

Plasma-Based microRNA Expression Analysis in Advanced Stage NSCLC Patients Treated with Nivolumab
 ,
,  ,
, 

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients’ Characteristics, Healthy Volunteers, and Blood Sample Collection
2.2. miRNA Expression: RNA Isolation from Plasma Samples & Quantitative Real-Time PCR Analysis
2.3. Assessment of Outcome of Immunotherapy
2.4. Statistical Analysis
3. Results
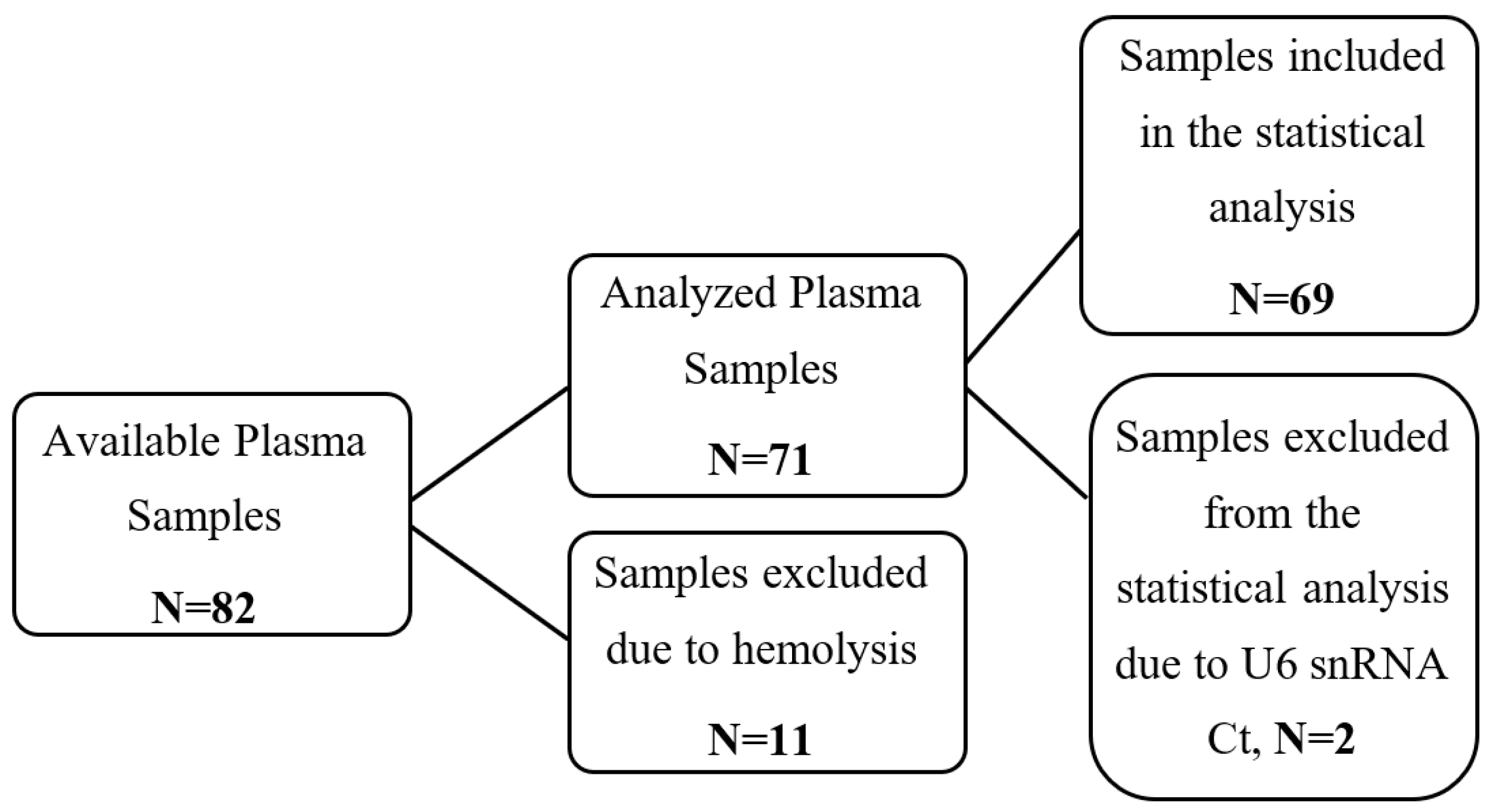
3.1. Study Design and Patients’ Clinicopathological Characteristics
3.2. miRNA Expression and Patients’ Clinicopathological Characteristics
3.3. miRNA Expression and Response to Immunotherapy
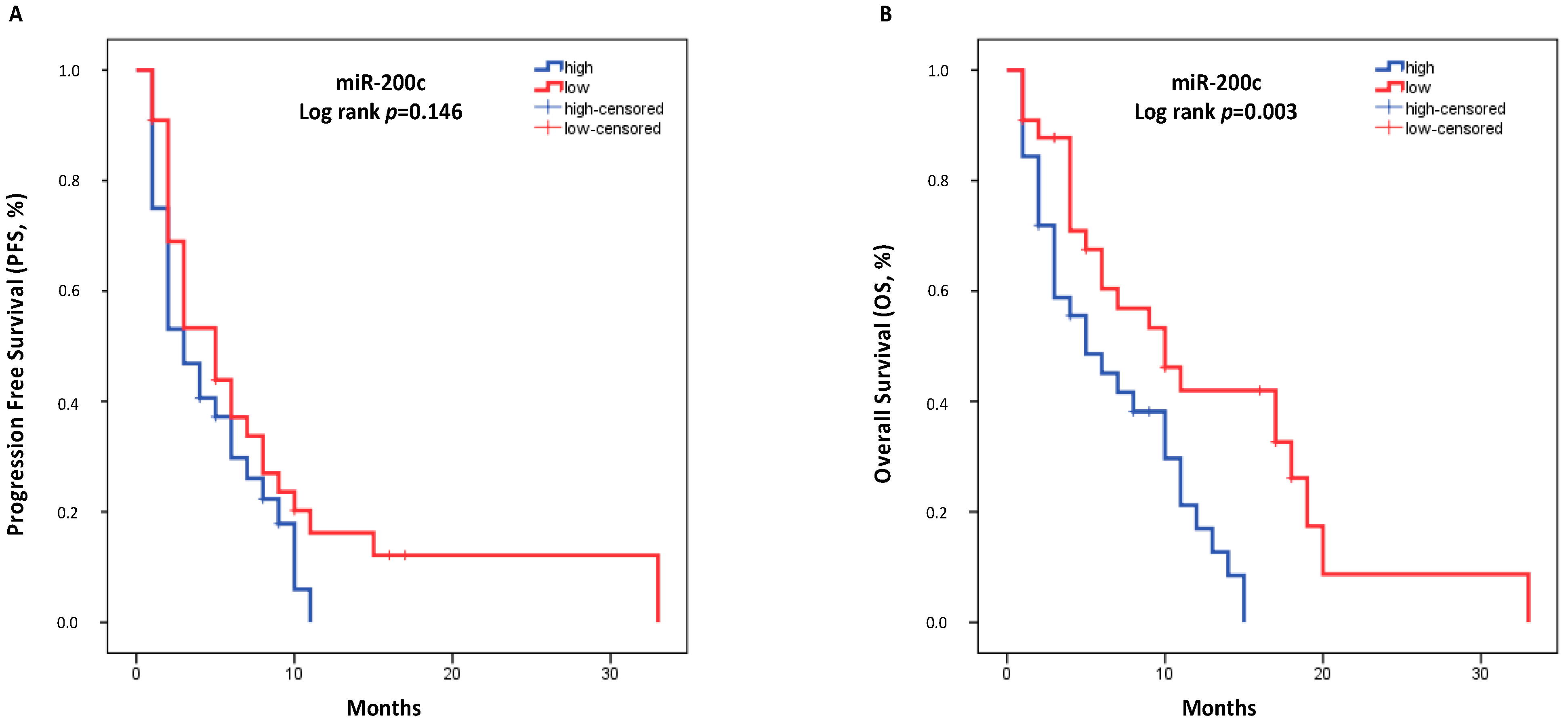
3.4. miRNA Expression and Survival Outcomes
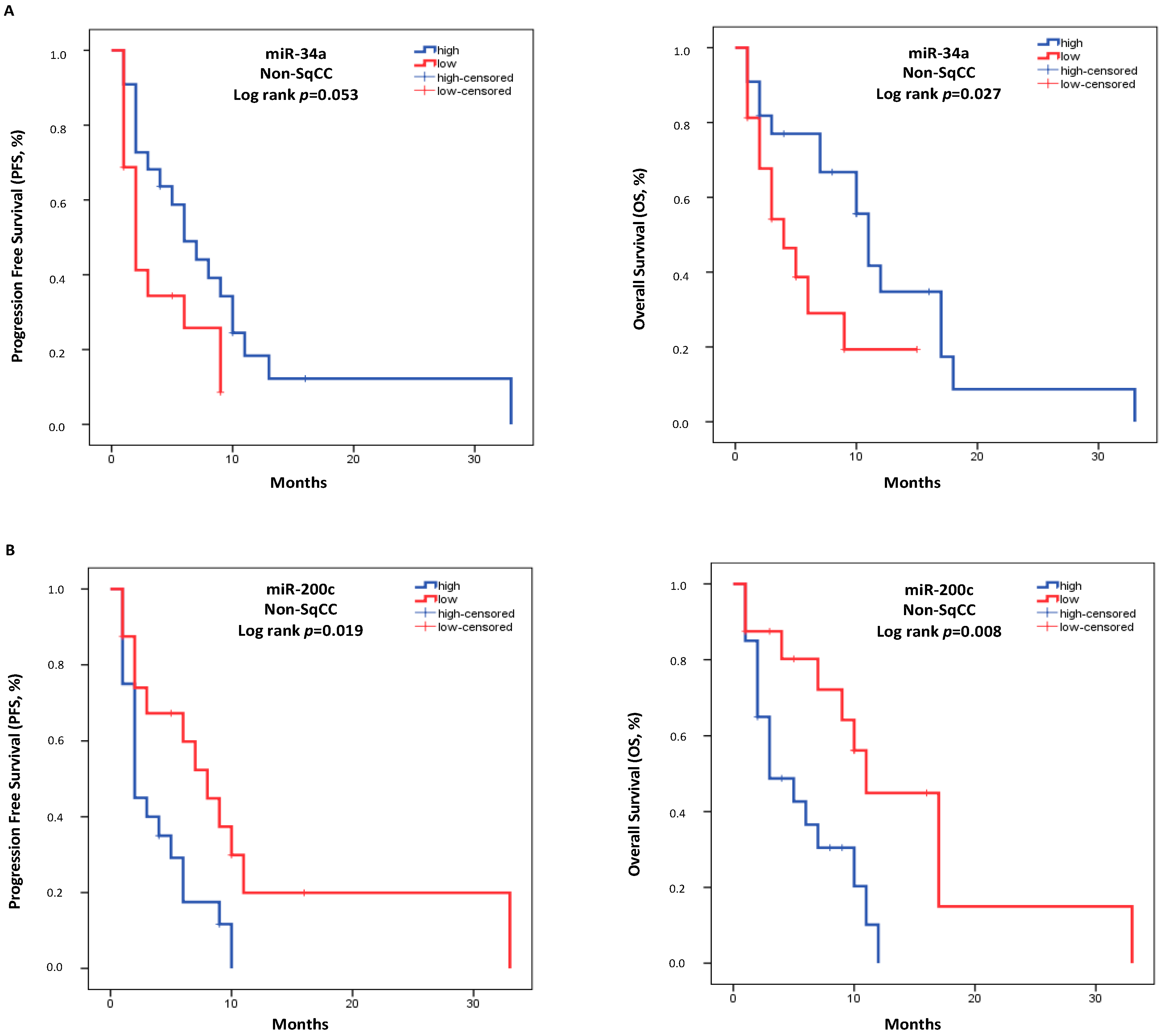
3.5. miRNA Expression and Survival Outcomes in the Histologic Subgroups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| cDNA | Complementary DNA |
| CI | Confidence intervals |
| CT | Computed tomography |
| Ct | Cycle threshold |
| DCR | Disease Control Rate |
| ECOG | Eastern Cooperative Oncology Group |
| EDTA | Ethylenediaminetetraacetic acid |
| EMT | Epithelial to Mesenchymal Transition |
| HR | Hazard ratio |
| ICIs | Immune Checkpoint Inhibitors |
| MDSCs | Myeloid-Derived Suppressor Cells |
| miRNAs | microRNAs |
| MRI | Magnetic resonance imaging |
| NK | Natural killer cells |
| non-SqCC | non-Squamous |
| NSCLC | Non-Small Cell Lung Cancer |
| ORR | Objective Response Rate |
| OS | Overall survival |
| PD | Progression disease |
| PDDC | Prolonged Duration of Disease Control |
| PFS | Progression-free survival |
| PR | Partial response |
| PS | Performance status |
| RT-qPCR | Real-time quantitative polymerase chain reaction |
| SD | Stable disease |
| SqCC | Squamous |
| TILs | Tumor-infiltrating lymphocytes |
| TME | Tumor microenvironment |
| TNBC | Triple-negative breast cancer |
| Tregs | T regulatory cells |
References
- Boeri, M.; Milione, M.; Proto, C.; Signorelli, D.; Russo, G.L.; Galeone, C.; Verri, C.; Mensah, M.; Centonze, G.; Martinetti, A.; et al. Circulating miRNAs and PD-L1 Tumor Expression Are Associated with Survival in Advanced NSCLC Patients Treated with Immunotherapy: A Prospective Study. Clin. Cancer Res. 2019, 25, 2166–2173. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Borghaei, H.; Ramalingam, S.S.; Horn, L.; De Castro Carpeño, J.; Pluzanski, A.; Burgio, M.A.; Garassino, M.; Chow, L.Q.M.; Gettinger, S.; et al. Four-Year Survival with Nivolumab in Patients with Previously Treated Advanced Non-Small-Cell Lung Cancer: A Pooled Analysis. Lancet Oncol. 2019, 20, 1395–1408. [Google Scholar] [CrossRef]
- Vokes, E.E.; Ready, N.; Felip, E.; Horn, L.; Burgio, M.A.; Antonia, S.J.; Frontera, O.A.; Gettinger, S.; Holgado, E.; Spigel, D.; et al. Nivolumab Versus Docetaxel in Previously Treated Advanced Non-Small-Cell Lung Cancer (CheckMate 017 and CheckMate 057): 3-Year Update and Outcomes in Patients with Liver Metastases. Ann. Oncol. 2018, 29, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Filin, I.Y.; Solovyeva, V.V.; Kitaeva, K.V.; Rutland, C.S.; Rizvanov, A.A. Current Trends in Cancer Immunotherapy. Biomedicines 2020, 8, 621. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Shields, M.D.; Marin-Acevedo, J.A.; Pellini, B. Immunotherapy for Advanced Non–Small Cell Lung Cancer: A Decade of Progress. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, e105–e127. [Google Scholar] [CrossRef]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crinò, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab Versus Docetaxel in Previously Treated Patients with Advanced Non–Small-Cell Lung Cancer: Two-Year Outcomes from Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef]
- Borghaei, H.; Gettinger, S.; Vokes, E.E.; Chow, L.Q.M.; Burgio, M.A.; Carpeno, J.D.C.; Pluzanski, A.; Arrieta, O.; Frontera, O.A.; Chiari, R.; et al. Five-Year Outcomes from the Randomized, Phase III Trials CheckMate 017 and 057: Nivolumab Versus Docetaxel in Previously Treated Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2021, 39, 723–733. [Google Scholar] [CrossRef]
- Wang, S.; Xie, K.; Liu, T. Cancer Immunotherapies: From Efficacy to Resistance Mechanisms—Not Only Checkpoint Matters. Front. Immunol. 2021, 12, 690112. [Google Scholar] [CrossRef]
- Jamieson, N.; Maker, A.V. Gene-Expression Profiling to Predict Responsiveness to Immunotherapy. Cancer Gene Ther. 2016, 24, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Spencer, K.R.; Wang, J.; Silk, A.W.; Ganesan, S.; Kaufman, H.L.; Mehnert, J.M. Biomarkers for Immunotherapy: Current Developments and Challenges. Am. Soc. Clin. Oncol. Educ. Book 2016, 36, e493–e503. [Google Scholar] [CrossRef] [PubMed]
- Fridman, W.H.; Pagès, F.; Sautes-Fridman, C.; Galon, J. The Immune Contexture in Human Tumours: Impact on Clinical Outcome. Nat. Cancer 2012, 12, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Anfossi, S.; Babayan, A.; Pantel, K.; Calin, G.A. Clinical Utility of Circulating Non-Coding Rnas—An Update. Nat. Rev. Clin. Oncol. 2018, 15, 541–563. [Google Scholar] [CrossRef]
- Mihnea, D.; Baoqing, C.; Xiao, F.; George, A.C. Key questions About the Checkpoint Blockade-Are Micrornas an Answer? Cancer Biol. Med. 2018, 15, 103–115. [Google Scholar] [CrossRef]
- Mehta, A.; Baltimore, D. MicroRNAs as Regulatory Elements in Immune System logic. Nat. Rev. Immunol. 2016, 16, 279–294. [Google Scholar] [CrossRef]
- Fan, J.; Yin, Z.; Xu, J.; Wu, F.; Huang, Q.; Yang, L.; Jin, Y.; Yang, G. Circulating Micrornas Predict the Response to Anti-PD-1 Therapy in Non-Small Cell Lung Cancer. Genomics 2019, 112, 2063–2071. [Google Scholar] [CrossRef]
- Cortez, M.A.; Ivan, C.; Valdecanas, D.; Wang, X.; Peltier, H.J.; Ye, Y.; Araujo, L.; Carbone, D.P.; Shilo, K.; Giri, D.K.; et al. PDL1 Regulation by p53 Via miR-34. JNCI J. Natl. Cancer Inst. 2015, 108, djv303. [Google Scholar] [CrossRef]
- Chen, L.; Gibbons, D.L.; Goswami, S.; Cortez, M.A.; Ahn, Y.-H.; Byers, L.A.; Zhang, X.; Yi, X.; Dwyer, D.; Lin, W.; et al. Metastasis is Regulated Via Microrna-200/ZEB1 Axis Control of Tumour Cell PD-L1 Expression and Intratumoral Immunosuppression. Nat. Commun. 2014, 5, 5241. [Google Scholar] [CrossRef]
- Lu, L.-F.; Boldin, M.P.; Chaudhry, A.; Lin, L.-L.; Taganov, K.D.; Hanada, T.; Yoshimura, A.; Baltimore, D.; Rudensky, A.Y. Function of miR-146a in Controlling Treg Cell-Mediated Regulation of Th1 Responses. Cell 2010, 142, 914–929. [Google Scholar] [CrossRef]
- Kohlhaas, S.; Garden, O.A.; Scudamore, C.; Turner, M.; Okkenhaug, K.; Vigorito, E. Cutting Edge: The Foxp3 Target miR-155 Contributes to the Development of Regulatory T Cells. J. Immunol. 2009, 182, 2578–2582. [Google Scholar] [CrossRef] [PubMed]
- El-Gazzar, M. microRNAs as Potential Regulators of Myeloid-Derived Suppressor Cell Expansion. Innate Immun. 2014, 20, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Monastirioti, A.; Papadaki, C.; Rounis, K.; Kalapanida, D.; Mavroudis, D.; Agelaki, S. A Prognostic Role for Circulating microRNAs Involved in Macrophage Polarization in Advanced Non-Small Cell Lung Cancer. Cells 2021, 10, 1988. [Google Scholar] [CrossRef] [PubMed]
- Schmittgen, T.D.; Livak, K.J. Analyzing Real-Time PCR Data by the Comparative C(T) Method. Nat. Protoc. 2008, 3, 1101–1108. [Google Scholar] [CrossRef]
- Nishino, M.; Jagannathan, J.P.; Ramaiya, N.H.; van den Abbeele, A.D. Revised RECIST Guideline Version 1.1: What Oncologists Want to Know and What Radiologists Need to Know. Am. J. Roentgenol. 2010, 195, 281–289. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK). JNCI: J. Natl. Cancer Inst. 2005, 97, 1180–1184. [Google Scholar] [CrossRef]
- Cui, M.; Wang, H.; Yao, X.; Zhang, D.; Xie, Y.; Cui, R.; Zhang, X. Circulating MicroRNAs in Cancer: Potential and Challenge. Front. Genet. 2019, 10, 626. [Google Scholar] [CrossRef]
- Pecot, C.V.; Rupaimoole, R.; Yang, D.; Akbani, R.; Ivan, C.; Lu, C.; Wu, S.; Han, H.-D.; Shah, M.Y.; Rodriguez-Aguayo, C.; et al. Tumour Angiogenesis Regulation by the miR-200 Family. Nat. Commun. 2013, 4, 1–14. [Google Scholar] [CrossRef]
- Dykxhoorn, D.M.; Wu, Y.; Xie, H.; Yu, F.; Lal, A.; Petrocca, F.; Martinvalet, D.; Song, E.; Lim, B.; Lieberman, J. miR-200 Enhances Mouse Breast Cancer Cell Colonization to Form Distant Metastases. PLoS ONE 2009, 4, e7181. [Google Scholar] [CrossRef]
- Korpal, M.; Ell, B.J.; Buffa, F.; Ibrahim, T.; Blanco, M.A.; Celià-Terrassa, T.; Mercatali, L.; Khan, Z.; Goodarzi, H.; Hua, Y.; et al. Direct targeting of Sec23a by miR-200s Influences Cancer Cell Secretome and Promotes Metastatic Colonization. Nat. Med. 2011, 17, 1101–1108. [Google Scholar] [CrossRef]
- Dvinge, H.; Git, A.; Gräf, S.; Salmon-Divon, M.; Curtis, C.; Sottoriva, A.; Zhao, Y.; Hirst, M.; Armisen, J.; Miska, E.; et al. The Shaping and Functional Consequences of the Microrna Landscape in Breast Cancer. Nature 2013, 497, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-G.; Zhu, W.-Y.; Huang, Y.-Y.; Ma, L.-N.; Zhou, S.-Q.; Wang, Y.-K.; Zeng, F.; Zhou, J.-H.; Zhang, Y.-K. High Expression of Serum Mir-21 and Tumor Mir-200c Associated with Poor Prognosis in Patients with Lung Cancer. Med. Oncol. 2012, 29, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Jung, S.B.; Kim, J.-S.; Roh, M.S.; Lee, J.H.; Lee, E.H.; Lee, H.W. Expression of microRNA miR-126 and miR-200c Is Associated with Prognosis in Patients with Non-Small Cell Lung Cancer. Virchows Arch. 2014, 465, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Tejero-Villalba, R.; Navarro, A.; Campayo, M.; Viñolas, N.; Marrades, R.M.; Cordeiro, A.; Ruíz-Martínez, M.; Santasusagna, S.; Molins, L.; Ramirez, J.; et al. miR-141 and miR-200c as Markers of Overall Survival in Early-Stage Non-Small Cell Lung Cancer Adenocarcinoma. PLoS ONE 2014, 9, e101899. [Google Scholar] [CrossRef]
- Anastasiadou, E.; Messina, E.; Sanavia, T.; Mundo, L.; Farinella, F.; Lazzi, S.; Megiorni, F.; Ceccarelli, S.; Pontecorvi, P.; Marampon, F.; et al. MiR-200c-3p Contrasts PD-L1 Induction by Combinatorial Therapies and Slows Proliferation of Epithelial Ovarian Cancer through Downregulation of β-Catenin and c-Myc. Cells 2021, 10, 519. [Google Scholar] [CrossRef]
- Cao, Q.; Lu, K.; Dai, S.; Hu, Y.; Fan, W. Clinicopathological and Prognostic Implications of the Mir-200 Family in Patients with Epithelial Ovarian Cancer. Int. J. Clin. Exp. Pathol. 2014, 7, 2392–2401. [Google Scholar]
- Okada, N.; Lin, C.-P.; Ribeiro, M.C.; Biton, A.; Lai, G.; He, X.; Bu, P.; Vogel, H.; Jablons, D.M.; Keller, A.C.; et al. A Positive Feedback Between P53 and Mir-34 Mirnas Mediates Tumor Suppression. Genes Dev. 2014, 28, 438–450. [Google Scholar] [CrossRef]
- Li, W.; Wang, Y.; Liu, R.; Kasinski, A.L.; Shen, H.; Slack, F.J.; Tang, D.G. MicroRNA-34a: Potent Tumor Suppressor, Cancer Stem Cell Inhibitor, and Potential Anticancer Therapeutic. Front. Cell Dev. Biol. 2021, 9, 640587. [Google Scholar] [CrossRef]
- Smolle, M.A.; Calin, H.N.; Pichler, M.; Calin, G.A. Noncoding RNAs and Immune Checkpoints-Clinical Implications as Cancer Therapeutics. FEBS J. 2017, 284, 1952–1966. [Google Scholar] [CrossRef]
- Basak, S.K.; Veena, M.S.; Oh, S.; Lai, C.; Vangala, S.; Elashoff, D.; Fishbein, M.C.; Sharma, S.; Rao, N.P.; Rao, D.; et al. The CD44high Tumorigenic Subsets in Lung Cancer Biospecimens Are Enriched for Low miR-34a Expression. PLoS ONE 2013, 8, e73195. [Google Scholar] [CrossRef]
- Zhao, K.; Cheng, J.; Chen, B.; Liu, Q.; Xu, D.; Zhang, Y. Circulating MicroRNA-34 Family Low Expression Correlates with Poor Prognosis in Patients with Non-Small Cell Lung Cancer. J. Thorac. Dis. 2017, 9, 3735–3746. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Chen, X.; Zhu, D.; Luo, Z.; Yang, M. Low Expression of Circulating MicroRNA-34c is Associated with Poor Prognosis in Triple-Negative Breast Cancer. Yonsei Med. J. 2017, 58, 697–702. [Google Scholar] [CrossRef] [PubMed]
- Gallardo, E.; Navarro, A.; Viñolas, N.; Marrades, R.M.; Diaz, T.; Gel, B.; Quera, A.; Bandres, E.; Garcia-Foncillas, J.; Ramirez, J.; et al. miR-34a as a Prognostic Marker of Relapse in Surgically Resected Non-Small-Cell Lung Cancer. Carcinogenesis 2009, 30, 1903–1909. [Google Scholar] [CrossRef] [PubMed]
- Monastirioti, A.; Papadaki, C.; Rounis, K.; Kalapanida, D.; Makrakis, D.; Vardakis, N.; Mavroudis, D.; Agelaki, S. Mir-34a as Predictor of Immunotherapy Efficacy in NSCLC Patients. J. Clin. Oncol. 2021, 39, e21191. [Google Scholar] [CrossRef]
- Cantoni, C.; Cignarella, F.; Ghezzi, L.; Mikesell, B.; Bollman, B.; Berrien-Elliott, M.; Ireland, A.R.; Fehniger, T.A.; Wu, G.F.; Piccio, L. Mir-223 Regulates the Number and Function of Myeloid-Derived Suppressor Cells in Multiple Sclerosis and Experimental Autoimmune Encephalomyelitis. Acta Neuropathol. 2017, 133, 61–77. [Google Scholar] [CrossRef]
- Jiao, P.; Wang, X.-P.; Luoreng, Z.-M.; Yang, J.; Jia, L.; Ma, Y.; Wei, D.-W. miR-223: An Effective Regulator of Immune Cell Differentiation and Inflammation. Int. J. Biol. Sci. 2021, 17, 2308–2322. [Google Scholar] [CrossRef]
- Zhao, F.-Y.; Han, J.; Chen, X.-W.; Wang, J.; Wang, X.-D.; Sun, J.-G.; Chen, Z.-T. miR-223 Enhances the Sensitivity of Non-Small Cell Lung Cancer Cells to Erlotinib by Targeting the Insulin-Like Growth Factor-1 Receptor. Int. J. Mol. Med. 2016, 38, 183–191. [Google Scholar] [CrossRef]
- Nian, W.; Ao, X.; Wu, Y.; Huang, Y.; Shao, J.; Wang, Y.; Chen, Z.; Chen, F.; Wang, D. miR-223 Functions as a Potent Tumor Suppressor of the Lewis Lung Carcinoma Cell Line by Targeting Insulin-Like Growth Factor-1 Receptor and Cyclin-Dependent Kinase 2. Oncol. Lett. 2013, 6, 359–366. [Google Scholar] [CrossRef]
- D’Antona, P.; Cattoni, M.; Dominioni, L.; Poli, A.; Moretti, F.; Cinquetti, R.; Gini, E.; Daffrè, E.; Noonan, D.M.; Imperatori, A.; et al. Serum miR-223: A Validated Biomarker for Detection of Early-Stage Non–Small Cell Lung Cancer. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1926–1933. [Google Scholar] [CrossRef]
- Luo, P.; Wang, Q.; Ye, Y.; Zhang, J.; Lu, D.; Cheng, L.; Zhou, H.; Xie, M.; Wang, B. MiR-223-3p Functions as a Tumor Suppressor in Lung Squamous Cell Carcinoma by miR-223-3p-Mutant p53 Regulatory Feedback Loop. J. Exp. Clin. Cancer Res. 2019, 38, 1–12. [Google Scholar] [CrossRef]
- Dong, J.; Liu, Y.; Liao, W.; Liu, R.; Shi, P.; Wang, L. miRNA-223 is a Potential Diagnostic and Prognostic Marker for Osteosarcoma. J. Bone Oncol. 2016, 5, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhu, X.; Han, B.; Ji, L.; Yao, L.; Wang, Z. High Expression of microRNA-223 Indicates a Good Prognosis in Triple-Negative Breast Cancer. Front. Oncol. 2021, 11, 630432. [Google Scholar] [CrossRef] [PubMed]
- Esaba, R.; Sorensen, D.L.; Booth, S.A. MicroRNA-146a: A Dominant, Negative Regulator of the Innate Immune Response. Front. Immunol. 2014, 5, 578. [Google Scholar] [CrossRef]
- Testa, U.; Pelosi, E.; Castelli, G.; Labbaye, C. miR-146 and miR-155: Two Key Modulators of Immune Response and Tumor Development. Non-Coding RNA 2017, 3, 22. [Google Scholar] [CrossRef]
- Park, H.; Huang, X.; Lu, C.; Cairo, M.S.; Zhou, X. MicroRNA-146a and MicroRNA-146b Regulate Human Dendritic Cell Apoptosis and Cytokine Production by Targeting TRAF6 and IRAK1 Proteins. J. Biol. Chem. 2015, 290, 2831–2841. [Google Scholar] [CrossRef]
- Shahriar, A.; Shiva, G.G.-A.; Ghader, B.; Farhad, J.; Hosein, A.; Parsa, H. The Dual Role of Mir-146a In Metastasis and Disease Progression. Biomed. Pharmacother. 2020, 126, 110099. [Google Scholar] [CrossRef]
- Wang, C.; Guan, S.; Liu, F.; Chen, X.; Shanghui, G.; Wang, D.; Nesa, E.U.; Wang, X.; Bao, C.; Wang, N.; et al. Prognostic and Diagnostic Potential of Mir-146a in Oesophageal Squamous Cell Carcinoma. Br. J. Cancer 2016, 114, 290–297. [Google Scholar] [CrossRef]
- Wilczyński, M.; Żytko, E.; Szymańska, B.; Dzieniecka, M.; Nowak, M.; Danielska, J.; Stachowiak, G.; Wilczyński, J.R. Expression of miR-146a in Patients with Ovarian Cancer and Its Clinical Significance. Oncol. Lett. 2017, 14, 3207–3214. [Google Scholar] [CrossRef]
- Chen, G.; Umelo, I.; Lv, S.; Teugels, E.; Fostier, K.; Kronenberger, P.; Dewaele, A.; Sadones, J.; Geers, C.; De Grève, J. miR-146a Inhibits Cell Growth, Cell Migration and Induces Apoptosis in Non-Small Cell Lung Cancer Cells. PLoS ONE 2013, 8, e60317. [Google Scholar] [CrossRef]
- Pavel, A.B.; Campbell, J.D.; Liu, G.; Elashoff, D.; Dubinett, S.; Smith, K.; Whitney, D.; Lenburg, M.E.; Spira, A. Alterations in Bronchial Airway miRNA Expression for Lung Cancer Detection. Cancer Prev. Res. 2017, 10, 651–659. [Google Scholar] [CrossRef]
- Becker, N.; Lockwood, C.M. Pre-Analytical Variables in miRNA Analysis. Clin. Biochem. 2013, 46, 861–868. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.S.; Milosevic, D.; Reddi, H.V.; Grebe, S.K.; Algeciras-Schimnich, A. Analysis of Circulating MicroRNA: Preanalytical and Analytical Challenges. Clin. Chem. 2011, 57, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Indini, A.; Rijavec, E.; Grossi, F. Circulating Biomarkers of Response and Toxicity of Immunotherapy in Advanced Non-Small Cell Lung Cancer (NSCLC): A Comprehensive Review. Cancers 2021, 13, 1794. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, A.R.; Sandhu, V.; Sprauten, M.; Flote, V.G.; Kure, E.H.; Brustugun, O.T.; Helland, A. Circulating microRNAs Associated with Prolonged Overall Survival in Lung Cancer Patients Treated with Nivolumab. Acta Oncol. 2018, 57, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Cui, C.; Cui, Q. The Relationship of Human Tissue Micrornas with Those from Body Fluids. Sci. Rep. 2020, 10, 5644. [Google Scholar] [CrossRef]
- Cojocneanu, R.; Braicu, C.; Raduly, L.; Jurj, A.; Zanoaga, O.; Magdo, L.; Irimie, A.; Muresan, M.-S.; Ionescu, C.; Grigorescu, M.; et al. Plasma and Tissue Specific miRNA Expression Pattern and Functional Analysis Associated to Colorectal Cancer Patients. Cancers 2020, 12, 843. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients | SqCC | Non-SqCC | |||||
|---|---|---|---|---|---|---|---|
| Characteristic | N | % | N | % | N | % | p Value |
| Number of patients | 69 | 31 | 44.9 | 38 | 55.1 | ||
| Gender | 0.009 a | ||||||
| Male | 58 | 84.1 | 30 | 96.8 | 28 | 73.7 | |
| Female | 11 | 15.9 | 1 | 3.2 | 10 | 26.3 | |
| Age (years) | 0.050 a | ||||||
| median (range) | 70.5 (39–82) | 72 (55–81) | 69 (39–82) | ||||
| ECOG PS | 0.553 a | ||||||
| 0 | 24 | 34.8 | 9 | 29.0 | 15 | 39.5 | |
| 1 | 31 | 44.9 | 16 | 51.6 | 15 | 39.5 | |
| 2 | 14 | 20.2 | 6 | 19.3 | 8 | 21.1 | |
| Smoking Status | 0.052 | ||||||
| Current Smoker | 42 | 60.9 | 15 | 48.4 | 27 | 71.1 | |
| Former Smoker | 23 | 33.3 | 15 | 48.4 | 8 | 21.1 | |
| Never Smoker | 4 | 5.8 | 1 | 3.2 | 3 | 7.9 | |
| Histology | ns a | ||||||
| Non-SqCC | 38 | 55.1 | |||||
| Squamous | 31 | 44.9 | |||||
| Number of metastatic sites | 0.217 a | ||||||
| 0 | 2 | 2.9 | 1 | 3.2 | 1 | 2.6 | |
| 1 | 16 | 23.1 | 9 | 29.0 | 7 | 18.4 | |
| 2 | 31 | 44.9 | 17 | 54.8 | 14 | 36.8 | |
| ≥3 | 20 | 29.0 | 4 | 12.9 | 16 | 42.1 | |
| Line of Immunotherapy Treatment | 0.083 | ||||||
| 2nd line | 59 | 85.5 | 29 | 93.5 | 30 | 78.9 | |
| 3rd line | 10 | 14.5 | 2 | 6.5 | 8 | 21.1 | |
| Response | 0.454 a | ||||||
| PR | 8 | 11.6 | 2 | 6.5 | 6 | 15.8 | |
| SD | 28 | 40.6 | 14 | 45.2 | 14 | 36.8 | |
| PD | 33 | 47.8 | 15 | 48.4 | 18 | 47.4 | |
| Response | ORR | DCR | PDDC | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Histology | SqCC | Non-SqCC | SqCC | Non-SqCC | SqCC | Non-SqCC | |||||||||||||
| Expression Levels | PR (%) | SD + PD (%) | p Value | PR (%) | SD + PD (%) | p Value | PR + SD (%) | PD (%) | p Value | PR + SD (%) | PD (%) | p Value | PR + SD > 6 Months (%) | SD < 6 Months + PD (%) | p Value | PR + SD > 6 Months (%) | SD < 6 Months + PD (%) | p Value | |
| miR-34a | High | 7.1 | 92.9 | 0.708 | 22.7 | 77.3 | 0.180 | 50.0 | 50.0 | 0.578 | 59.1 | 40.9 | 0.038 * | 28.6 | 71.4 | 0.637 | 50.0 | 50.0 | 0.111 |
| Low | 5.9 | 94.1 | 6.2 | 93.8 | 47.1 | 52.9 | 25.0 | 75.0 | 29.4 | 70.6 | 25.0 | 75.0 | |||||||
| miR-146a | High | 7.7 | 92.3 | 0.671 | 13.0 | 87.0 | 0.444 | 61.5 | 38.5 | 0.189 | 39.1 | 60.9 | 0.299 | 53.8 | 46.2 | 0.014 * | 30.4 | 69.6 | 0.142 |
| Low | 5.6 | 94.4 | 20.0 | 80.0 | 38.9 | 61.1 | 53.3 | 46.7 | 11.1 | 88.9 | 53.3 | 46.7 | |||||||
| miR-155 | High | 7.1 | 92.9 | 0.708 | 22.7 | 77.3 | 0.180 | 64.3 | 35.7 | 0.106 | 45.5 | 54.5 | 0.590 | 42.9 | 57.1 | 0.127 | 36.4 | 63.6 | 0.449 |
| Low | 5.9 | 94.1 | 6.2 | 93.8 | 35.3 | 64.7 | 43.8 | 56.2 | 17.6 | 82.4 | 43.8 | 56.2 | |||||||
| miR-200b | High | 9.1 | 90.9 | 0.591 | 20.8 | 79.2 | 0.264 | 54.5 | 45.5 | 0.447 | 41.7 | 58.3 | 0.435 | 45.5 | 54.5 | 0.140 | 37.5 | 62.5 | 0.505 |
| Low | 5.0 | 95.0 | 7.1 | 92.9 | 45.0 | 55.0 | 50.0 | 50.0 | 20.0 | 80.0 | 42.9 | 57.1 | |||||||
| mir-200c | High | 8.3 | 91.7 | 0.665 | 5.0 | 95.0 | 0.049 * | 58.3 | 41.7 | 0.413 | 30.0 | 70.0 | 0.106 | 41.7 | 58.3 | 0.263 | 20.0 | 80.0 | 0.028 * |
| Low | 5.9 | 94.1 | 31.2 | 68.8 | 47.1 | 52.9 | 56.2 | 43.8 | 23.5 | 76.5 | 56.2 | 43.8 | |||||||
| miR-223 | High | 7.1 | 92.9 | 0.708 | 13.6 | 86.4 | 0.502 | 57.1 | 42.9 | 0.300 | 45.5 | 54.5 | 0.590 | 50.0 | 50.0 | 0.026 * | 36.4 | 63.6 | 0.449 |
| Low | 5.9 | 94.1 | 18.8 | 81.2 | 41.2 | 58.8 | 43.8 | 56.2 | 11.8 | 88.2 | 43.8 | 56.2 | |||||||
| Variable | Progression Free Survival (PFS) | Overall Survival (OS) | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (<60 vs. ≥60) | 1.106 (0.558–2.192) | 0.773 | - | - | 1.105 (0.518–2.356) | 0.796 | - | - |
| Gender (male vs. female) | 1.149 (0.564–2.341) | 0.702 | - | - | 1.361 (0.633–2.929) | 0.430 | - | - |
| Smoker (Yes vs. No) | 1.679 (0.522–5.403) | 0.384 | - | - | 2.446 (0.589–10.154) | 0.218 | - | - |
| ECOG PS (≥2 vs. 0–1) | 1.804 (0.981–3.318) | 0.058 | - | - | 2.295 (1.223–4.305) | 0.010 * | 1.819 (0.949–3.486) | 0.071 |
| Histology (SqCC vs. Non-SqCC) | 1.197 (0.712–2.011) | 0.497 | - | - | 1.010 (0.584–1.748) | 0.971 | - | - |
| Immunotherapy Line (2nd vs. 3rd) | 1.060 (0.534–2.104) | 0.868 | - | - | 1.030 (0.497–2.134) | 0.936 | - | - |
| No. of Metastatic Sites (≥3 vs. 0–2) | 1.202 (0.679–2.125) | 0.528 | - | - | 1.760 (0.971–3.189) | 0.062 | - | - |
| miR-34a (low vs. high) | 1.424 (0.848–2.390) | 0.181 | - | - | 1.083 (0.623–1.881) | 0.778 | - | - |
| miR-146a (high vs. low) | 1.110 (0.662–1.861) | 0.693 | - | - | 1.180 (0.678–2.052) | 0.558 | - | - |
| miR-155 (high vs. low) | 1.039 (0.616–1.752) | 0.885 | - | - | 1.379 (0.785–2.426) | 0.264 | - | - |
| miR-200b (high vs. low) | 1.076 (0.642–1.803) | 0.781 | - | - | 1.618 (0.952–2.828) | 0.092 | - | - |
| miR-200c (high vs. low) | 1.438 (0.838–2.468) | 0.187 | - | - | 2.382 (1.291–4.393) | 0.005 * | 2.243 (1.208–4.163) | 0.010 * |
| miR-223 (high vs. low) | 1.163 (0.693–1.952) | 0.568 | - | - | 1.379 (0.788–2.412) | 0.260 | - | - |
| Variable | Progression Free Survival (PFS) | Overall Survival (OS) | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (<60 vs. ≥60) | 1.247 (0.555–2.806) | 0.593 | - | - | 1.066 (0.444–2.557) | 0.886 | - | - |
| Gender (male vs. female) | 1.114 (0.498–2.494) | 0.792 | - | - | 1.261 (0.518–3.069) | 0.610 | - | - |
| Smoker (Yes vs. No) | 2.094 (0.493–8.889) | 0.316 | - | - | 5.059 (0.670–38-183) | 0.116 | - | - |
| ECOG PS (≥2 vs. 0–1) | 1.876 (0.813–4.330) | 0.141 | - | - | 1.663 (0.715–3.869) | 0.237 | - | - |
| Immunotherapy Line (2nd vs. 3rd) | 1.029 (0.456–2.324) | 0.945 | - | - | 1.316 (0.564–3.071) | 0.526 | - | - |
| No. of Metastatic Sites (≥3 vs. 0–2) | 1.314 (0.636–2.712) | 0.461 | - | - | 1.646 (0.749–3.615) | 0.215 | - | - |
| miR-34a (low vs. high) | 1.970 (0.918–4.226) | 0.082 | - | - | 2.500 (1.050–5.952) | 0.038 * | 3.189 (1.193–8.527) | 0.021* |
| miR-146a (high vs. low) | 1.286 (0.621–2.664) | 0.499 | - | - | 1.423 (0.622–3.252) | 0.403 | - | - |
| miR-155 (high vs. low) | 1.203 (0.583–2.482) | 0.617 | - | - | 1.198 (0.543–2.643) | 0.655 | - | - |
| miR-200b (high vs. low) | 1.061 (0.507–2.221) | 0.874 | - | - | 1.642 (0.712–3.787) | 0.245 | - | - |
| miR-200c (high vs. low) | 2.346 (1.053–5.226) | 0.037* | - | - | 3.112 (1.247–7.766) | 0.015 * | 2.809 (1.116–7.074) | 0.028* |
| miR-223 (high vs. low) | 1.245 (0.603–2.567) | 0.554 | - | - | 1.759 (0.753–4.108) | 0.192 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monastirioti, A.; Papadaki, C.; Kalapanida, D.; Rounis, K.; Michaelidou, K.; Papadaki, M.A.; Mavroudis, D.; Agelaki, S. Plasma-Based microRNA Expression Analysis in Advanced Stage NSCLC Patients Treated with Nivolumab. Cancers 2022, 14, 4739. https://doi.org/10.3390/cancers14194739
Monastirioti A, Papadaki C, Kalapanida D, Rounis K, Michaelidou K, Papadaki MA, Mavroudis D, Agelaki S. Plasma-Based microRNA Expression Analysis in Advanced Stage NSCLC Patients Treated with Nivolumab. Cancers. 2022; 14(19):4739. https://doi.org/10.3390/cancers14194739
Chicago/Turabian StyleMonastirioti, Alexia, Chara Papadaki, Despoina Kalapanida, Konstantinos Rounis, Kleita Michaelidou, Maria A. Papadaki, Dimitrios Mavroudis, and Sofia Agelaki. 2022. "Plasma-Based microRNA Expression Analysis in Advanced Stage NSCLC Patients Treated with Nivolumab" Cancers 14, no. 19: 4739. https://doi.org/10.3390/cancers14194739
APA StyleMonastirioti, A., Papadaki, C., Kalapanida, D., Rounis, K., Michaelidou, K., Papadaki, M. A., Mavroudis, D., & Agelaki, S. (2022). Plasma-Based microRNA Expression Analysis in Advanced Stage NSCLC Patients Treated with Nivolumab. Cancers, 14(19), 4739. https://doi.org/10.3390/cancers14194739