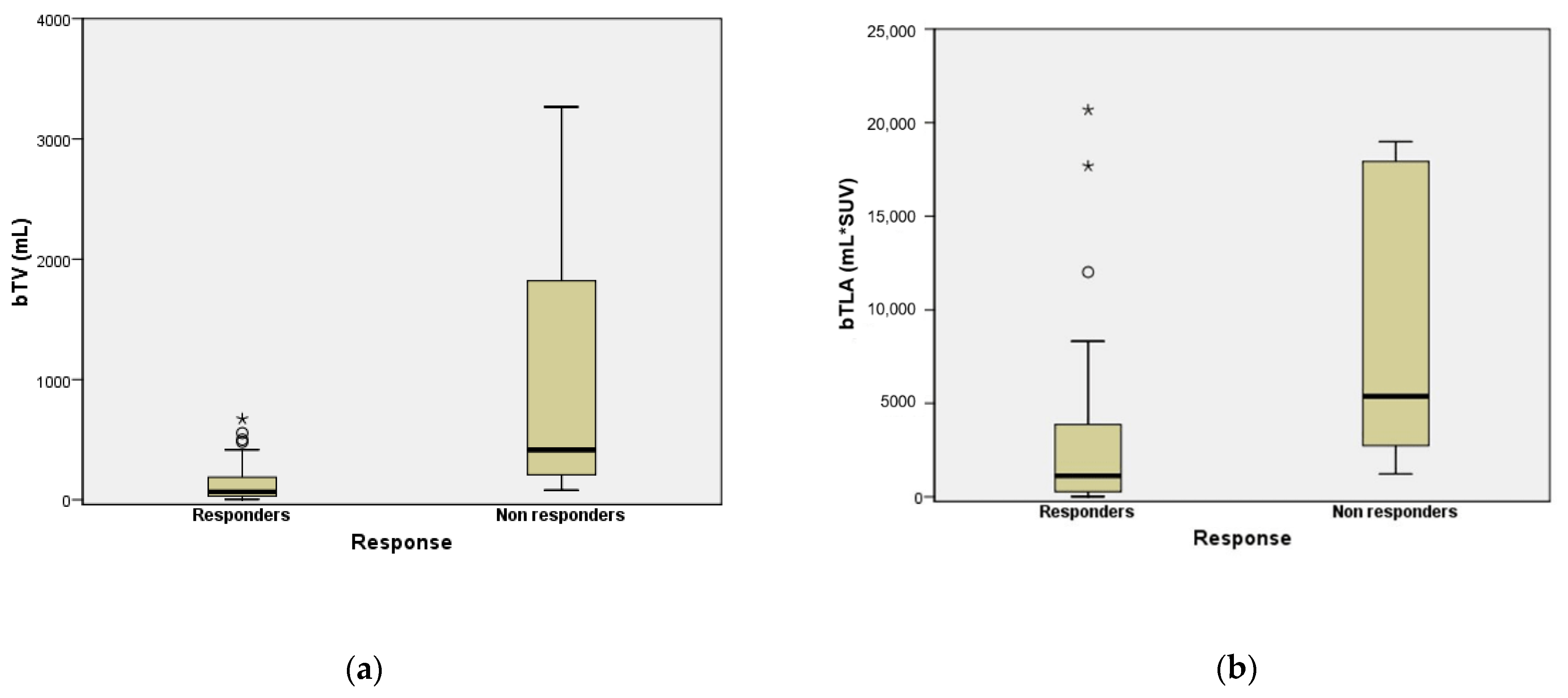
| bTV | <0.001 | |||
| Mean (SD) | 371 (665.5) | 143.7 (177.6) | 1073.5 (1061,4) | |
| Median (IQR) | 143.8 (32.9–354) | 77.6 (31–186.8) | 496.2 (218.3–2029.4) | |
| bTLA | 0.001 | |||
| Mean (SD) | 5339.5 (8171.4) | 3108.13 (4971.1) | 12,236.4 (11,959) | |
| Median (IQR) | 1834 (342–6309) | 1341 (272.3–3865) | 6078.3 (2813–18,959) | |
| ΔSUVmax | 0.89 | |||
| Mean (SD) | 23.9 (117.7) | 25.2 (129,6) | 18.1 (62) | |
| Median (IQR) | 1.1 (−21.2–22.1) | −2.5 (−21.2–22.2) | 3.5 (−26.6–22.1) | |
| ΔSUVmean | 0.84 | |||
| Mean (SD) | 25.5 (79.2) | 45.6 (128) | 19 (55,9) | |
| Median (IQR) | 4.2 (−17.8–39.4) | 6.2 (−16.5–25.4) | −10.2 (−27.4–47.6) | |
| ΔSUVratioT/S | 0.42 | |||
| Mean (SD) | 1.3 (2) | 1.9 (0.8) | 1.4 (0.9) | |
| Median (IQR) | −1.1 (−41.5–24.5) | −11.5 (−40.5–20.9) | 1.9 (−46.8–32.3) | |
| ΔTV | 0.51 | |||
| Mean (SD) | 61 (170) | 27.1 (55,6) | 71.5 (756,7) | |
| Median (IQR) | 32.4 (−10.2–70.6) | 32.4 (−5.5–69.2) | 32.4 (−23.9–79.9) | |
| ΔTLA | 0.92 | |||
| Mean (SD) | 143 (668,4) | 45.7 (79,1) | 171.9 (756.7) | |
| Median (IQR) | 25 (−12.5–80.9) | 24.3 (−0.4–80) | 36 (−22.5–111) |
| PET Parameters | Univariate Analysis | |
|---|---|---|
| OR (95%CI) | p Value | |
| SUVmax | 1.06 (0.99–1.13) | 0.09 |
| SUVmean | 0.8 (0.55–1.15) | 0.23 |
| SUVratio T/S | 0.84 (0.52–1.35) | 0.48 |
| bTV | 1.17 (1.02–1.32) | 0.02 |
| bTLA | 0.99 (0.93–1.01) | 0.08 |
| ΔSUVmax | 0.97 (0.93–1.01) | 0.25 |
| ΔSUVmean | 1.007 (0.98–1.01) | 0.259 |
| ΔSUVratioT/S | 0.99 (0.98–1.01) | 0.839 |
| ΔTV | 0.99 (0.98–1.01) | 0.922 |
| ΔTLA | 0.99 (0.98–1.01) | 0.70 |
| PET Parameter | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95%CI) | p Value | HR (95%CI) | p Value | |
| SUVmax (<22.02) | 0.99 (0.12–8.20) | 0.99 | - | - |
| SUVmean (≤5.45) | 0.31 (0.06–1.51) | 0.26 | - | - |
| SUVratioT/S (≤1.31) | 0.84 (0.08–8.23) | 0.87 | - | - |
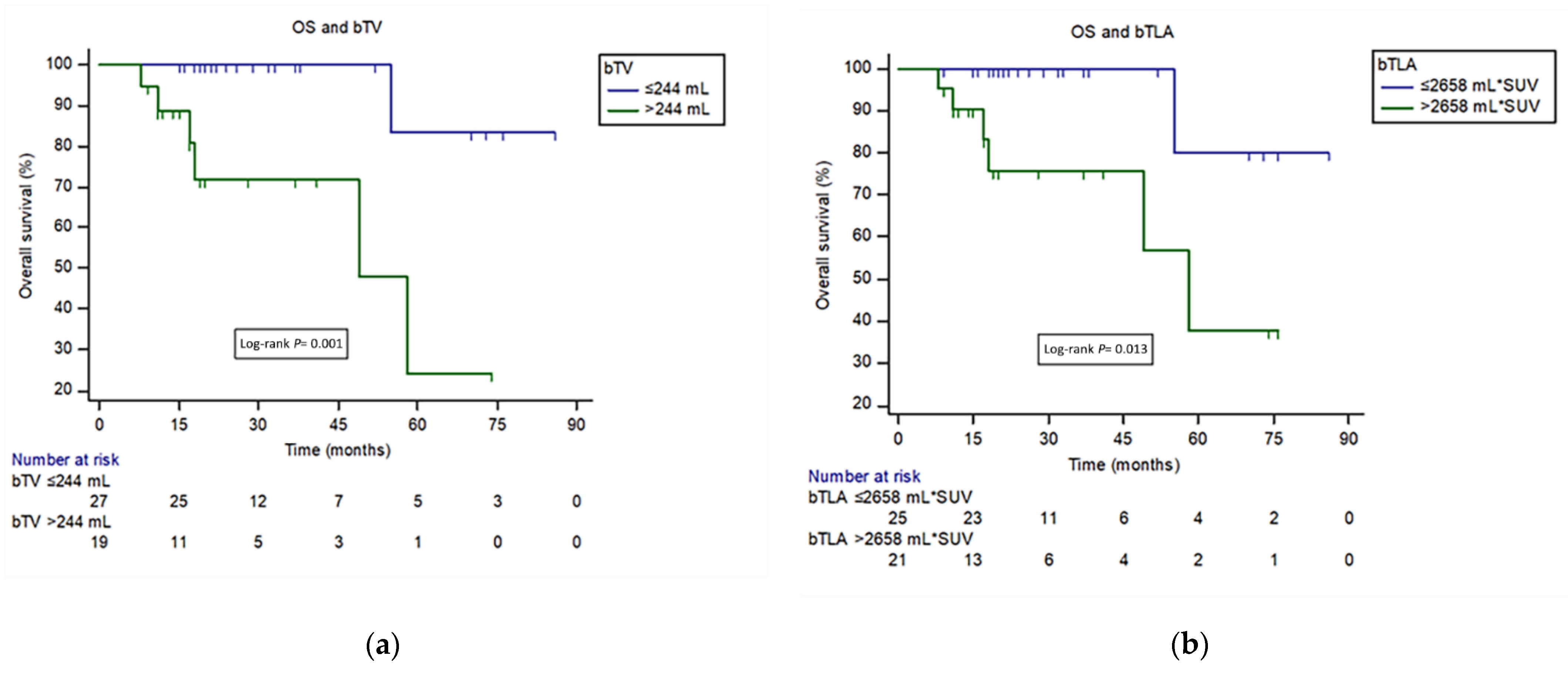
| bTV (>244.48) | 13 (2.6–64.1) | 0.001 | 12.76(1.53–107) | 0.01 |
| bTLA (>2658.62) | 9.08 (1.09–75.76) | 0.04 | 7.15 (0.96–68.1) | 0.98 |
| ΔSUVmax (>5.5598) | 0.15 (0.03–0.67) | 0.04 | 0.17 (0.02–1.46) | 0.1 |
| ΔSUVmean (>24.4984) | 0.65 (0.05–7.87) | 0.68 | - | - |
| ΔSUVratioT/S (>−0.75) | 0.14 (0.017–1.28) | 0.08 | - | - |
| ΔTV (≤−15.876) | 0.23(0.02–1.86) | 0.354 | - | - |
| ΔTLA (>80.2) | 0.45 (0.082–2.48) | 0.2737 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durmo, R.; Filice, A.; Fioroni, F.; Cervati, V.; Finocchiaro, D.; Coruzzi, C.; Besutti, G.; Fanello, S.; Frasoldati, A.; Versari, A. Predictive and Prognostic Role of Pre-Therapy and Interim 68Ga-DOTATOC PET/CT Parameters in Metastatic Advanced Neuroendocrine Tumor Patients Treated with PRRT. Cancers 2022, 14, 592. https://doi.org/10.3390/cancers14030592
Durmo R, Filice A, Fioroni F, Cervati V, Finocchiaro D, Coruzzi C, Besutti G, Fanello S, Frasoldati A, Versari A. Predictive and Prognostic Role of Pre-Therapy and Interim 68Ga-DOTATOC PET/CT Parameters in Metastatic Advanced Neuroendocrine Tumor Patients Treated with PRRT. Cancers. 2022; 14(3):592. https://doi.org/10.3390/cancers14030592
Chicago/Turabian StyleDurmo, Rexhep, Angelina Filice, Federica Fioroni, Veronica Cervati, Domenico Finocchiaro, Chiara Coruzzi, Giulia Besutti, Silvia Fanello, Andrea Frasoldati, and Annibale Versari. 2022. "Predictive and Prognostic Role of Pre-Therapy and Interim 68Ga-DOTATOC PET/CT Parameters in Metastatic Advanced Neuroendocrine Tumor Patients Treated with PRRT" Cancers 14, no. 3: 592. https://doi.org/10.3390/cancers14030592
APA StyleDurmo, R., Filice, A., Fioroni, F., Cervati, V., Finocchiaro, D., Coruzzi, C., Besutti, G., Fanello, S., Frasoldati, A., & Versari, A. (2022). Predictive and Prognostic Role of Pre-Therapy and Interim 68Ga-DOTATOC PET/CT Parameters in Metastatic Advanced Neuroendocrine Tumor Patients Treated with PRRT. Cancers, 14(3), 592. https://doi.org/10.3390/cancers14030592