

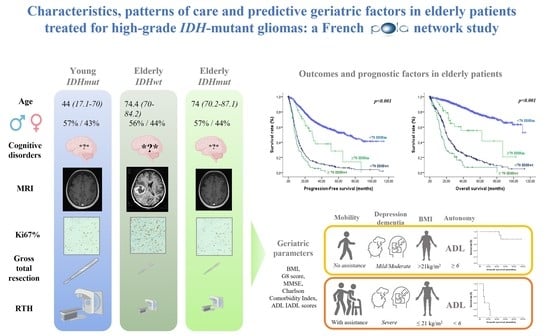
Characteristics, Patterns of Care and Predictive Geriatric Factors in Elderly Patients Treated for High-Grade IDH-Mutant Gliomas: A French POLA Network Study
 , , , add
Show full author list
, , , add
Show full author list
Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Elderly Patients IDHm HGG
3.1.1. Clinical Characteristics and Patterns of Care
3.1.2. Geriatric Characteristics
3.1.3. Feasibility and Safety of Adjuvant Treatment Chemotherapy and Radiotherapy
3.2. Characteristics and Patterns of Care Group Comparisons and Outcomes
3.2.1. Comparison between Elderly Patients IDHm HGG (n = 39) and IDHwt HGG (n = 80)
3.2.2. Comparison between Elderly (n = 39) and Non-Elderly (n = 919) Patients IDHm HGG
3.2.3. Outcomes
3.3. Prognostic Factors in Elderly Patients IDHm HGG
3.4. Towards a Brain Tumor Geriatric Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, C.; Hentschel, B.; Wick, W.; Capper, D.; Felsberg, J.; Simon, M.; Westphal, M.; Schackert, G.; Meyermann, R.; Pietsch, T.; et al. Patients with IDH1 wild type anaplastic astrocytomas exhibit worse prognosis than IDH1-mutated glioblastomas, and IDH1 mutation status accounts for the unfavorable prognostic effect of higher age: Implications for classification of gliomas. Acta Neuropathol. 2010, 120, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.-B.; Yue, W.; Xie, C.; Zhang, R.-Y.; Hu, S.-S.; Wang, Z. IDH1 mutation is associated with improved overall survival in patients with glioblastoma: A meta-analysis. Tumor Biol. 2013, 34, 3555–3559. [Google Scholar] [CrossRef] [PubMed]
- Van den Bent, M.J.; Baumert, B.; Erridge, S.C.; Vogelbaum, M.A.; Nowak, A.K.; Sanson, M.; Brandes, A.A.; Clement, P.M.; Baurain, J.F.; Mason, W.P.; et al. Interim results from the CATNON trial (EORTC study 26053-22054) of treatment with concurrent and adjuvant temozolomide for 1p/19q non-co-deleted anaplastic glioma: A phase 3, randomised, open-label intergroup study. Lancet 2017, 390, 1645–1653. [Google Scholar] [CrossRef]
- Van Den Bent, M.J.; Carpentier, A.F.; Brandes, A.A.; Sanson, M.; Taphoorn, M.J.B.; Bernsen, H.J.J.A.; Frenay, M.; Tijssen, C.C.; Grisold, W.; Sipos, L.; et al. Adjuvant Procarbazine, Lomustine, and Vincristine Improves Progression-Free Survival but Not Overall Survival in Newly Diagnosed Anaplastic Oligodendrogliomas and Oligoastrocytomas: A Randomized European Organisation for Research and Treatment of Cancer Phase III Trial. J. Clin. Oncol. 2006, 24, 2715–2722. [Google Scholar] [CrossRef]
- Shaw, E.G.; Wang, M.; Coons, S.W.; Brachman, D.G.; Buckner, J.C.; Stelzer, K.J.; Barger, G.R.; Brown, P.D.; Gilbert, M.R.; Mehta, M. Randomized Trial of Radiation Therapy Plus Procarbazine, Lomustine, and Vincristine Chemotherapy for Supratentorial Adult Low-Grade Glioma: Initial Results of RTOG 9802. J. Clin. Oncol. 2012, 30, 3065–3070. [Google Scholar] [CrossRef]
- Andrews, C.; Prayson, R.A. IDH mutations in older patients with diffuse astrocytic gliomas. Ann. Diagn. Pathol. 2020, 49, 151653. [Google Scholar] [CrossRef]
- Bauchet, L.; Ostrom, Q.T. Epidemiology and Molecular Epidemiology. Neurosurg. Clin. N. Am. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Fang, J.; Lin, D.; Deng, X.; Li, D.; Sheng, H.; Lin, J.; Zhang, N.; Yin, B. Epidemiological trends, relative survival, and prognosis risk factors of WHO Grade III gliomas: A population-based study. Cancer Med. 2019, 8, 3286–3295. [Google Scholar] [CrossRef]
- Stupp, R.; Brada, M.J.; van den Bent, M.; Tonn, J.-C.; Pentheroudakis, G.; on behalf of the ESMO Guidelines Working Group. High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii93–iii101. [Google Scholar] [CrossRef]
- Weller, M.; dan der Bent, M.; Tonn, J.C.; Stupp, R.; Preusser, M.; Cohen-Jonathan-Moyal, E.; Henriksson, R.; Le Rhun, E.; Balana, C.; Chinot, O.; et al. European Association for Neuro-Oncology (EANO) guideline on the diagnosis and treatment of adult astrocytic and oligodendroglial gliomas. Lancet Oncol. 2017, 18, e315–e329. [Google Scholar] [CrossRef]
- Harrison, R.A.; de Groot, J.F. Treatment of Glioblastoma in the Elderly. Drugs Aging 2018, 35, 707–718. [Google Scholar] [CrossRef]
- Braun, K.; Ahluwalia, M.S. Treatment of Glioblastoma in Older Adults. Curr. Oncol. Rep. 2017, 19, 81. [Google Scholar] [CrossRef]
- Gállego Pérez-Larraya, J.; Delattre, J.-Y. Management of Elderly Patients with Gliomas. Oncologist 2014, 19, 1258–1267. [Google Scholar] [CrossRef]
- Hanna, C.; Lawrie, T.A.; Rogozińska, E.; Kernohan, A.; Jefferies, S.; Bulbeck, H.; Ali, U.M.; Robinson, T.; Grant, R. Treatment of newly diagnosed glioblastoma in the elderly: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 2020, CD013261. [Google Scholar] [CrossRef]
- Jordan, J.T.; Gerstner, E.R.; Batchelor, T.T.; Cahill, D.P.; Plotkin, S.R. Glioblastoma care in the elderly. Cancer 2016, 122, 189–197. [Google Scholar] [CrossRef]
- Bellera, C.A.; Rainfray, M.; Mathoulin-Pélissier, S.; Mertens, C.; Delva, F.; Fonck, M.; Soubeyran, P.L. Screening older cancer patients: First evaluation of the G-8 geriatric screening tool. Ann. Oncol. 2012, 23, 2166–2172. [Google Scholar] [CrossRef]
- Soubeyran, P.; Bellera, C.; Goyard, J.; Heitz, D.; Curé, H.; Rousselot, H.; Albrand, G.; Servent, V.; Jean, O.S.; Van Praagh, I.; et al. Screening for Vulnerability in Older Cancer Patients: The ONCODAGE Prospective Multicenter Cohort Study. PLoS ONE 2014, 9, e115060. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged. The index of Adl: A standardized measure of biological and phychological funcation. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Houillier, C.; Wang, X.; Kaloshi, G.; Mokhtari, K.; Guillevin, R.; Laffaire, J.; Paris, S.; Boisselier, B.; Idbaih, A.; Laigle-Donadey, F.; et al. IDH1 or IDH2 mutations predict longer survival and response to temozolomide in low-grade gliomas. Neurology 2010, 75, 1560–1566. [Google Scholar] [CrossRef] [PubMed]
- Figarella-Branger, D.; Mokhtari, K.; Dehais, C.; Jouvet, A.; Uro-Coste, E.; Colin, C.; Carpentier, C.; Forest, F.; Maurage, C.-A.; Vignaud, J.-M.; et al. Mitotic index, microvascular proliferation, and necrosis define 3 groups of 1p/19q codeleted anaplastic oligodendrogliomas associated with different genomic alterations. Neurooncology 2014, 16, 1244–1254. [Google Scholar] [CrossRef] [PubMed]
- Kaloshi, G.; Benouaich-Amiel, A.; Diakite, F.; Taillibert, S.; Lejeune, J.; Laigle-Donadey, F.; Renard, M.-A.; Iraqi, W.; Idbaih, A.; Paris, S.; et al. Temozolomide for low-grade gliomas: Predictive impact of 1p/19q loss on response and outcome. Neurology 2007, 68, 1831–1836. [Google Scholar] [CrossRef]
- Ewelt, C.; Goeppert, M.; Rapp, M.; Steiger, H.-J.; Stummer, W.; Sabel, M. Glioblastoma multiforme of the elderly: The prognostic effect of resection on survival. J. Neuro-Oncology 2011, 103, 611–618. [Google Scholar] [CrossRef]
- Chaichana, K.L.; Garzon-Muvdi, T.; Parker, S.; Weingart, J.D.; Olivi, A.; Bennett, R.; Brem, H.; Quiñones-Hinojosa, A. Supratentorial Glioblastoma Multiforme: The Role of Surgical Resection Versus Biopsy among Older Patients. Ann. Surg. Oncol. 2011, 18, 239–245. [Google Scholar] [CrossRef]
- Almenawer, S.A.; Badhiwala, J.H.; Alhazzani, W.; Greenspoon, J.; Farrokhyar, F.; Yarascavitch, B.; Algird, A.; Kachur, E.; Cenic, A.; Sharieff, W.; et al. Biopsy vs. partial vs. gross total resection in older patients with high-grade glioma: A systematic review and meta-analysis. Neuro-Oncology 2015, 17, 868–881. [Google Scholar] [CrossRef]
- Keime-Guibert, F.; Chinot, O.; Taillandier, L.; Cartalat-Carel, S.; Frenay, M.; Kantor, G.; Guillamo, J.-S.; Jadaud, E.; Colin, P.; Bondiau, P.-Y.; et al. Radiotherapy for Glioblastoma in the Elderly. N. Engl. J. Med. 2007, 356, 1527–1535. [Google Scholar] [CrossRef]
- Perry, J.R.; Laperriere, N.; O’Callaghan, C.J.; Brandes, A.A.; Menten, J.; Phillips, C.; Fay, M.; Nishikawa, R.; Cairncross, J.G.; Roa, W.; et al. Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma. N. Engl. J. Med. 2017, 376, 1027–1037. [Google Scholar] [CrossRef]
- Ackerl, M.; Flechl, B.; Dieckmann, K.; Preusser, M.; Widhalm, G.; Sax, C.; Marosi, C. Outcome evaluation in glioblastoma patients older than 65 years: Importance of individual assessment of treatment tolerance. Clin. Neuropathol. 2014, 33, 399–406. [Google Scholar] [CrossRef]
- Giaccherini, L.; Galaverni, M.; Renna, I.; Timon, G.; Galeandro, M.; Pisanello, A.; Russo, M.; Botti, A.; Iotti, C.; Ciammella, P. Role of multidimensional assessment of frailty in predicting outcomes in older patients with glioblastoma treated with adjuvant concurrent chemo-radiation. J. Geriatr. Oncol. 2019, 10, 770–778. [Google Scholar] [CrossRef]
- Schneider, M.; Potthoff, A.-L.; Scharnböck, E.; Heimann, M.; Schäfer, N.; Weller, J.; Schaub, C.; Jacobs, A.H.; Güresir, E.; Herrlinger, U.; et al. Newly diagnosed glioblastoma in geriatric (65+) patients: Impact of patients frailty, comorbidity burden and obesity on overall survival. J. Neuro-Oncol. 2020, 149, 421–427. [Google Scholar] [CrossRef]
- Lombardi, G.; Bergo, E.; Caccese, M.; Padovan, M.; Bellu, L.; Brunello, A.; Zagonel, V. Validation of the Comprehensive Geriatric Assessment as a Predictor of Mortality in Elderly Glioblastoma Patients. Cancers 2019, 11, 1509. [Google Scholar] [CrossRef]
- Lorimer, C.F.; Saran, F.; Chalmers, A.J.; Brock, J. Glioblastoma in the elderly—How do we choose who to treat? J. Geriatr. Oncol. 2016, 7, 453–456. [Google Scholar] [CrossRef]
- Deluche, E.; Leobon, S.; Lamarche, F.; Tubiana-Mathieu, N. First validation of the G-8 geriatric screening tool in older patients with glioblastoma. J. Geriatr. Oncol. 2019, 10, 159–163. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Elderly IDHm (n = 39) | Elderly IDHwt (n = 80) | Younger IDHm (n = 919) | IDHm vs. IDHwt Elderly | IDHm Elderly vs. Younger | |
|---|---|---|---|---|---|
| Characteristics | N (% or Range) | N (% or Range) | N (% or Range) | p-Value | p-Value |
| Age (years, median, range) | 74.0 (70.2–87.1) | 74.4 (70–84.2) | 44 (17.1–70) | 0.914 | 0.001 |
| Gender | |||||
| Male | 22 (56.4) | 45 (56.2) | 526 (57.2) | 0.728 | 0.830 |
| Female | 17 (43.6) | 35 (43.8) | 393 (42.8) | ||
| Symptoms at diagnosis | |||||
| Epilepsy | 17 (43.6) | 31 (40.3) | 546 (61.1) | 0.438 | 0.063 |
| Cognitive disorders | 9 (23.1) | 25 (32.9) | 104 (11.7) | 0.045 | 0.053 |
| Neuro-imaging characteristics | |||||
| Contrast enhancement | 26 (78.8) | 69 (95.8) | 551 (69.1) | 0.001 | 0.406 |
| Necrosis | 7 (31.8) | 40 (78.4) | 117 (25.3) | 0.022 | 0.633 |
| WHO 2021 diagnoses | |||||
| Anaplastic oligodendroglioma | 28 (71.8) | 0 | 496 (54) | ||
| IDHm Anaplastic Astrocytoma | 5 (12.8) | 2 (2.5) | 210 (22.9) | ||
| IDHm grade IV Astrocytoma | 6 (15.4) | 78 (97.5) | 213 (23.1) | ||
| Histological characteristics | |||||
| Necrosis | 7 (17.9) | 41 (51.3) | 185 (20.2) | 0 | 0.672 |
| Microvascular Proliferation | 28 (71.8) | 67 (83.8) | 595 (64.9) | 0.031 | 0.554 |
| p53 expression | 22 (57.9) | 52 (65) | 566 (61.9) | 0.34 | 0.527 |
| Ki 67 expression (mean, range) | 15 (1–40) | 20 (3–90) | 15 (1–90) | 0.005 | 0.929 |
| Post-operative KPS (median, range) | 80 (50–100) | 80 (30–100) | 90 (10–100) | 0.715 | 0.005 |
| Corticosteroid intake | 16 (48.5) | 48 (65.8) | 448 (54.6) | 0.113 | 0.661 |
| Extent of resection | |||||
| Gross total/Subtotal | 9 (24.3) | 23 (31) | 437 (50.3) | 0.746 | 0.002 |
| Partial | 5 (13.5) | 10 (13.5) | 264 (30.4) | ||
| Biopsy | 23 (62.2) | 41 (55.4) | 167 (19.2) | ||
| Adjuvant Treatment | <0.001 | <0.001 | |||
| Wait and scan policy | 3 (7.7) | 0 | 37 (4.2) | ||
| Radiotherapy alone | 3 (7.7) | 11 (14.9) | 114 (13) | ||
| Chemotherapy alone (TMZ or PCV) | 16 (41) | 11 (14.9) | 129 (14.7) | ||
| RT-TMZ | 10 (25.6) | 46 (62.2) | 299 (34) | ||
| RT-PCV | 6 (15.4) | 1 (1.4) | 290 (33) | ||
| Palliative care | 1 (2.6) | 5 (6.8) | 6 (0.7) |
| Parameters | N | % |
|---|---|---|
| Post-operative KPS ≥ 70 | 16/21 | 76 |
| Cognitive disorders | ||
| MMSE ≥ 24 | 10/11 | 91 |
| Neuropsychological disorders a | 7/25 | 28 |
| Mobility | ||
| Getting out without assistance | 16/24 | 67 |
| Comorbidities | ||
| Charlson’s index ≥ 5 | 23/32 | 72 |
| Medications > 3 | 17/26 | 65 |
| Nutrition | ||
| Anorexia | 6/24 | 25 |
| Weight loss | 12/25 | 48 |
| BMI < 21 | 7/27 | 26 |
| Autonomy | ||
| ADL < 6 | 6/18 | 33.3 |
| IADL < 4 | 8/17 | 47 |
| Not a good self-reported state of health | 4/17 | 23.5 |
| G8 score estimation ≤ 14/17 | 16/25 | 64 |
| Factors | PFS | OS | ||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate b | Univariate | Mutivariate a | |||
| p Value | p Value | HR | p Value | p Value | HR | |
| G8 score (items) | ||||||
| Anorexia (yes vs. no) | 0.349 | 0.511 | ||||
| Weight loss (yes vs. no) | 0.775 | 0.052 | ||||
| Mobility (able to get out of chair/bed vs. go out) | 0.003 | 0.018 | 4.74 (1.30–17.21) | <0.001 | 0.008 | 9.93 (1.82–53.98) |
| Neuropsychological disorders (severe vs. mild or moderate depression or dementia) | 0.003 | 0.005 | 4.31 (1.56–11.92) | 0.036 | 0.047 | 3.51 (1.02–12.14) |
| BMI (≤21 kg/m2 vs. > 21 kg/m2) | <0.001 | 0.002 | 5.26 (1.83–15.04) | 0.002 | 0.006 | 5.85 (1.66–20.61) |
| Number of medications > 3 (yes vs. no) | 0.186 | 0.346 | ||||
| Self-reported state of health (lower vs. similar/better) | 0.775 | 0.047 | ||||
| Age ranges (>80 vs. <80 years) | 0.379 | 0.741 | ||||
| Autonomy | ||||||
| ADL (<6 vs. 6) | <0.001 | 0.002 | 14.97 (2.73–81.95) | <0.001 | 0.010 | 21.56 (2.11–219.86) |
| IADL (<4 vs. 4) | 0.002 | 0.132 | ||||
| Charlson’s index score (≥5 vs. <5) | 0.603 | 0.366 | ||||
| Biological factors | ||||||
| Haemoglobin serum level (≤ vs. >median) | 0.034 | 0.200 | 0.506 | |||
| Lymphocyte count b (≤ vs. >median) | 0.009 | 0.020 | 4.80 (1.28–18.08) | 0.143 | 0.309 | |
| Neutrophil count (≤ vs. >median) | 0.527 | 0.061 | ||||
| Platelet count (≤ vs. >median) | 0.458 | 0.863 | ||||
| Elevation of serum creatinine (≥ vs. <median) | 0.588 | 0.599 | ||||
| Serum albumin level (≤ vs. >median) | 0.641 | 0.346 | ||||
| Post-operative KPS (<70 vs. ≥70) | 0.012 | 0.023 | 3.77 (1.20–11.80) | 0.002 | 0.007 | 5.30 (1.57–17.95) |
| Grade (III vs. IV) | 0.004 | 0.001 | ||||
| Codeletion (yes vs. no) | 0.109 | 0.043 | ||||
| Type of surgery (biopsy vs. total/subtotal resection) | 0.827 | 0.675 | ||||
| Steroids intake (<10 vs. ≥10 mg/per day) | 0.019 | 0.380 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montégut, C.; Guillamo, J.-S.; Ducray, F.; Dehais, C.; Cohen-Jonathan Moyal, E.; Desenclos, C.; Petit, A.; Seizeur, R.; Bekaert, L.; Gaultier, C.; et al. Characteristics, Patterns of Care and Predictive Geriatric Factors in Elderly Patients Treated for High-Grade IDH-Mutant Gliomas: A French POLA Network Study. Cancers 2022, 14, 5509. https://doi.org/10.3390/cancers14225509
Montégut C, Guillamo J-S, Ducray F, Dehais C, Cohen-Jonathan Moyal E, Desenclos C, Petit A, Seizeur R, Bekaert L, Gaultier C, et al. Characteristics, Patterns of Care and Predictive Geriatric Factors in Elderly Patients Treated for High-Grade IDH-Mutant Gliomas: A French POLA Network Study. Cancers. 2022; 14(22):5509. https://doi.org/10.3390/cancers14225509
Chicago/Turabian StyleMontégut, Coline, Jean-Sébastien Guillamo, François Ducray, Caroline Dehais, Elisabeth Cohen-Jonathan Moyal, Christine Desenclos, Antoine Petit, Romuald Seizeur, Lien Bekaert, Claude Gaultier, and et al. 2022. "Characteristics, Patterns of Care and Predictive Geriatric Factors in Elderly Patients Treated for High-Grade IDH-Mutant Gliomas: A French POLA Network Study" Cancers 14, no. 22: 5509. https://doi.org/10.3390/cancers14225509
APA StyleMontégut, C., Guillamo, J.-S., Ducray, F., Dehais, C., Cohen-Jonathan Moyal, E., Desenclos, C., Petit, A., Seizeur, R., Bekaert, L., Gaultier, C., Motuo Fotso, M. J., Blonski, M., Frenel, J.-S., Vauléon, E., Langlois, O., Noel, G., Carpentier, A. F., Di Stefano, A. L., Bronnimann, C., ... Tabouret, E. (2022). Characteristics, Patterns of Care and Predictive Geriatric Factors in Elderly Patients Treated for High-Grade IDH-Mutant Gliomas: A French POLA Network Study. Cancers, 14(22), 5509. https://doi.org/10.3390/cancers14225509