
Diagnostic Outcomes and Treatment Modalities in Patients with Mycosis Fungoides in West Sweden—A Retrospective Register-Based Study

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
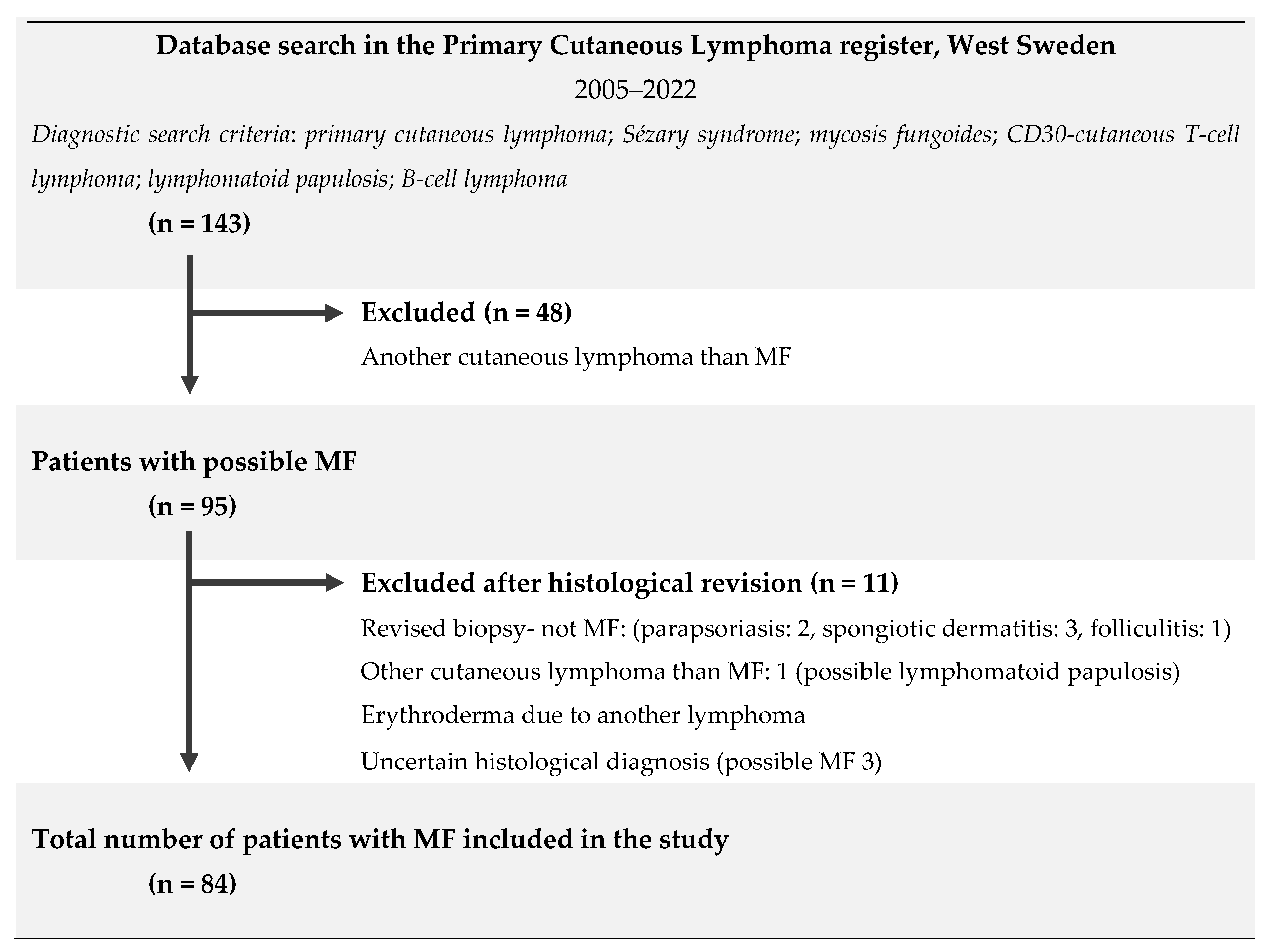
2. Materials and Methods
3. Results
3.1. Patient Demographics
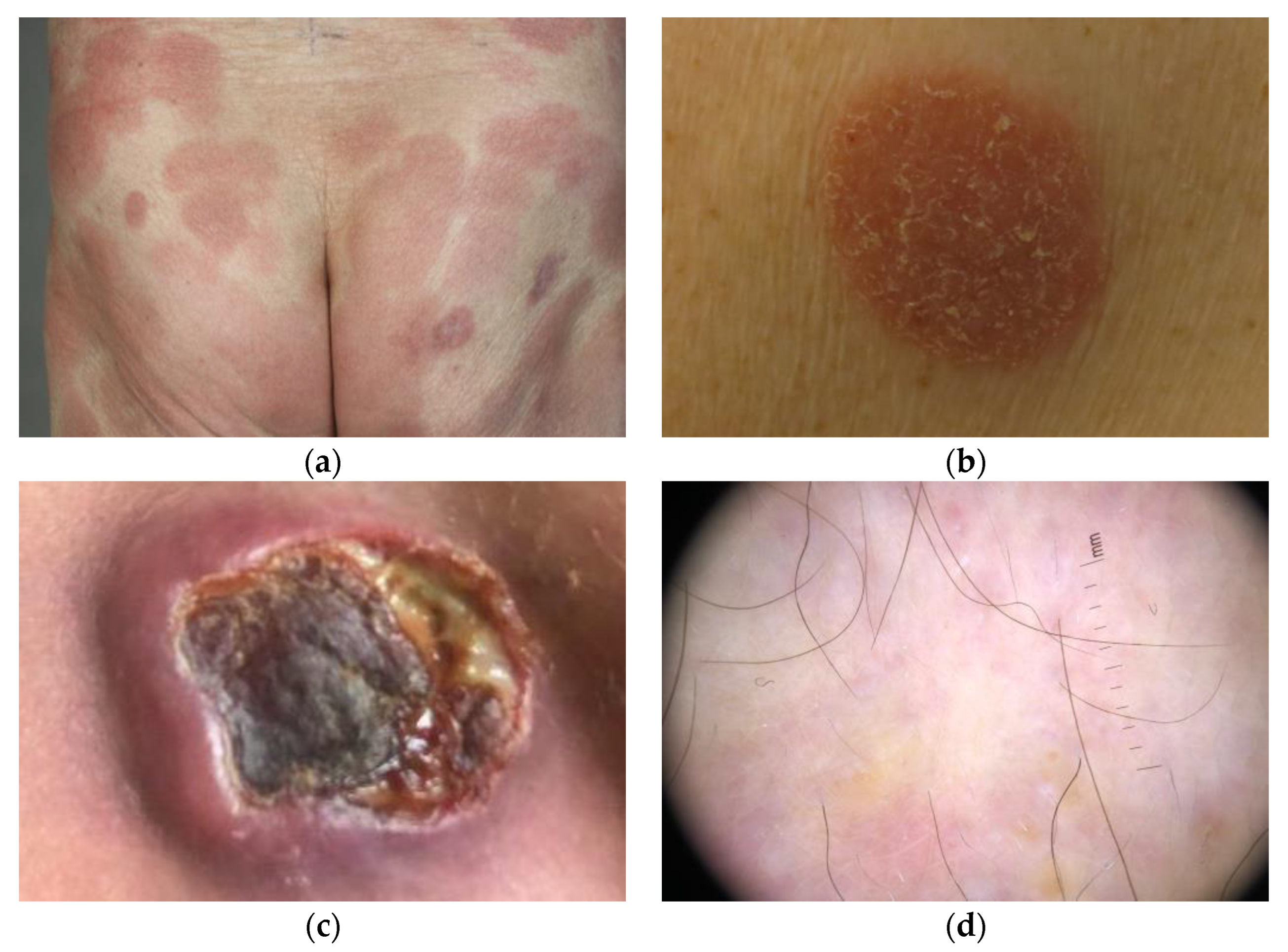
3.2. Clinical Characteristics at the Debut
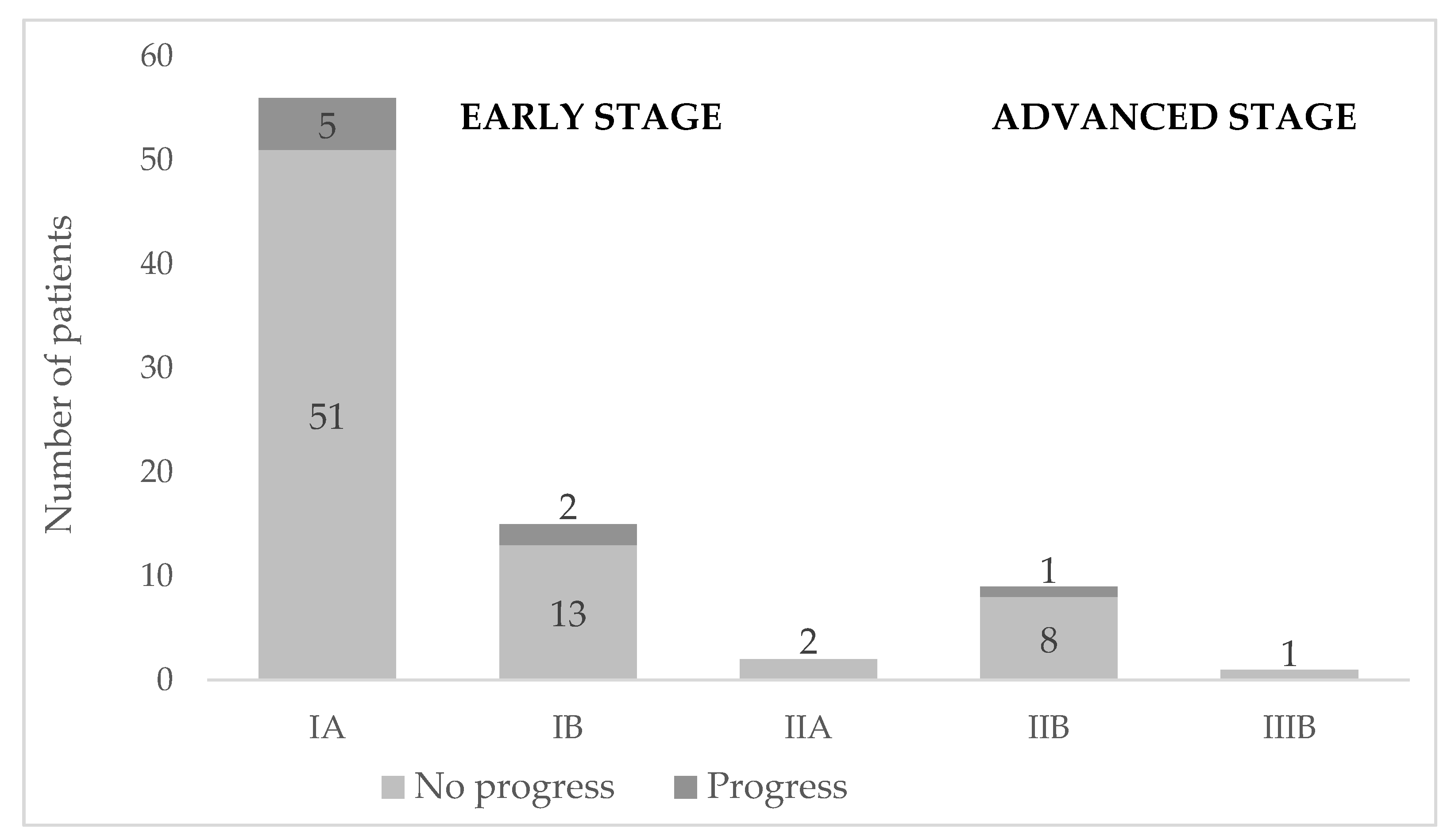
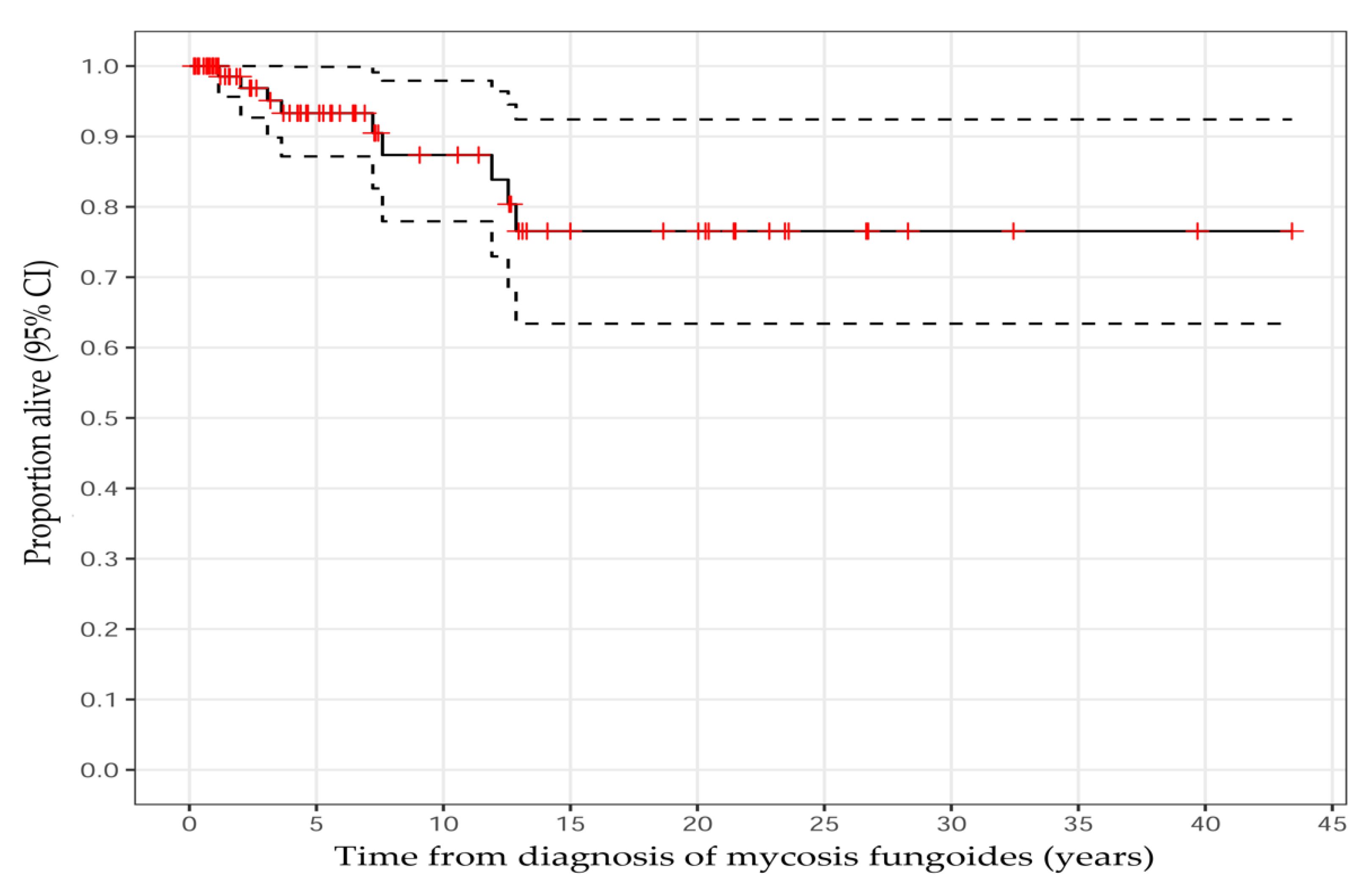
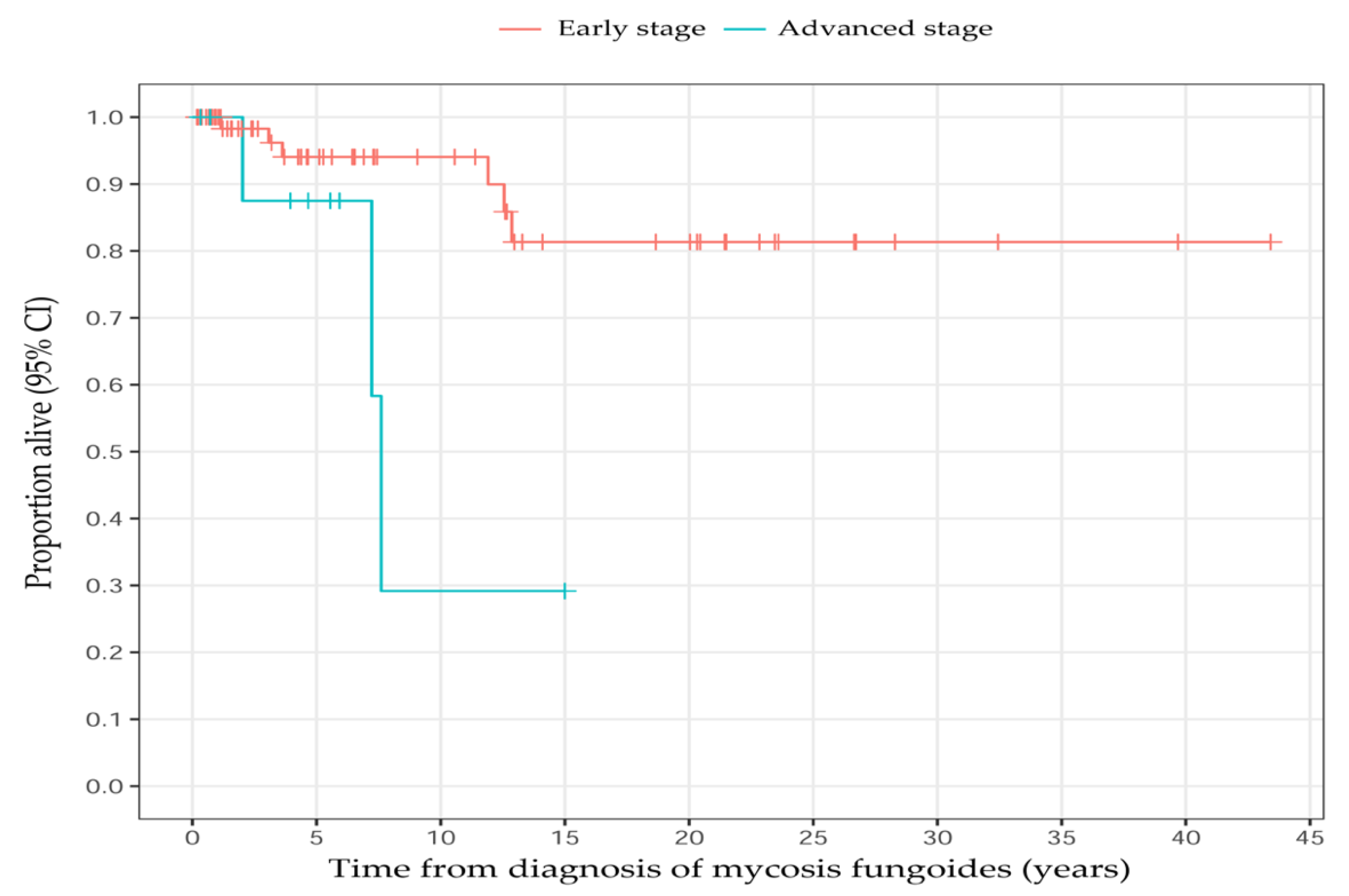
3.3. Staging and Disease Progression
3.4. Histopathological Findings
3.5. Immunohistochemical Findings
3.6. T-Cell Receptor Clonality Findings
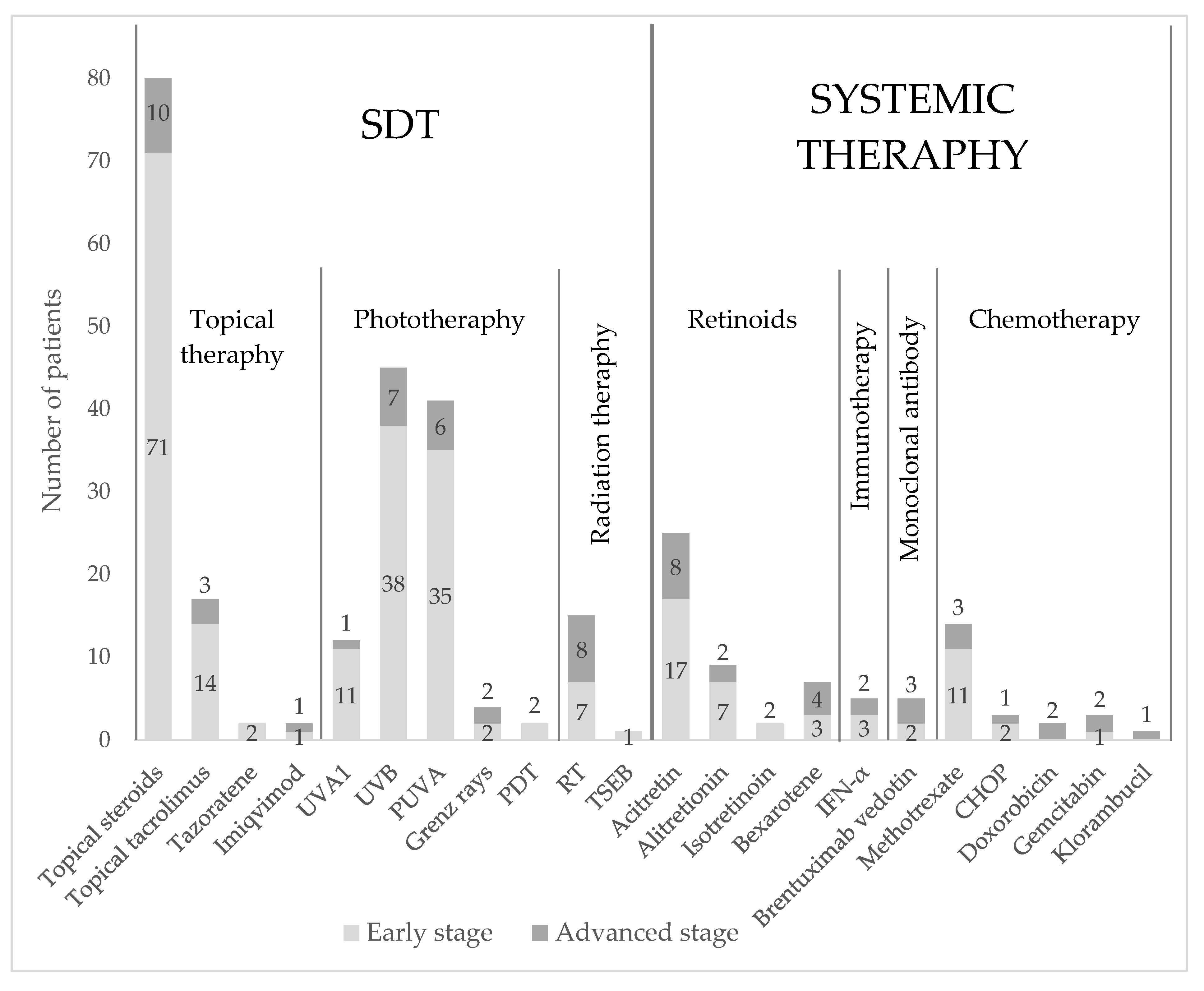
3.7. Treatment Modalities
3.7.1. Initial Treatment Outcome and Overall Response
- Early-stage disease at diagnosis
- Advanced-stage disease at diagnosis
3.7.2. Combination Therapies
4. Discussion
4.1. General Results
4.2. Demographic Factors
4.3. Immunohistochemical Findings
4.4. T-Cell Receptor Clonality Findings
4.5. Treatment Regimens
4.6. Treatment Response and Overall Response Rates
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Willemze, R.; Cerroni, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019, 133, 1703–1714. [Google Scholar] [CrossRef] [PubMed]
- Bradford, P.T.; Devesa, S.S.; Anderson, W.F.; Toro, J.R. Cutaneous lymphoma incidence patterns in the United States: A population-based study of 3884 cases. Blood 2009, 113, 5064–5073. [Google Scholar] [CrossRef] [PubMed]
- Korgavkar, K.; Xiong, M.; Weinstock, M. Changing incidence trends of cutaneous T-cell lymphoma. JAMA Dermatol. 2013, 149, 1295–1299. [Google Scholar] [CrossRef] [PubMed]
- Saunes, M.; Nilsen, T.I.; Johannesen, T.B. Incidence of primary cutaneous T-cell lymphoma in Norway. Br. J. Dermatol. 2009, 160, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Dobos, G.; de Masson, A.; Ram-Wolff, C.; Beylot-Barry, M.; Pham-Ledard, A.; Ortonne, N.; Ingen-Housz-Oro, S.; Battistella, M.; d’Incan, M.; Rouanet, J.; et al. Epidemiological changes in cutaneous lymphomas: An analysis of 8593 patients from the French Cutaneous Lymphoma Registry. Br. J. Dermatol. 2021, 184, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Assaf, C.; Dobos, G.; Zech, I.M.; Doess, A.; Hibbe, T.; Jadasz, J.J. Care structure of patients with mycosis fungoides and Sézary syndrome in Germany—Care research based on SHI claims data. J. Dtsch. Dermatol. Ges. 2022, 20, 643–651. [Google Scholar] [CrossRef]
- Girardi, M.; Heald, P.W.; Wilson, L.D. The pathogenesis of mycosis fungoides. N. Engl. J. Med. 2004, 350, 1978–1988. [Google Scholar] [CrossRef] [PubMed]
- Sławińska, M.; Sokołowska-Wojdyło, M.; Olszewska, B.; Nowicki, R.J.; Sobjanek, M.; Zalaudek, I. Dermoscopic and trichoscopic features of primary cutaneous lymphomas—Systematic review. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1470–1484. [Google Scholar] [CrossRef]
- Lallas, A.; Apalla, Z.; Lefaki, I.; Tzellos, T.; Karatolias, A.; Sotiriou, E.; Lazaridou, E.; Ioannides, D.; Zalaudek, I.; Argenziano, G. Dermoscopy of early stage mycosis fungoides. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Ghahramani, G.K.; Goetz, K.E.; Liu, V. Dermoscopic characterization of cutaneous lymphomas: A pilot survey. Int. J. Dermatol. 2018, 57, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Liu, J.; Wang, T.; Luo, Y.; Liu, Y. Dermoscopic patterns of early-stage mycosis fungoides in a Chinese population. Clin. Exp. Dermatol. 2019, 44, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, M.K.; Zindancı, I.; Zemheri, E. Dermoscopy of stage llA mycosis fungoides. North. Clin. Istanb. 2020, 7, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Jaffe, E.S.; Burg, G.; Cerroni, L.; Berti, E.; Swerdlow, S.H.; Ralfkiaer, E.; Chimenti, S.; Diaz-Perez, J.L.; Duncan, L.M.; et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005, 105, 3768–3785. [Google Scholar] [CrossRef] [PubMed]
- Jawed, S.I.; Myskowski, P.L.; Horwitz, S.; Moskowitz, A.; Querfeld, C. Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): Part I. Diagnosis: Clinical and histopathologic features and new molecular and biologic markers. J. Am. Acad. Dermatol. 2014, 70, 205.E1–205.E16. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Abbade, L.P.; Marques, M.E.; Marques, S.A. Mycosis fungoides and Sézary syndrome: Clinical, histopathological and immunohistochemical review and update. An. Bras. Dermatol. 2012, 87, 817–828. [Google Scholar] [CrossRef] [PubMed]
- Pimpinelli, N.; Olsen, E.A.; Santucci, M.; Vonderheid, E.; Haeffner, A.C.; Stevens, S.; Burg, G.; Cerroni, L.; Dreno, B.; Glusac, E.; et al. Defining early mycosis fungoides. J. Am. Acad. Dermatol. 2005, 53, 1053–1063. [Google Scholar] [CrossRef]
- Robson, A. Immunocytochemistry and the diagnosis of cutaneous lymphoma. Histopathology 2010, 56, 71–90. [Google Scholar] [CrossRef]
- Hodak, E.; David, M.; Maron, L.; Aviram, A.; Kaganovsky, E.; Feinmesser, M. CD4/CD8 double-negative epidermotropic cutaneous T-cell lymphoma: An immunohistochemical variant of mycosis fungoides. J. Am. Acad. Dermatol. 2006, 55, 276–284. [Google Scholar] [CrossRef]
- Bachelez, H.; Bioul, L.; Flageul, B.; Baccard, M.; Moulonguet-Michau, I.; Verola, O.; Morel, P.; Dubertret, L.; Sigaux, F. Detection of clonal T-cell receptor gamma gene rearrangements with the use of the polymerase chain reaction in cutaneous lesions of mycosis fungoides and Sézary syndrome. Arch. Dermatol. 1995, 131, 1027–1031. [Google Scholar] [CrossRef]
- Bakels, V.; van Oostveen, J.W.; van der Putte, S.C.; Meijer, C.J.; Willemze, R. Immunophenotyping and gene rearrangement analysis provide additional criteria to differentiate between cutaneous T-cell lymphomas and pseudo-T-cell lymphomas. Am. J. Pathol. 1997, 150, 1941–1949. [Google Scholar]
- Muche, J.M.; Lukowsky, A.; Asadullah, K.; Gellrich, S.; Sterry, W. Demonstration of frequent occurrence of clonal T cells in the peripheral blood of patients with primary cutaneous T-cell lymphoma. Blood 1997, 90, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Sproul, A.M.; Goodlad, J.R. Clonality testing of cutaneous lymphoid infiltrates: Practicalities, pitfalls and potential uses. J. Hematop. 2012, 5, 69–82. [Google Scholar] [CrossRef]
- Gilson, D.; Whittaker, S.J.; Child, F.J.; Scarisbrick, J.J.; Illidge, T.M.; Parry, E.J.; Mohd Mustapa, M.F.; Exton, L.S.; Kanfer, E.; Rezvani, K.; et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br. J. Dermatol. 2019, 180, 496–526. [Google Scholar] [CrossRef]
- Olsen, E.; Vonderheid, E.; Pimpinelli, N.; Willemze, R.; Kim, Y.; Knobler, R.; Zackheim, H.; Duvic, M.; Estrach, T.; Lamberg, S.; et al. Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: A proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood 2007, 110, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Nationellt Vårdprogram Hudlymfom. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/hudlymfom/vardprogram/ (accessed on 15 August 2022).
- Eklund, Y.; Aronsson, A.; Schmidtchen, A.; Relander, T. Mycosis Fungoides: A retrospective study of 44 Swedish cases. Acta Derm. Venereol. 2016, 96, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Gip, L.; Nilsson, E. Clustering of mycosis fungoides in the County of Västernorrland. Lakartidningen 1977, 74, 1174–1176. [Google Scholar] [PubMed]
- Nenonen, J.; Winther, A.H.; Leijonhufvud, E.; Belfrage, E.; Smedby, K.E.; Brauner, H. Overall survival and registration of cutaneous T-cell lymphoma patients in Sweden: A multi-center cohort and validation study. Acta Oncol. 2022, 61, 597–601. [Google Scholar] [CrossRef]
- Wilcox, R.A. Cutaneous T-cell lymphoma: 2017 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2017, 92, 1085–1102. [Google Scholar] [CrossRef]
- Olsen, E.A.; Whittaker, S.; Grazia Bernengo, M.; Ortiz-Romero, P.L.; Bagot, M.; Estrach, T.; Guitart, J.; Knobler, R.; Antonio Sanches, J.; Iwatsuki, K.; et al. Clinical end points and response criteria in Mycosis Fungoides and Sézary Syndrome: A consensus statement of the international society for Cutaneous Lymphomas, the United States Cutaneous Lymphoma Consortium, and the Cutaneous Lymphoma task force of the European Organisation for research and treatment of Cancer. J. Clin. Oncol. 2011, 29, 2598–2607. [Google Scholar] [CrossRef]
- Scarisbrick, J.J.; Morris, S. How big is your hand and should you use it to score skin in cutaneous T-cell lymphoma? Br. J. Dermatol. 2013, 169, 260–265. [Google Scholar] [CrossRef]
- Mirvish, J.J.; Pomerantz, R.G.; Falo, L.D., Jr.; Geskin, L.J. Role of infectious agents in cutaneous T-cell lymphoma: Facts and controversies. Clin. Dermatol. 2013, 31, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Panahi, Y.; Beiraghdar, F.; Amirhamzeh, A.; Poursaleh, Z.; Saadat, A.; Sahebkar, A. Environmental toxicant exposure and cancer: The role of epigenetic changes and protection by phytochemicals. Curr. Pharm. Des. 2016, 22, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Agar, N.S.; Wedgeworth, E.; Crichton, S.; Mitchell, T.J.; Cox, M.; Ferreira, S.; Robson, A.; Calonje, E.; Stefanato, C.M.; Wain, E.M.; et al. Survival outcomes and prognostic factors in Mycosis Fungoides/Sézary Syndrome: Validation of the Revised international society for Cutaneous Lymphomas/European Organisation for research and treatment of cancer staging proposal. J. Clin. Oncol. 2010, 28, 4730–4739. [Google Scholar] [CrossRef] [PubMed]
- Quaglino, P.; Pimpinelli, N.; Berti, E.; Calzavara-Pinton, P.; Alfonso Lombardo, G.; Rupoli, S.; Alaibac, M.; Bottoni, U.; Carbone, A.; Fava, P.; et al. Time course, clinical pathways, and long-term hazards risk trends of disease progression in patients with classic mycosis fungoides. Cancer 2012, 118, 5830–5839. [Google Scholar] [CrossRef]
- Nielsen, P.R.; Eriksen, J.O.; Wehkamp, U.; Lindahl, L.M.; Gniadecki, R.; Fogh, H.; Fabricius, S.; Bzorek, M.; Ødum, N.; Gjerdrum, L.M. Clinical and Histological Characteristics of Mycosis Fungoides and Sézary Syndrome: A Retrospective, Single-centre Study of 43 Patients from Eastern Denmark. Acta Derm. Venereol. 2019, 99, 1231–1236. [Google Scholar] [CrossRef]
- Eder, J.; Kern, A.; Moser, J.; Kitzwögerer, M.; Sedivy, R.; Trautinger, F. Frequency of primary cutaneous lymphoma variants in Austria: Retrospective data from a dermatology referral centre between 2006 and 2013. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1517–1523. [Google Scholar] [CrossRef]
- Chandra, P.; Oyarzo, M.P.; Jones, D. Cutaneous T-cell Lymphomas. In Neoplastic Hematopathology: Experimental and Clinical Approaches; Jones, D., Ed.; Humana Press: Totowa, NJ, USA, 2010; pp. 427–447. [Google Scholar] [CrossRef]
- Florell, S.R.; Cessna, M.; Lundell, R.B.; Boucher, K.M.; Bowen, G.M.; Harris, R.M.; Petersen, M.J.; Zone, J.J.; Tripp, S.; Perkins, S.L. Usefulness (or Lack Thereof) of Immunophenotyping in Atypical Cutaneous T-Cell Infiltrates. Am. J. Clin. Pathol. 2006, 125, 727–736. [Google Scholar] [CrossRef]
- Alberti-Violetti, S.; Talpur, R.; Schlichte, M.; Sui, D.; Duvic, M. Advanced-stage mycosis fungoides and Sézary syndrome: Survival and response to treatment. Clin. Lymphoma Myeloma Leuk. 2015, 15, e105–e112. [Google Scholar] [CrossRef]
- Xu, C.; Wan, C.; Wang, L.; Yang, H.-J.; Tang, Y.; Liu, W.-P. Diagnostic significance of TCR gene clonal rearrangement analysis in early mycosis fungoides. Chin. J. Cancer 2011, 30, 264. [Google Scholar] [CrossRef]
- Alessi, E.; Coggi, A.; Venegoni, L.; Merlo, V.; Gianotti, R. The usefulness of clonality for the detection of cases clinically and/or histopathologically not recognized as cutaneous T-cell lymphoma. Br. J. Dermatol. 2005, 153, 368–371. [Google Scholar] [CrossRef]
- Ponte, P.; Serrão, V.; Apetato, M. Efficacy of narrowband UVB vs. PUVA in patients with early-stage mycosis fungoides. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.M.D.; Zug, K.A.M.D. Phototherapy for cutaneous T-cell lymphoma: Online survey and literature review. J. Am. Acad. Dermatol. 2008, 60, 39–50. [Google Scholar] [CrossRef]
- Zackheim, H.S. Treatment of patch-stage mycosis fungoides with topical corticosteroids. Dermatol. Ther. 2003, 16, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Goekdemir, G.; Barutcuoglu, B.; Sakiz, D.; Koeslue, A. Narrowband UVB phototherapy for early-stage mycosis fungoides: Evaluation of clinical and histopathological changes. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J.J.; Roenigk, H.H.; Hurria, A.; Kuzel, T.M.; Samuelson, E.; Rademaker, A.W.; Rosen, S.T. Treatment of mycosis fungoides with photochemotherapy (PUVA): Long-term follow-up. J. Am. Acad. Dermatol. 1995, 33, 234–242. [Google Scholar] [CrossRef]
- Trautinger, F.; Eder, J.; Assaf, C.; Bagot, M.; Cozzio, A.; Dummer, R.; Gniadecki, R.; Klemke, C.-D.; Ortiz-Romero, P.L.; Papadavid, E.; et al. European Organisation for Research and Treatment of Cancer consensus recommendations for the treatment of mycosis fungoides/Sézary syndrome—Update 2017. Eur. J. Cancer 2017, 77, 57–74. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Values |
|---|---|
| Age at time of diagnosis, years, median (range) | 55.4 (8.6–91.8) |
| Mean ± SD | 52.4 ± 20.5 |
| Sex (male/female), n (%) | |
| Male | 54 (64.3) |
| Female | 29 (33.5) |
| Time from onset of skin symptoms to initial diagnosis, years, median (range) | 3.3 (0.2–45.6) |
| Time from referral to first visit at the clinic, days, median (range) | 32 (0–338) |
| Diagnosis received after first visit at dermatology clinic, n (%) | |
| Yes | 61 (73.5) |
| No | 22 (26.5) |
| No data | 1 (1.2) |
| Clinical features, debut, n (%) | |
| Papule | 19 (22.6) |
| Macule | 15(17.9) |
| Patch | 54 (64.3) |
| Plaque | 33 (39.2) |
| Nodule | 1 (1.2) |
| Tumor | 7 (8.3) |
| Poikiloderma | 1 (1.2) |
| Hypopigmentation | 5 (5.9) |
| Hyperpigmentation | 5 (5.9) |
| Erythroderma | 3 (3.6) |
| Body area of skin disease, debut, n (%) | |
| Head | 16 (19) |
| Face | 12 (14.3) |
| Scalp | 4 (4.8) |
| Trunk | 41 (48.8) |
| Sun-exposed | 26 (31) |
| Unexposed to the sun | 21 (25) |
| Upper extremity | 53 (63) |
| Sun-exposed | 28 (33) |
| Unexposed to the sun | 32 (33) |
| Lower extremity | 58 (69) |
| Sun-exposed | 26 (31) |
| Unexposed to the sun | 41 (48.8) |
| Percentage of skin area involved at time of diagnosis, n (%) | |
| <10% | 63 (75) |
| ≥10% | 21 (25) |
| m-SWAT at time of diagnosis, median (range) | 4 (0–156) |
| Mean ± SD | 14.1 ± 29.8 |
| Clinical stage at time of diagnosis, n (%) | |
| IA | 56 (67.5) |
| IB | 15 (18.1) |
| IIA | 2 (2.4) |
| IIB | 9 (10.8) |
| IIIA | 0 |
| IIIB | 1 (1.2) |
| IVA1 | 0 |
| IVA2 | 0 |
| IVB | 0 |
| No data | 1 (1.2) |
| Staging, n (%) | |
| Early (IA–IIA) | 73 (88) |
| Advanced (IIB–IVB) | 10 (12) |
| Types, n (%) | |
| Classic MF | 63 (75) |
| Folliculotropic MF | 9 (10.7) |
| Syringotropic MF | 4 (4.8) |
| Hypopigmented MF | 1 (1.2) |
| CD30-positive transformation | 7 (8.3) |
| Skin type according to Fitzpatrick, n (%) | |
| I | 3 (3.75) |
| II | 55 (68.8) |
| III | 20 (25) |
| IV | 2 (2.5) |
| No data | 4 (5) |
| Remission at last appointment, n (%) | 14 (16.7) |
| Deceased patients, n (%) | |
| MF-related death | 4 (4.8) |
| Other causes of death | 4 (4.8) |
| No data | 1 (1.2) |
| Skin Cancers | Total |
|---|---|
| Basal cell carcinoma | 14 |
| Squamous cell carcinoma in situ | 4 |
| Squamous cell carcinoma | 3 |
| Melanoma in situ | 2 |
| Lentigo maligna | 1 |
| Lentigo malignant melanoma | 1 |
| Malignant melanoma | 2 |
| Merkel cell carcinoma | 1 |
| Hematological malignancies | Total |
| Anaplastic large-cell lymphoma | 1 |
| Chronic lymphocytic leukemia | 1 |
| Chronic myelomonocytic leukemia | 1 |
| Diffuse large B-cell lymphoma | 1 |
| Epstein–Barr virus–positive diffuse large B-cell lymphoma) | 2 |
| Follicular lymphoma | 1 |
| Hodgkin lymphoma | 1 |
| Marginal zone lymphoma | 1 |
| Solid tumors | Total |
| Prostate cancer | 4 |
| Breast cancer | 3 |
| Esophagus cancer | 1 |
| Endometrial cancer | 1 |
| Urinary bladder cancer | 1 |
| Colon cancer | 1 |
| Rectal cancer | 1 |
| Myxofibrosarcoma | 1 |
| Characteristics | Values |
|---|---|
| Histopathological characteristics, n (%) | |
| Epidermotropism | |
| Yes | 55 (69.6) |
| No | 19 (24) |
| uncertain | 3 (3.8) |
| Atypical lymphocytes | |
| Yes | 67 (84.8) |
| No | 9 (11.4) |
| uncertain | 2 (2.5) |
| TCR clonality, n (%) | |
| Monoclonal | 63 (75) |
| Gamma | 60 (71.4) |
| Beta | 49 (58) |
| Immunohistochemistry, n (%) | |
| CD2+ | 13 (16.7) |
| CD3+ | 65 (83.3) |
| CD4+ | 68 (87.2) |
| CD5+ | 20 (25.6) |
| CD7+ | 9 (11.5) |
| CD8− | 13 (16.7) |
| CD8+ | 51 (65.4) |
| CD20− | 6 (7.7) |
| CD20+ | 24 (30.8) |
| CD30− | 14 (17.9) |
| CD30+ | 26 (33.) |
| CD45+ | 4 (5.1) |
| SDT Treatments | CR | PR | SD | PD | ORR | NA | Patients | |
|---|---|---|---|---|---|---|---|---|
| Topical therapy | ||||||||
| Topical steroids | 6 | 26 | 29 | 11 | 32 | (44%) | 12 | 72 |
| Early stage | 6 | 23 | 25 | 7 | 29 | (47%) | 12 | 62 |
| Advanced stage | - | 3 | 3 | 4 | 3 | (30%) | - | 10 |
| Topical tacrolimus | - | 4 | 7 | 1 | 4 | (33%) | 5 | 12 |
| Early stage | - | 4 | 5 | 1 | 4 | (40%) | 4 | 10 |
| Advanced stage | - | - | 2 | - | - | 1 | 2 | |
| Tazarotene | - | - | 2 | - | - | - | 2 | |
| Early stage | - | - | 2 | - | - | - | 2 | |
| Advanced stage | - | - | - | - | - | - | - | |
| Imiquimod | - | 1 | 1 | - | 1 | (50%) | - | 2 |
| Early stage | - | 1 | - | - | 1 | (100%) | - | 1 |
| Advanced stage | - | - | 1 | - | - | - | 1 | |
| Phototherapy | ||||||||
| UVA1 | 2 | 7 | 2 | - | 9 | (75%) | 1 | 12 |
| Early stage | 2 | 7 | 1 | - | 9 | (82%) | 1 | 11 |
| Advanced stage | - | - | 1 | - | - | - | - | 1 |
| UVB | 4 | 15 | 10 | 7 | 19 | (51%) | 8 | 37 |
| Early stage | 4 | 13 | 10 | 4 | 17 | (57%) | 7 | 30 |
| Advanced stage | - | 3 | - | 3 | 3 | (43%) | 1 | 7 |
| PUVA | 17 | 17 | 2 | 2 | 34 | (89%) | 3 | 38 |
| Early stage | 17 | 10 | 2 | 2 | 27 | (84%) | 3 | 32 |
| Advanced stage | - | 6 | - | - | 6 | (100%) | - | 6 |
| Grenz rays | 1 | 1 | 1 | 1 | 2 | (50%) | - | 4 |
| Early stage | 1 | - | - | 1 | 1 | (50%) | - | 2 |
| Advanced stage | - | 1 | 1 | - | 1 | (50%) | - | 2 |
| PDT | - | 1 | 1 | - | 1 | (50%) | - | 2 |
| Early stage | - | 1 | 1 | - | 1 | (50%) | - | 2 |
| Advanced stage | - | - | - | - | - | - | - | |
| Radiation therapy | ||||||||
| RT | 7 | 3 | 3 | - | 10 | 1 | 13 | |
| Early stage | 4 | 1 | 1 | - | 5 | (83%) | 1 | 6 |
| Advanced stage | 3 | 2 | 2 | - | 5 | (71%) | - | 7 |
| TSEB | - | 1 | - | - | 1 | (100%) | - | 1 |
| Early stage | - | 1 | - | - | 1 | (100%) | - | 1 |
| Advanced stage | - | - | - | - | - | - | - | |
| Systemic Treatments | CR | PR | SD | PD | ORR | NA | Patients | |
|---|---|---|---|---|---|---|---|---|
| Retinoids | ||||||||
| Acitretin | 1 | 10 | 6 | 6 | 11 | (48%) | 3 | 23 |
| Early stage | 1 | 6 | 5 | 3 | 7 | (47%) | 3 | 15 |
| Advanced stage | - | 4 | 1 | 3 | 4 | (50%) | - | 8 |
| Alitretinoin | - | 2 | - | 1 | 2 | (67%) | 6 | 3 |
| Early stage | - | 1 | - | - | 1 | (100%) | 6 | 1 |
| Advanced stage | - | 1 | - | 1 | 1 | (50%) | - | 2 |
| Isotretinoin | - | 2 | - | - | 2 | (100%) | - | 2 |
| Early stage | - | 2 | - | - | 2 | (100%) | - | 2 |
| Advanced stage | - | - | - | - | - | - | - | - |
| Bexarotene | - | - | 1 | 3 | - | - | 3 | 4 |
| Early stage | - | - | - | 3 | - | - | - | 3 |
| Advanced stage | - | - | 1 | - | - | - | 3 | 1 |
| Immunotherapy | ||||||||
| IFN-α | - | - | 1 | 3 | - | - | 1 | 4 |
| Early stage | - | - | - | 2 | - | - | 1 | 2 |
| Advanced stage | - | - | 1 | 1 | - | - | - | 2 |
| Monoclonal antibody | ||||||||
| Brentuximab vedotin | - | 2 | 1 | - | 2 | (67%) | 1 | 3 |
| Early stage | - | 1 | - | - | 1 | (100%) | 1 | 1 |
| Advanced stage | - | 1 | 1 | - | 1 | (50%) | - | 2 |
| Chemotherapy | ||||||||
| Methotrexate | - | 3 | 6 | 4 | 3 | (23%) | 1 | 13 |
| Early stage | - | 2 | 5 | 2 | 2 | (20%) | 1 | 10 |
| Advanced stage | - | - | 2 | 2 | - | - | - | 3 |
| Doxorubicin | - | - | 1 | 1 | - | - | - | 2 |
| Early stage | - | - | - | - | - | - | - | - |
| Advanced stage | - | - | 1 | 1 | - | - | - | 2 |
| Gemcitabin | - | - | 1 | 2 | - | - | - | 3 |
| Early stage | - | - | 1 | - | - | - | - | 1 |
| Advanced stage | - | - | - | 2 | - | - | - | 2 |
| Chlorambucil | - | 1 | - | - | 1 | (100%) | - | 1 |
| Early stage | - | - | - | - | - | - | - | - |
| Advanced stage | - | 1 | - | - | 1 | (100%) | - | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wojewoda, K.; Gillstedt, M.; Englund, H.; Ali, S.; Lewerin, C.; Osmancevic, A. Diagnostic Outcomes and Treatment Modalities in Patients with Mycosis Fungoides in West Sweden—A Retrospective Register-Based Study. Cancers 2022, 14, 4661. https://doi.org/10.3390/cancers14194661
Wojewoda K, Gillstedt M, Englund H, Ali S, Lewerin C, Osmancevic A. Diagnostic Outcomes and Treatment Modalities in Patients with Mycosis Fungoides in West Sweden—A Retrospective Register-Based Study. Cancers. 2022; 14(19):4661. https://doi.org/10.3390/cancers14194661
Chicago/Turabian StyleWojewoda, Karolina, Martin Gillstedt, Hanna Englund, Shada Ali, Catharina Lewerin, and Amra Osmancevic. 2022. "Diagnostic Outcomes and Treatment Modalities in Patients with Mycosis Fungoides in West Sweden—A Retrospective Register-Based Study" Cancers 14, no. 19: 4661. https://doi.org/10.3390/cancers14194661
APA StyleWojewoda, K., Gillstedt, M., Englund, H., Ali, S., Lewerin, C., & Osmancevic, A. (2022). Diagnostic Outcomes and Treatment Modalities in Patients with Mycosis Fungoides in West Sweden—A Retrospective Register-Based Study. Cancers, 14(19), 4661. https://doi.org/10.3390/cancers14194661