
Remdesivir Decreases Mortality in COVID-19 Patients with Active Malignancy
 ,
,  , ,
, ,  , , , , , , , ,
, , , , , , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tian, Y.; Qiu, X.; Wang, C.; Zhao, J.; Jiang, X.; Niu, W.; Huang, J.; Zhang, F. Cancer associates with risk and severe events of COVID-19: A systematic review and meta-analysis. Int. J. Cancer 2021, 148, 363–374. [Google Scholar] [CrossRef] [PubMed]
- García-Suárez, J.; de la Cruz, J.; Cedillo, Á.; Llamas, P.; Duarte, R.; Jiménez-Yuste, V.; Hernández-Rivas, J.Á.; Gil-Manso, R.; Kwon, M.; Sánchez-Godoy, P.; et al. Impact of hematologic malignancy and type of cancer therapy on COVID-19 severity and mortality: Lessons from a large population-based registry study. J. Hematol. Oncol. 2020, 13, 133. [Google Scholar] [CrossRef] [PubMed]
- Saini, K.S.; Tagliamento, M.; Lambertini, M.; McNally, R.; Romano, M.; Leone, M.; Curigliano, G.; de Azambuja, E. Mortality in patients with cancer and coronavirus disease 2019: A systematic review and pooled analysis of 52 studies. Eur. J. Cancer 2020, 139, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Mulangu, S.; Dodd, L.E.; Davey, R.T., Jr.; Tshiani Mbaya, O.; Proschan, M.; Mukadi, D.; Lusakibanza Manzo, M.; Nzolo, D.; Tshomba Oloma, A.; Ibanda, A.; et al. A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics. N. Engl. J. Med. 2019, 381, 2293–2303. [Google Scholar] [CrossRef]
- Sheahan, T.P.; Sims, A.C.; Graham, R.L.; Menachery, V.D.; Gralinski, L.E.; Case, J.B.; Leist, S.R.; Pyrc, K.; Feng, J.Y.; Trantcheva, I.; et al. Broad-spectrum antiviral GS-5734 inhibits both epidemic and zoonotic coronaviruses. Sci. Transl. Med. 2017, 9, eaal3653. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dood, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Preliminary Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Goldman, J.D.; Lye, D.C.B.; Hui, D.S.; Marks, K.M.; Bruno, R.; Montejano, R.; Spinner, C.D.; Galli, M.; Ahn, M.Y.; Nahass, R.G.; et al. Remdesivir for 5 or 10 Days in Patients with Severe COVID-19. N. Engl. J. Med. 2020, 83, 1827–1837. [Google Scholar] [CrossRef]
- Flisiak, R.; Zarębska-Michaluk, D.; Berkan-Kawińska, A.; Tudrujek-Zdunek, M.; Rogalska, M.; Piekarska, A.; Kozielewicz, D.; Kłos, K.; Rorat, M.; Bolewska, B.; et al. Remdesivir-based therapy improved recovery of patients with COVID-19 in the SARSTer multicentre, real-world study. Pol. Arch. Intern. Med. 2021, 131, 103–110. [Google Scholar] [CrossRef]
- Pagliano, P.; Sellitto, C.; Scarpati, G.; Ascione, T.; Conti, V.; Franci, G.; Piazza, O.; Filippelli, A. An overview of the preclinical discovery and development of remdesivir for the treatment of coronavirus disease 2019 (COVID-19). Expert Opin. Drug Discov. 2021, 27, 1–10. [Google Scholar] [CrossRef]
- Okoli, G.N.; Rabbani, R.; Copstein, L.; Al-Juboori, A.; Askin, N.; Abou-Setta, A.M. Remdesivir for coronavirus disease 2019 (COVID-19): A systematic review with meta-analysis and trial sequential analysis of randomized controlled trials. Infect. Dis. 2021, 53, 691–699. [Google Scholar] [CrossRef]
- Gholamhoseini, M.T.; Yazdi-Feyzabadi, V.; Goudarzi, R.; Mehrolhassani, M.H. Safety and Efficacy of Remdesivir for the Treatment of COVID-19: A Systematic Review and Meta-Analysis. J. Pharm. Pharm. Sci. 2021, 24, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Khera, D.; Chugh, A.; Khera, P.S.; Chugh, V.K. Efficacy and safety of remdesivir in COVID-19 caused by SARS-CoV-2: A systematic review and meta-analysis. BMJ Open 2021, 11, e048416. [Google Scholar] [CrossRef] [PubMed]
- IDSA Guidelines on the Treatment and Management of Patients with COVID-19. Available online: https://www.idsociety.org/practice-guideline/covid-19-guideline-treatment-and-management/ (accessed on 7 March 2022).
- Helleberg, M.; Niemann, C.U.; Moestrup, K.S.; Kirk, O.; Lebech, A.M.; Lane, C.; Lundgren, J. Persistent COVID-19 in an Immunocompromised Patient Temporarily Responsive to Two Courses of Remdesivir Therapy. J. Infect. Dis. 2020, 222, 1103–1107. [Google Scholar] [CrossRef] [PubMed]
- Palomba, E.; Carrabba, M.; Zuglian, G.; Alagna, L.; Saltini, P.; Fortina, V.; Hu, C.; Bandera, A.; Fabio, G.; Gori, A.; et al. Treatment of SARS-CoV-2 relapse with remdesivir and neutralizing antibodies cocktail in a patient with X-linked agammaglobulinaemia. Int. J. Infect. Dis. 2021, 110, 338–340. [Google Scholar] [CrossRef]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Parczewski, M.; Piekarska, A.; Simon, K.; Tomasiewicz, K.; Zarębska-Michaluk, D. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of 31 March 2020. Pol. Arch. Intern. Med. 2020, 130, 352–357. [Google Scholar]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of 26 April 2021. Pol. Arch. Intern. Med. 2021, 131, 487–496. [Google Scholar] [CrossRef]
- Lee, L.Y.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Williams, M.; Mi, E.; Le Calvez, K.; Chen, J.; Pakzad-Shahabi, L.; Dadhania, S.; Wang, J.; Ho, A.; Rabinowicz, S. Estimating the Risk of Death from COVID-19 in Adult Cancer Patients. Clin. Oncol. 2021, 33, e172–e179. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Mamlouk, O.; Turin, A.; D’Achiardi, D.; Simbaqueba, C.; Dickson, K.; Franco-Vega, M.; Halm, J.; Mandayam, S. Clinical characteristics and outcomes of cancer patients with chronic kidney disease and coronavirus disease 2019. J. Clin. Oncol. 2021, 39, e18815. [Google Scholar] [CrossRef]
- Zarębska-Michaluk, D.; Jaroszewicz, J.; Rogalska, M.; Lorenc, B.; Rorat, M.; Szymanek-Pasternak, A.; Piekarska, A.; Berkan-Kawińska, A.; Sikorska, K.; Tudrujek-Zdunek, M.; et al. Impact of Kidney Failure on the Severity of COVID-19. J. Clin. Med. 2021, 10, 2042. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.W.; Cazier, J.B.; Starkey, T.; Briggs, S.E.W.; Arnold, R.; Bisht, V.; Booth, S.; Campton, N.A.; Cheng, V.W.T.; Collins, G.; et al. UK Coronavirus Cancer Monitoring Project Team. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: A prospective cohort study. Lancet Oncol. 2020, 21, 1309–1316. [Google Scholar] [CrossRef]
- Shah, V.; Ko Ko, T.; Zuckerman, M.; Vidler, J.; Sharif, S.; Mehra, V.; Gandhi, S.; Kuhnl, A.; Yallop, D.; Avenoso, D.; et al. Poor outcome and prolonged persistence of SARS-CoV-2 RNA in COVID-19 patients with haematological malignancies; King’s College Hospital experience. Br. J. Haematol. 2020, 190, e279–e282. [Google Scholar] [CrossRef]
- NCCN Best Practices Guidance: Management of COVID-19 Infection in Patients with Cancer. Available online: https://www.nccn.org/docs/default-source/covid-19/2021-covid-infectious-disease-management.pdf?sfvrsn=63f70c30_7 (accessed on 15 January 2022).
- Spinner, C.D.; Gottlieb, R.L.; Criner, G.J.; Arribas López, J.R.; Cattelan, A.M.; Soriano Viladomiu, A.; Ogbuagu, O.; Malhotra, P.; Mullane, K.M.; Castagna, A.; et al. Effect of Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients with Moderate COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1048–1057. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Poissy, J.; Belhadi, D.; Diallo, A.; Lê, M.P.; Peytavin, G.; Staub, T.; et al. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): A phase 3, randomised, controlled, open-label trial. Lancet Infect. Dis. 2021, 22, 209–221. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium; Pan, H.; Peto, R.; Henao-Restrepo, A.M.; Preziosi, M.P.; Sathiyamoorthy, V.; Abdool Karim, Q.; Alejandria, M.M.; Hernández García, C.; Kieny, M.P.; et al. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [PubMed]
- WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group; Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; et al. Association between administration of systemic corticosteroids and mortality among critically ill patients with COVID-19: A meta-analysis. JAMA 2020, 324, 1330–1341. [Google Scholar]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of dexamethasone on days alive and ventilator-free in patients with moderate or severe acute respiratory distress syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Nr with Data | All N = 222 | Died N = 59 | Survived N = 163 | p Value |
|---|---|---|---|---|---|
| Male sex, n (%) | 222 | 115 (51.8) | 39 (66.1) | 76 (46.6) | 0.0146 * |
| Age in years, median (IQR) | 222 | 70.0 (63.0–78.0) | 70 (63–81) | 70 (63–78) | 0.3105 * |
| BMI in kg/m2, median (IQR) | 175 | 26.5 (23.5–29.8) | 26.0 (23.9–31.0) | 26.5 (23.5–29.4) | 0.7718 ** |
| Hematological cancer, n (%) | 222 | 60 (27.0) | 12 (29.3) | 48 (29.4) | 0.2310 * |
| SpO2 in % at hospital admission, median (IQR) | 221 | 92 (85–95) | 84 (78–94) | 92 (88–95) | <0.0001 ** |
| CRP baseline [mg/dL], median (IQR) | 222 | 88.3 (26.2–134.7) | 96.5 (40.7–155) | 57.3 (22–113.3) | 0.0008 ** |
| Procalcitonin baseline [ng/mL], median (IQR) | 167 | 0.13 (0.05–0.37) | 0.27 (0.1–0.91) | 0.11 (0.05–0.3) | 0.0017 ** |
| WBC baseline [/μL], median (IQR) | 221 | 5500 (3700–9150) | 7840 (3970–12,860) | 5360 (3610–8060) | 0.1280 ** |
| Lymphocytes baseline [/μL], median (IQR) | 214 | 895 (590–1300) | 670 (490–950) | 990 (660–1350) | 0.0014 ** |
| Neutrocytes baseline [/μL], median (IQR) | 214 | 3855 (2290–6930) | 5190 (2380–10,460) | 3260 (2290–5690) | 0.0091 ** |
| PLT baseline [/μL], median (IQR) | 221 | 178,000 (127,000–255,000) | 164,000 (117,000–251,000) | 178,500 (134,000–255,000) | 0.5771 ** |
| IL-6 baseline [pg/mL], median (IQR) | 132 | 49.1 (22.8–116.8) | 139.7 (52.7–344.3) | 43.9 (17.4–90.5) | <0.0001 ** |
| D-dimers baseline [μg/mL], median (IQR) | 202 | 1228 (755–2290) | 1712 (1041–4152) | 1095 (699–1929) | 0.0025 ** |
| eGFR < 60 mL/min/m2 baseline, n (%) | 220 | 76 (34.5) | 31 (54.4) | 45 (27.6) | 0.0004 * |
| Use of other medication at baseline, n (%) | 219 | 188 (85.8) | 51 (87.9) | 137 (85.1) | 0.6666 * |
| Multimorbidity | 222 | 155 (69.8) | 112 (68.7) | 43 (72.9) | 0.6212 * |
| Use of RDV, n (%) | - | 58 (26.1) | 9 (15.5) | 49 (30.1) | 0.0370 * |
| Days from symptoms, median (IQR): | 66 | 6 (4–8) | 8 (6–9) | 6 (4–8) | 0.1279 ** |
| Days from diagnosis, median (IQR): | 68 | 2 (1–5) | 1.5 (1–5) | 2 (2–4.5) | 0.4186 ** |
| Days on RDV, median (IQR): | 68 | 5 (5–5) | 5 (4.5–5) | 5 (5–5) | 0.0047 ** |
| Use of TCZ, n (%) | - | 36 (16.2) | 13 (22.0) | 23 (14.1) | 0.2150 * |
| Days from symptoms, median (IQR): | 34 | 10 (8–13) | 9 (8–10) | 10 (7–14) | 0.7048 ** |
| Days from diagnosis, median (IQR): | 38 | 5 (2–9) | 4 (3–8) | 5 (2–10) | 0.9736 ** |
| Use of dexamethasone, n (%) | - | 110 (49.5) | 37 (62.7) | 73 (44.8) | 0.0226 * |
| Days from diagnosis, median (IQR): | 125 | 2 (1–5) | 1 (1–5) | 3 (1–5) | 0.1184 ** |
| Days on dexamethasone, median (IQR): | 123 | 9 (6–12) | 8 (3–12) | 9 (7–12) | 0.0233 ** |
| Use of convalescent plasma, n (%) | - | 43 (19.4) | 8 (13.6) | 35 (21.5) | 0.2488 * |
| Days from diagnosis, median (IQR): | 52 | 4 (2–8) | 3 (2–7) | 4 (2–8) | 0.9249 ** |
| Characteristic | Nr with Data | All N = 222 | Other N = 162 | Hematological N = 60 | p Value |
|---|---|---|---|---|---|
| Male sex, n (%) | 222 | 115 (51.8) | 90 (55.6) | 25 (41.7) | 0.0713 * |
| Age in years, median (IQR) | 222 | 70.0 (63.0–78.0) | 70 (64.0–79.0) | 69.0 (57.0–78.0) | 0.1550 ** |
| BMI in kg/m2, median (IQR) | 175 | 26.5 (23.5–29.8) | 27.7 (23.9–30.5) | 25.3 (23.0–28.6) | 0.0703 ** |
| SpO2 in % at hospital admission, median (IQR) | 221 | 92 (85–95) | 91 (85–95) | 92 (89–95) | 0.5531 ** |
| CRP baseline [mg/dL], median (IQR) | 222 | 88.3 (26.2–134.7) | 68.3 (24.0–133.0) | 58.3 (31.1–141.6) | 0.3484 |
| Procalcitonin baseline [ng/mL], median (IQR) | 167 | 0.13 (0.05–0.37) | 0.13 (0.05–0.31) | 0.13 (0.06–0.45) | 0.5876 ** |
| WBC baseline [/μL], median (IQR) | 221 | 5500 (3700–9150) | 6070 (3970–9250) | 4795 (2750–7685) | 0.0368 ** |
| Lymphocytes baseline [/μL], median (IQR) | 214 | 895 (590–1300) | 900 (640–1330) | 900 (390–1300) | 0.1504 ** |
| Neutrocytes baseline [/μL], median (IQR) | 214 | 3855 (2290–6930) | 4180 (2500–7300) | 2700 (1090–4360) | 0.0002 ** |
| PLT baseline [/μL], median (IQR) | 221 | 178,000 (127,000–255,000) | 192,000 (146,000–266,000) | 1042 (755–1741) | <0.0001 ** |
| IL–6 baseline [pg/mL], median (IQR) | 132 | 49.1 (22.8–116.8) | 50.1 (18.1–114.2) | 45.7 (28.8–107.2) | 0.4065 ** |
| D–dimers baseline [μg/mL], median (IQR) | 202 | 1228 (755–2290) | 1301 (743–2590) | 1042 (755–1742) | 0.3318 ** |
| eGFR < 60 mL/min/m2 baseline, n (%) | 220 | 76 (34.5) | 105 (65.6) | 39 (65.0) | 1.0000 * |
| Use of other medication at baseline, n (%) | 219 | 188 (85.8) | 134 (83.7) | 54 (91.5) | 0.1903 * |
| Multimorbidity | 222 | 155 (69.8) | 121 (74.7) | 34 (56.7) | 0.0132 * |
| Died, n (%) | 222 | 59 (26.6) | 47 (29.0) | 12 (20.0) | 0.2310 * |
| For patients receiving RDV, median(IQR): | – | 58 (26.1) | 39 (24.1) | 19 (31.7) | 0.3021 * |
| Days from symptoms, median(IQR): | 66 | 6 (4–8) | 7 (5–9) | 5 (3–8) | 0.0832 ** |
| Days from diagnosis, median(IQR): | 68 | 2 (1–5) | 2 (2–5) | 2 (1–5) | 0.2000 ** |
| Days on RDV, median(IQR): | 68 | 5 (5–5) | 5 (5–5) | 5 (5–5) | 0.1028 ** |
| Use of TCZ, n (%) | – | 36 (16.2) | 28 (17.3) | 8 (13.3) | 0.5441 * |
| Days from symptoms, median(IQR): | 34 | 10 (8–13) | 9 (5–12) | 12.5 (10–15) | 0.1147 ** |
| Days from diagnosis, median(IQR): | 38 | 5 (2–9) | 4 (2–7) | 4 (9.5–15) | 0.0425 ** |
| Use of dexamethasone, n (%) | – | 110 (49.5) | 77 (47.5) | 33 (55.0) | 0.3657 * |
| Days from diagnosis, median(IQR): | 125 | 2 (1–5) | 2 (1–5) | 3 (1–7) | 0.0423 ** |
| Days on dexamethasone, median(IQR): | 123 | 9 (6–12) | 9 (6–12) | 8 (6–10) | 0.7506 ** |
| Use of convalescent plasma, n (%) | – | 43 (19.4) | 23 (14.2) | 20 (33.3) | 0.0021 * |
| Days from diagnosis, median(IQR): | 52 | 4 (2–8) | 4 (2–7) | 6 (2–14) | 0.5002 ** |
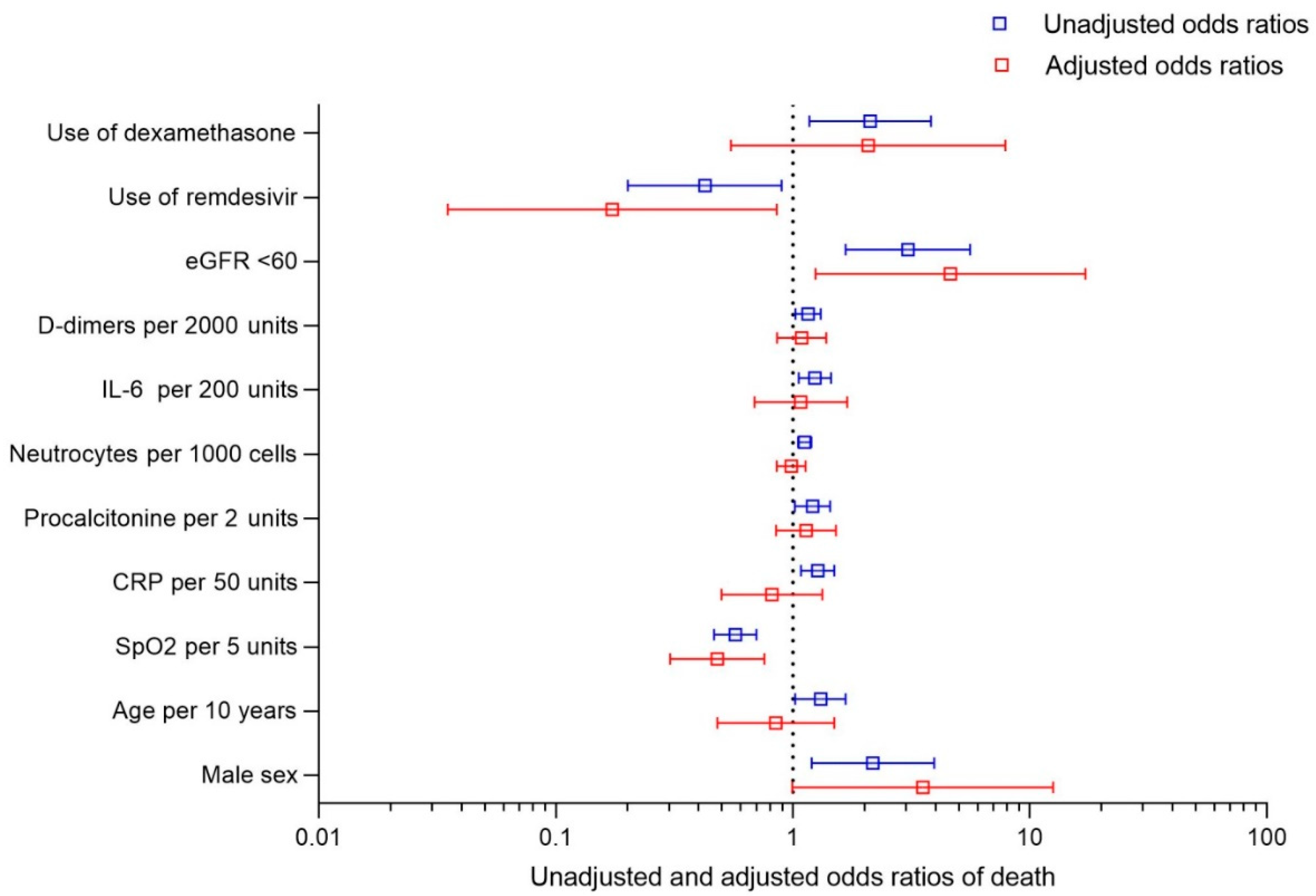
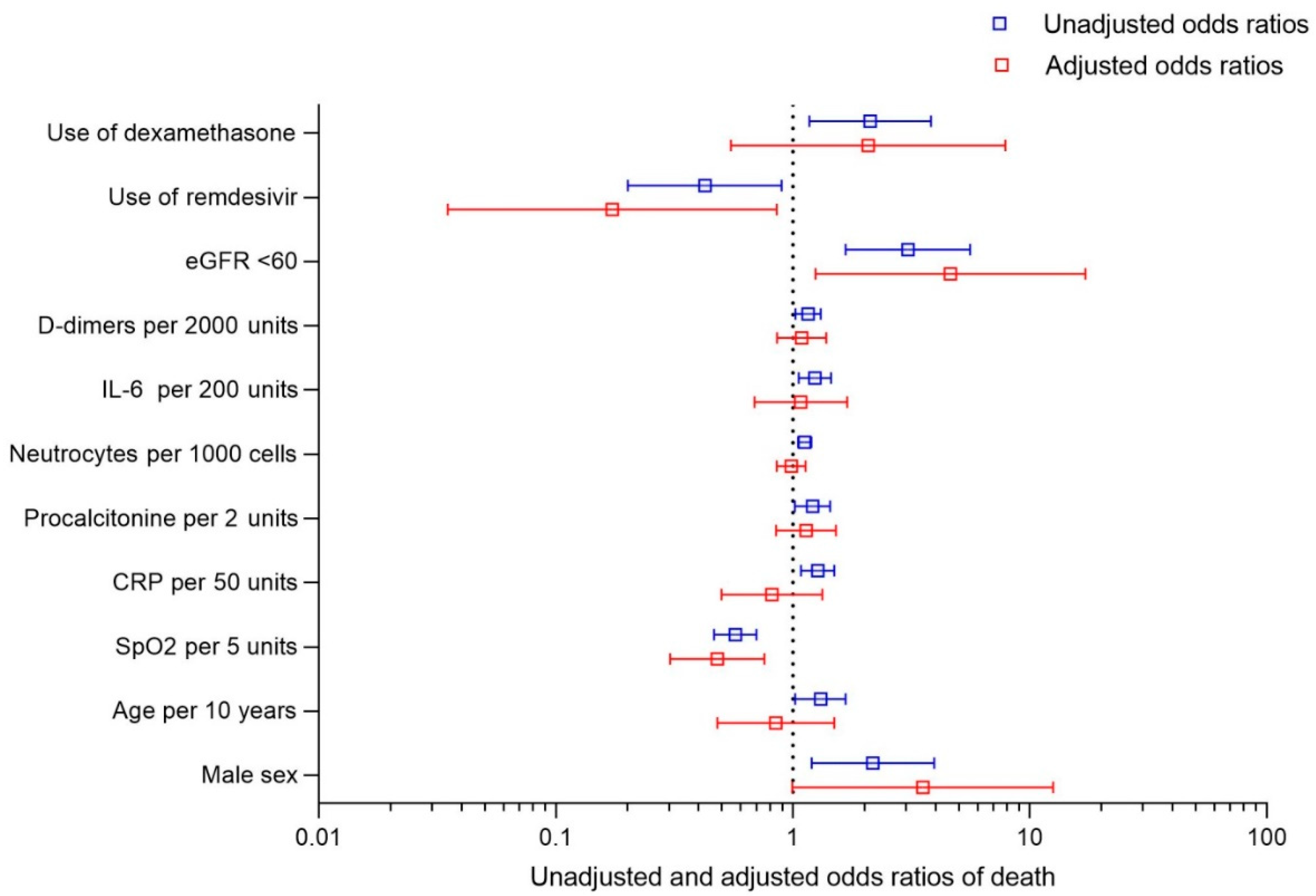
| Univariate | Multivariate * | |||
|---|---|---|---|---|
| Characteristic | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Male sex | 2.174 (1.200–3.939) | 0.0104 | 3.529 (0.994–12.53) | 0.0511 |
| Age per 10 years | 1.309(1.200–3.939) | 0.0330 | 0.847 (0.479–1.496) | 0.5667 |
| BMI per 1 unit | 1.008 (0.940–1.081) | 0.8261 | - | |
| SpO2 at hospital admission per 5 units [%] | 0.571 (0.465–0.701) | <0.0001 | 0.479 (0.303–0.758) | 0.0017 |
| CRP per 50 units [mg/dL] | 1.272 (1.082–1.496) | 0.0036 | 0.816 (0.500–1.331) | 0.4154 |
| Procalcitonin per 2 units [ng/mL] | 1.210 (1.019–1.435) | 0.0292 | 1.136 (0.850–1.518) | 0.3888 |
| WBC per 1000 units [/μL] | 1.026 (0.995–1.058) | 0.1012 | - | |
| Leukocytes per 100 units [/μL] | 0.994 (0.981–1.008) | 0.4278 | - | |
| Neutrocytes per 1000 units [/μL] | 1.120 (1.050–1.195) | 0.0006 | 0.983 (0.855–1.129) | 0.8045 |
| Platelets per 10,000 [/μL] | 0.994 (0.968–1.020) | 0.6315 | - | |
| IL-6 per 200 units [pg/mL] | 1.239 (1.059–1.450) | 0.0074 | 1.079 (0.688–1.693) | 0.7411 |
| D-dimers per 2000 units [μg/mL] | 1.159 (1.025–1.309) | 0.0185 | 1.088 (0.857–1.381) | 0.4866 |
| eGFR < 60 mL/min/m2 | 3.055 (1.671–5.584) | 0.0003 | 4.621 (1.244–17.17) | 0.0223 |
| Use of other medication | 1.509 (0.625–3.641) | 0.3604 | - | |
| Multimorbidity (CVD, COPD, Asthma, DM) | 1.234 (0.652–2.336) | 0.5188 | - | |
| Hematological cancer | 0.621 (0.306–1.261) | 0.1878 | - | |
| Use of remdesivir | 0.425 (0.201–0.895) | 0.0243 | 0.173 (0.035–0.855) | 0.0314 |
| Use of tocilizumab | 1.712 (0.812–3.611) | 0.1578 | - | |
| Use of dexamethasone | 2.121 (1.175–3.827) | 0.0125 | 2.077 (0.548–7.880) | 0.2824 |
| Use of convalescent plasma | 0.829 (0.394–1.744) | 0.6213 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaroszewicz, J.; Kowalska, J.; Pawłowska, M.; Rogalska, M.; Zarębska-Michaluk, D.; Rorat, M.; Lorenc, B.; Czupryna, P.; Sikorska, K.; Piekarska, A.; et al. Remdesivir Decreases Mortality in COVID-19 Patients with Active Malignancy. Cancers 2022, 14, 4720. https://doi.org/10.3390/cancers14194720
Jaroszewicz J, Kowalska J, Pawłowska M, Rogalska M, Zarębska-Michaluk D, Rorat M, Lorenc B, Czupryna P, Sikorska K, Piekarska A, et al. Remdesivir Decreases Mortality in COVID-19 Patients with Active Malignancy. Cancers. 2022; 14(19):4720. https://doi.org/10.3390/cancers14194720
Chicago/Turabian StyleJaroszewicz, Jerzy, Justyna Kowalska, Małgorzata Pawłowska, Magdalena Rogalska, Dorota Zarębska-Michaluk, Marta Rorat, Beata Lorenc, Piotr Czupryna, Katarzyna Sikorska, Anna Piekarska, and et al. 2022. "Remdesivir Decreases Mortality in COVID-19 Patients with Active Malignancy" Cancers 14, no. 19: 4720. https://doi.org/10.3390/cancers14194720
APA StyleJaroszewicz, J., Kowalska, J., Pawłowska, M., Rogalska, M., Zarębska-Michaluk, D., Rorat, M., Lorenc, B., Czupryna, P., Sikorska, K., Piekarska, A., Dworzańska, A., Zaleska, I., Mazur, W., Kozielewicz, D., Kłos, K., Podlasin, R., Angielski, G., Oczko-Grzesik, B., Figlerowicz, M., ... Tomasiewicz, K. (2022). Remdesivir Decreases Mortality in COVID-19 Patients with Active Malignancy. Cancers, 14(19), 4720. https://doi.org/10.3390/cancers14194720