
Clinical Presentation and Prognostic Features in Patients with Immunotherapy-Induced Vitiligo-like Depigmentation: A Monocentric Prospective Observational Study

 , , , , and
, , , , and 
Abstract
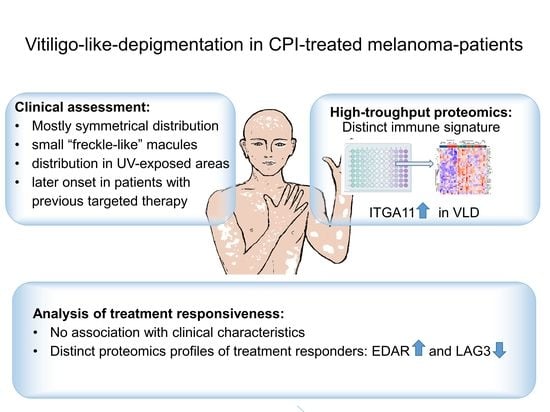
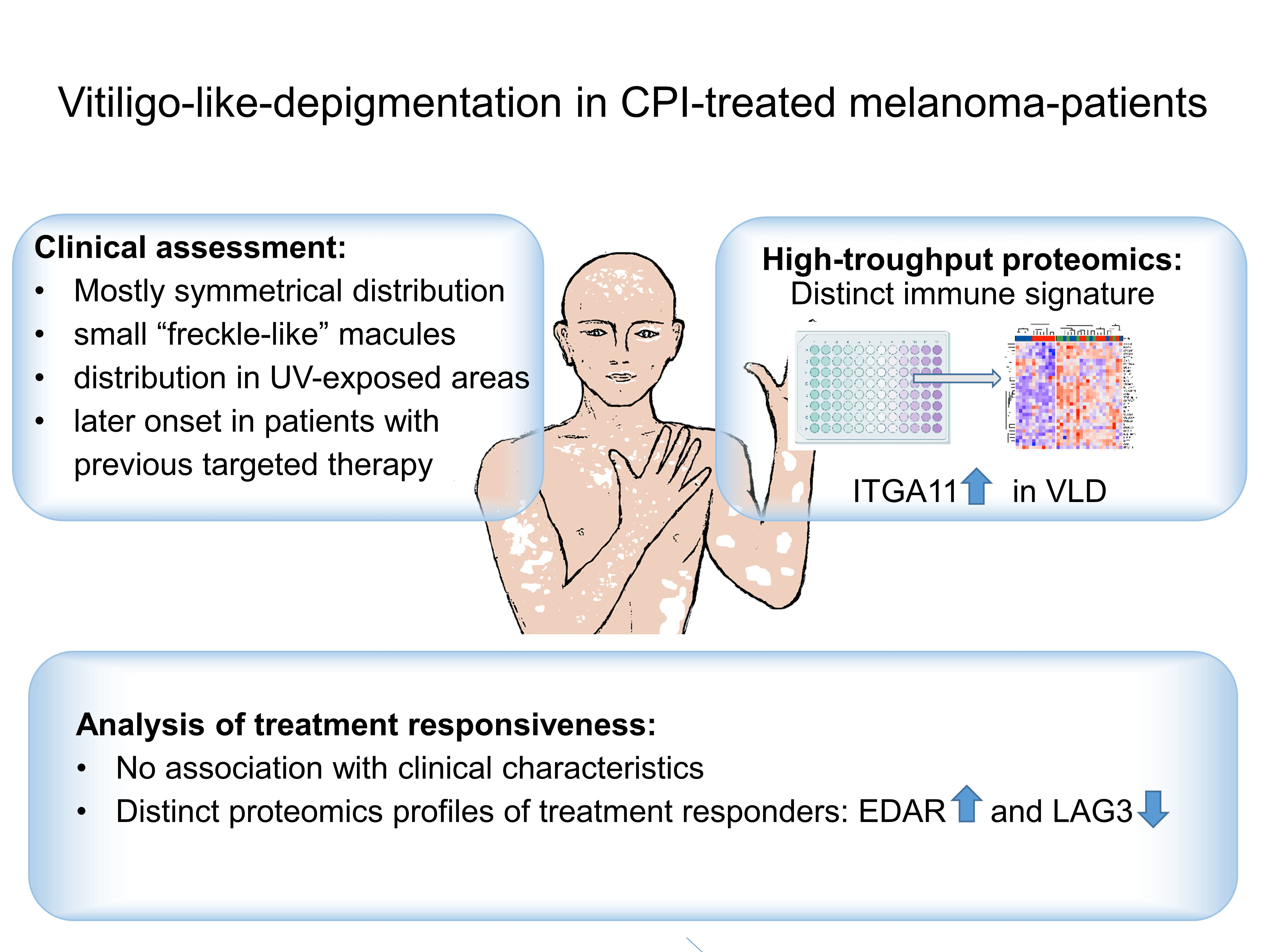
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Skin Assessments
2.2. OLINK High-Throughput Proteomics
2.3. Histopathological Examination, Immunohistochemistry Staining
2.4. Data Analysis and Statistics
3. Results
3.1. Demographics and Patient Characteristics
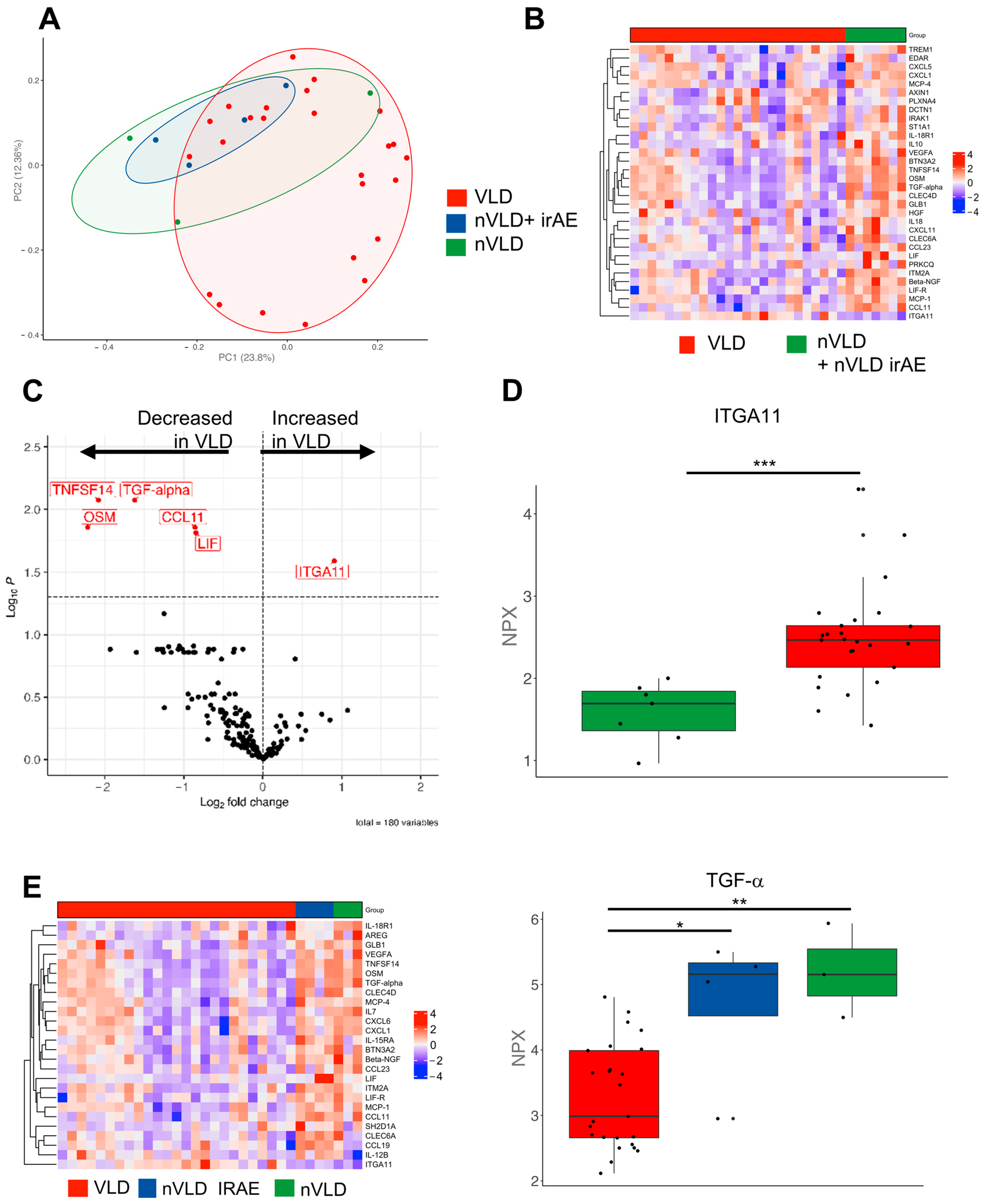
3.2. The Distinct Molecular Signature of VLD
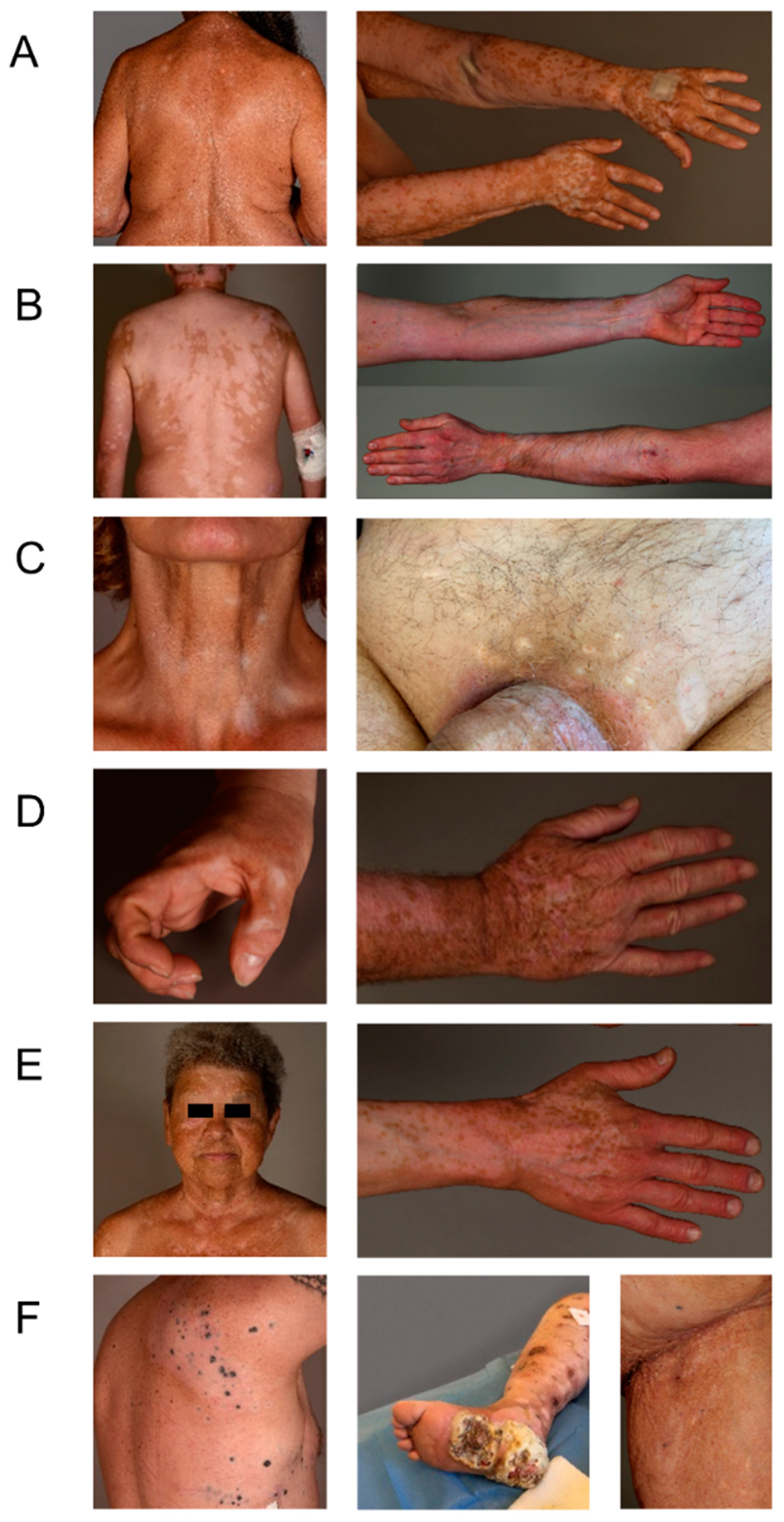
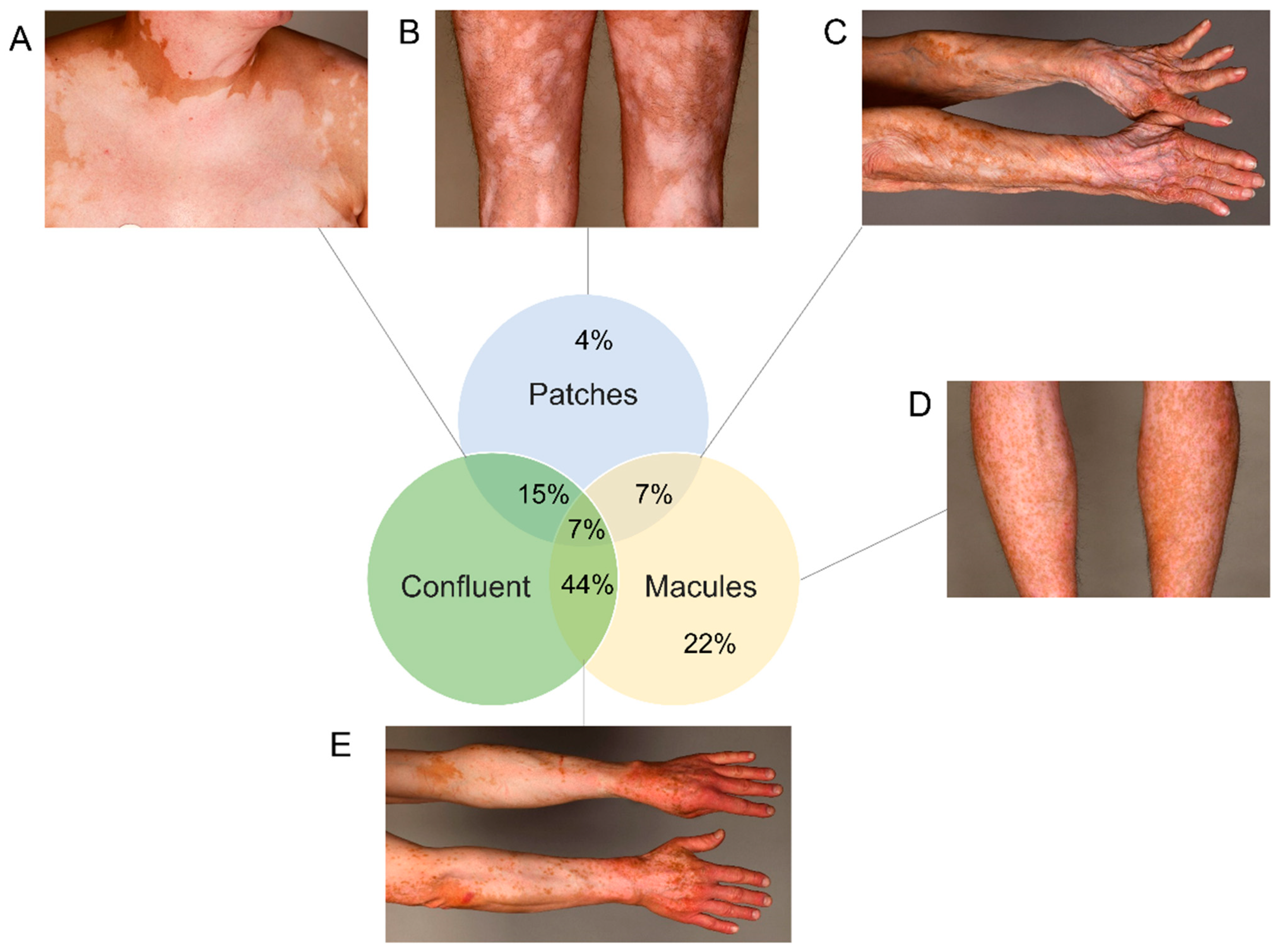
3.3. Clinical and Histopathological Characterization of VLD
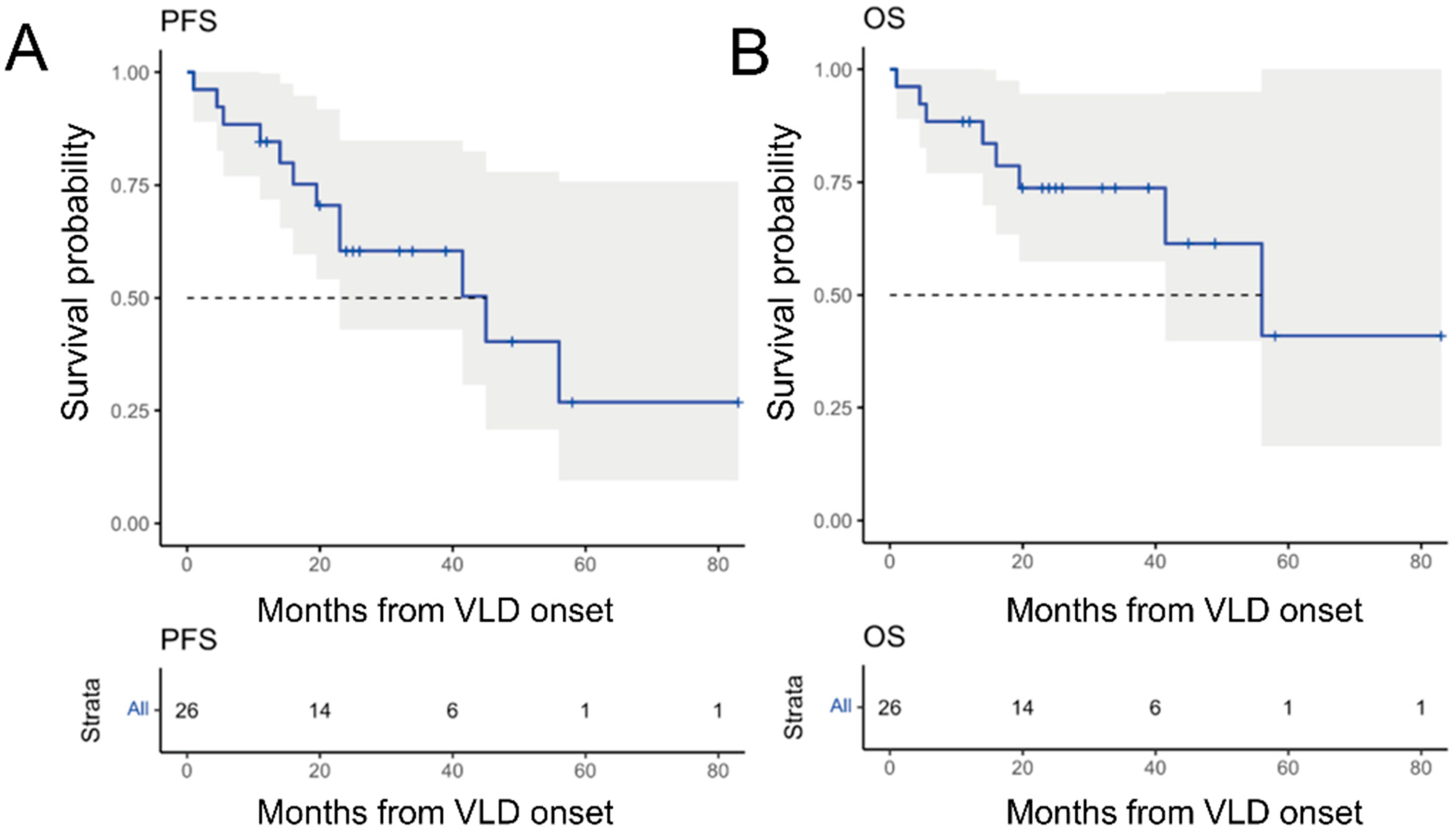
3.4. Overall Responsiveness to Immunotherapy
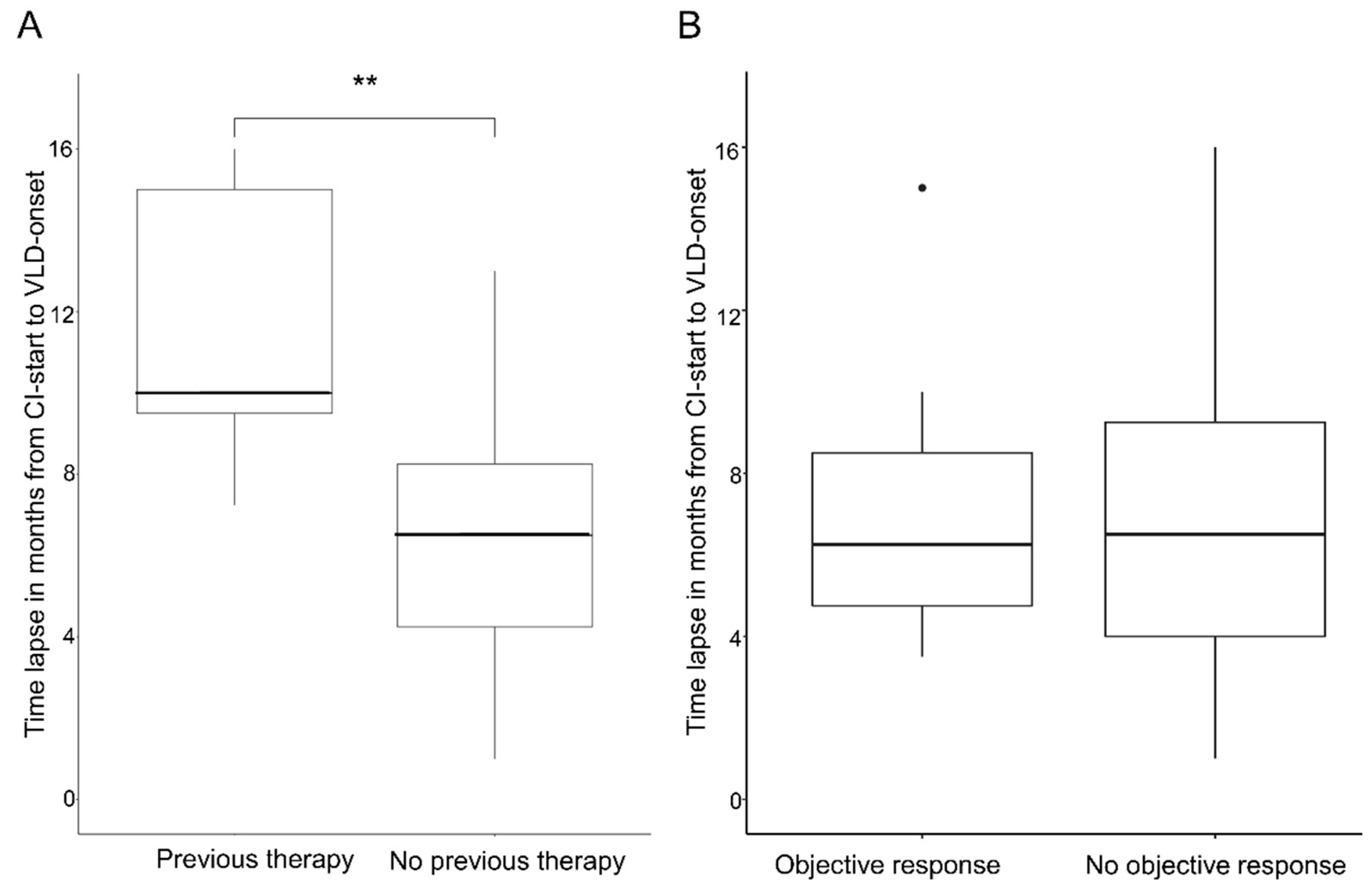
3.5. Parameters Associated with a Better Outcome
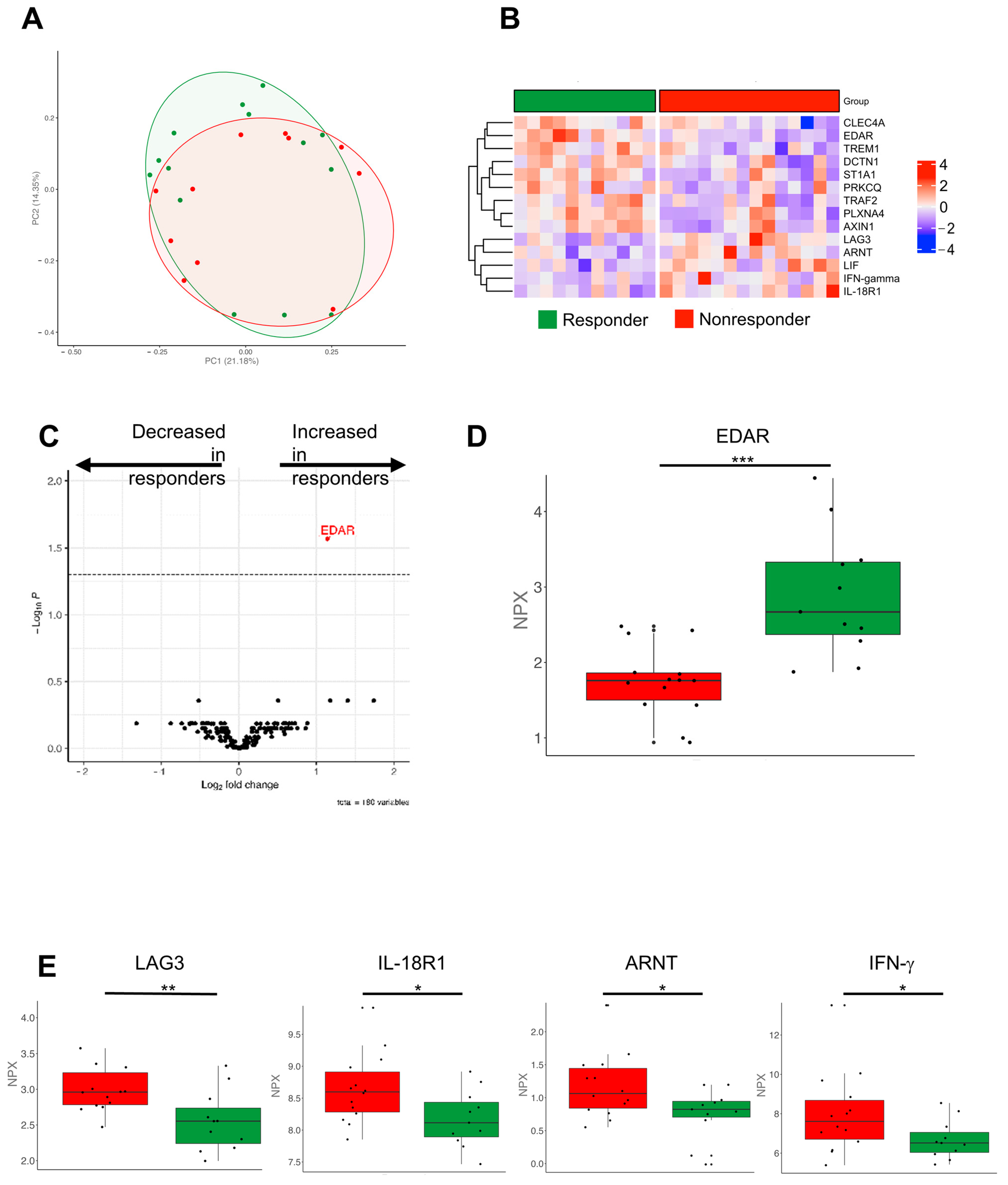
3.6. Molecular Immune Profiles Associated with a Better Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed]
- Dummer, R.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandalà, M.; Kirkwood, J.M.; Sileni, V.C.; Larkin, J.; Nyakas, M.; Dutriaux, C.; et al. Five-Year Analysis of Adjuvant Dabrafenib plus Trametinib in Stage III Melanoma. N. Engl. J. Med. 2020, 383, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Di Giacomo, A.M.; Mortier, L.; Rutkowski, P.; Hassel, J.C.; McNeil, C.M.; Kalinka, E.A.; et al. Five-Year Outcomes With Nivolumab in Patients With Wild-Type BRAF Advanced Melanoma. J. Clin. Oncol. 2020, 38, 3937–3946. [Google Scholar] [CrossRef]
- Robert, C.; Grob, J.J.; Stroyakovskiy, D.; Karaszewska, B.; Hauschild, A.; Levchenko, E.; Chiarion Sileni, V.; Schachter, J.; Garbe, C.; Bondarenko, I.; et al. Five-Year Outcomes with Dabrafenib plus Trametinib in Metastatic Melanoma. N. Engl. J. Med. 2019, 381, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Seidel, J.; Otsuka, A.; Kabashima, K. Anti-PD-1 and Anti-CTLA-4 Therapies in Cancer: Mechanisms of Action, Efficacy, and Limitations. Front. Oncol. 2018, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Quach, H.T.; Dewan, A.K.; Davis, E.J.; Ancell, K.K.; Fan, R.; Ye, F.; Johnson, D.B. Association of Anti–Programmed Cell Death 1 Cutaneous Toxic Effects With Outcomes in Patients With Advanced Melanoma. JAMA Oncol. 2019, 5, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef]
- Rudzki, J.D. Management of adverse events related to checkpoint inhibition therapy. memo-Mag. Eur. Med Oncol. 2018, 11, 132–137. [Google Scholar] [CrossRef]
- Freeman-Keller, M.; Kim, Y.; Cronin, H.; Richards, A.; Gibney, G.; Weber, J.S. Nivolumab in Resected and Unresectable Metastatic Melanoma: Characteristics of Immune-Related Adverse Events and Association with Outcomes. Clin. Cancer Res. 2016, 22, 886–894. [Google Scholar] [CrossRef]
- Hua, C.; Boussemart, L.; Mateus, C.; Routier, E.; Boutros, C.; Cazenave, H.; Viollet, R.; Thomas, M.; Roy, S.; Benannoune, N.; et al. Association of Vitiligo with Tumor Response in Patients with Metastatic Melanoma Treated with Pembrolizumab. JAMA Dermatol. 2016, 152, 45–51. [Google Scholar] [CrossRef]
- Cohen, B.E.; Manga, P.; Lin, K.; Elbuluk, N. Vitiligo and Melanoma-Associated Vitiligo: Understanding Their Similarities and Differences. Am. J. Clin. Dermatol. 2020, 21, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Tanaka, R.; Asami, Y.; Teramoto, Y.; Imamura, T.; Sato, S.; Maruyama, H.; Fujisawa, Y.; Matsuya, T.; Fujimoto, M.; et al. Correlation between vitiligo occurrence and clinical benefit in advanced melanoma patients treated with nivolumab: A multi-institutional retrospective study. J. Dermatol. 2017, 44, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Mineiro dos Santos Garrett, N.F.; Carvalho da Costa, A.C.; Barros Ferreira, E.; Damiani, G.; Diniz dos Reis, P.E.; Inocêncio Vasques, C. Prevalence of dermatological toxicities in patients with melanoma undergoing immunotherapy: Systematic review and meta-analysis. PLoS ONE 2021, 16, e0255716. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, O.; ElHalawani, H.; Ahmed, H. Risk of selected dermatological toxicities in cancer patients treated with MEK inhibitors: A comparative systematic review and meta-analysis. Future Oncol. 2015, 11, 3307–3319. [Google Scholar] [CrossRef]
- Sadreddini, S.; Baradaran, B.; Aghebati-Maleki, A.; Sadreddini, S.; Shanehbandi, D.; Fotouhi, A.; Aghebati-Maleki, L. Immune checkpoint blockade opens a new way to cancer immunotherapy. J. Cell. Physiol. 2019, 234, 8541–8549. [Google Scholar] [CrossRef] [PubMed]
- Curry, J.L.; Tetzlaff, M.T.; Nagarajan, P.; Drucker, C.; Diab, A.; Hymes, S.R.; Duvic, M.; Hwu, W.J.; Wargo, J.A.; Torres-Cabala, C.A.; et al. Diverse types of dermatologic toxicities from immune checkpoint blockade therapy. J. Cutan. Pathol. 2017, 44, 158–176. [Google Scholar] [CrossRef]
- Boniface, K.; Seneschal, J.; Picardo, M.; Taieb, A. Vitiligo: Focus on Clinical Aspects, Immunopathogenesis, and Therapy. Clin. Rev. Allergy Immunol. 2018, 54, 52–67. [Google Scholar] [CrossRef]
- Zottarelli, F.; Giorgione, R.; Gironi, L.C.; Farinelli, P.; Sponghini, A.P.; Rondonotti, D.; Savoia, P. Vitiligo-like depigmentation patterns in patients receiving immunotherapy for metastatic melanoma. Ital. J. Dermatol. Venerol. 2021, 156, 97–99. [Google Scholar] [CrossRef]
- Larsabal, M.; Marti, A.; Jacquemin, C.; Rambert, J.; Thiolat, D.; Dousset, L.; Taieb, A.; Dutriaux, C.; Prey, S.; Boniface, K.; et al. Vitiligo-like lesions occurring in patients receiving anti-programmed cell death-1 therapies are clinically and biologically distinct from vitiligo. J. Am. Acad. Dermatol. 2017, 76, 863–870. [Google Scholar] [CrossRef]
- Boniface, K.; Jacquemin, C.; Darrigade, A.S.; Dessarthe, B.; Martins, C.; Boukhedouni, N.; Vernisse, C.; Grasseau, A.; Thiolat, D.; Rambert, J.; et al. Vitiligo Skin Is Imprinted with Resident Memory CD8 T Cells Expressing CXCR3. J. Investig. Dermatol. 2018, 138, 355–364. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Expert Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Gu, Z. Complex Heatmap Visualization. iMeta 2022, 1, e43. [Google Scholar] [CrossRef]
- Blighe, K.; Rana, S.; Lewis, M. EnhancedVolcano: Publication-Ready Volcano Plots with Enhanced Colouring and Labeling. Available online: https://github.com/kevinblighe/EnhancedVolcano (accessed on 14 September 2022).
- Ando, T.; Kage, H.; Matsumoto, Y.; Zokumasu, K.; Yotsumoto, T.; Maemura, K.; Amano, Y.; Watanabe, K.; Nakajima, J.; Nagase, T.; et al. Integrin alpha11 in non-small cell lung cancer is associated with tumor progression and postoperative recurrence. Cancer Sci. 2020, 111, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Wang, Y.; Wu, Y.; Jia, Z.; Song, Y.; Liang, N. Expression and prognostic analyses of ITGA11, ITGB4 and ITGB8 in human non-small cell lung cancer. PeerJ 2019, 7, e8299. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, L.; Lu, M. Inhibition of integrin subunit alpha 11 restrains gastric cancer progression through phosphatidylinositol 3-kinase/Akt pathway. Bioengineered 2021, 12, 11909–11921. [Google Scholar] [CrossRef] [PubMed]
- Dousset, L.; Pacaud, A.; Barnetche, T.; Kostine, M.; Dutriaux, C.; Pham-Ledard, A.; Beylot-Barry, M.; Gérard, E.; Prey, S.; Andreu, N.; et al. Analysis of tumor response and clinical factors associated with vitiligo in patients receiving anti-programmed cell death-1 therapies for melanoma: A cross-sectional study. JAAD Int. 2021, 5, 112–120. [Google Scholar] [CrossRef]
- Van Geel, N.; Speeckaert, R.; Taieb, A.; Picardo, M.; Böhm, M.; Gawkrodger, D.J.; Schallreuter, K.; Bennett, D.C.; van der Veen, W.; Whitton, M.; et al. Koebner’s phenomenon in vitiligo: European position paper. Pigment Cell Melanoma Res. 2011, 24, 564–573. [Google Scholar] [CrossRef]
- Long, G.V.; Wilmott, J.S.; Haydu, L.E.; Tembe, V.; Sharma, R.; Rizos, H.; Thompson, J.F.; Howle, J.; Scolyer, R.A.; Kefford, R.F. Effects of BRAF inhibitors on human melanoma tissue before treatment, early during treatment, and on progression. Pigment Cell Melanoma Res. 2013, 26, 499–508. [Google Scholar] [CrossRef]
- Sumimoto, H.; Imabayashi, F.; Iwata, T.; Kawakami, Y. The BRAF-MAPK signaling pathway is essential for cancer-immune evasion in human melanoma cells. J. Exp. Med. 2006, 203, 1651–1656. [Google Scholar] [CrossRef]
- Patterson, J.W. Weedon’s Skin Pathology, 5th ed.; Elsevier: London, UK, 2020. [Google Scholar]
- Kim, Y.C.; Kim, Y.J.; Kang, H.Y.; Sohn, S.; Lee, E.S. Histopathologic features in vitiligo. Am. J. Dermatopathol. 2008, 30, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Ramondetta, A.; Ribero, S.; Conti, L.; Fava, P.; Marra, E.; Broganelli, P.; Caliendo, V.; Picciotto, F.; Guida, M.; Fierro, M.T.; et al. Clinical and Pathological Relevance of Drug-induced Vitiligo in Patients Treated for Metastatic Melanoma with Anti-PD1 or BRAF/MEK Inhibitors. Acta Derm. Venereol. 2020, 100, adv00001. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Long-Term Outcomes With Nivolumab Plus Ipilimumab or Nivolumab Alone Versus Ipilimumab in Patients With Advanced Melanoma. J. Clin. Oncol. 2022, 40, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Matsuya, T.; Nakamura, Y.; Matsushita, S.; Tanaka, R.; Teramoto, Y.; Asami, Y.; Uehara, J.; Aoki, M.; Yamamura, K.; Nakamura, Y.; et al. Vitiligo expansion and extent correlate with durable response in anti-programmed death 1 antibody treatment for advanced melanoma: A multi-institutional retrospective study. J. Dermatol. 2020, 47, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Guida, M.; Strippoli, S.; Maule, M.; Quaglino, P.; Ramondetta, A.; Chiaron Sileni, V.; Antonini Cappellini, G.; Queirolo, P.; Ridolfi, L.; Del Vecchio, M.; et al. Immune checkpoint inhibitor associated vitiligo and its impact on survival in patients with metastatic melanoma: An Italian Melanoma Intergroup study. ESMO Open 2021, 6, 100064. [Google Scholar] [CrossRef]
- Long, G.V.; Schachter, J.; Ribas, A.; Arance, A.M.; Grob, J.-J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. 4-year survival and outcomes after cessation of pembrolizumab (pembro) after 2-years in patients (pts) with ipilimumab (ipi)-naive advanced melanoma in KEYNOTE-006. J. Clin. Oncol. 2018, 36, 9503. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Teulings, H.E.; Limpens, J.; Jansen, S.N.; Zwinderman, A.H.; Reitsma, J.B.; Spuls, P.I.; Luiten, R.M. Vitiligo-like depigmentation in patients with stage III-IV melanoma receiving immunotherapy and its association with survival: A systematic review and meta-analysis. J. Clin. Oncol. 2015, 33, 773–781. [Google Scholar] [CrossRef]
- Tawbi, H.A.; Schadendorf, D.; Lipson, E.J.; Ascierto, P.A.; Matamala, L.; Castillo Gutierrez, E.; Rutkowski, P.; Gogas, H.J.; Lao, C.D.; De Menezes, J.J.; et al. Relatlimab and Nivolumab versus Nivolumab in Untreated Advanced Melanoma. N. Engl. J. Med. 2022, 386, 24–34. [Google Scholar] [CrossRef]
- Vial, J.; Royet, A.; Cassier, P.; Tortereau, A.; Dinvaut, S.; Maillet, D.; Gratadou-Hupon, L.; Creveaux, M.; Sadier, A.; Tondeur, G.; et al. The Ectodysplasin receptor EDAR acts as a tumor suppressor in melanoma by conditionally inducing cell death. Cell Death Differ. 2019, 26, 443–454. [Google Scholar] [CrossRef]
- Biechele, T.L.; Kulikauskas, R.M.; Toroni, R.A.; Lucero, O.M.; Swift, R.D.; James, R.G.; Robin, N.C.; Dawson, D.W.; Moon, R.T.; Chien, A.J. Wnt/beta-catenin signaling and AXIN1 regulate apoptosis triggered by inhibition of the mutant kinase BRAFV600E in human melanoma. Sci. Signal. 2012, 5, ra3. [Google Scholar] [CrossRef] [PubMed]
- Celus, W.; Oliveira, A.I.; Rivis, S.; Van Acker, H.H.; Landeloos, E.; Serneels, J.; Cafarello, S.T.; Van Herck, Y.; Mastrantonio, R.; Kohler, A.; et al. Plexin-A4 Mediates Cytotoxic T-cell Trafficking and Exclusion in Cancer. Cancer Immunol. Res. 2022, 10, 126–141. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical and Disease Features of Patients with VLD | |
|---|---|
| Characteristics (n = 28 patients) | |
| Sex, n (%) | |
| Female | 9 (32) |
| Male | 19 (68) |
| Checkpoint inhibitor, n (%) | |
| Nivolumab | 3 (11) |
| Pembrolizumab | 10 (36) |
| Ipilimumab/Nivolumab | 9 (32) |
| Clinical Studies * | 6 (21) |
| Type of melanoma, n (%) | |
| ALM | 1 (4) |
| Nodular | 7 (25) |
| Not clear | 4 (14) |
| Sinunasal | 3 (11) |
| SSM | 4 (14) |
| Unknown primary | 5 (18) |
| Uveal | 3 (11) |
| NA | 1 (4) |
| Previous targeted therapy | |
| Yes | 5 (18) |
| No | 22 (79) |
| NA | 1 (4) |
| BRAF mutated | |
| Yes | 9 (32) |
| No | 18 (64) |
| NA | 1 (4) |
| LDH elevated | |
| Yes | 15(54) |
| No | 13 (46) |
| Tumor stage at melanoma diagnosis, n (%) | |
| I | 1 (4) |
| I-II (uveal) | 3 (11) |
| IIB | 2 (7) |
| IIC | 1 (4) |
| IIIB | 8 (29) |
| IIIC | 6 (21) |
| IV | 6 (21) |
| NA | 1 (4) |
| Tumor stage at VLD diagnosis, n (%) | |
| IIIB | 1 (4) |
| IIIC | 3 (11) |
| IV | 24 (86) |
| Line of immunotherapy before VLD onset, n (%) | |
| Adjuvant | 2 (7) |
| 1st line | 20 (71) |
| 2nd line | 5 (18) |
| 3rd line | 1 (4) |
| Line of systemic therapy in general before VLD onset, n (%) | |
| 1st line | 20 (71) |
| 2nd line | 5 (18) |
| 3rd line | 2 (7) |
| 4th line | 1 (4) |
| Clinical and Disease Features of Patients with VLD | |
|---|---|
| Characteristics (n = 28 patients) | |
| Distribution pattern, n (%) | |
| Symmetric | 20 (71) |
| Asymmetric | 5 (18) |
| NA | 3 (11) |
| Face, n (%) | |
| Yes | 15 (54) |
| No | 5 (18) |
| NA | 8 (29) |
| Scalp, n (%) | |
| Yes | 8 (29) |
| No | 7 (25) |
| NA | 13 (46) |
| Hair, n (%) | |
| Yes | 8 (29) |
| No | 8 (29) |
| NA | 12 (43) |
| Acral, n (%) | |
| Yes | 20 (71) |
| No | 3 (11) |
| NA | 5 (18) |
| Upper extremities, n (%) | |
| Yes | 23 (82) |
| No | 2 (7) |
| NA | 3 (11) |
| Lower extremities, n (%) | |
| Yes | 11 (39) |
| No | 6 (21) |
| NA | 11 (39) |
| Genital area, n (%) | |
| Yes | 3 (11) |
| No | 4 (14) |
| NA | 21 (75) |
| Oral mucosa, n (%) | |
| Yes | 3 (11) |
| No | 7 (25) |
| NA | 18 (64) |
| Neck trunk sun-exposed, n (%) | |
| Yes | 21 (75) |
| No | 3 (11) |
| NA | 4 (14) |
| Lower trunk, n (%) | |
| Yes | 13 (46) |
| No | 7 (25) |
| NA | 8 (29) |
| Trunk general, n (%) | |
| Yes | 20 (71) |
| No | 4 (14) |
| NA | 4 (14) |
| Koebner areas, n (%) | |
| Yes | 16 (57) |
| No | 11 (39) |
| NA | 1 (4) |
| Univariable and Multivariable Cox Regression Analyses of PFS (n = 26) | |||||
|---|---|---|---|---|---|
| Variable | Hazard Ratio (95% CI) | p-Value | Variable | Hazard Ratio (95% CI) | p-Value |
| PFS univariate analysis | PFS multivariate analysis | ||||
| LDH elevated | 0.03 | LDH elevated | 0.02 | ||
| Yes | 1 | Yes | 1 | ||
| No | 0.18 (0.04–0.83) | No | 0.12 (0.021–0.73) | ||
| Dist symmetric | 0.94 | Dist symmetric | 0.80 | ||
| Yes | 1 | Yes | 1 | ||
| No | 0.95 (0.24–3.81) | No | 0.79 (0.15–4.32) | ||
| BRAF mutated | 0.46 | BRAF mutated | 0.49 | ||
| Yes | 1 | Yes | 1 | ||
| No | 1.65 (0.44–6.16) | No | 1.84 (0.32–10.49) | ||
| Koebner | 0.85 | Koebner | 0.61 | ||
| Yes | Yes | ||||
| No | 1.12 (0.35–3.58) | No | 0.62 (0.097–3.94) | ||
| Patches | 0.56 | Patches | 0.81 | ||
| Yes | 1 | Yes | 1 | ||
| No | 0.71 (0.22–2.25) | No | 0.77 (0.09–6.47) | ||
| Macules | 0.49 | Macules | 0.27 | ||
| Yes | 1 | Yes | 1 | ||
| No | 1.52 (0.45–5.17) | No | 0.27 (0.025–2.80) | ||
| Confluent | 0.52 | ||||
| Yes | 1 | ||||
| No | 1.48 (0.45–4.78) | ||||
| Univariable and Multivariable Cox Regression Analyses of OS (n = 26) | |||||
|---|---|---|---|---|---|
| Variable | Hazard Ratio (95% CI) | p-Value | Variable | Hazard Ratio (95% CI) | p-Value |
| OS univariate analysis | OS multivariate analysis | ||||
| LDH elevated | 0.06 | LDH elevated | 0.05 | ||
| Yes | 1 | Yes | 1 | ||
| No | 0.13 (0.016–1.06) | No | 0.10 (0.01–1.04) | ||
| Distribution symmetric | 0.41 | Distribution symmetric | 0.44 | ||
| Yes | 1 | Yes | 1 | ||
| No | 1.96 (0.40–9.53) | No | 2.33 (0.27–19.8) | ||
| BRAF mutated | 0.55 | BRAF mutated | 0.32 | ||
| Yes | 1 | Yes | 1 | ||
| No | 1.63 (0.32–8.20) | No | 4.02 (0.27–60.4) | ||
| Koebner | 0.9 | Koebner | 0.26 | ||
| Yes | Yes | ||||
| No | 0.9 (0.21–3.8) | No | 0.32 (0.04–2.33) | ||
| Patches | 0.26 | Macules | 0.17 | ||
| Yes | 1 | Yes | 1 | ||
| No | 0.43 (0.10–1.85) | No | 0.14 (0.001–2.39) | ||
| Macules | 0.37 | ||||
| Yes | 1 | ||||
| No | 1.93 (0.45–8.19) | ||||
| Confluent | 0.34 | ||||
| Yes | 1 | ||||
| No | 1.99 (0.48–8.30) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hermann, N.; Maul, L.V.; Ameri, M.; Traidl, S.; Ziadlou, R.; Papageorgiou, K.; Kolm, I.; Levesque, M.; Maul, J.-T.; Brüggen, M.-C. Clinical Presentation and Prognostic Features in Patients with Immunotherapy-Induced Vitiligo-like Depigmentation: A Monocentric Prospective Observational Study. Cancers 2022, 14, 4576. https://doi.org/10.3390/cancers14194576
Hermann N, Maul LV, Ameri M, Traidl S, Ziadlou R, Papageorgiou K, Kolm I, Levesque M, Maul J-T, Brüggen M-C. Clinical Presentation and Prognostic Features in Patients with Immunotherapy-Induced Vitiligo-like Depigmentation: A Monocentric Prospective Observational Study. Cancers. 2022; 14(19):4576. https://doi.org/10.3390/cancers14194576
Chicago/Turabian StyleHermann, Nicola, Lara Valeska Maul, Milad Ameri, Stephan Traidl, Reihane Ziadlou, Karolina Papageorgiou, Isabel Kolm, Mitchell Levesque, Julia-Tatjana Maul, and Marie-Charlotte Brüggen. 2022. "Clinical Presentation and Prognostic Features in Patients with Immunotherapy-Induced Vitiligo-like Depigmentation: A Monocentric Prospective Observational Study" Cancers 14, no. 19: 4576. https://doi.org/10.3390/cancers14194576
APA StyleHermann, N., Maul, L. V., Ameri, M., Traidl, S., Ziadlou, R., Papageorgiou, K., Kolm, I., Levesque, M., Maul, J.-T., & Brüggen, M.-C. (2022). Clinical Presentation and Prognostic Features in Patients with Immunotherapy-Induced Vitiligo-like Depigmentation: A Monocentric Prospective Observational Study. Cancers, 14(19), 4576. https://doi.org/10.3390/cancers14194576