Acupuncture for Managing Cancer-Related Fatigue in Breast Cancer Patients: A Systematic Review and Meta-Analysis

 , , , , , and
, , , , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Registration
2.2. Database and Search Strategy
2.3. Inclusion and Exclusion Criteria
2.3.1. Study Design
2.3.2. Participants
2.3.3. Interventions
2.3.4. Comparators
2.3.5. Outcomes
2.4. Study Selection and Data Extraction
2.5. Risk of Bias (ROB) Assessment
2.6. Certainty of Evidence (CoE)
2.7. Data Analysis
3. Results
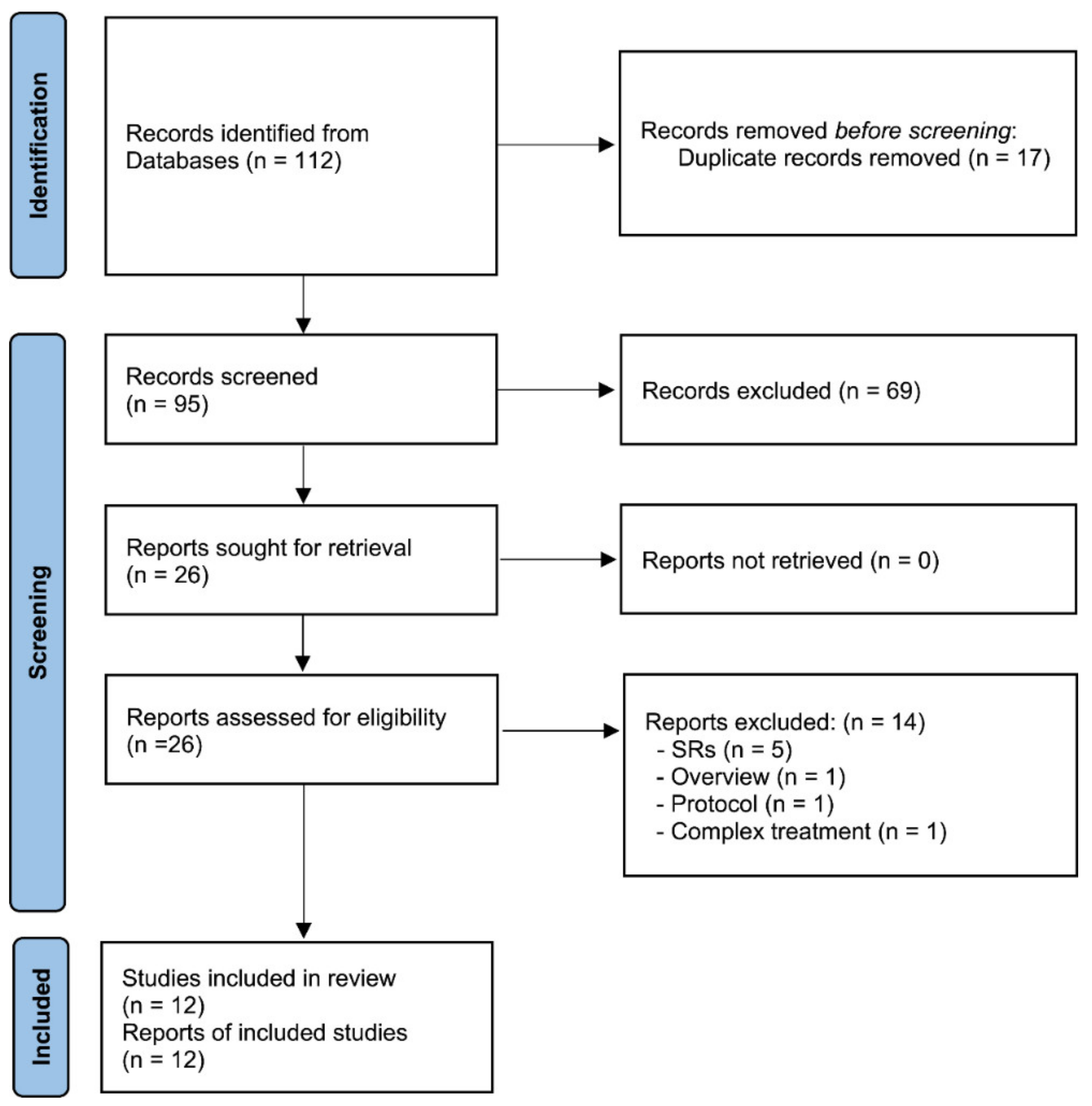
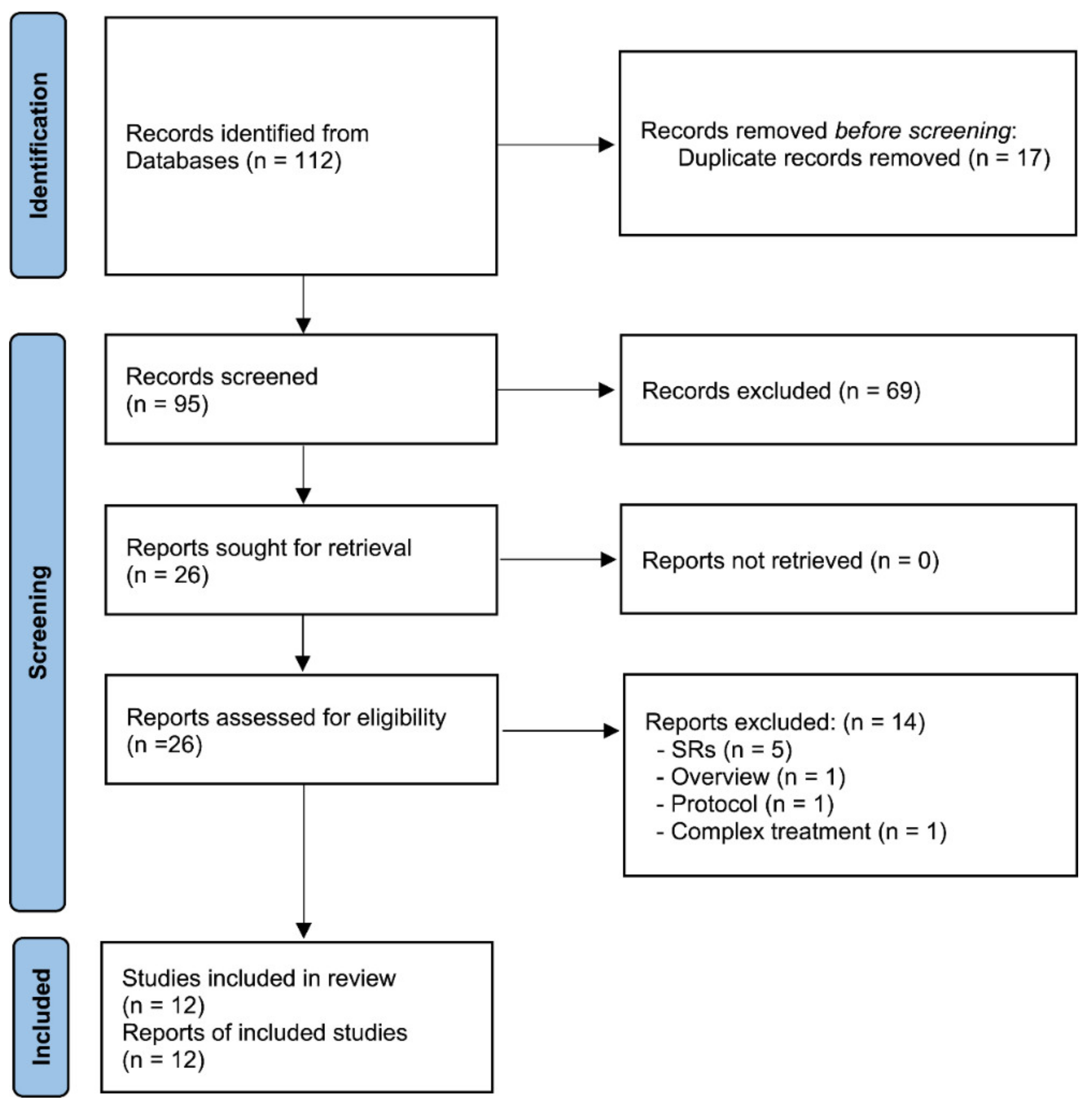
3.1. Study Identification
3.2. Characteristics of the Included Studies
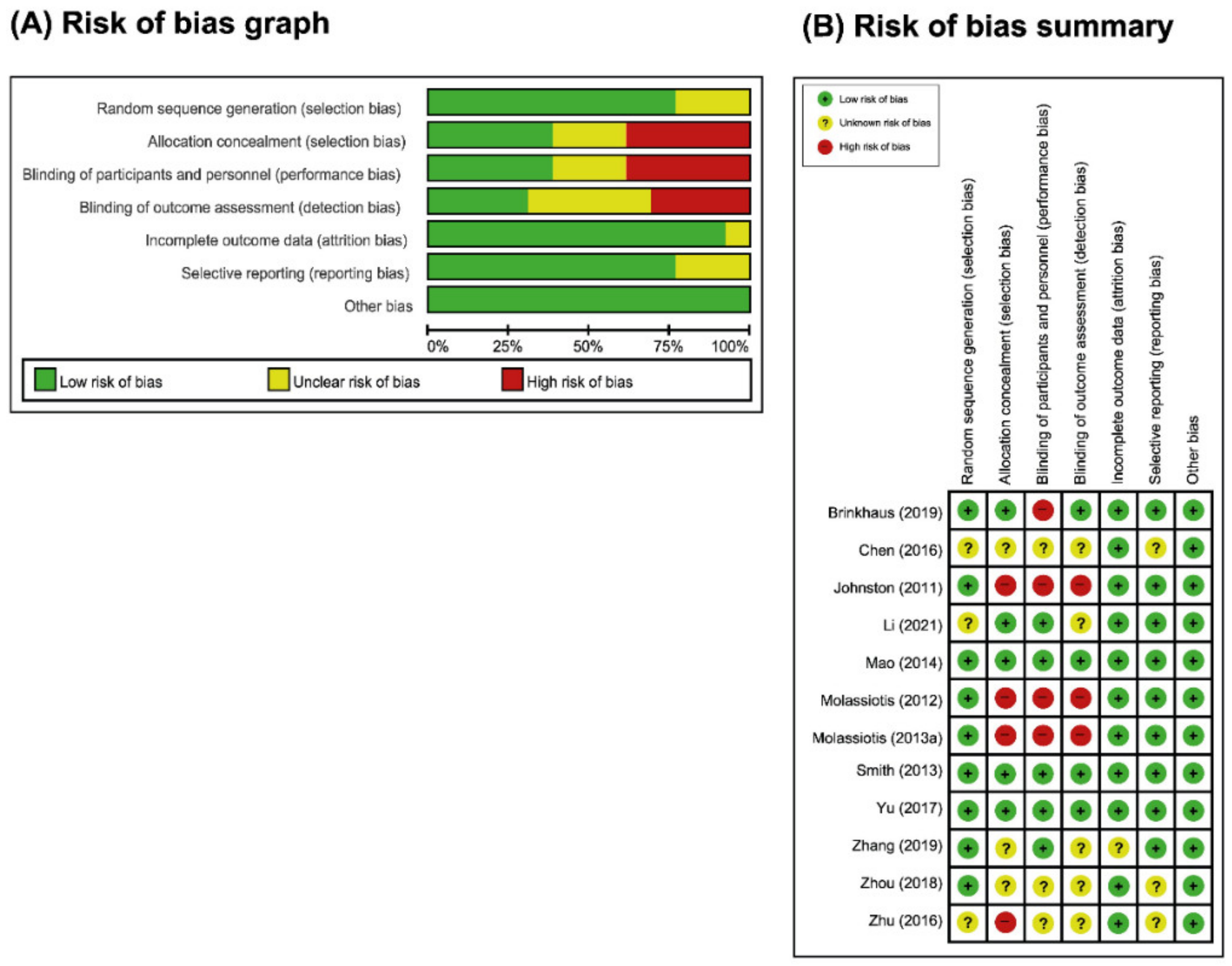
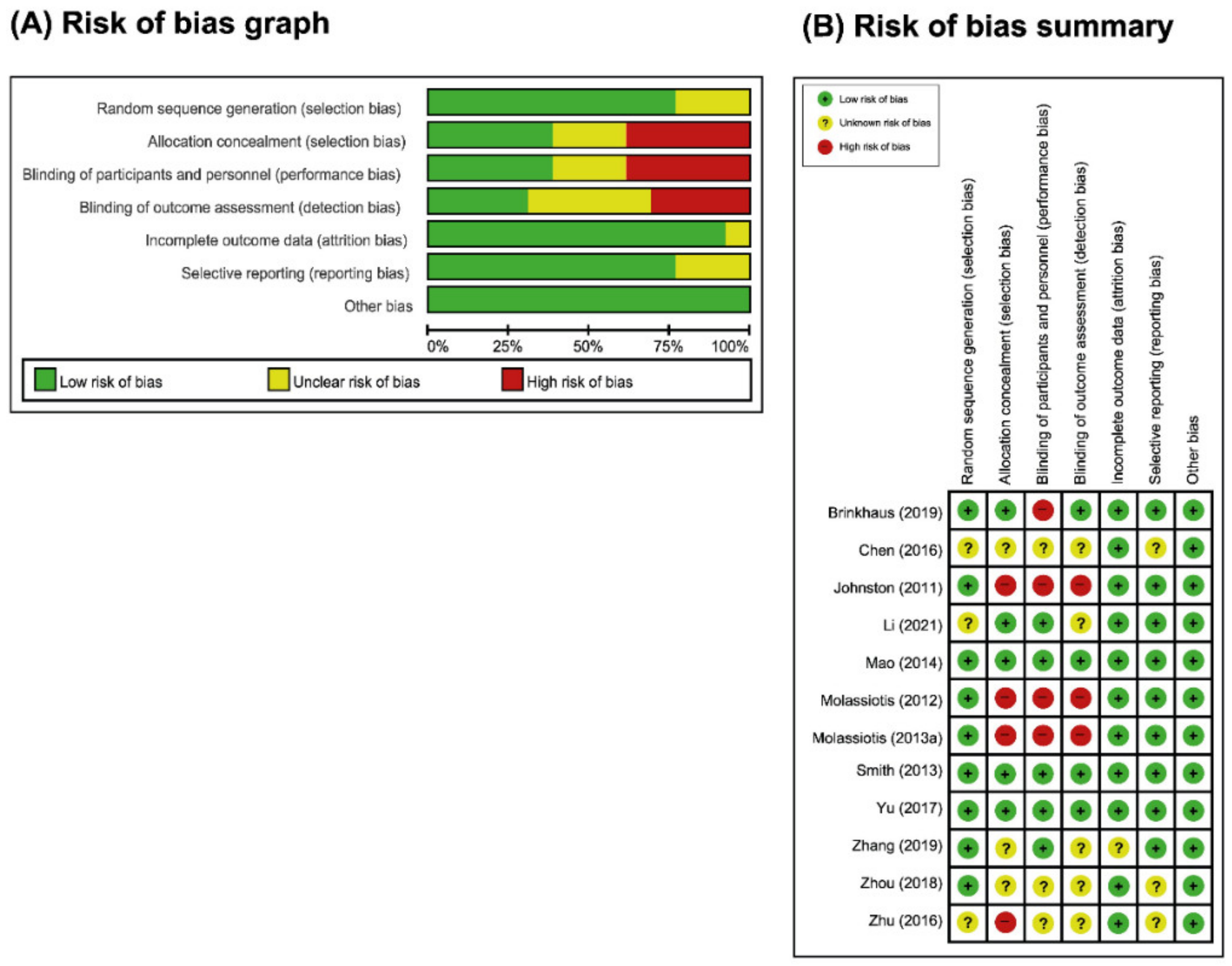
3.3. ROB Assessment
3.4. Outcome Measures
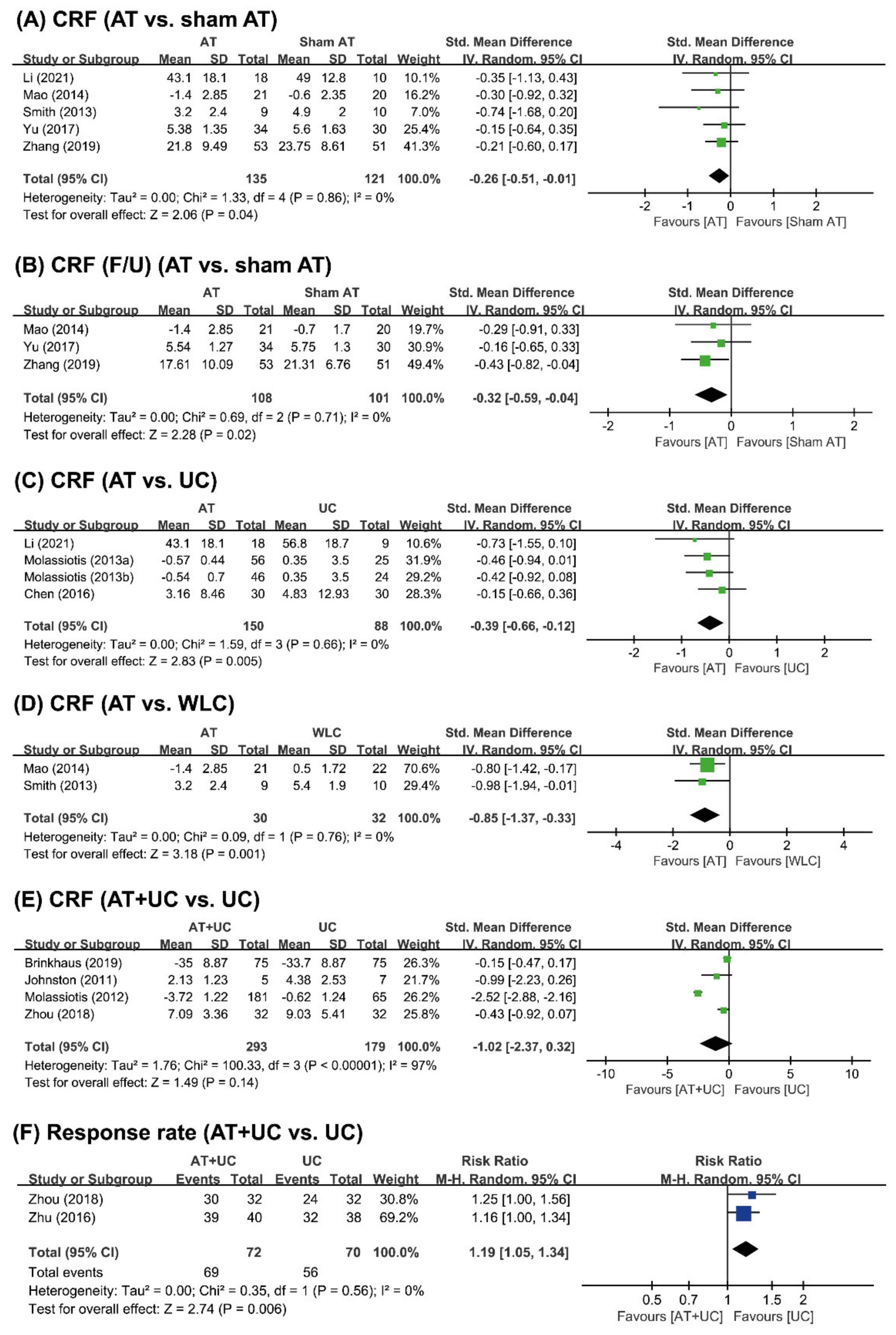
3.4.1. AT vs. Sham AT
3.4.2. AT vs. UC or WLC
3.4.3. AT+UC vs. UC
3.5. AEs
3.6. Certainty of Evidence
4. Discussion
4.1. Summary of Main Results
4.2. Overall Completeness and Applicability of Evidence
4.3. Agreements and Disagreements with Other Reviews
4.4. Limitations of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Juvet, L.K.; Thune, I.; Elvsaas, I.; Fors, E.A.; Lundgren, S.; Bertheussen, G.; Leivseth, G.; Oldervoll, L.M. The effect of exercise on fatigue and physical functioning in breast cancer patients during and after treatment and at 6 months follow-up: A meta-analysis. Breast 2017, 33, 166–177. [Google Scholar] [CrossRef]
- Noal, S.; Levy, C.; Hardouin, A.; Rieux, C.; Heutte, N.; Ségura, C.; Collet, F.; Allouache, D.; Switsers, O.; Delcambre, C.; et al. One-year longitudinal study of fatigue, cognitive functions, and quality of life after adjuvant radiotherapy for breast cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 795–803. [Google Scholar] [CrossRef]
- Ebede, C.C.; Jang, Y.; Escalante, C.P. Cancer-related fatigue in cancer survivorship. Med. Clin. N. Am. 2017, 101, 1085–1097. [Google Scholar] [CrossRef] [PubMed]
- Minton, O.; Stone, P. How common is fatigue in disease-free breast cancer survivors? a systematic review of the literature. Breast Cancer Res. Treat 2008, 112, 5–13. [Google Scholar] [CrossRef]
- Saligan, L.N.; Olson, K.; Filler, K.; Larkin, D.; Cramp, F.; Yennurajalingam, S.; Escalante, C.P.; del Giglio, A.; Kober, K.M.; Kamath, J.; et al. The biology of cancer-related fatigue: A review of the literature. Support. Care Cancer 2015, 23, 2461–2478. [Google Scholar] [CrossRef]
- Maass, S.; Brandenbarg, D.; Boerman, L.M.; Verhaak, P.F.M.; de Bock, G.H.; Berendsen, A.J. Fatigue among long-term breast cancer survivors: A controlled cross-sectional study. Cancers 2021, 13, 1301. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.B.; Zhai, J.; Wang, T.; Zhou, H.J.; Zhao, I.; Liu, X.L. Self-Managed Non-Pharmacological Interventions for Breast Cancer Survivors: Systematic Quality Appraisal and Content Analysis of Clinical Practice Guidelines. Front. Oncol. 2022, 12, 866284. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.S.; Woodruff, J.F. Cancer-related and treatment-related fatigue. Gynecol. Oncol. 2015, 136, 446–452. [Google Scholar] [CrossRef]
- Berger, A.M.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.S.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; Escalante, C.P.; et al. Cancer-Related Fatigue, Version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 1012–1039. [Google Scholar] [CrossRef]
- Lau, C.H.Y.; Wu, X.; Chung, V.C.H.; Liu, X.; Hui, E.P.; Cramer, H.; Lauche, R.; Wong, S.Y.S.; Lau, A.Y.L.; Sit, R.W.S.; et al. Acupuncture and related therapies for symptom management in palliative cancer care: Systematic review and meta-analysis. Medicine 2016, 95, e2901. [Google Scholar] [CrossRef]
- Cheng, C.S.; Chen, L.Y.; Ning, Z.Y.; Zhang, C.Y.; Chen, H.; Chen, Z.; Zhu, X.Y.; Xie, J. Acupuncture for cancer-related fatigue in lung cancer patients: A randomized, double blind, placebo-controlled pilot trial. Support. Care Cancer 2017, 25, 3807–3814. [Google Scholar] [CrossRef] [PubMed]
- Pudkasam, S.; Feehan, J.; Talevski, J.; Vingrys, K.; Polman, R.; Chinlumprasert, N.; Stojanovska, L.; Apostolopoulos, V. Motivational strategies to improve adherence to physical activity in breast cancer survivors: A systematic review and meta-analysis. Maturitas 2021, 152, 32–47. [Google Scholar] [CrossRef] [PubMed]
- Roldan-Jimenez, C.; Pajares, B.; Ruiz-Medina, S.; Trinidad-Fernandez, M.; Gonzalez-Sanchez, M.; Ribelles, N.; Garcia-Almeida, J.M.; Rios-Lopez, M.J.; Alba, E.; Cuesta-Vargas, A.I. Design and implementation of a standard care programme of therapeutic exercise and education for breast cancer survivors. Support. Care Cancer 2022, 30, 1243–1251. [Google Scholar] [CrossRef] [PubMed]
- Birch, S.; Lee, M.S.; Alraek, T.; Kim, T.H. Evidence, safety and recommendations for when to use acupuncture for treating cancer related symptoms: A narrative review. Integr. Med. Res. 2019, 8, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Mao, H.; Mao, J.J.; Guo, M.; Cheng, K.; Wei, J.; Shen, X.; Shen, X. Effects of infrared laser moxibustion on cancer-related fatigue: A randomized, double-blind, placebo-controlled trial. Cancer 2016, 122, 3667–3672. [Google Scholar] [CrossRef] [PubMed]
- Chien, T.J.; Liu, C.Y.; Fang, C.J. The effect of acupuncture in breast cancer-related Lymphoedema (BCRL): A systematic review and meta-analysis. Integr. Cancer Ther. 2019, 18, 1534735419866910. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Pei, L.; Song, Y.; Wu, J.; Geng, H.; Chen, L.; Wang, Y.; Hu, Y.; Zhou, J.; Sun, J. Acupuncture therapy for breast cancer-related lymphedema: A systematic review and meta-analysis. J. Obstet. Gynaecol. Res. 2019, 45, 2307–2317. [Google Scholar] [CrossRef]
- Chen, Y.P.; Liu, T.; Peng, Y.Y.; Wang, Y.P.; Chen, H.; Fan, Y.F.; Zhang, L. Acupuncture for hot flashes in women with breast cancer: A systematic review. J. Cancer Res. Ther. 2016, 12, 535–542. [Google Scholar] [CrossRef]
- Chien, T.J.; Hsu, C.H.; Liu, C.Y.; Fang, C.J. Effect of acupuncture on hot flush and menopause symptoms in breast cancer—A systematic review and meta-analysis. PLoS ONE 2017, 12, e0180918. [Google Scholar] [CrossRef] [Green Version]
- Chien, T.J.; Liu, C.Y.; Chang, Y.F.; Fang, C.J.; Hsu, C.H. Acupuncture for treating aromatase inhibitor-related arthralgia in breast cancer: A systematic review and meta-analysis. J. Altern. Complement. Med. 2015, 21, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lu, J.; Wang, G.; Chen, X.; Xv, H.; Huang, J.; Xue, M.; Tang, J. Acupuncture for arthralgia Induced by aromatase inhibitors in patients with breast cancer: A systematic review and meta-analysis. Integr. Cancer Ther. 2021, 20, 1534735420980811. [Google Scholar] [CrossRef]
- Shih, Y.W.; Su, J.Y.; Kung, Y.S.; Lin, Y.H.; To Anh, D.T.; Ridwan, E.S.; Tsai, H.T. Effectiveness of acupuncture in relieving chemotherapy-induced leukopenia in patients with breast cancer: A systematic review with a meta-analysis and trial sequential analysis. Integr. Cancer Ther. 2021, 20, 15347354211063884. [Google Scholar] [CrossRef]
- Li, H.; Schlaeger, J.M.; Jang, M.K.; Lin, Y.; Park, C.; Liu, T.; Sun, M.; Doorenbos, A.Z. Acupuncture improves multiple treatment-related symptoms in breast cancer survivors: A systematic review and meta-analysis. J. Altern. Complement. Med. 2021, 27, 1084–1097. [Google Scholar] [CrossRef]
- Zhang, Y.; Sun, Y.; Li, D.; Liu, X.; Fang, C.; Yang, C.; Luo, T.; Lu, H.; Li, H.; Zhang, H.; et al. Acupuncture for breast cancer: A systematic review and meta-analysis of patient-reported outcomes. Front. Oncol 2021, 11, 646315. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Tang, Y.; Liang, H.; Chen, G.; Shen, X.; Dong, Y.; Cui, Q.; Qi, M. Acupuncture for hormone therapy-related side effects in breast cancer patients: A GRADE-assessed systematic review and updated meta-analysis. Integr. Cancer Ther. 2020, 19, 1534735420940394. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, L.; Li, H.; Hu, Y.; Tian, L. Effects of acupuncture on cancer-related fatigue: A meta-analysis. Support. Care Cancer 2018, 26, 415–425. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Bmj 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Birch, S.; Lee, M.S.; Kim, T.-H.; Alraek, T. On defining acupuncture and its techniques: A commentary on the problem of sham. Integr. Med. Res. 2022, 11, 100834. [Google Scholar] [CrossRef]
- Birch, S.; Lee, M.S.; Kim, T.-H.; Alraek, T. Historical perspectives on using sham acupuncture in acupuncture clinical trials. Integr. Med. Res. 2022, 11, 100725. [Google Scholar] [CrossRef]
- Lee, I.-S.; Chae, Y. Cognitive components of acupuncture treatment. Integr. Med. Res. 2021, 10, 100754. [Google Scholar] [CrossRef]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D.; on behalf of the, STRICTA Revision Group. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT Statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-P. GRADE Methods in traditional medicine. Integr. Med. Res. 2022, 11, 100836. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.F.; Liu, D.Q.; Nie, J.Y.; Chen, D.D.; Yan, M.; Zuo, Z.; Liu, L.X.; Wang, W.Y.; Zhu, M.S.; Li, W.H. ATAS acupuncture reduces chemotherapy induced fatigue in breast cancer through Regulating ADROA1 expression: A randomized sham-controlled pilot trial. Onco. Targets Ther. 2020, 13, 11743–11754. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.; Carmady, B.; Thornton, C.; Perz, J.; Ussher, J.M. The effect of acupuncture on post-cancer fatigue and well-being for women recovering from breast cancer: A pilot randomised controlled trial. Acupunct. Med. 2013, 31, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.J.; Farrar, J.T.; Bruner, D.; Zee, J.; Bowman, M.; Seluzicki, C.; DeMichele, A.; Xie, S.X. Electroacupuncture for fatigue, sleep, and psychological distress in breast cancer patients with aromatase inhibitor-related arthralgia: A randomized trial. Cancer 2014, 120, 3744–3751. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, C.; Xu, X.H.; Zhang, Q. Clinical observation on acupuncture of reconciling qi and blood, tonifying heart and mind method in the treatment of 53 patients of breast cancer chemotherapy-related cognitive impairment with disorder of qi and blood syndrome. J. Tradit. Chin. Med. 2019, 60, 509–513. [Google Scholar] [CrossRef]
- Yu, M.W.; Li, D.R.; Yang, G.W.; Xu, Y.M.; Wang, X.M. Effects of acupuncture on cacner-related fatigue in breast cancer patients at the rehabilitation stage: A randimized controlled trial. Chin. Med. Herald 2017, 14, 89–93. [Google Scholar]
- Chen, J.; Fang, N.Q.; Wang, L.; Wu, X.M.; Xia, H.; Sun, C.L. Clinical study on 30 cases of cancer-related fatigue in patients with breast cancer treated with acupuncture. Jiangsu J. Tradit. Chin. Med. 2016, 48, 56–58. [Google Scholar]
- Molassiotis, A.; Bardy, J.; Finnegan-John, J.; Mackereth, P.; Ryder, W.D.; Filshie, J.; Ream, E.; Eaton, D.; Richardson, A. A randomized, controlled trial of acupuncture self-needling as maintenance therapy for cancer-related fatigue after therapist-delivered acupuncture. Ann. Oncol. 2013, 24, 1645–1652. [Google Scholar] [CrossRef]
- Brinkhaus, B.; Kirschbaum, B.; Stöckigt, B.; Binting, S.; Roll, S.; Carstensen, M.; Witt, C.M. Prophylactic acupuncture treatment during chemotherapy with breast cancer: A randomized pragmatic trial with a retrospective nested qualitative study. Breast Cancer Res. Treat. 2019, 178, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Tian, H.Q.; Zeng, B.Y.; He, X.F. Clinical observation on acupuncture on three anti-fatigue acupoints in the treatment of cancer-induced fatigue in patients with breast cancer. Acta. Chin. Med. 2018, 33, 950–953. [Google Scholar] [CrossRef]
- Molassiotis, A.; Bardy, J.; Finnegan-John, J.; Mackereth, P.; Ryder, D.W.; Filshie, J.; Ream, E.; Richardson, A. Acupuncture for cancer-related fatigue in patients with breast cancer: A pragmatic randomized controlled trial. J. Clin. Oncol. 2012, 30, 4470–4476. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.F.; Hays, R.D.; Subramanian, S.K.; Elashoff, R.M.; Axe, E.K.; Li, J.J.; Kim, I.; Vargas, R.B.; Lee, J.; Yang, L.; et al. Patient education integrated with acupuncture for relief of cancer-related fatigue randomized controlled feasibility study. BMC Complement. Altern. Med. 2011, 11, 49. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.L.; Lu, H.Y.; Lu, Y.Y.; Wu, L.J. Clinical observation on leukopenia after chemotherapy for breast cancer treated with acupuncture for nourishing qi and blood. Shanghai J. Acupunct. Moxi. 2016, 35, 964–966. [Google Scholar] [CrossRef]
- Cybularz, P.A.; Brothers, K.; Singh, G.M.; Feingold, J.L.; Lewis, M.E.; Niesley, M.L. The safety of acupuncture in patients with cancer therapy-related thrombocytopenia. Med. Acupunct. 2015, 27, 224–229. [Google Scholar] [CrossRef]
- Hoxtermann, M.D.; Haller, H.; Aboudamaah, S.; Bachemir, A.; Dobos, G.; Cramer, H.; Voiss, P. Safety of acupuncture in oncology: A systematic review and meta-analysis of randomized controlled trials. Cancer 2022, 128, 2159–2173. [Google Scholar] [CrossRef] [PubMed]
- Halámková, J.; Dymáčková, R.; Adámková Krákorová, D. Acupuncture from the perspective of evidence-based medicine—Options of clinical use based on National Comprehensive Cancer Network (NCCN) guidelines. Klin. Onkol. 2022, 35, 94–99. [Google Scholar] [CrossRef]
- Fabi, A.; Bhargava, R.; Fatigoni, S.; Guglielmo, M.; Horneber, M.; Roila, F.; Weis, J.; Jordan, K.; Ripamonti, C.I. Cancer-related fatigue: ESMO clinical practice guidelines for diagnosis and treatment. Ann. Oncol. 2020, 31, 713–723. [Google Scholar] [CrossRef]
- Arring, N.M.; Barton, D.L.; Brooks, T.; Zick, S.M. Integrative therapies for cancer-related fatigue. Cancer J. 2019, 25, 349–356. [Google Scholar] [CrossRef]
- Pan, Y.; Yang, K.; Shi, X.; Liang, H.; Shen, X.; Wang, R.; Ma, L.; Cui, Q.; Yu, R.; Dong, Y. Clinical benefits of acupuncture for the reduction of hormone therapy-related side effects in breast cancer patients: A systematic review. Integr. Cancer Ther. 2018, 17, 602–618. [Google Scholar] [CrossRef] [PubMed]
- Choi, T.Y.; Ang, L.; Jun, J.H.; Alraek, T.; Lee, M.S. Acupuncture and moxibustion for cancer-related Fatigue: An overview of systematic reviews and meta-analysis. Cancers 2022, 14, 2347. [Google Scholar] [CrossRef] [PubMed]
- Witt, C.M.; Aickin, M.; Baca, T.; Cherkin, D.; Haan, M.N.; Hammerschlag, R.; Hao, J.J.; Kaplan, G.A.; Lao, L.; McKay, T.; et al. Effectiveness Guidance Document (EGD) for acupuncture research—A consensus document for conducting trials. BMC Complement. Altern. Med. 2012, 12, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Author (Year) [Ref] Country | Sample Size/ Cancer Stage/Current Antitumor Treatment Mean Age (Year) | Intervention (Regimen, Randomized/ Analysed) | Control (Regimen, Randomized/ Analysed) | Fatigue Measurement | Result | AEs/Trial Registration Number |
|---|---|---|---|---|---|---|
| Li (2020) [34] China | 40/I to III/ongoing-chemo A: 47.5; B: 42; C: 50.5 | (A) AT (1 time weekly for 20 weeks, n = 20/18) | (B) Sham AT (noninsertive stimulation at non-AT points, n = 10/10) (C) UC (n = 10/10) | MFI-20 | A vs. B: MD −5.90 [−17.43, 5.63], p = 0.32; A vs. C: MD −13.70 [−28.50, 1.10], p = 0.07 | Bruising ChiCTR-IPR-17013652 |
| Smith (2013) [35] Australia | 30/NR/off-treatment A: 55.0; B: 53.0; C: 58.0 | (A) AT (2 times weekly for 3 weeks and once weekly for 3 weeks, n = 10/9) | (B) Sham AT (noninsertive stimulation at non-AT points, n = 10/10) (C) WLC (n = 10/10) | BFI | A vs. B: MD −1.70 [−3.70, 0.30], p = 0.10; A vs. C: MD −2.20 [−4.16, −0.24], p = 0.03 | NR/ACTRN12610000720011 |
| Mao (2014) [36] USA | 67/I to III/ongoing- HT A: 57.5; B: 60.9; C: 60.6 | (A) EA (2 times weekly for 2 weeks and once weekly for 6 weeks, n = 22/21) | (B) Sham EA (noninsertive stimulation at non-AT points, n = 22/20) (C) WLC (n = 23/22) | BFI | A vs. B: MD −0.80 [−2.40, 0.80], p = 0.33; F/U: MD −0.70 [−2.13, 0.73], p = 0.34 A vs. C: MD −1.90 [−3.32, −0.48], p = 0.008; F/U: MD −1.60 [−3.14, −0.06], p = 0.04 | NR/NCT01013337 |
| Zhang (2019) [37] China | 104/I to IV/off-surgery A: 45.1; B: 45.6 | (A) AT (2 times weekly for 8 weeks, n = 53/53) | (B) Sham AT (noninsertive stimulation at non-AT points, n = 51/51) | EORTC QLQ-C30_Fatigue | MD −1.95 [−5.43, 1.53], p = 0.27; F/U: MD −3.70 [−6.99, −0.41], p = 0.03 | NR/NR |
| Yu (2017) [38] China | 72/I to III/off-treatment A: 50.2; B: 51.4 | (A) AT (2 times weekly for 4 weeks, n = 36/34) | (B) Sham AT (noninsertive stimulation at non-AT points, n = 36/30) | PFS | MD −0.22 [−0.96, 0.52], p = 0.56; F/U: MD −0.21 [−0.84, 0.42], p = 0.51 | NR/ISRCTN71727232 |
| Chen (2016) [39] China | 60/I to IV/ongoing-chemo A: 50.9; B: 51.2 | (A) AT (1 session [1 time daily for 10 days], total 2 session, n = 30/30) | (B) UC (n = 30/30) | (1) BFI (2) ER | (1) MD −1.67 [−7.20, 3.86], p = 0.55 (2) RR 1.21 [1.00, 1.46], p = 0.05 | NR/NR |
| Molassiotis (2013) [40] UK | 197/I to III/off-treatment NR | (A) AT (1 time weekly for 10 weeks, n = 65/56) (B) Self AT (n = 67/46) | (C) UC (n = 65/49) | MFI | A vs. C: MD −0.92 [−2.30, 0.46], p = 0.19; B vs. C: MD −0.89 [−2.30, 0.52], p = 0.22 | NR/NCT00957112 |
| Brinkhaus (2019) [41] Germany | 150/I to III/ongoing-chemo A: 51.4; B: 50.6 | (A) AT (NR for 6 months, least 6 sessions), n = 75/65) + (B) | (B) UC (n = 75/55) | FACIT-fatigue | MD −1.30 [−4.49, 1.89,], p = 0.42 | NR/NCT01727362 |
| Zhou (2018) [42] China | 64/I to IV/mix off and ongoing chemo A: 52; B: 50 | (A) AT (3 times weekly for 5 weeks, n = 32/32) + (B) | (B) UC (n = 32/32) | (1) TCM Symptom Evaluation-fatigue (2) ER | (1) MD −1.94 [−4.15, 0.27], p = 0.08 (2) RR 1.25 [1.00, 1.56], p = 0.05 | NR/NR |
| Molassiotis (2012) [43] UK | 302/NR/off-treatment A: 52; B: 53 | (A) AT (1 time weekly for 6 weeks, n = 227/181) + (B) | (B) UC (n = 75/65) | MFI | MD −3.10 [−3.45, −2.75], p < 0.00001 | None/NCT00957112 |
| Johnston (2011) [44] USA | 13/NR/off-treatment A: 55; B: 53 | (A) AT (1 time weekly for 8 weeks, n = 6/5) + (B) | (B) UC (n = 7/7) | BFI | MD −2.25 [−4.41, −0.09], p = 0.04 | None/NCT00646633 |
| Zhu (2016) [45] China | 78/I to IV/ongoing-chemo A: 47; B: 46 | (A) AT (1 time for 5 days, n = 40/40) + (B) | (B) UC (n = 38/38) | ER (TCM Symptom Evaluation-fatigue) | RR 1.16 [1.00, 1.34], p = 0.05 | NR/NR |
| First Author (Year) (Ref) | Acupuncture Rationale | Names of Acupoints | Response Sought | Needle Retention Time | Treatment Regime (Total Session)/Follow-Up |
|---|---|---|---|---|---|
| Li (2021) [34] | TCM | NR | NR | 30 min | Once weekly for 20 weeks (20 sessions)/NR |
| Smith (2013) [35] | TCM | KI3, KI27, ST36, SP6, CV4, CV6 | De qi | 20~40 min | Twice weekly for 3 weeks and once weekly for 3 weeks (9 sessions)/NR |
| Mao (2014) [36] | TCM | SP6, ST36 | De qi | 30 min | Twice weekly for 2 weeks and once weekly for 6 weeks (10 sessions)/12 weeks |
| Zhang (2019) [37] | TCM | ST36, SP10, CV17, CV12, GV20 CV7, GV16, BL15, BL45, HT5, KI6 | De qi | 20 min | Twice weekly for 8 weeks (16 sessions)/16 weeks |
| Yu (2017) [38] | TCM | GV20, PC6, CV6, ST36, SP6 | De qi | NR | Twice weekly for 4 weeks (8 sessions)/8 weeks |
| Chen (2016) [39] | TCM | GV20, HT7, GV4, GB39, SP6, ST36, SP10 | De qi | 30 min | Once daily for 10 days, rest 2 days, total 2 courses (20 sessions)/NR |
| Molassiotis (2013) [40] | TCM | LI4, SP6, ST36 | De qi | 20 min | Once weekly for 10 weeks (10 sessions)/NR |
| Brinkhaus (2019) [41] | TCM | PC6, ST36, ST44, CV10, CV12, ST42, LI11, LI10, GV20, CV4, CV6 | De qi | NR | NR for 6 months (least 6 sessions)/NR |
| Zhou (2018) [42] | TCM | Sishen, SP6, ST36, LR3, LR5 | De qi | 30 min | Third weekly for 5 weeks (15 sessions)/NR |
| Molassiotis (2012) [43] | TCM | LI4, SP6, ST36 | De qi | 20 min | Once weekly for 6 weeks (6 session)/NR |
| Johnston (2011) [44] | TCM/clinical experience | KI 3, LI4, SP6, ST36, SP6, SP4, LU7, KI4, EX-HN3, GV20, HT7, KI4, BL62 | De qi | 30 min | Once weekly for 8 weeks (8 session)/NR |
| Zhu (2016) [45] | TCM | ST36, SP10, CV4, SP6, BL23, BL19 | De qi | 30 min | Once for 5 days (5 session)/NR |
| Outcomes | No of Studies (Participants) | Certainty of the Evidence (GRADE) | Relative Effect (95% CI) | Absolute Effects (95% CI) |
|---|---|---|---|---|
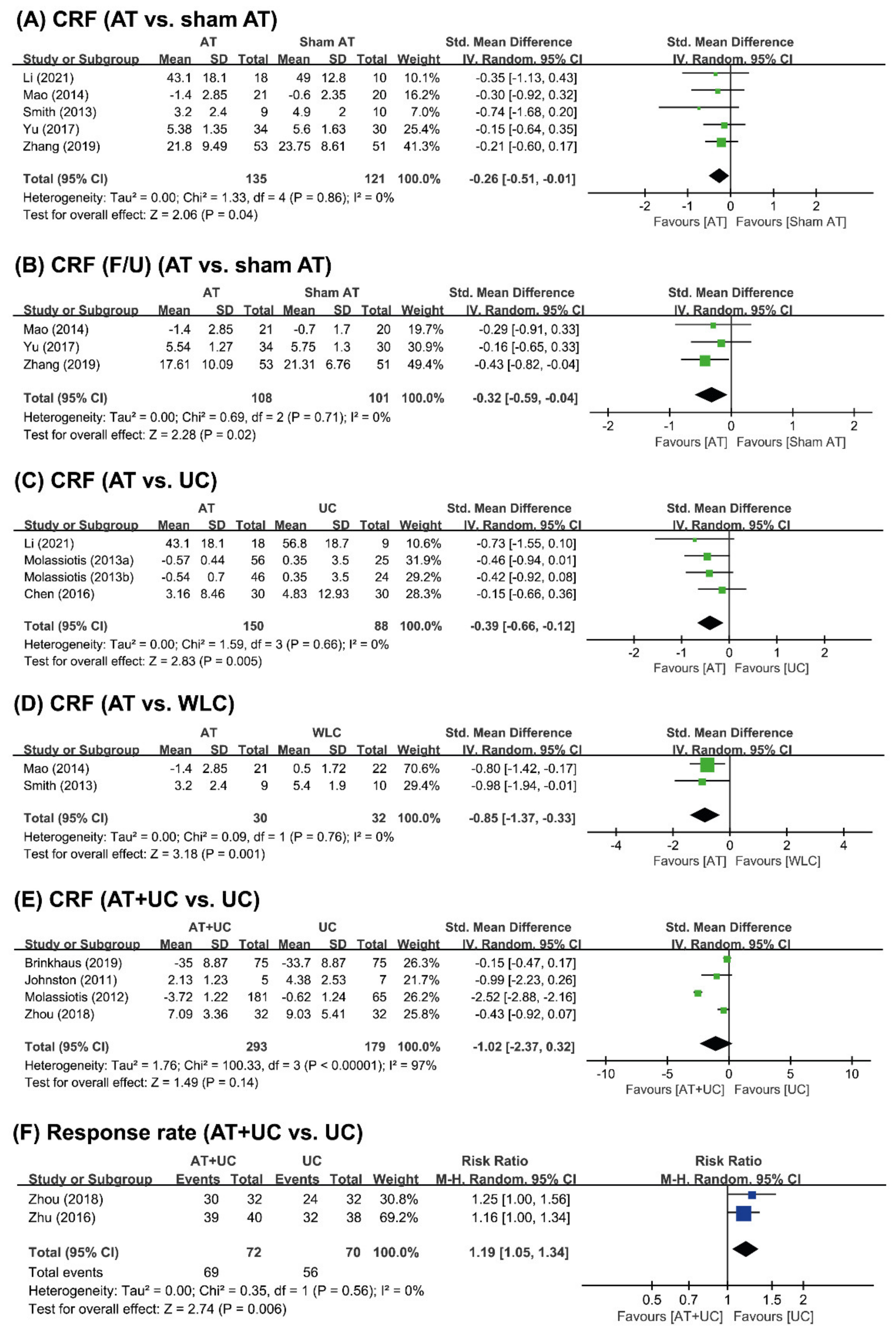
| CRF (AT vs. sham AT) | 5 (256) | ⨁⨁◯◯ LOW a,b | - | SMD 0.26 lower (0.51 lower to 0.01 lower) |
| CRF (F/U) (AT vs. sham AT) | 3 (209) | ⨁⨁◯◯ LOW a,b | - | SMD 0.32 lower (0.59 lower to 0.04 lower) |
| CRF (AT vs. UC) | 4 (238) | ⨁⨁◯◯ LOW a,b | - | SMD 0.39 lower (0.66 lower to 0.12 lower |
| CRF (AT vs. WLC) | 2 (62) | ⨁⨁◯◯ LOW b,c | - | SMD 0.85 lower (1.37 lower to 0.33 lower) |
| CRF (AT+UC vs. UC) | 4 (472) | ⨁⨁⨁◯ MODERATE a | - | SMD 1.02 lower (2.37 lower to 0.32 higher) |
| Response rate (AT+UC vs. UC) | 2 (142) | ⨁◯◯◯ VERY LOW b,d | RR 1.19 (1.05 to 1.34) | 152 more per 1000 (from 40 more to 272 more) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, T.-Y.; Ang, L.; Jun, J.H.; Alraek, T.; Birch, S.; Lu, W.; Lee, M.S. Acupuncture for Managing Cancer-Related Fatigue in Breast Cancer Patients: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 4419. https://doi.org/10.3390/cancers14184419
Choi T-Y, Ang L, Jun JH, Alraek T, Birch S, Lu W, Lee MS. Acupuncture for Managing Cancer-Related Fatigue in Breast Cancer Patients: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(18):4419. https://doi.org/10.3390/cancers14184419
Chicago/Turabian StyleChoi, Tae-Young, Lin Ang, Ji Hee Jun, Terje Alraek, Stephen Birch, Weidong Lu, and Myeong Soo Lee. 2022. "Acupuncture for Managing Cancer-Related Fatigue in Breast Cancer Patients: A Systematic Review and Meta-Analysis" Cancers 14, no. 18: 4419. https://doi.org/10.3390/cancers14184419
APA StyleChoi, T.-Y., Ang, L., Jun, J. H., Alraek, T., Birch, S., Lu, W., & Lee, M. S. (2022). Acupuncture for Managing Cancer-Related Fatigue in Breast Cancer Patients: A Systematic Review and Meta-Analysis. Cancers, 14(18), 4419. https://doi.org/10.3390/cancers14184419