
Survival Benefit of Adjuvant Chemotherapy in Pulmonary Carcinoid Tumors



Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
- Study contains subjects who were surgically treated for well-differentiated typical or atypical carcinoid.
- Study must contain patients that received chemotherapy.
- Study must give a recommendation, whether qualitative or quantitative, concerning the benefit of chemotherapy if any.
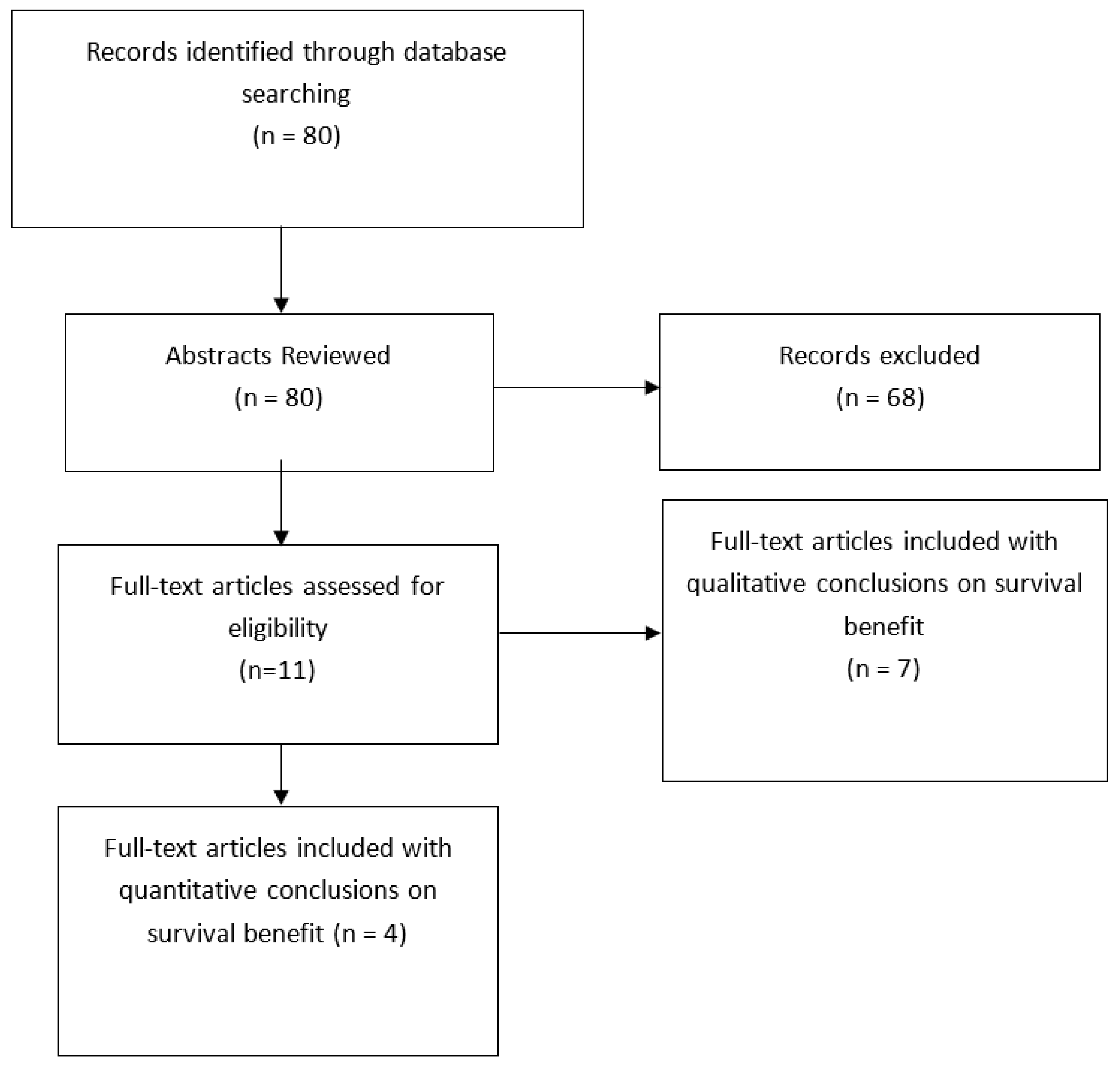
2.2. Study Selection
2.3. Data Collection
2.4. Study Risk Bias Assessment
2.5. Additional Analyses
3. Results
3.1. Main Results
3.2. Subgroup Analysis
4. Discussion
4.1. Clinical Implications
4.1.1. Survival Benefit with Adjuvant therapy
4.1.2. Survival Benefit Based on Nodal Status, Ki-67 Index, and Metastasis
4.1.3. Current Guideline Based Therapy
4.2. Genomics of Carcinoid Tumors
4.2.1. Profiling of Carcinoid Tumors
4.2.2. Genomic Spectrum of Carcinoids
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bertino, E.M.; Confer, P.D.; Colonna, J.E.; Ross, P.; Otterson, G.A. Pulmonary neuroendocrine/carcinoid tumors: A review article. Cancer 2009, 115, 4434–4441. [Google Scholar] [CrossRef]
- Hendifar, A.E.; Marchevsky, A.M.; Tuli, R. Neuroendocrine tumors of the lung: Current challenges and advances in the diagnosis and management of well-differentiated disease. J. Thorac. Oncol. 2017, 12, 425–436. [Google Scholar] [CrossRef]
- Gosain, R.; Mukherjee, S.; Yendamuri, S.S.; Iyer, R. Management of typical and atypical pulmonary carcinoids based on different established guidelines. Cancers 2018, 10, 510. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Baudin, E.; Ferolla, P.; Filosso, P.; Garcia-Yuste, M.; Lim, E.; Oberg, K.; Pelosi, G.; Perren, A.; Rossi, R.E.; et al. Pulmonary neuroendocrine (carcinoid) tumors: European neuroendocrine tumor society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids. Ann. Oncol. 2015, 26, 1604–1620. [Google Scholar] [CrossRef]
- Kaltsas, G.; Caplin, M.; Davies, P.; Ferone, D.; Garcia-Carbonero, R.; Grozinsky-Glasberg, S.; Hörsch, D.; Tiensuu Janson, E.; Kianmanesh, R.; Kos-Kudla, B.; et al. ENETS consensus guidelines for the standards of care in neuroendocrine tumors: Pre- and perioperative therapy in patients with neuroendocrine tumors. Neuroendocrinology 2017, 105, 245–254. [Google Scholar] [CrossRef]
- Noel-Savina, E.; Descourt, R. Focus on treatment of lung carcinoid tumor. OncoTargets Ther. 2013, 6, 1533–1537. [Google Scholar] [CrossRef] [PubMed]
- Tsoukalas, N.; Baxevanos, P.; Aravantinou-Fatorou, E.; Tolia, M.; Galanopoulos, M.; Tsapakidis, K.; Kyrgias, G.; Toumpanakis, C.; Kaltsas, G. Advances on systemic treatment for lung neuroendocrine neoplasms. Ann. Transl. Med. 2018, 6, 146. [Google Scholar] [CrossRef]
- Clark, O.H.; Benson, A.B., III; Berlin, J.D.; Choti, M.A.; Doherty, G.M.; Engstrom, P.F.; Gibbs, J.F.; Heslin, M.J.; Kessinger, A.; Kulke, M.H.; et al. NCCN clinical practice guidelines in oncology: Neuroendocrine tumors. J. Natl. Compr. Cancer Netw. 2009, 7, 712–747. [Google Scholar]
- Phan, A.T.; Oberg, K.; Choi, J.; Harrison, J.; Lynn, H.; Hassan, M.M.; Strosberg, J.R.; Krenning, E.P.; Kocha, W.; Woltering, E.A.; et al. NANETS consensus guideline for the diagnosis and management of neuroendocrine tumors: Well-differentiated neuroendocrine tumors of the thorax (includes lung and thymus). Pancreas 2010, 39, 784–798. [Google Scholar] [CrossRef]
- Öberg, K.; Hellman, P.; Ferolla, P.; Papotti, M. Neuroendocrine bronchial and thymic tumors: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23 (Suppl. A7), vii120–vii123. [Google Scholar] [CrossRef]
- Nussbaum, D.P.; Speicher, P.J.; Gulack, B.C.; Hartwig, M.G.; Onaitis, M.W.; D’Amico, T.A.; Berry, M.F. Defining the role of adjuvant chemotherapy after lobectomy for typical bronchopulmonary carcinoid tumors. Ann. Thorac. Surg. 2015, 99, 428–434. [Google Scholar] [CrossRef]
- Anderson, K.L.; Mulvihill, M.S.; Speicher, P.J.; Yerokun, B.A.; Gulack, B.C.; Nussbaum, D.P.; Harpole, D.H.; D’Amico, T.A.; Berry, M.F.; Hartwig, M.G. Adjuvant chemotherapy does not confer superior survival in patients with atypical carcinoid tumors. Ann. Thorac. Surg. 2017, 104, 1221–1230. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Zang, R.; Liu, L.; Dan, X.; Gao, S. Long-term outcomes and prognostic factors of patients with surgically treated pulmonary atypical carcinoid tumors: Our institutional experience with 68 patients. J. Thorac. Dis. 2018, 10, 4204–4211. [Google Scholar] [CrossRef] [PubMed]
- Wegner, R.E.; Abel, S.; Hasan, S.; Horne, Z.D.; Colonias, A.; Weksler, B.; Verma, V. The role of adjuvant therapy for atypical bronchopulmonary carcinoids. Lung Cancer 2019, 131, 90–94. [Google Scholar] [CrossRef]
- Gosain, R.; Groman, A.; Yendamuri, S.S.; Iyer, R.; Mukherjee, S. Role of adjuvant chemotherapy in pulmonary carcinoids: An NCDB analysis. Anticancer Res. 2019, 39, 6835–6842. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, X.; Lu, T.; Li, M.; Zhao, M.; Yang, X.; Ma, K.; Wang, S.; Zhan, C.; Liu, Y.; et al. Assessment of the prognostic factors in patients with pulmonary carcinoid tumor: A population-based study. Cancer Med. 2018, 7, 2434–2441. [Google Scholar] [CrossRef]
- Tancredi, A.; Muscarella, L.; la Torre, A.; Scaramuzzi, R.; Valori, V.; Fazio, V.; Scaramuzzi, G. The post-surgical long-term behaviour of lung carcinoid tumours. Indian J. Surg. 2015, 77, 481–485. [Google Scholar] [CrossRef]
- Furqan, M.; Tien, Y.; Schroeder, M.C.; Parekh, K.R.; Keech, J.; Allen, B.G.; Thomas, A.; Zhang, J.; Clamon, G.; Abu Hejleh, T. Lobar versus sub-lobar surgery for pulmonary typical carcinoid, a population-based analysis. J. Thorac. Dis. 2018, 10, 5850–5859. [Google Scholar] [CrossRef]
- Chong, C.R.; Wirth, L.J.; Nishino, M.; Chen, A.B.; Sholl, L.M.; Kulke, M.H.; Mcnamee, C.J.; Jänne, P.A.; Johnson, B.E. Chemotherapy and irradiation for locally advanced and metastatic pulmonary carcinoid tumors. Lung Cancer 2014, 86, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Forde, P.M.; Hooker, C.M.; Boikos, S.A.; Petrini, I.; Giaccone, G.; Rudin, C.M.; Yang, S.C.; Illei, P.B.; Hann, C.L.; Ettinger, D.S.; et al. Systemic therapy, clinical outcomes, and overall survival in locally advanced or metastatic pulmonary carcinoid: A brief report. J. Thorac. Oncol. 2014, 9, 414–418. [Google Scholar] [CrossRef]
- Robelin, P.; Hadoux, J.; Forestier, J.; Planchard, D.; Hervieu, V.; Berdelou, A.; Scoazec, J.; Valette, P.; Leboulleux, S.; Ducreux, M.; et al. Characterization, prognosis, and treatment of patients with metastatic lung carcinoid tumors. J. Thorac. Oncol. 2019, 14, 993–1002. [Google Scholar] [CrossRef]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing but NET: A review of neuroendocrine tumors and carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef] [PubMed]
- Boland, J.M.; Kroneman, T.N.; Jenkins, S.M.; Simone, B.S.P.; Terra, M.D.; Xie, H.; Molina, J.; Mounajjed, T.; Roden, A.C. Ki-67 labeling index in pulmonary carcinoid tumors: Comparison between small biopsy and resection using tumor tracing and hot spot methods. Arch. Pathol. Lab. Med. 2020, 144, 982–990. [Google Scholar] [CrossRef]
- Marchiò, C.; Gatti, G.; Massa, F.; Bertero, L.; Filosso, P.; Pelosi, G.; Cassoni, P.; Volante, M.; Papotti, M. Distinctive pathological and clinical features of lung carcinoids with high proliferation index. Virchows Arch. 2017, 471, 713–720. [Google Scholar] [CrossRef]
- Chirieac, L.R. Ki-67 expression in pulmonary tumors. Transl. Lung Cancer Res. 2016, 5, 547–551. [Google Scholar] [CrossRef]
- Swarts, D.R.A.; Rudelius, M.; Claessen, S.M.H.; Cleutjens, J.P.; Seidl, S.; Volante, M.; Ramaekers, F.C.S.; Speel, E.J.M. Limited additive value of the ki-67 proliferative index on patient survival in world health organization-classified pulmonary carcinoids. Histopathology 2017, 70, 412–422. [Google Scholar] [CrossRef]
- Dermawan, J.; Farver, C. The role of histologic grading and ki-67 index in predicting outcomes in pulmonary carcinoid tumors. Am. J. Surg. Pathol. 2020, 44, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Walts, A.E.; Ines, D.; Marchevsky, A.M. Limited role of ki-67 proliferative index in predicting overall short-term survival in patients with typical and atypical pulmonary carcinoid tumors. Mod. Pathol. 2012, 25, 1258–1264. [Google Scholar] [CrossRef]
- Childs, A.; Kirkwood, A.; Edeline, J.; Luong, T.V.; Watkins, J.; Lamarca, A.; Alrifai, D.; Nsiah-Sarbeng, P.; Gillmore, R.; Mayer, A.; et al. Ki-67 index and response to chemotherapy in patients with neuroendocrine tumours. Endocr. Relat. Cancers 2016, 23, 563–570. [Google Scholar] [CrossRef]
- Skov, B.G.; Holm, B.; Erreboe, A.; Skov, T.; Mellemgaard, A. ERCC1 and Ki67 in small cell lung carcinoma and other neuroendocrine tumors of the lung: Distribution and impact on survival. J. Thorac. Oncol. 2010, 5, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Grimaldi, F.; Muser, D.; Beltrami, C.A.; Machin, P.; Morelli, A.; Pizzolitto, S.; Talmassons, G.; Marciello, F.; Colao, A.A.L.; Monaco, R.; et al. Partitioning of bronchopulmonary carcinoids in two different prognostic categories by ki-67 score. Front. Endocrinol. 2011, 2, 20. [Google Scholar] [CrossRef]
- Rindi, G.; Klersy, C.; Inzani, F.; Fellegara, G.; Ampollini, L.; Ardizzoni, A.; Campanini, N.; Carbognani, P.; De Pas, T.M.; Galetta, D.; et al. Grading the neuroendocrine tumors of the lung: An evidence-based proposal. Endocr.-Relat. Cancer 2014, 21, 1–16. [Google Scholar] [CrossRef]
- Wirth, L.J.; Carter, M.R.; Jänne, P.A.; Johnson, B.E. Outcome of patients with pulmonary carcinoid tumors receiving chemotherapy or chemoradiotherapy. Lung Cancer 2004, 44, 213–220. [Google Scholar] [CrossRef]
- Pavel, M.E.; Hainsworth, J.D.; Baudin, E.; Peeters, M.; Hörsch, D.; Winkler, R.E.; Klimovsky, J.; Lebwohl, D.; Jehl, V.; Wolin, E.M.; et al. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): A randomised, placebo-controlled, phase 3 study. Lancet (Br. Ed.) 2011, 378, 2005–2012. [Google Scholar] [CrossRef]
- Lassen, U.; Kristjansen, P.E.G.; Østerlind, K.; Bergman, B.; Sigsgaard, T.C.; Hirsch, F.R.; Hansen, M.; Dombernowsky, P.; Hansen, H.H. Superiority of cisplatin or carboplatin in combination with teniposide and vincristine in the induction chemotherapy of small-cell lung cancer. A randomized trial with 5 years follow up. Ann. Oncol. 1996, 7, 365–372. [Google Scholar] [CrossRef]
- Catherine Pietanza, M.; Kadota, K.; Chan, T.A.; Rizvi, N.A.; Azzoli, C.G.; Riely, G.J.; Kris, M.G.; Krug, L.M.; Huberman, K.; Sima, C.S.; et al. Phase II trial of temozolomide in patients with relapsed sensitive or refractory small cell lung cancer, with assessment of methylguanine-DNA methyltransferase as a potential biomarker. Clin. Cancer Res. 2012, 18, 1138–1145. [Google Scholar] [CrossRef]
- Zauderer, M.G.; Drilon, A.; Kadota, K.; Huberman, K.; Sima, C.S.; Bergagnini, I.; Sumner, D.K.; Travis, W.D.; Heguy, A.; Ginsberg, M.S.; et al. Trial of a 5-day dosing regimen of temozolomide in patients with relapsed small cell lung cancers with assessment of methylguanine-DNA methyltransferase. Lung Cancer 2014, 86, 237–240. [Google Scholar] [CrossRef]
- Pelosi, G.; Sonzogni, A.; Harari, S.; Albini, A.; Bresaola, E.; Marchiò, C.; Massa, F.; Righi, L.; Gatti, G.; Papanikolaou, N.; et al. Classification of pulmonary neuroendocrine tumors: New insights. Transl. Lung Cancer Res. 2017, 6, 513–529. [Google Scholar] [CrossRef]
- Fernandez-Cuesta, L.; Peifer, M.; Lu, X.; Sun, R.; Ozretić, L.; Seidal, D.; Zander, T.; Leenders, F.; George, J.; Müller, C.; et al. Frequent mutations in chromatin-remodelling genes in pulmonary carcinoids. Nat. Commun. 2014, 5, 3518. [Google Scholar] [CrossRef]
- Simbolo, M.; Barbi, S.; Fassan, M.; Mafficini, A.; Ali, G.; Vicentini, C.; Sperandio, N.; Corbo, V.; Rusev, B.; Mastracci, L.; et al. Gene expression profiling of lung atypical carcinoids and large cell neuroendocrine carcinomas identifies three transcriptomic subtypes with specific genomic alterations. J. Thorac. Oncol. 2019, 14, 1651–1661. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Chung, Y.S.; Kim, K.A.; Shim, H.S. Genomic profiling and clinicopathological characteristics of neuroendocrine tumors of the lung in east asian patients. In Vivo 2020, 34, 3375–3385. [Google Scholar] [CrossRef]
- Rekhtman, N.; Desmeules, P.; Litvak, A.M.; Pietanza, M.C.; Santos-Zabala, M.L.; Ni, A.; Montecalvo, J.; Chang, J.C.; Beras, A.; Preeshagul, I.R.; et al. Stage IV lung carcinoids: Spectrum and evolution of proliferation rate, focusing on variants with elevated proliferation indices. Mod. Pathol. 2019, 32, 1106–1122. [Google Scholar] [CrossRef]
- Asiedu, M.K.; Thomas, J.; Charles, F.; Dong, J.; Schulte, S.C.; Khadka, P.; Sun, Z.; Kosari, F.; Jen, J.; Molina, J.; et al. Pathways impacted by genomic alterations in pulmonary carcinoid tumors. Clin. Cancer Res. 2018, 24, 1691–1704. [Google Scholar] [CrossRef]
- Alcala, N.; Leblay, N.; Gabriel, A.A.G.; Mangiante, L.; Hervas, D.; Giffon, T.; Sertier, A.S.; Ferrari, A.; Derks, J.; Ghantous, A.; et al. Integrative and comparative genomic analyses identify clinically relevant pulmonary carcinoid groups and unveil the supra-carcinoids. Nat. Commun. 2019, 10, 3407. [Google Scholar] [CrossRef]


{kind=link}
| Article1 | Type of Study | Study Analysis | TC and AC (n) | Nodal Status(n) | Survival Analysis | p Value | Study Conclusions |
|---|---|---|---|---|---|---|---|
|
Wegener [14] The role of adjuvant therapy for atypical bronchopulmonary carcinoids (2019) | Retrospective Review | Analysis of NCDB: patients with stage I-III atypical carcinoid treated surgically +/- adjuvant therapy | TC—N/A AC—67 | I/II-38 III-29 | Median survival:
| 0.89 | No benefit with adjuvant therapy |
|
Nussbaum [11] Defining the role of adjuvant chemotherapy after lobectomy for typical bronchopulmonary carcinoid tumors (2014) | Retrospective Review | Analysis of NCDB for patients who underwent lobectomy for typical carcinoid with metastatic disease treated with adjuvant chemotherapy | TC—37 AC—N/A | I/II/III-37 | Survival at 5 years:
| 0.042 | Use of adjuvant chemotherapy is associated with worse overall survival among both unadjusted and propensity matched groups with typical carcinoid that are nodal positive Propensity score matching showed inferior survival that was not statistically significant |
|
Anderson [12] Adjuvant Chemotherapy Does Not Confer Superior Survival in Patients with Atypical Carcinoid Tumors (2017) | Retrospective Review | Analysis of NCDB to determine whether a survival advantage exists in patients receiving chemotherapy for pN0 or pN+ atypical carcinoid tumors | TC—N/A AC–104 | pN0—15pN+—89 | Adjuvant Chemotherapy: 12 mo—98.9% 60 mo—47.9% Surgery alone: 12 mo—98.4%, 60 mo—67.1% | 0.46 | Use of adjuvant chemotherapy postoperatively in patients with pN+ and pN0 disease conferred no survival advantage |
|
Song [13] Long-term outcomes and prognostic factors of patients with surgically treated pulmonary atypical carcinoid tumors: our institutional experience with 68 patients (2018) | Retrospective Review | All patients with a diagnosis of primary pulmonary AC tumor treated from 1999 to 2013 were reviewed. | TC—N/A AC—31 | N/A | RFS and OS between those who received adjuvant chemotherapy after resection and those who had operation alone (p = 0.957 and p = 0.718, respectively | 0.957 and 0.718 | The use of adjuvant chemotherapy postoperatively in patients with pathologically lymph node-positive and pathologically lymph node-negative disease seems to have no survival advantage. |
|
Gosain [15] Role of Adjuvant Chemotherapy in Pulmonary Carcinoids: An NCDB Analysis (2019) | Retrospective Review | Using codes for TC and AC in the National Cancer Database (NCDB), all surgically resected cases from 2004–2014 were included to evaluate the need for adjuvant chemotherapy | 6673 cases were included: TC—88% AC—12% | N/A | TC patients did well with surgery alone in all Stages AC patients: Stage 1–5-year OS with S vs. S + CT: 84% and 52% Stage II—5 year OS with S vs. S + CT: 81% and 55% Stage III—5-year OS with S vs. S + CT: 46% vs. 54% | N/A | No benefit was seen from adjuvant chemotherapy in TCs. Adjuvant therapy may add benefit in stage III AC, the results were not statistically significant |
|
Huang [16] Assessment of the prognostic factors in patients with pulmonary carcinoid tumor: a population study (2018) | Retrospective Review | Cases of pulmonary carcinoid tumors were extracted from the Surveillance Epidemiology and End Results database. | N/A | N/A | N/A | N/A | Multivariate analyses showed that radiotherapy and chemotherapy were negative prognostic factors |
|
Tancredi [17] The Post-Surgical Long-Term Behaviour of Lung Carcinoid Tumours (2015) | Retrospective Review | Retrospective evaluation of long-term behaviour of lung carcinoids after surgery. A total of 23 patients (17 with typical pulmonary carcinoids and 6 with atypical pulmonary carcinoids) were enrolled in our hospital from April 1994 to July 2009 | TC-2 | N/A | N/A | N/A | There is no role for adjuvant and neoadjuvant chemotherapy in typical and atypical carcinoid |
|
Furqan [18] Lobar versus sub-lobar surgery for pulmonary typical carcinoid, a population-based Analysis (2018) | Retrospective Review | The Surveillance, Epidemiology, and End Results (SEER) Program was used to select patients ≥66 years old, and diagnosed between 2000 and 2012 with pulmonary TC. | N/A | N/A | N/A | N/A | Role of adjuvant CTX and XRT is unclear as these did not improve survival in this study The number of patients who received adjuvant CTX was small, we did not see survival advantage from it |
|
Chong [19] Chemotherapy and irradiation for locally advanced and metastatic pulmonary carcinoid tumors (2014) | Retrospective Review | Analysis of typical and atypical carcinoid tumors treated between 1990 and 2012 | 7—not specified | N/A | N/A | N/A | The small number of patients receiving adjuvant treatment and the long duration of follow-up needed in this disease makes it difficult to draw conclusions on the impact this approach has in the survival of patients with resected disease |
|
Forde [20] Systemic Therapy, Clinical Outcomes, and Overall Survival in Locally Advanced or Metastatic Pulmonary Carcinoid: A Brief Report (2014) | Retrospective Review | The Johns Hopkins Pathology Database was reviewed for APC patients treated between January 1992 and December 2012. Data on time to recurrence, progression-free survival, and overall survival were estimated by using the Kaplan–Meier method. | N/A | N/A | Response rate and PFS for each therapy were estimated using both radiology and clinical notes and thus reflect real-life practice; however, as a consequence have a degree of associated uncertainty. | N/A | Both TC and AC tumors demonstrate response to platinum/etoposide chemotherapy and we consider this to be a standard first-line option at our institution |
| Robelin [21] Characterization, Prognosis, and Treatment of Patients with Metastatic Lung Carcinoid Tumors (2019) | Retrospective Review | Retrospectively analyzed the medical records MLC patients treated at two tertiary referral centers in France (Gustave Roussy Institute—EURACAN center, and Hospices Civil de Lyon—ENETS center of excellence) from November 1995 to June 2017. | 108—type not specified | N/A | PFS
| N/A | Further studies are required to define the therapeutic strategy that would most benefit patients |
| NCCN | NANETS | ESMO | ENETS | |
|---|---|---|---|---|
| ADJUVANT THERAPY | Atypical: Observation or Cytotoxic Chemotherapy | No Recommendation | No Recommendation | Consider in AC with high proliferative index |
| GRADE OF EVIDENCE | 2B | N/A | N/A | Level IV |
| Boland [23] | ||||
| Median Ki-67 | Ki-67 Range | p-value (N/A) | ||
| Typical (n = 41) | 1.6 | 0–10.7 | ||
| Atypical (n = 14) | 4.3 | 1.2–12.2 | ||
| Marchió [24] | ||||
| Ki-67 < 4% (n = 147) | Ki-67 < 4–9% (n = 60) | Ki-67 ≥ 10% (n = 32) | p-value (0.02) | |
| Homogenous | 80 | 32 | 18 | |
| Heterogeneous | 13 | 8 | 11 | |
| Childs [29] | ||||
| Ki-67 ≤ 2% | Ki-67 3 ≤ 20% | Ki-67 > 20% | p-value (0.002) | |
| 18 | 80 | 75 | N = 173 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobash, P.T.; Ullah, A.; Karim, N.A. Survival Benefit of Adjuvant Chemotherapy in Pulmonary Carcinoid Tumors. Cancers 2022, 14, 4730. https://doi.org/10.3390/cancers14194730
Sobash PT, Ullah A, Karim NA. Survival Benefit of Adjuvant Chemotherapy in Pulmonary Carcinoid Tumors. Cancers. 2022; 14(19):4730. https://doi.org/10.3390/cancers14194730
Chicago/Turabian StyleSobash, Philip T., Asad Ullah, and Nagla Abdel Karim. 2022. "Survival Benefit of Adjuvant Chemotherapy in Pulmonary Carcinoid Tumors" Cancers 14, no. 19: 4730. https://doi.org/10.3390/cancers14194730
APA StyleSobash, P. T., Ullah, A., & Karim, N. A. (2022). Survival Benefit of Adjuvant Chemotherapy in Pulmonary Carcinoid Tumors. Cancers, 14(19), 4730. https://doi.org/10.3390/cancers14194730