

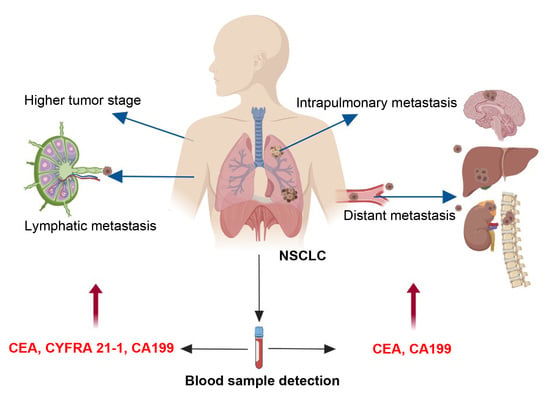
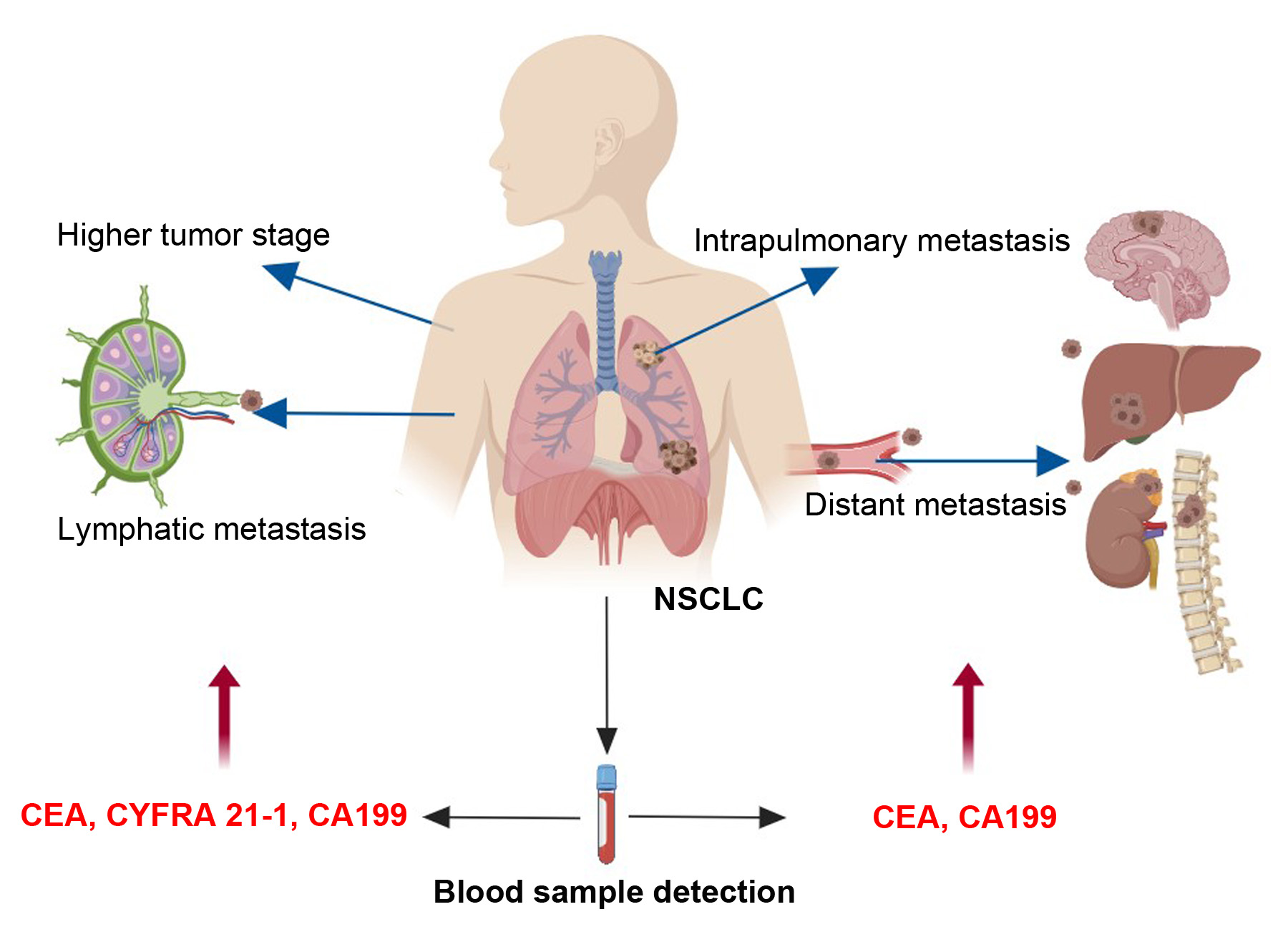
The Indicative Value of Serum Tumor Markers for Metastasis and Stage of Non-Small Cell Lung Cancer

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Control Subjects
2.2. Sample Collection and Measurement
2.3. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics
3.2. Clinical Data and Risk Factor of Tumor Metastasis and Stage in NSCLC Patients
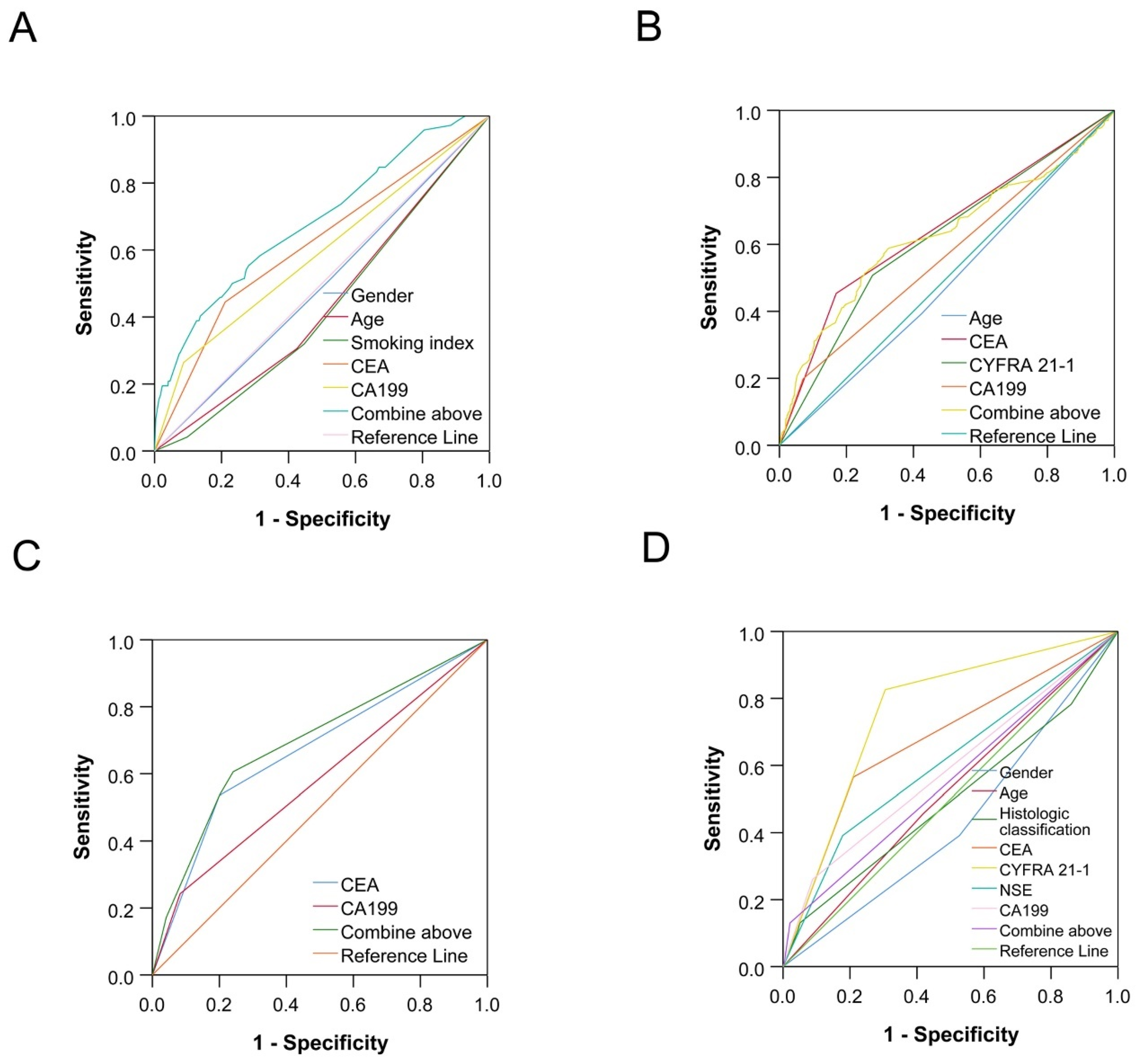
3.3. The Predictions of Single and Combined Factors for Tumor Metastasis and Stage in NSCLC Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Elbeyli, L.; Sanli, M.; Kasap, M.; Gezici, S.; Ozaslan, M.; Akpinar, G. Comparative Proteomics and Bioinformatics Analysis of Tissue from Non-Small Cell Lung Cancer Patients. Curr. Proteom. 2017, 14, 58–77. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 60, 277–300. [Google Scholar] [CrossRef]
- Zhan, M.; Wen, F.; Liu, L.; Chen, Z.; Wei, H.; Zhou, H. JMJD1A promotes tumorigenesis and forms a feedback loop with EZH2/let-7c in NSCLC cells. Tumor Biol. 2016, 37, 11237–11247. [Google Scholar] [CrossRef] [PubMed]
- Funakoshi, T.; Tachibana, I.; Kimura, H.; Takeda, Y.; Kijima, T.; Hoshida, Y.; Nishino, K.; Goto, H.; Yoneda, T.; Kumagai, T.; et al. Expression of tetraspanins in human lung cancer cells: Frequent downregulation of CD9 and its contribution to cell motility in small cell lung cancer. Oncogene 2003, 22, 674–687. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wang, Q.; Liu, Q.; Zhang, Q.; Huang, Q.; Yu, Z. The Serum Tumor Markers in Combination for Clinical Diagnosis of Lung Cancer. Clin. Lab. 2020, 66. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Teng, J.; Zhang, L.; Cong, P.; Yao, Y.; Sun, G.; Liu, Z.; Yu, T.; Liu, M. The Combination of the Tumor Markers Suggests the Histological Diagnosis of Lung Cancer. Biomed. Res. Int. 2017, 2017, 2013989. [Google Scholar] [CrossRef] [PubMed]
- Molina, R.; Auge, J.M.; Escudero, J.M.; Marrades, R.; Viñolas, N.; Carcereny, E.; Ramirez, J.; Filella, X. Mucins CA 125, CA 19.9, CA 15.3 and TAG-72.3 as tumor markers in patients with lung cancer: Comparison with CYFRA 21-1, CEA, SCC and NSE. Tumour Biol. 2008, 29, 371–380. [Google Scholar] [CrossRef]
- Hu, Q.; Xiao, P.; Li, J.; Yu, P. A retrospective analysis of serum tumor markers found in non-small cell lung cancer. J. Cancer Res. 2016, 12, 117–120. [Google Scholar]
- Nisman, B.; Biran, H.; Ramu, N.; Heching, N.; Barak, V.; Peretz, T. The diagnostic and prognostic value of ProGRP in lung cancer. Anticancer. Res. 2009, 29, 4827–4832. [Google Scholar]
- Wang, C.F.; Peng, S.J.; Liu, R.Q.; Yu, Y.J.; Ge, Q.M.; Liang, R.B.; Li, Q.Y.; Li, B.; Shao, Y. The Combination of CA125 and NSE Is Useful for Predicting Liver Metastasis of Lung Cancer. Dis. Markers 2020, 2020, 8850873. [Google Scholar] [CrossRef]
- Wang, L.; Wang, D.; Zheng, G.; Yang, Y.; Du, L.; Dong, Z.; Zhang, X.; Wang, C. Clinical Evaluation and Therapeutic Monitoring Value of Serum Tumor Markers in Lung Cancer. Int. J. Biol. Markers 2016, 31, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Molina, R.; Filella, X.; Augé, J.M.; Fuentes, R.; Bover, I.; Rifa, J.; Moreno, V.; Canals, E.; Viñolas, N.; Marquez, A.; et al. Tumor Markers (CEA, CA 125, CYFRA 21-1, SCC and NSE) in Patients with Non-Small Cell Lung Cancer as an Aid in Histological Diagnosis and Prognosis. Tumor Biol. 2003, 24, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Cedrés, S.; Nuñez, I.; Longo, M.; Martinez, P.; Checa, E.; Torrejón, D.; Felip, E. Serum Tumor Markers CEA, CYFRA21-1, and CA-125 Are Associated with Worse Prognosis in Advanced Non–Small-Cell Lung Cancer (NSCLC). Clin. Lung Cancer 2011, 12, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Bello, M.G.D.; Filiberti, R.A.; Alama, A.; Orengo, A.M.; Mussap, M.; Coco, S.; Vanni, I.; Boccardo, S.; Rijavec, E.; Genova, C.; et al. The role of CEA, CYFRA21-1 and NSE in monitoring tumor response to Nivolumab in advanced non-small cell lung cancer (NSCLC) patients. J. Transl. Med. 2019, 17, 74. [Google Scholar] [CrossRef] [PubMed]
- Shirasu, H.; Ono, A.; Omae, K.; Nakashima, K.; Omori, S.; Wakuda, K.; Kenmotsu, H.; Naito, T.; Murakami, H.; Endo, M.; et al. CYFRA 21-1 predicts the efficacy of nivolumab in patients with advanced lung adenocarcinoma. Tumor Biol. 2018, 40, 101042831876042. [Google Scholar] [CrossRef]
- Li, Q.; Sang, S. Diagnostic Value and Clinical Significance of Combined Detection of Serum Markers CYFRA21-1, SCC Ag, NSE, CEA and ProGRP in Non-Small Cell Lung Carcinoma. Clin. Lab. 2020, 66, 11. [Google Scholar] [CrossRef]
- Kang, S.J.; Cho, Y.R.; Park, G.M.; Ahn, J.M.; Han, S.B.; Lee, J.Y.; Kim, W.J.; Park, D.W.; Lee, S.W.; Kim, Y.H.; et al. Predictors for functionally significant in-stent restenosis: An integrated analysis using coronary angiography, IVUS, and myocardial perfusion imaging. JACC Cardiovasc. Imaging 2013, 6, 1183–1190. [Google Scholar] [CrossRef]
- Vinolas, N.; Molina, R.; Fuentes, R.; Bover, I.; Rifa, J.; Moreno, V.; Canals, E.; Marquez, A.; Barreiro, E.; Borras, J.; et al. Tumor markers (CEA, CA 125, CYFRA 21.1, SCC and NSE) in non small cell lung cancer (NSCLC) patients as an aid in histological diagnosis and prognosis: Comparison with the main clinical and pathological prognostic factors. Lung Cancer 2000, 29, 195. [Google Scholar] [CrossRef]
- Zamcheck, N. The present status of carcinoembryonic antigen (CEA) in diagnosis, detection of recurrence, prognosis and evaluation of therapy of colonic and pancreatic cancer. Clin. Gastroenterol. 1976, 5, 625–638. [Google Scholar] [CrossRef]
- Grunnet, M.; Sorensen, J.B. Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung Cancer 2012, 76, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.N.; Joo, N.S.; Je, S.Y.; Kim, K.M.; Kim, B.T.; Park, S.B.; Cho, D.Y.; Park, R.W.; Lee, D.J. Carcinoembryonic Antigen Level Can be Overestimated in Metabolic Syndrome. J. Korean Med. Sci. 2011, 26, 759–764. [Google Scholar] [CrossRef][Green Version]
- Hall, C.; Clarke, L.; Pal, A.; Buchwald, P.; Eglinton, T.; Wakeman, C.; Frizelle, F. A Review of the Role of Carcinoembryonic Antigen in Clinical Practice. Ann. Coloproctol. 2019, 35, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Hao, C.; Zhang, G.; Zhang, L. Serum CEA levels in 49 different types of cancer and noncancer diseases. Prog. Mol. Biol. Transl. Sci. 2019, 162, 213–227. [Google Scholar] [PubMed]
- Suzuki, Y.; Nakano, T.; Ohno, T.; Abe, A.; Morita, S.; Tsujii, H. Serum CYFRA 21-1 in cervical cancer patients treated with radiation therapy. J. Cancer Res. Clin. Oncol. 2000, 126, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Holdenrieder, S.; Molina, R.; Qiu, L.; Zhi, X.; Rutz, S.; Engel, C.; Kasper-Sauer, P.; Dayyani, F.; Mkorse, C. Technical and clinical performance of a new assay to detect squamous cell carcinoma antigen levels for the differential diagnosis of cervical, lung, and head and neck cancer. Tumour Biol. 2018, 40, 1010428318772202. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.; Velcovsky, H.G.; Morr, H.; Katz, N.; Neu, K.; Eigenbrodt, E. Comparison of the tumor markers tumor M2-PK, CEA, CYFRA 21-1, NSE and SCC in the diagnosis of lung cancer. Anticancer. Res. 2000, 20, 5053–5058. [Google Scholar]
- Jiang, Z.F.; Wang, M.; Xu, J.L. Thymidine kinase 1 combined with CEA, CYFRA21-1 and NSE improved its diagnostic value for lung cancer. Life Sci. 2018, 194, 1–6. [Google Scholar] [CrossRef]
- Zissimopoulos, A.; Stellos, K.; Permenopoulou, V.; Petrakis, G.; Theodorakopoulos, P.; Baziotis, N.; Thalassinos, N. The importance of the tumor marker CYFRA 21-1 in patients with lung cancer after surgery or chemotherapy. Hell. J. Nucl. Med. 2007, 10, 62–66. [Google Scholar]
- Sandoval, J.A.; Malkas, L.H.; Hickey, R.J. Clinical significance of serum biomarkers in pediatric solid mediastinal and abdominal tumors. Int. J. Mol. Sci. 2012, 13, 1126–1153. [Google Scholar] [CrossRef]
- Kamiya, N.; Suzuki, H.; Kawamura, K.; Imamoto, T.; Naya, Y.; Tochigi, N.; Kakuta, Y.; Yamaguchi, K.; Ishikura, H.; Ichikawa, T. Neuroendocrine differentiation in stage D2 prostate cancers. Int. J. Urol. 2008, 15, 423–428. [Google Scholar] [CrossRef]
- Rosati, R.; Adil, M.R.; Ali, M.A.; Eliason, J.; Orosz, A.; Sebestyén, F.; Kalemkerian, G.P. Induction of apoptosis by a short-chain neuropeptide analog in small cell lung cancer. Peptides 1998, 19, 1519–1523. [Google Scholar] [CrossRef]
- Tiseo, M.; Ardizzoni, A.; Cafferata, M.A.; Loprevite, M.; Chiaramondia, M.; Filiberti, R.; Marroniet, P.; Grossi, F.; Paganuzzi, M. Predictive and prognostic significance of neuron-specific enolase (NSE) in non-small cell lung cancer. Anticancer. Res. 2008, 28, 507–513. [Google Scholar] [PubMed]
- Yang, Q.; Zhang, P.; Wu, R.; Lu, K.; Zhou, H. Identifying the Best Marker Combination in CEA, CA125, CY211, NSE, and SCC for Lung Cancer Screening by Combining ROC Curve and Logistic Regression Analyses: Is It Feasible? Dis. Markers 2018, 2018, 2082840. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.J.; Tao, Z.; Gu, W.; Sun, L.H. Clinical observations on the association between diagnosis of lung cancer and serum tumor markers in combination. Asian Pac. J. Cancer Prev. 2013, 14, 4369–4371. [Google Scholar] [CrossRef]
- Chu, X.Y.; Hou, X.B.; Song, W.A.; Xue, Z.Q.; Wang, B.; Zhang, L.B. Diagnostic values of SCC, CEA, Cyfra21-1 and NSE for lung cancer in patients with suspicious pulmonary masses: A single center analysis. Cancer Biol. 2011, 11, 995–1000. [Google Scholar] [CrossRef]
- Hatate, K.; Yamashita, K.; Hirai, K.; Kumamoto, H.; Sato, T.; Ozawa, H.; Nakamura, T.; Onozato, W.; Kokuba, Y.; Ihara, A.; et al. Liver metastasis of colorectal cancer by protein-tyrosine phosphatase type 4A, 3 (PRL-3) is mediated through lymph node metastasis and elevated serum tumor markers such as CEA and CA19-9. Oncol Rep 2008, 20, 737–743. [Google Scholar]


{kind=link}
{kind=link}
| Patient Characteristics | Case or Median | % |
|---|---|---|
| Age | ||
| median (P25–P75, year) | 61 (55–67) | |
| Gender | ||
| male | 1812 | 55.4 |
| female | 1460 | 44.6 |
| Smoking index | ||
| median (P25–P75) | 1.5 (0.00–600) | |
| non-smoking | 1633 | 49.9 |
| ≤600 * | 1009 | 31.2 |
| >600 | 630 | 19.5 |
| Intrapulmonary metastasis | ||
| none | 2656 | 83.8 |
| yes | 512 | 16.2 |
| Lymphatic metastasis | ||
| none | 2147 | 67.6 |
| yes | 1031 | 32.4 |
| Distant metastasis | ||
| none | 2607 | 81.7 |
| yes | 585 | 18.3 |
| Histologic classification | ||
| Squamous carcinoma | 735 | 22.5 |
| Adenocarcinoma | 2354 | 72.0 |
| Adenosquamous carcinoma | 44 | 1.3 |
| Others | 139 | 4.2 |
| Staging | ||
| Ι | 1997 | 61.3 |
| ΙΙ | 503 | 15.4 |
| ΙΙΙ | 175 | 5.4 |
| ΙV | 585 | 17.9 |
| Variables | IM | LM | DM | Staging | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| None | Yes | p | None | Yes | p | None | Yes | p | Ι | ΙΙ | ΙΙΙ | ΙV | p | |
| Gender (case) | ||||||||||||||
| Male | 1417 | 327 | <0.001 | 1079 | 670 | <0.001 | 1403 | 360 | 0.098 | 966 | 346 | 129 | 360 | <0.001 |
| Female | 1239 | 185 | 1068 | 361 | 1204 | 225 | 1031 | 157 * | 46 * | 225 *#& | ||||
| Age (case) | ||||||||||||||
| ≤61 years | 1377 | 221 | <0.001 | 1111 | 494 | 0.047 | 1318 | 290 | 0.701 | 1064 | 206 | 77 | 290 | <0.001 |
| >61 years | 1279 | 291 | 1036 | 537 | 1289 | 295 | 933 | 297 * | 98 * | 295 | ||||
| Smoking index (case) | ||||||||||||||
| non | 1356 | 231 | <0.001 | 1170 | 423 | <0.001 | 1307 | 289 | 0.003 | 1112 | 178 | 52 | 289 | <0.001 |
| 600 | 849 | 140 | 669 | 321 | 837 | 159 | 616 | 176 | 52 | 159 | ||||
| >600 | 451 | 141 | 308 | 287 | 463 | 137 | 268 | 149 * | 71 *# | 137 *#& | ||||
| Variables | IM | LM | DM | ||||||
|---|---|---|---|---|---|---|---|---|---|
| None | Yes | p | None | Yes | p | None | Yes | p | |
| CEA | 3.02 | 6.71 | <0.001 | 2.71 | 5.67 | <0.001 | 2.94 | 10.58 | <0.001 |
| (1.78–5.86) | (3.18–34.55) | (1.64–4.98) | (2.91–25.93) | (1.73–5.47) | (3.43–58.54) | ||||
| SCC-Ag | 0.9 | 0.9 | 0.129 | 0.9 | 1 | <0.001 | 0.9 | 0.9 | 0.45 |
| (0.70–1.30) | (0.60–1.80) | (0.70–1.30) | (070–1.80) | (0.70–1.40) | (0.60–1.70) | ||||
| CYFRA 21-1 | 2.77 | 4.96 | <0.001 | 2.59 | 4.6 | <0.001 | 2.77 | 4.83 | <0.001 |
| (1.92–4.56) | (2.63–10.13) | (1.85–3.95) | (2.63–10.13) | (1.92–4.47) | (2.58–12.57) | ||||
| NSE | 13.32 | 16.5 | <0.001 | 13.4 | 15.2 | <0.001 | 13.36 | 16.09 | <0.001 |
| (11.30–16.35) | (13.00–20.70) | (11.30–16.00) | (12.33–20.70) | (11.30–16.35) | (12.47–23.64) | ||||
| ProGRP | 32.79 | 32.37 | 0.674 | 32.37 | 34.38 | 0.013 | 32.66 | 33.79 | 0.44 |
| (26.23–40.64) | (26.04–38.82) | (26.06–40.28) | (27.90–42.08) | (26.16–40.66) | (27.48–39.34) | ||||
| TPSA | 45.73 | 50.12 | 0.17 | 44.46 | 56.28 | <0.001 | 46.21 | 39.49 | 0.58 |
| (26.10–85.73) | (35.07–87.54) | (25.74–81.91) | (29.61–101.00) | (26.20–85.83) | (25.27–80.74) | ||||
| CA199 | 0.39 | 0.46 | 0.073 | 0.38 | 0.45 | <0.001 | 0.39 | 0.48 | <0.001 |
| (0.26–0.63) | (0.26–1.03) | (0.25–0.61) | (0.31–0.87) | (0.25–0.63) | (0.31–1.05) | ||||
| Variables | I | II | III | IV | p |
|---|---|---|---|---|---|
| CEA | 2.59 (1.57–4.64) | 4.10 (2.45–10.12) * | 5.39 (3.26–15.75) *# | 10.58 (3.43–58.54) *#& | <0.001 |
| SCC-Ag | 0.90 (0.70–1.20) | 1.00 (0.70–2.10) * | 1.10 (0.80–2.90) *# | 0.90 (0.60–1.70) *#& | <0.001 |
| CYFRA 21-1 | 2.50 (1.81–3.68) | 4.21 (2.48–8.56) * | 5.72 (3.62–14.22) *# | 4.83 (2.58–12.57) *#& | <0.001 |
| NSE | 12.93 (11.07–15.60) | 14.72 (12.20–18.59) * | 17.45 (12.82–24.96) *# | 16.09 (12.47–23.64) *# | <0.001 |
| ProGRP | 32.64 (26.15–40.76) | 32.40 (26.01–39.19) | 34.51 (29.14–41.78) | 33.79 (27.48–39.34) | 0.526 |
| TPSA | 44.37 (25.82–82.10) | 56.94 (30.34–118.79) * | 58.57 (45.11–128.41) * | 39.49 (25.27–80.74) #& | <0.001 |
| CA199 | 2.31 (1.35–5.60) | 2.85 (1.36–7.35) * | 3.01 (1.44–8.29) *# | 3.25 (1.43–10.72) * | <0.001 |
| Variables | IM | LM | DM | Staging | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Gender | 0.64 (0.53–0.77) | <0.001 | 0.54 (0.47–0.63) | <0.001 | 0.73 (0.61–0.87) | <0.001 | 0.69 (0.64–0.76) | <0.001 |
| Age | 1.04 (1.03–1.05) | <0.001 | 1.02 (1.01–1.03) | <0.001 | 1.02 (1.01–1.03) | <0.001 | 1.01 (1.01–1.02) | <0.001 |
| Smoking index | ||||||||
| non | Reference | Reference | Reference | Reference | ||||
| 600 | 0.60 (0.48–0.75) | <0.001 | 0.82 (0.69–0.97) | 0.019 | 0.60 (0.48–0.75) | <0.001 | 0.85 (0.78–0.94) | 0.001 |
| >600 | 2.00 (1.64–2.45) | <0.001 | 2.39 (2.00–2.86) | <0.001 | 1.55 (1.27–1.90) | <0.001 | 1.54 (1.39–1.71) | <0.001 |
| Histologic classification | ||||||||
| Squamous carcinoma | Reference | Reference | Reference | Reference | ||||
| Adenocarcinoma | 0.82 (0.66–1.03) | 0.086 | 0.63 (0.74–1.62) | <0.001 | 0.98 (0.77–1.25) | 0.873 | 0.63 (0.54–0.73) | <0.001 |
| Adenosquamous carcinoma | 1.33 (0.62–2.87) | 0.469 | 1.80 (0.96–3.40) | 0.068 | 1.55 (0.72–3.34) | 0.259 | 1.31 (0.75–2.29) | 0.338 |
| Others | 0.52 (0.29–0.93) | 0.027 | 0.91 (0.62–1.34) | 0.912 | 0.95 (0.55–1.64) | 0.858 | 0.84 (0.60–1.19) | 0.331 |
| CEA | 3.19 (2.66–3.82) | <0.001 | 3.60 (3.09–4.19) | <0.001 | 4.27 (3.57–5.11) | <0.001 | 2.40 (2.20–2.62) | <0.001 |
| SCC-Ag | 1.82 (1.49–2.22) | <0.001 | 2.02 (1.70–2.40) | <0.001 | 1.63 (1.34–2.00) | <0.001 | 1.52 (1.38–1.67) | <0.001 |
| CYFRA 21-1 | 4.15 (3.38–5.08) | <0.001 | 4.28 (3.65–5.02) | <0.001 | 3.69 (3.04–4.47) | <0.001 | 2.63 (2.41–2.84) | <0.001 |
| NSE | 3.11 (2.59–3.74) | <0.001 | 2.59 (2.21–3.03) | <0.001 | 2.88 (2.41–3.44) | <0.001 | 1.95 (1.78–2.13) | <0.001 |
| ProGRP | 0.76 (0.18–3.17) | 0.707 | 1.84 (1.07–3.16) | 0.028 | 1.38 (0.55–3.51) | 0.495 | 1.23 (0.89–1.69) | 0.205 |
| TPSA | 0.92 (0.54–1.57) | 0.760 | 1.61 (1.26–2.06) | <0.001 | 0.89 (0.57–1.40) | 0.615 | 1.21 (1.05–1.39) | 0.007 |
| CA199 | 3.82 (2.23–6.54) | <0.001 | 0.32 (0.23–0.44) | <0.001 | 4.00 (2.53–6.31) | <0.001 | 2.08 (1.73–2.50) | <0.001 |
| Variables | IM | LM | DM | Staging | ||||
|---|---|---|---|---|---|---|---|---|
| T | VIF | T | VIF | T | VIF | T | VIF | |
| Gender | 0.635 | 1.576 | 0.633 | 1.580 | 0.636 | 1.572 | 0.633 | 1.581 |
| Age | 0.937 | 1.067 | 0.937 | 1.067 | 0.936 | 1.068 | 0.937 | 1.067 |
| Smoking index | 0.629 | 1.589 | 0.628 | 1.591 | 0.629 | 1.589 | 0.628 | 1.592 |
| Histologic classification | 0.944 | 1.059 | 0.939 | 1.064 | - | - | 0.939 | 1.064 |
| CEA | 0.891 | 1.122 | 0.892 | 1.122 | 0.895 | 1.118 | 0.891 | 1.122 |
| SCC-Ag | 0.900 | 1.111 | 0.896 | 1.116 | 0.911 | 1.097 | 0.896 | 1.116 |
| CYFRA 21-1 | 0.863 | 1.159 | 0.737 | 1.356 | 0.872 | 1.147 | 0.737 | 1.357 |
| NSE | 0.975 | 1.025 | 0.976 | 1.025 | 0.980 | 1.020 | 0.976 | 1.025 |
| TPSA | - | - | 0.797 | 1.254 | - | - | 0.797 | 1.254 |
| CA199 | 0.922 | 1.085 | 0.922 | 1.084 | 0.925 | 1.081 | 0.922 | 1.084 |
| Variables | IM | LM | DM | Staging | ||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Gender | 0.52 (0.29–0.94) | 0.031 | 0.85 (0.61–1.19) | 0.335 | 0.66 (0.39–1.13) | 0.117 | 0.68 (0.49–0.94) | 0.021 |
| Age | 0.58 (0.34–0.99) | 0.045 | 0.64 (0.48–0.83) | 0.001 | 0.66 (0.42–1.03) | 0.068 | 0.76 (0.59–0.98) | 0.036 |
| Smoking index | ||||||||
| non | Reference | Reference | Reference | Reference | ||||
| 600 | 0.53 (0.27–1.03) | 0.059 | 1.00 (0.70–1.42) | 0.987 | 0.66 (0.37–1.15) | 0.144 | 0.95 (0.67–1.34) | 0.775 |
| >600 | 0.28 (0.08–0.99) | 0.048 | 1.22 (0.75–2.00) | 0.413 | 0.45 (0.18–1.11) | 0.082 | 1.03 (0.65–1.64) | 0.889 |
| Histologic classification | ||||||||
| Squamous carcinoma | Reference | Reference | Reference | Reference | ||||
| Adenocarcinoma | 2.69 (0.78–9.31) | 0.119 | 0.92 (0.62–1.38) | 0.695 | - | - | 0.68 (0.47–0.97) | 0.033 |
| Adenosquamous carcinoma | - | - | 1.58 (0.35–7.15) | 0.553 | - | - | 1.05 (0.26–4.31) | 0.948 |
| Others | 1.28 (0.20–8.12) | 0.793 | 1.32 (0.72–2.43) | 0.365 | - | - | 0.87 (0.49–1.54) | 0.628 |
| CEA | 2.66 (1.53–4.63) | <0.001 | 3.08 (2.33–4.07) | <0.001 | 4.51 (2.86–7.12) | <0.001 | 2.85 (2.17–3.75) | <0.001 |
| SCC-Ag | 0.40 (0.14–1.18) | 0.096 | 1.35 (0.95–1.93) | 0.093 | 0.50 (0.24–1.03) | 0.060 | 1.04 (0.74–1.45) | 0.842 |
| CYFRA 21-1 | 1.27 (0.73–2.22) | 0.394 | 2.00 (1.48–2.69) | <0.001 | 1.06 (0.66–1.69) | 0.822 | 2.56 (1.92–3.42) | <0.001 |
| NSE | 1.51 (0.86–2.66) | 0.155 | 1.15 (0.84–1.57) | 0.382 | 1.26 (0.77–2.08) | 0.362 | 1.76 (1.33–2.34) | <0.001 |
| TPSA | - | - | 0.98 (0.72–1.32) | 0.876 | - | - | 0.75 (0.56–1.01) | 0.055 |
| CA199 | 2.80 (1.49–5.17) | 0.001 | 2.04 (1.41–2.96) | <0.001 | 2.20 (1.31–3.69) | 0.003 | 2.20 (1.54–3.14) | <0.001 |
| Variables | IM | LM | DM | Staging | ||||
|---|---|---|---|---|---|---|---|---|
| AUC (95% CI) | p | AUC (95% CI) | p | AUC (95% CI) | p | AUC (95% CI) | p | |
| Gender | 0.49 (0.43–0.56) | 0.862 | - | - | - | - | 0.43 (0.35–0.52) | 0.116 |
| Age | 0.44 (0.38–0.51) | 0.085 | 0.48 (0.45–0.52) | 0.362 | - | - | 0.52 (0.43–0.60) | 0.659 |
| Smoking index | 0.43 (0.37–0.49) | 0.044 | - | - | - | - | - | - |
| Histologic classification | - | - | - | - | - | - | 0.50 (0.40–0.59) | 0.949 |
| CEA | 0.62 (0.55–0.69) | 0.001 | 0.64 (0.61–0.68) | <0.001 | 0.67 (0.61–0.73) | <0.001 | 0.68 (0.59–0.76) | <0.001 |
| CYFRA 21-1 | - | - | 0.62 (0.58–0.65) | <0.001 | - | - | 0.76 (0.70–0.83) | <0.001 |
| NSE | - | - | - | - | - | - | 0.61 (0.52–0.70) | 0.013 |
| CA199 | 0.59 (0.52–0.66) | 0.011 | 0.56 (0.53–0.60) | <0.001 | 0.58 (0.52–0.64) | 0.007 | 0.59 (0.49–0.68) | 0.046 |
| Combine | 0.69 (0.62–0.75) | <0.001 | 0.62 (0.59–0.66) | <0.001 | 0.69 (0.63–0.75) | <0.001 | 0.55 (0.46–0.65) | 0.205 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, C.; Zhao, M.; Hou, S.; Hu, X.; Huang, J.; Wang, H.; Ren, C.; Pan, X.; Zhang, T.; Wu, S.; et al. The Indicative Value of Serum Tumor Markers for Metastasis and Stage of Non-Small Cell Lung Cancer. Cancers 2022, 14, 5064. https://doi.org/10.3390/cancers14205064
Jiang C, Zhao M, Hou S, Hu X, Huang J, Wang H, Ren C, Pan X, Zhang T, Wu S, et al. The Indicative Value of Serum Tumor Markers for Metastasis and Stage of Non-Small Cell Lung Cancer. Cancers. 2022; 14(20):5064. https://doi.org/10.3390/cancers14205064
Chicago/Turabian StyleJiang, Chunyang, Mengyao Zhao, Shaohui Hou, Xiaoli Hu, Jinchao Huang, Hongci Wang, Changhao Ren, Xiaoying Pan, Ti Zhang, Shengnan Wu, and et al. 2022. "The Indicative Value of Serum Tumor Markers for Metastasis and Stage of Non-Small Cell Lung Cancer" Cancers 14, no. 20: 5064. https://doi.org/10.3390/cancers14205064
APA StyleJiang, C., Zhao, M., Hou, S., Hu, X., Huang, J., Wang, H., Ren, C., Pan, X., Zhang, T., Wu, S., Zhang, S., & Sun, B. (2022). The Indicative Value of Serum Tumor Markers for Metastasis and Stage of Non-Small Cell Lung Cancer. Cancers, 14(20), 5064. https://doi.org/10.3390/cancers14205064