

Integrative Approaches to the Treatment of Cancer



Abstract
Simple Summary
Abstract
1. Introduction
2. Addressing Modifiable Factors Associated with Cancer
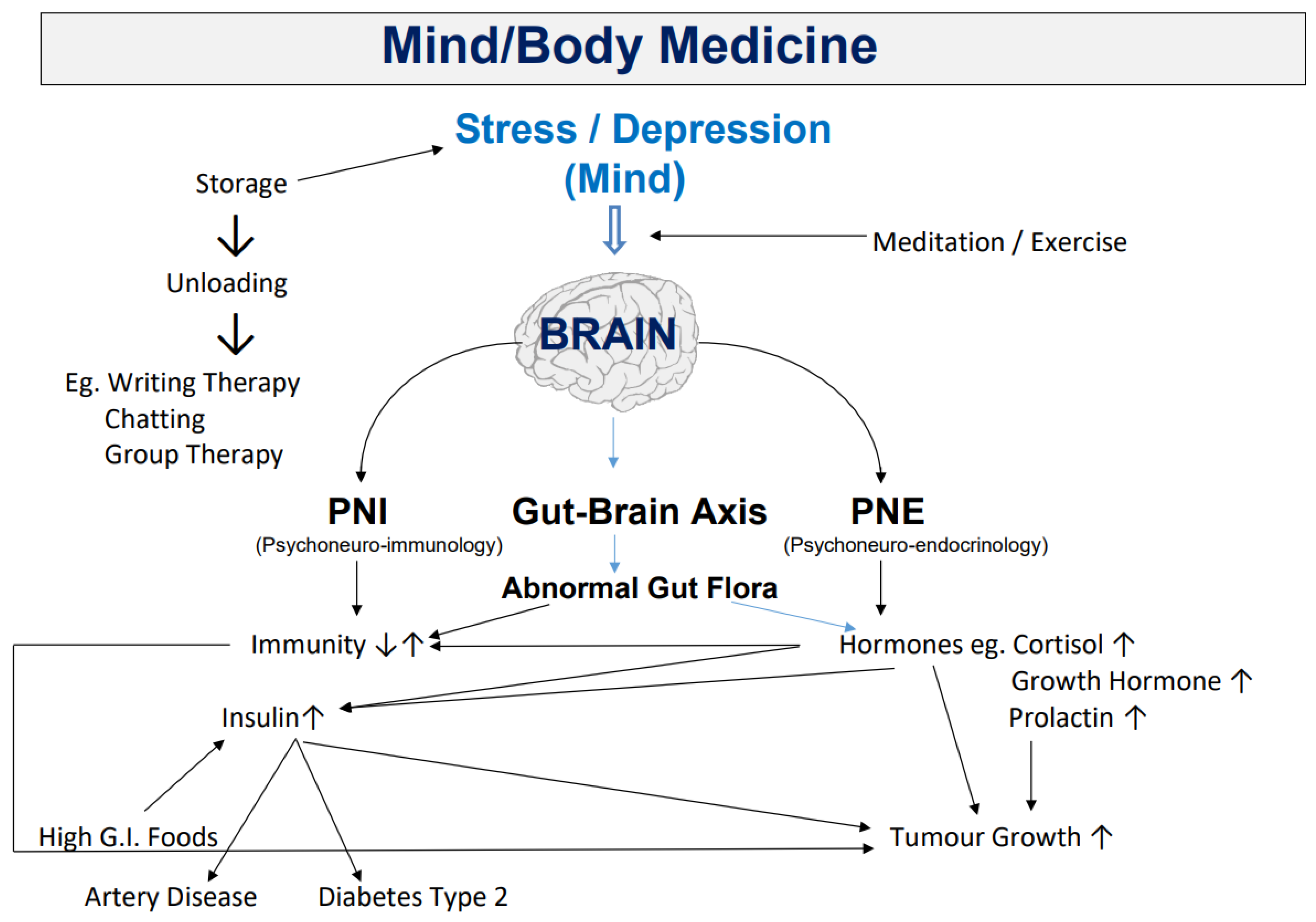
2.1. Stress
2.2. Disturbed Sleep
2.3. Diet and Nutrition
2.4. Inadequate Vitamin D
2.5. Inadequate Physical Activity
3. Complementary Medicines and Approaches in the Integrative Management of Cancer
3.1. Dietary Supplements
3.2. Intravenous Supplements
3.3. Herbal Medicine
3.4. Acupuncture
3.5. Massage
4. Repurposing of Current Drugs and Their Influence on Metabolic Blockade
5. Other Therapies for Cancer Treatment
6. Mitigating Risk in an Integrative Approach to Cancer Treatment
7. How to Practise Integrative Oncology
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- O’Brien, K. Cannabidiol (CBD) in Cancer Management. Cancers 2022, 14, 885. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, W.M.M.; et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef]
- Rarecells Diagnostics, France. Available online: https://www.rarecells.com/scientific-publications (accessed on 16 November 2022).
- Ried, K.; Eng, P.; Sali, A. Screening for Circulating Tumour Cells allows early detection of cancer and monitoring of treatment effectiveness: An observational study. Asian Pac. J. Cancer Prev. 2017, 18, 2275–2285. [Google Scholar] [CrossRef]
- Ried, K.; Tamanna, T.; Matthews, S.; Eng, P.; Sali, A. New Screening Test Improves Detection of Prostate Cancer Using Circulating Tumor Cells and Prostate-Specific Markers. Front. Oncol. 2020, 10, 582. [Google Scholar] [CrossRef]
- O’Brien, K.; Moore, A.; Percival-Smith, S.; Venkatraman, S.; Grubacevic, V.; Scoble, J.; Gilham, L.; Greenway, T.; Coghill, K.; Wale, J.; et al. An investigation into the usability of a drug-complementary medicines interactions database in a consumer group of women with breast cancer. Eur. J. Integr. Med. 2020, 33, 101004. [Google Scholar] [CrossRef]
- Ernst, E.; Cassileth, B.R. The prevalence of complementary/alternative medicine in cancer: A systematic review. Cancer 1998, 83, 777–782. [Google Scholar] [CrossRef]
- Kang, D.H.; McArdle, R.; Suh, Y. Changes in complementary and alternative medi-cine use across cancer treatment and relationship to stress, mood, and quality of life. J. Altern. Complement. Med. 2014, 20, 853–859. [Google Scholar] [CrossRef]
- Morris, K.T.; Johnson, N.; Homer, L.; Walts, D. A comparison of complementary therapy use between breast cancer patients and patients with other primary tumor sites. Am. J. Surg. 2000, 179, 407–411. [Google Scholar] [CrossRef]
- Richardson, M.A.; Sanders, T.; Palmer, J.L.; Greisinger, A.; Singletary, S.E. Complementary/alternative medicine use in a comprehensive cancer center and the implications for oncology. J. Clin. Oncol. 2000, 18, 2505–2514. [Google Scholar] [CrossRef]
- Wyatt, G.; Sikorskii, A.; Wills, C.E.; Su, H. Complementary and Alternative Medicine Use, Spending, and Quality of Life in Early Stage Breast Cancer. Nurs. Res. 2010, 59, 58–66. [Google Scholar] [CrossRef]
- O’Brien, K.; Sali, A. A Clinician’s Guide to Integrative Oncology. What You Should Be Talking about with Cancer Patients and Why; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Australian Health Policy Collaboration. The State of Self Care in Australia. Available online: https://www.chpaustralia.com.au/Self-Care/Research (accessed on 10 October 2022).
- Jentzsch, V.; Davis, J.A.A.; Djamgoz, M.B. Pancreatic cancer (PDAC): Introduction of evidence-based complementary measures into integrative clinical management. Cancers 2020, 12, 3096. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. The hallmarks of cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Kenny, P.A.; Nelson, C.M.; Bissell, M.J. The ecology of tumors: By perturbing the microenvironment, wounds and infection may be key to tumor development. Scientist 2006, 20, 30. [Google Scholar] [PubMed]
- Anderson, M.N.; Simon, M.C. The tumor microenvironment. Curr. Biol. 2020, 30, R921–R925. [Google Scholar] [CrossRef]
- Kim, Y.S.; Young, M.R.; Bobe, G.; Colburn, N.H.; Milner, J.A. Bioactive food components, inflammatory targets, and cancer prevention. Cancer Prev. Res. Phila. 2009, 2, 200–208. [Google Scholar] [CrossRef]
- Schäfer, M.; Werner, S. Cancer as an overhealing wound: An old hypothesis revisited. Nat. Rev. Mol. Cell Biol. 2008, 9, 628–638. [Google Scholar] [CrossRef]
- Baraldi, J.H.; Martyn, G.V.; Shurin, G.V.; Shurin, M.R. Tumor innervation: History, methodologies, and significance. Cancers 2022, 14, 1979. [Google Scholar] [CrossRef]
- Mravec, B. Neurobiology of cancer: Definition, historical overview, and clinical implications. Cancer Med. 2022, 11, 903–921. [Google Scholar] [CrossRef]
- Scheff, N.N.; Saloman, J.L. Neuroimmunology of cancer and associated symptomology. Immunol. Cell Biol. 2021, 99, 949–961. [Google Scholar] [CrossRef] [PubMed]
- Luo, W. Nasopharyngeal carcinoma ecology theory: Cancer a multidimensional spatiotermporal “unity of ecology and evolution” pathological ecosystem. Preprints 2022, 2022100226. [Google Scholar]
- O’Brien, K.A.; Xue, C.C. The theoretical framework of Chinese medicine. In A Comprehensive Guide to Chinese Medicine, 2nd ed.; Leung, P.-C., Xue, C.C., Cheng, Y.-C., Eds.; World Scientific Press: Hackensack, NJ, USA, 2016. [Google Scholar]
- Ayalew, M.; Deribe, B.; Duko, B.; Geleta, D.; Bogale, N.; Gemechu, L.; Gebretsadik, A.; Bedaso, A. Prevalence of depression and anxiety symptoms and their determinant factors among patients with cancer in southern Ethiopia: A cross-sectional study. BMJ Open 2022, 12, e051317. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, M.M.; Isometsä, E.T.; Hietanen, P.S.; Aro, H.M.; Lonnqvist, J.K. Mental disorders in cancer suicides. J. Affect. Disord. 1995, 36, 11–20. [Google Scholar] [CrossRef]
- Hong, J.S.; Tian, J. Prevalence of anxiety and depression and their risk factors in Chinese cancer patients. Support. Care Cancer 2013, 22, 453–459. [Google Scholar] [CrossRef]
- Lloyd-Williams, M. Depression- the hidden symptom in advanced cancer. J. Royal. Soc. Med. 2003, 96, 577–581. [Google Scholar]
- Naser, A.Y.; Hameed, A.N.; Mustafa, N.; Alwafi, H.; Dahmash, E.Z.; Alyami, H.S.; Khalil, H. Depression and Anxiety in Patients With Cancer: A Cross-Sectional Study. Front. Psychol. 2021, 12, 585534. [Google Scholar] [CrossRef]
- Gold, M.; Dunn, L.B.; Phoenix, B.; Paul, S.M.; Hamolsky, D.; Levine, J.D.; Miaskowski, C. Co-occurrence of anxiety and depressive symptoms following breast cancer surgery and its impact on quality of life. Eur. J. Oncol. Nurs. 2016, 20, 97–105. [Google Scholar] [CrossRef]
- Ho, R.T.H.; Kwan, T.T.C.; Cheung, I.K.M.; Chan, C.K.P.; Lo, P.H.Y.; Yip, P.S.F.; Luk, M.-Y.; Chan, C.L.W. Association of Fatigue with Perceived Stress in Chinese Women with Early Stage Breast Cancer Awaiting Adjuvant Radiotherapy. Stress Health 2015, 31, 214–221. [Google Scholar] [CrossRef]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Johnson, E.O.; Roth, T.; Breslau, N. The association of insomnia with anxiety orders and depression: Exploration of the direction of risk. J. Psychiatr. Res. 2006, 40, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H.; Reidel, B.W.; Bush, A.J. Epidemiology of Insomnia, Depression, and Anxiety. Sleep 2005, 28, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Saini, S.; Nautiyal, V.; Verma, S.; Gupta, M.; Kalra, B.; Ahmad, M. Cancer pain, anxiety, and depression in admitted patients at a tertiary care hospital: A prospective observational study. Indian J. Palliat. Care 2019, 25, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Xu, Y.; Luo, X.; Wen, Y.; Ding, K.; Xu, W.; Garg, S.; Yang, Y.; Sun, H. Alleviating excessive worries improves co-occurring depression and pain in adolescent and young adult cancer patients: A network approach. Neuropsychiatr. Dis. Treat. 2022, 18, 1843–1854. [Google Scholar] [CrossRef] [PubMed]
- Niedzwiedz, C.L.; Knifton, L.; Robb, K.A.; Katikireddi, S.V.; Smith, D.J. Depression and anxiety among people living with and beyond cancer: A growing clinical and research priority. BMC Cancer 2019, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fagundes, C.P.; Glaser, R.; Malarkey, W.B.; Kiecolt-Glaser, J.K. Childhood adversity and herpesvirus latency in breast cancer survivors. Health Psychol. 2013, 32, 337–344. [Google Scholar] [CrossRef]
- Lillberg, K.; Verkasalo, P.K.; Kaprio, J.; Teppo, L.; Helenius, H.; Koskenvuo, M. Stressful Life Events and Risk of Breast Cancer in 10,808 Women: A Cohort Study. Am. J. Epidemiol. 2003, 157, 415–423. [Google Scholar] [CrossRef]
- Chida, Y.; Hamer, M.; Wardle, J.; Steptoe, A. Do stress-related psychosocial factors contribute to cancer incidence and survival? Nat. Rev. Clin. Oncol. 2008, 5, 466–475. [Google Scholar] [CrossRef]
- Brown, K.W.; Levy, A.R.; Rosberger, Z.; Edgar, L. Psychological distress and cancer survival: A follow-up 10 years after diagnosis. Psychosom. Med. 2003, 65, 636–643. [Google Scholar] [CrossRef]
- Oerlemans, M.E.; Akker, M.V.D.; Schuurman, A.G.; Kellen, E.; Buntinx, F. A meta-analysis on depression and subsequent cancer risk. Clin. Pract. Epidemiol. Ment. Health 2007, 3, 29. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Guralnik, J.M.; Havlik, R.J.; Pahor, M.; Ferrucci, L.; Cerhan, J.; Wallace, R.B. Chronically Depressed Mood and Cancer Risk in Older Persons. JNCI J. Natl. Cancer Inst. 1998, 90, 1888–1893. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, D.; Giese-Davis, J. Depression and cancer: Mechanisms and disease progression. Biol. Psychiatr. 2003, 54, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Dai, S.; Mo, Y.; Wang, Y.; Xiang, B.; Liao, Q.; Zhou, M.; Li, X.; Li, Y.; Xiong, W.; Li, G.; et al. Chronic Stress Promotes Cancer Development. Front. Oncol. 2020, 10, 01492. [Google Scholar] [CrossRef] [PubMed]
- Lutgendorf, S.K.; Sood, A.K. Biobehavioural factors and cancer progression: Physiological pathways and mechanisms. Psychosom. Med. 2011, 73, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Lutgendorf, S.K.; DeGeest, K.; Sung, C.Y.; Arevalo, J.M.; Penedo, F.; Lucci, J.; Goodheart, M.; Lubaroff, D.; Farley, D.M.; Sood, A.K.; et al. Depression, social support, and beta-adrenergic transcription control in human ovarian cancer. Brain, Behav. Immun. 2009, 23, 176–183. [Google Scholar] [CrossRef]
- Kroenke, C.H.; Michael, Y.L.; Poole, E.M.; Kwan, M.L.; Nechuta, S.; Leas, E.; Caan, B.J.; Pierce, J.; Shu, X.-O.; Zheng, Y.; et al. Postdiagnosis social networks and breast cancer mortality in the After Breast Cancer Pooling Project. Cancer 2016, 123, 1228–1237. [Google Scholar] [CrossRef]
- Fawzy, F.I.; Canada, A.L.; Fawzy, N.W. Malignant melanoma: Effects of a brief, structured psychiatric intervention on survival and recurrence at 10-year follow-up. Arch. Gen. Psychiatr. 2003, 60, 100–103. [Google Scholar] [CrossRef][Green Version]
- Maunsell, E.; Brisson, J.; Deschěnes, L. Social support and survival among women with breast cancer. Cancer 1995, 76, 631–637. [Google Scholar] [CrossRef]
- Spiegel, K.; Bloom, J.R.; Kraemer, H.C.; Gotthiel, E. Effect of psycho-social treatment on survival of patients with metastatic breast cancer. Lancet 1989, 2, 888–891. [Google Scholar] [CrossRef]
- Schneider, R.H.; Alexander, C.N.; Staggers, F.; Rainforth, M.; Salerno, J.W.; Hartz, A.; Arndt, S.; Barnes, V.A.; Nidich, S.I. Long-Term Effects of Stress Reduction on Mortality in Persons ≥55 Years of Age With Systemic Hypertension. Am. J. Cardiol. 2005, 95, 1060–1064. [Google Scholar] [CrossRef]
- Meares, A. Regression of cancer after intensive meditation. Med. J. Aust. 1976, 2, 184. [Google Scholar] [CrossRef] [PubMed]
- Orme-Johnson, D. Medical care utilisation and the transcendental meditation program. Psychosom. Med. 1987, 49, 493–507. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Luo, T.; Xie, H.; Huang, M.; Cheng, A.S. Health benefits of qigong or tai chi for cancer patients: A systematic review and meta-analyses. Complement. Ther. Med. 2014, 22, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Fleishman, S.B.; Homel, P.; Chen, M.R.; Rosenwald, V.; Abolencia, V.; Gerber, J.; Nadesan, S. Beneficial effects of animal-assisted visits on quality of life during multimodal radiation-chemotherapy regimes. J. Community Support. Oncol. 2015, 13, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, M.; Trangeled, K.; Mambrini, A.; Tagliani, M.; Ferrarini, A.; Zanetti, L.; Tartarini, R.; Pacetti, P.; Cantore, M. Pet therapy effects on oncological day hospital patients undergoing chemotherapy treatment. Anticancer. Res. 2008, 27, 4301–4303. [Google Scholar]
- Bar-Sela, G.; Atid, L.; Danos, S.; Gabay, N.; Epelbaum, R. Art therapy improved depression and influenced fatigue levels in cancer patients on chemotherapy. Psychooncology 2007, 16, 980–984. [Google Scholar] [CrossRef]
- Lawson, L.M.; Williams, P.; Glennon, C.; Carithers, K.; Schnabel, E.; Andrejack, A.; Wright, N. Effect of art making on cancer-related symptoms of blood and marrow transplantation recipients. Oncol. Nurs. Forum. 2012, 39, E353–E360. [Google Scholar] [CrossRef]
- Nainis, N.; Paice, J.A.; Ratner, J.; Wirth, J.H.; Lai, J.; Shott, S. Relieving Symptoms in Cancer: Innovative Use of Art Therapy. J. Pain Symptom Manag. 2006, 31, 162–169. [Google Scholar] [CrossRef]
- Stuckey, H.L.; Nobel, J. The Connection Between Art, Healing, and Public Health: A Review of Current Literature. Am. J. Public Health 2010, 100, 254–263. [Google Scholar] [CrossRef]
- Thyme, K.E.; Sundin, E.C.; Wiberg, B.; Öster, I.; Åström, S.; Lindh, J. Individual brief art therapy can be helpful for women with breast cancer: A randomized controlled clinical study. Palliat. Support. Care 2009, 7, 87–95. [Google Scholar] [CrossRef]
- Bradt, J.; Dileo, C.; Magill, L.; Teague, A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 2016, 15, CD006911. [Google Scholar] [CrossRef]
- Bradt, J.; Dileo, C.; Myers-Coffman, K.; Biondo, J. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 2021, 10, CD006911. [Google Scholar] [PubMed]
- Morgan, N.P.; Graves, K.D.; Poggi, E.A.; Cheson, B.D. Implementing an Expressive Writing Study in a Cancer Clinic. Oncologist 2008, 13, 196–204. [Google Scholar] [CrossRef]
- Ornish, D.; Weidner, G.; Fair, W.R.; Marlin, R.; Pettengill, E.B.; Raisin, C.J.; Dunn-Emke, S.; Crutchfield, L.; Jacobs, F.N.; Barnard, R.J.; et al. Intensive lifestyle changes may affect the progression of prostate cancer. J. Urol. 2005, 174, 1065–1070. [Google Scholar] [CrossRef]
- Ornish, D.; Magbanua, M.J.M.; Weidner, G.; Weinberg, V.; Kemp, C.; Green, C.; Mattie, M.D.; Marlin, R.; Simko, J.; Shinohara, K.; et al. Changes in prostate gene expression in men undergoing an intensive nutrition and lifestyle intervention. Proc. Natl. Acad. Sci. USA 2008, 105, 8369–8374. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, L.; Ancoli-Israel, S. Sleep dysfunction in patients with cancer. Curr. Treat Options Neurol. 2007, 9, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, L.; Rissling, M.; Liu, L.; Ancoli-Israel, S. The symptom cluster of sleep, fatigue and depressive symptoms in breast cancer patients: Severity of the problem and treatment options. Drug Discov. Today Dis. Model. 2012, 8, 167–173. [Google Scholar] [CrossRef]
- Harrold, E.C.; Idris, A.F.; Keegan, N.M.; Corrigan, L.; Teo, M.Y.; O’Donnell, M.; Lim, S.T.; Duff, E.; O’Donnell, D.M.; Kennedy, M.J.; et al. Prevalence of Insomnia in an Oncology Patient Population: An Irish Tertiary Referral Center Experience. J. Natl. Compr. Cancer Netw. 2020, 18, 1623–1630. [Google Scholar] [CrossRef]
- Engstrom, C.A.; Strohl, R.A.; Rose, L.; Lewandowski, L.; Stefanek, M.E. Sleep alterations in cancer patients. Cancer Nurs. 1999, 22, 143–148. [Google Scholar] [CrossRef]
- Vachani, C. Sleep Problems (Insomnia) in the Cancer Patient. 2016. OncoLink. Available online: https://www.oncolink.org/support/side-effects/insomnia/sleep-problems-insomnia-in-the-cancer-patient (accessed on 4 January 2017).
- O’Donnell, J.F. Insomnia in cancer patients. Clin. Cornerstone 2004, 6, S6–S14. [Google Scholar] [CrossRef]
- National Cancer Institute. Sleep Problems in People with Cancer. Reviewed 12 August 2021. Available online: https://www.cancer.gov/about-cancer/treatment/side-effects/sleep-problems (accessed on 19 November 2022).
- Shi, T.; Min, M.; Sun, C.; Zhang, Y.; Liang, M.; Sun, Y. Does insomnia predict a high risk of cancer? A systematic review and meta-analysis of cohort studies. J. Sleep Res. 2019, 29, e12876. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.Y.; Huang, C.J.; Fan, Y.C.; Tsai, P.S. Insomnia but not hypnotics use associates with the risk of breast cancer: A popula- tion-based matched cohort study. J. Womens Health 2018, 27, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Sands, M.; Wactawski-Wende, J.; Song, Y.; Margolis, K.L. Sleep disturbance and incidence of thyroid cancer in postmenopausal women the Women’s Health Initiative. Am. J. Epidemiol. 2013, 177, 42–49. [Google Scholar] [CrossRef]
- Sen, A.; Opdahl, S.; Strand, L.B.; Vatten, L.J.; Laugsand, L.E.; Janszky, I. Insomnia and the Risk of Breast Cancer: The HUNT Study. Psychosom. Med. 2017, 79, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Sigurdardottir, L.; Valdimarsdottir, U.A.; Mucci, L.; Fall, K.; Rider, J.R.; Schernerhammer, E.S.; Czeisler, C.A.; Launer, L.; Harris, T.B.; Stampfer, M.J. Insomnia among elderly men and risk of prostate cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. 2012, 30, 78. [Google Scholar] [CrossRef]
- Gapstur, S.M.; Diver, W.R.; Stevens, V.L.; Carter, B.D.; Teras, L.R.; Jacobs, E.J. Work schedule, sleep duration, insomnia, and risk of fatal prostate cancer. Am. J. Prev. Med. 2014, 46, S26–S33. [Google Scholar] [CrossRef] [PubMed]
- Luojus, M.K.; Lehto, S.M.; Tolmunen, T.; Erkkilä, A.T.; Kauhanen, J. Sleep duration and incidence of lung cancer in age-ing men. BMC Public Health 2014, 14, 295–301. [Google Scholar] [CrossRef]
- Sturgeon, S.R.; Luisi, N.; Balasubramanian, R.; Reeves, K.W. Sleep duration and endometrial cancer risk. Cancer Causes Control. 2012, 23, 547–553. [Google Scholar] [CrossRef]
- Vogtmann, E.; Levitan, E.B.; Hale, L.; Shikany, J.M.; Shah, N.A.; Endeshaw, Y.; Lewis, C.E.; Manson, J.E.; Chlebowski, R.T. Association between sleep and breast cancer incidence among postmenopausal women in the Women’s Health Initiative. Sleep 2013, 36, 1437–1444. [Google Scholar] [CrossRef]
- Berisha, A.; Shutkind, K.; Borniger, J.C. Sleep Disruption and Cancer: Chicken or the Egg? Front. Neurosci. 2022, 16, 856235. [Google Scholar] [CrossRef]
- Hakim, F.; Wang, Y.; Zhang, S.X.; Zheng, J.; Yolcu, E.S.; Carreras, A.; Khalyfa, A.; Shirwan, H.; Almendros, I.; Gozal, D. Fragmented Sleep Accelerates Tumor Growth and Progression through Recruitment of Tumor-Associated Macrophages and TLR4 Signaling. Cancer Res. 2014, 74, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Möller-Levet, C.S.; Archer, S.N.; Bucca, G.; Laing, E.E.; Slak, A.; Kabiljo, R.; Lo, J.C.Y.; Santhi, N.; von Schantz, M.; Smith, C.P.; et al. Effects of insufficient sleep on circadian rhythmicity and expression amplitude of the human blood transcriptome. Proc. Natl. Acad. Sci. USA 2013, 110, E1132–E1141. [Google Scholar] [CrossRef] [PubMed]
- Haus, E.L.; Smolensky, M.H. Shift work and cancer risk: Potential mechanistic roles of circadian disruption, light at night, and sleep deprivation. Sleep Med. Rev. 2013, 17, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Mazzoccoli, G.; Tarquini, R.; Durfort, T.; Francois, J.C. Chronodisruption in lung cancer and possible therapeutic approaches. Biomed. Pharmacother. 2011, 65, 500–508. [Google Scholar] [CrossRef]
- Fu, L.; Lee, C.C. The circadian clock: Pacemaker and tumour suppressor. Nat. Rev. Cancer 2003, 3, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Cos, S.; González, A.; Martinez-Campa, C.; Mediavilla, M.D.; Alonso-González, C.; Sánchez-Barceló, E.J. Estrogen-signaling pathway: A link between breast cancer and melatonin oncostatic actions. Cancer Detect. Prev. 2006, 30, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Bovbjerg, D.H. Circadian disruption and cancer: Sleep and immune regulation. Brain Behav. Immun. 2003, 17, S48–S50. [Google Scholar] [CrossRef]
- Guarino, V.; Castellone, M.D.; Avilla, E.; Melillo, R.M. Thyroid cancer and inflammation. Mol. Cell. Endocrinol. 2010, 321, 94–102. [Google Scholar] [CrossRef]
- Buman, M.P.; Phillips, B.A.; Youngstedt, S.D.; Kline, C.E.; Hirshkowitz, M. Does nighttime exercise really disturb sleep? Results from the 2013 National Sleep Foundation Sleep in America Poll. Sleep Med. 2014, 15, 755–761. [Google Scholar] [CrossRef]
- Phelps, K. The Cancer Recovery Guide; MacMillan Publishers: Sydney, NSW, Australia, 2015. [Google Scholar]
- Anand, P.; Kunnumakara, A.B.; Sundarum, C.; Harikumar, K.B.; Tharakan, S.T.; Lai, O.S.; Sung, B.; Aggarwal, B.B. Cancer is a preventable disease that requires major lifestyle changes. Pharm. Res. 2008, 25, 2097–2116. [Google Scholar] [CrossRef]
- Campbell and Campbell. The China Study; Wakefield Press: Adelaide, SA, Australia, 2007. [Google Scholar]
- Calle, E.E.; Kaaks, R. Overweight, obesity and cancer: Epidemiological evidence and proposed mechanisms. Nat. Rev. Cancer 2004, 4, 579–591. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute Obesity and Cancer Risk Fact Sheet. Updated 5 April 2022. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/obesity-fact-sheet (accessed on 7 January 2022).
- Sung, H.; Siegel, R.L.; Torre, L.A.; Pearson-Stuttard, J.; Islami, F.; Fedewa, S.A.; Sauer, A.G.; Shuval, K.; Gapstur, S.M.; Jacobs, E.J.; et al. Global patterns in excess body weight and the associated cancer burden. CA Cancer J. Clin. 2018, 69, 88–112. [Google Scholar] [CrossRef] [PubMed]
- Benetou, V.; Trichopoulou, A.; Orfanos, P.; Naska, A.; Lagiou, P.; Boffetta, P.; Trichopoulos, D. Conformity to traditional Mediterranean diet and cancer incidence: The Greek EPIC cohort. Br. J. Cancer 2008, 99, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Casas, R.; Sacanella, E.; Estruch, R. The immune protective effect of the Mediterranean Diet against chronic low-grade inflammatory diseases. Endocr. Metab. Immune Disord. Drug Targets 2014, 14, 245–254. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed. Pharm. 2002, 56, 365–379. [Google Scholar] [CrossRef]
- Simopoulos, A.P. Evolutionary aspects of diet: The omega-6/omega-3 ratio and the brain. Mol. Neurobiol. 2011, 44, 203. [Google Scholar] [CrossRef]
- Wilkinson, D. Can Food Be Medicine Against Cancer? Inspiring Publishers: Canberra, Australia, 2015.
- Jing, K.; Wu, T.; Lim, K. Omega-3 polyunsaturated fatty acids and cancer. Anticancer. Agents. Med. Chem. 2013, 13, 1162–1167. [Google Scholar] [CrossRef]
- Escrich, E.; Moral, R.; Solanas, M. Olive oil, an essential component of the Mediterrean diet, and breast cancer. Public Health Nutr. 2011, 14, 2323–2332. [Google Scholar] [CrossRef]
- Carroll, K.L.; Frugé, A.D.; Heslin, M.J.; Lipke, E.A.; Greene, M.W. Diet as a risk factor for early-onset colorectal adenoma and carcinoma: A systematic review. Front. Nutr. 2022, 9, 896330. [Google Scholar] [CrossRef]
- Cohen, J.H.; Kristal, A.; Stanford, J.L. Fruit and vegetable intakes and prostate cancer risk. Gynecol. Oncol. 2000, 92, 61–68. [Google Scholar] [CrossRef]
- Kwan, M.L.; Weltzien, E.; Kushi, L.H.; Castillo, A.; Slattery, M.L.; Caan, B.J. Dietary patterns and breast cancer recurrence and survival among women with early-stage breast cancer. J. Clin. Oncol. 2009, 27, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-W.; Aronson, W.; Feedland, S.J. Nutrition, dietary interventions and prostate cancer: The latest evidence. BMC Med. 2015, 13, 3. [Google Scholar] [CrossRef]
- Rock, C.L.; Demark-Wahnefried, W. Nutrition and Survival After the Diagnosis of Breast Cancer: A Review of the Evidence. J. Clin. Oncol. 2002, 20, 3302–3316. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Flatt, S.W.; Natarajan, L.; Thomson, C.A.; Bardwell, W.A.; Newman, V.A.; Hollenbach, K.A.; Jones, L.; Caan, B.J.; Pierce, J.P. Plasma Carotenoids and Recurrence-Free Survival in Women with a History of Breast Cancer. J. Clin. Oncol. 2005, 23, 6631–6638. [Google Scholar] [CrossRef] [PubMed]
- Steinmetz, K.A.; Kushi, L.H.; Bostick, R.M.; Folsum, A.R.; Potter, J.D. Vegetables, fruit, and colon cancer in the lowa Women’s Health Study. Am. J. Epidemiol. 1994, 139, 1–15. [Google Scholar] [CrossRef]
- Markellos, C.; Ourailidou, M.-E.; Gavriatopoulou, M.; Halvatsiotis, P.; Sergentanis, T.N.; Psaltopoulou, T. Olive oil intake and cancer risk: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0261649. [Google Scholar] [CrossRef]
- Roberts, D.C.; Chidambaram, S.; Kinross, J.M. The role of the colonic microbiota and bile acids in colorectal cancer. Curr. Opin. Gastroenterol. 2022, 38, 179–188. [Google Scholar] [CrossRef]
- Hajishafiee, M.; Saneei, P.; Benisi-Kohansal, S.; Esmaillzadeh, A. Cereal fibre intake and risk of mortality from all causes, CVD, cancer and inflammatory diseases: A systematic review and meta-analysis of prospective cohort studies. Br. J. Nutr. 2016, 116, 343–352. [Google Scholar] [CrossRef]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 1017. [Google Scholar] [CrossRef]
- Shanahan, F. Fiber man meets microbial man. Am. J. Clin. Nutr. 2014, 101, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Chassaing, B.; Singh, V.; Pellizzon, M.; Ricci, M.; Fythe, M.D.; Kumar, M.V.; Gewirtz, A.T. Fiber-Mediated Nourishment of Gut Microbiota Protects against Diet-Induced Obesity by Restoring IL-22-Mediated Colonic Health. Cell Host Microbe. 2017, 23, 41–53.e4. [Google Scholar] [CrossRef] [PubMed]
- Bauer, S.R.; Hankinson, S.E.; Bertone-Johnstone, E.R.; Ding, E.L. Plasma vitamin D levels, menopause, and risk of breast cancer: Dose-response meta-analysis of prospective studies. Med. Baltim. 2013, 92, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Boniol, M.; Haukka, J.; Byrnes, G.; Cox, B.; Sneyd, M.J.; Mullie, P.; Autier, P. Meta-analysis of observational studies of serum 25-hydroxyvitamin D levels and colorectal, breast and prostate cancer and colorectal adenoma. Int. J. Cancer 2011, 128, 1414–1424. [Google Scholar] [CrossRef]
- Gorham, E.D.; Garland, C.F.; Garland, F.C.; Grant, W.; Mohr, S.B.; Lipkin, M.; Newmark, H.L.; Giovannucci, E.; Wei, M.; Holick, M. Optimal Vitamin D Status for Colorectal Cancer Prevention: A Quantitative Meta Analysis. Am. J. Prev. Med. 2007, 32, 210–216. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, P.; Wang, F.; Yang, J.; Liu, Z.; Qin, H. Association Between Vitamin D and Risk of Colorectal Cancer: A Systematic Review of Prospective Studies. J. Clin. Oncol. 2011, 29, 3775–3782. [Google Scholar] [CrossRef]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Wetterslev, J.; Simonetti, R.G.; Bjelakovic, M.; Gluud, C. Vitamin D supplementation for prevention of mortality in adults. Cochrane Database Syst. Rev. 2014, CD007470. [Google Scholar] [CrossRef]
- Kim, Y.; Je, Y. Vitamin D intake, blood 25(OH)D levels, and breast cancer risk or mortality: A meta-analysis. Br. J. Cancer 2014, 110, 2772–2784. [Google Scholar] [CrossRef]
- Mohr, S.B.; Gorham, E.D.; Kim, J.; Hofflich, H.; Cuomo, R.E.; Garland, C.F. Could vitamin D sufficiency improve the survival of colorectal cancer patients? J. Steroid. Biochem. 2015, 148, 239–244. [Google Scholar] [CrossRef]
- Mohr, S.B.; Gorham, E.D.; Kim, J.; Hofflich, H.; Garland, C.F. Meta-analysis of vitamin D sufficiency for improving survival of patients with breast cancer. Anticancer Res. 2014, 34, 1163–1166. [Google Scholar]
- Zgaga, L.; Theodoratou, E.; Farrington, S.M.; Din, F.V.; Ooi, L.Y.; Glodzik, D.; Johnston, S.; Tenesa, A.; Campbell, H.; Dunlop, M.G. Plasma Vitamin D Concentration Influences Survival Outcome After a Diagnosis of Colorectal Cancer. J. Clin. Oncol. 2014, 32, 2430–2439. [Google Scholar] [CrossRef] [PubMed]
- Moukayed, M.; Grant, W.B. Molecular link between vitamin D and cancer prevention. Nutrients 2013, 5, 3993–4021. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D Metabolism, mechanisms of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Díaz, G.D.; Paraskeva, C.; Thomas, M.G.; Binderup, L.; Hague, A. Apoptosis is induced by the active metabolite of vitamin D3 and its analogue EB1089 in colorectal adenoma and carcinoma cells: Possible implications for prevention and therapy. Cancer Res. 2000, 60, 2304–2312. [Google Scholar]
- Scaglione-Sewell, B.A.; Bissonnette, M.; Skarosi, S.; Abraham, C.; Brasitus, T.A. A vitamin D3 analog induces a G1-phase arrest in CaCo-2 cells by inhibiting cdk2 and cdk6: Roles of cyclin E, p21Waf1, and p27Kip1. Endocrinology 2000, 141, 3931–3939. [Google Scholar] [CrossRef]
- Chandler, P.D.; Chen, W.Y.; Ajala, O.N.; Hazra, A.; Cook, N.; Bubes, V.; Lee, I.-M.; Giovannucci, G.L.; Willett, W.; Buring, J.E. Effect of Vitamin D3 Supplements on development of advanced cancer: A secondary analysis of the VITAL randomized clinical trial. JAMA Netw Open 2020, 3, e2025850. [Google Scholar] [CrossRef]
- Urashima, M.; Ohdaira, H.; Akutsu, T.; Odaira, H.; Suzuki, Y.; Urashima, M. Effect of vitamin D supplementation on relapse-free survival among patients with digestive tract cancers: The AMATERASU randomized clinical trial. JAMA 2019, 321, 1361–1369. [Google Scholar] [CrossRef]
- Ng, K.; Nimeiri, H.S.; McCleary, N.J.; Abrams, T.A.; Yurgelun, M.B.; Cleary, J.M.; Rubinson, D.A.; Schrag, D.; Miksad, R.; Bullock, A.J.; et al. Effect of high-dose vs. standard-dose vitamin D3 supplementation on progression-free survival among patients with advanced or metastatic colorectal cancer: The SUNSHINE randomized clinical trial. JAMA 2019, 321, 1370–1379. [Google Scholar] [CrossRef]
- Keum, N.; Giovannucci, E. Vitamin D supplements and cancer incidence and mortality: A meta-analysis. Br. J. Cancer 2014, 111, 976–980. [Google Scholar] [CrossRef]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Cristen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef]
- Shen, D.; Mao, W.; Liu, T. Sedentary behavior and incident cancer: A meta-analysis of prospective studies. PLoS ONE 2014, 9, e105709. [Google Scholar] [CrossRef] [PubMed]
- Lynch, B. Sedentary behaviour and cancer: A systematic review of the literature and proposed biological mechanisms. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2691–2709. [Google Scholar] [CrossRef] [PubMed]
- Cong, Y.J.; Gan, Y.; Sun, H.L.; Deng, J.; Cao, S.Y.; Xu, X.; Lu, Z.X. Association of sedentary behaviour with colon and rectal cancer: A meta-analysis of observational studies. Br. J. Cancer 2014, 110, 817–826. [Google Scholar] [CrossRef]
- Meyerhardt, J.A.; Giovannucci, E.L.; Holmes, M.D.; Chan, A.T.; Chan, J.A.; Colditz, G.A.; Fuchs, G.S. Physical activity and survival after colorectal cancer diagnosis. J. Clin. Oncol. 2006, 24, 3527–3534. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.E.; Chang-Claude, J.; Vrieling, A.; Seibold, P.; Heinz, J.; Obi, N.; Flesch-Janys, D.; Steindorf, K. Association of pre-diagnosis physical activity with recurrence and mortality among women with breast cancer. Int. J. Cancer 2013, 133, 1431–1441. [Google Scholar] [CrossRef]
- Hamer, M.; Stamatakis, E.; Saxton, J.M. The impact of physical activity on all-cause mortality in men and women after a cancer diagnosis. Cancer Causes Control. 2008, 20, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical activity, obesity and sedentary behavior in cancer etiology: Epidemiologic evidence and biologic mechanisms. Mol. Oncol. 2020, 15, 790–800. [Google Scholar] [CrossRef]
- Birks, S.; Peeters, A.; Backholer, K.; O’Brien, P.; Brown, W. A systematic review of the impact of weight loss on cancer incidence and mortality. Obes. Rev. 2012, 13, 868–891. [Google Scholar] [CrossRef]
- Jurdana, M. Physical activity and cancer risk. Actual knowledge and possible biological mechanisms. Radiol. Oncol. 2021, 55, 7–17. [Google Scholar] [CrossRef]
- Lahart, I.; Metsios, G.S.; Nevill, A.; Carmichael, A.R. Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies. Acta Oncol. 2015, 54, 635–654. [Google Scholar] [CrossRef]
- Moore, S.C.; Lee, I.-M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; de Gonzalez, A.B.; Hartge, P.; et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Swift DLMcGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The effects of exercise and physical activity on weight loss and maintenance. Prog. Cardiovasc. Dis. 2018, 61, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Metsios, G.S.; Moe, R.H.; Kitas, G.D. Exercise and inflammation. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101504. [Google Scholar] [CrossRef]
- Zhong, D.; Li, Y.; Huang, Y.; Hong, X.; Li, J.; Jin, R. Molecular Mechanisms of Exercise on Cancer: A Bibliometrics Study and Visualization Analysis via CiteSpace. Front. Mol. Biosci. 2022, 8, 797902. [Google Scholar] [CrossRef] [PubMed]
- Dimeo, F.C. Effects of exercise on cancer-related fatigue. Cancer Relat. Fatigue New Dir. Res. 2001, 92, 1689–1693. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.; Matthews, C.; Ligibel, J.; Gerber, L.; et al. Exercise guidelines for cancer survivors: Consensus statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef]
- Holmes, M.D.; Chen, W.Y.; Feskanich, D.; Kroenke, C.H.; Colditz, G.A. Physical Activity and Survival After Breast Cancer Diagnosis. Obstet. Gynecol. Surv. 2005, 60, 798–800. [Google Scholar] [CrossRef][Green Version]
- Lee, I.-M.; Wolin, K.Y.; Freeman, S.E.; Sattlemair, J.; Sesso, H.D.; Sattelmair, J. Physical activity and survival after cancer diagnosis in men. J. Phys. Act. Health 2014, 11, 85–90. [Google Scholar] [CrossRef]
- Kim, J.-S.; Wilson, R.L.; Taaffe, D.R.; Galvão, D.A.; Gray, E.; Newton, R.U. Myokine expression and tumor-suppressive effect of serum after 12 wk of exercise in prostate cancer patients on ADT. Med. Sci. Sports Exerc. 2022, 54, 197–205. [Google Scholar] [CrossRef]
- Kim, J.-S.; Galvao, D.A.; Newton, R.U.; Gray, E.; Taaffe, D.R. Exercise-induced myokines and their effect on prostate cancer. Nat. Rev. Urol. 2021, 18, 519–542. [Google Scholar] [CrossRef]
- Hayes, S.C.; Spence, R.A.; Galvao, D.; Newton, R.U. Australian Association for Exercise and Sport Science position stand: Optimising cancer outcomes through exercise. J. Sci. Med. Sport 2009, 12, 428–434. [Google Scholar] [CrossRef]
- Wang, Q.; Zhou, W. Roles and molecular mechanisms of physical exercise in cancer prevention and treatment. J. Sport Health Sci. 2021, 10, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Maggini, S.; Wintergerst, E.S.; Beveridge, S.; Hornig, D.H. Selected vitamins and trace elements support immune function by strengthening epithelial barriers and cellular and humoral immune responses. Br. J. Nutr. 2007, 98, S29–S35. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Prabhu, K.S.; Mastro, A.M. Review: Is selenium a potential treatment for cancer metastasis? Nutrients 2013, 5, 1149–1168. [Google Scholar] [CrossRef] [PubMed]
- Perlmutter, D. Brain Maker; Yellow Kite Books: London, UK, 2015. [Google Scholar]
- Schwabe, R.F.; Jobin, C. The microbiome and cancer. Nat. Rev. Cancer 2013, 13, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Al-Qadami, G.; Van Sebille, Y.; Bowen, J.; Wardill, H. Oral-gut microbiome axis in the pathogenesis of cancer treatment-induced oral mucositis. Front. Oral Health 2022, 3, 881949. [Google Scholar] [CrossRef] [PubMed]
- Deleemans, J.M.; Chleilat, F.; Reimer, R.A.; Henning, J.-W.; Baydoun, M.; Piedalue, K.-A.; McLennan, A.; Carlson, L.E. The chemo-gut study: Investigating the long-term effects of chemotherapy on gut microbiota, metabolic, immune, psychological and cognitive parameters in young adult Cancer survivors; study protocol. BMC Cancer 2019, 19, 1243. [Google Scholar] [CrossRef]
- Starr, P. Oral Nicotinamide Prevents Common Skin Cancers in High-Risk Patients, Reduces Costs. Am. Health Drug Benefits 2015, 8, 13–14. [Google Scholar]
- Dettman, I.; Meakin, C.; Allen, R. Co-infusing Glutathione and Vitamin C during cancer treatment: A reply. ACNEM J. 2012, 31, 8–11. [Google Scholar]
- Mikirova, N.; Jackson, J.; Riordan, N. The effect of high dose IV Vitamin C on plasma antioxidant capacity and level of oxidative stress in cancer patients and healthy subjects. Orthomol. Med. 2007, 22, 153–160. [Google Scholar]
- Shiota, M.; Yokomizo, A.; Naito, S. Oxidative stress and androgen receptor signaling in the development and progression of castration-resistant prostate cancer. Free. Radic. Biol. Med. 2011, 51, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- Shiota, M.; Song, Y.; Takeuchi, A.; Yokomizo, A.; Kashiwagi, E.; Kuroiwa, K.; Tatsugami, K.; Uchiumi, T.; Oda, Y.; Naito, S. Antioxidant therapy alleviates oxidative stress by androgen deprivation and prevents conversion from androgen dependent to castration resistant prostate cancer. J. Urol. 2012, 187, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Rhodes, C.J.; Moncol, J.; Izakovic, M.; Mazur, M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem. Biol. Interact. 2006, 160, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Wybieralska, E.; Koza, M.; Sroka, J.; Czyż, J.; Madeja, Z. Ascorbic acid inhibits the migration of walker 256 carcinosarcoma cells. Cell. Mol. Biol. Lett. 2008, 13, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.J.; Miranda-Massari, J.R.; Mora, E.M.; Guzman, A.; Riordan, N.H.; Casciari, J.J.; Jackson, J.A.; Roman-Franco, A. Orthomolecular oncology review: Ascorbic acid and cancer 25 years later. Integr. Cancer Ther. 2005, 4, 32–44. [Google Scholar] [CrossRef]
- Block, K.I.; Koch, A.C.; Mead, M.N.; Tothy, P.K.; Newman, R.A.; Gyllenhaal, C. Impact of antioxidant supplementation on chemotherapeutic efficacy: A systematic review of the evidence from randomized controlled trials. Cancer Treat. Rev. 2007, 33, 407–418. [Google Scholar] [CrossRef]
- Block, K.I.; Koch, A.C.; Mead, M.N.; Tothy, P.K.; Newman, R.A.; Gyllenhaal, C. Impact of antioxidant supplementation on chemotherapeutic toxicity: A systematic review of the evidence from randomized controlled trials. Int. J. Cancer 2008, 123, 1227–1239. [Google Scholar] [CrossRef]
- Bohm, S.; Oriana, S.; Spatti, G.; Di Re, F.; Breasciani, g.; Pirovano, C.; Grosso, I.; Martini, C.; Caraceni, A.; Pilotti, S.; et al. Dose intensification of platinum compounds with glutathione protection as induction chemotherapy for advanced ovarian cancer. Oncology 1999, 57, 115–120. [Google Scholar] [CrossRef]
- Cascinu, S.; Catalano, V.; Cordella, L.; Labianca, R.; Giordani, P.; Baldelli, A.M.; Beretta, G.D.; Ubiali, E.; Catalano, G. Neuroprotective effect of reduced glutathione on oxaliplatin-based chemotherapy in advanced colorectal cancer: A randomized, double-blind, placebo-controlled trial. J. Clin. Oncol. 2002, 20, 3478–3483. [Google Scholar] [CrossRef]
- Böttger, F.; Vallés-Martí, A.; Cahn, L.; Jimenez, C.R. High-dose intravenous vitamin C, a promising multi-targeting agent in the treatment of cancer. J. Exp. Clin. Cancer Res. 2021, 40, 343. [Google Scholar] [CrossRef]
- González, M.J.; Rosario-Pérez, G.; Guzmán, A.M.; Miranda-Massari, J.R.; Duconge, J.; Lavergne, J.; Fernandez, N.; Ortiz, N.; Quintero, A.; Mikirova, N.; et al. Mitochondria, Energy and Cancer: The Relationship with Ascorbic Acid. J. Orthomol. Med. Off. J. Acad. Orthomol. Med. 2010, 25, 29–38. [Google Scholar]
- Vollbracht, C.; Schneider, B.; Leendert, V.; Weiss, G.; Auerbach, L.; Beuth, J. Intravenous vitamin C administration improves quality of life in breast cancer patients during chemo-/radiation therapy and aftercare: Results of a retrospective, multicentre, epidemiological cohort study in Germany. In Vivo 2011, 25, 983–990. [Google Scholar]
- Travica, N.; Ried, K.; Hudson, I.; Scholey, A.; Pipingas, A.; Sali, A. The effects of surgery on plasma/serum vitamin C concentrations: A systematic review and meta-analysis. Br. J. Nutr. 2020, 127, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, J.; Prasad, S.; Aggarwal, B.B. Curcumin and Cancer Cells: How Many Ways Can Curry Kill Tumor Cells Selectively? AAPS J. 2009, 11, 495–510. [Google Scholar] [CrossRef] [PubMed]
- Wilken, R.; Veena, M.S.; Wang, M.B.; Srivatsan, E.S. Curcumin: A review of anti-cancer properties and therapeutic activity in head and neck squamous cell carcinoma. Mol. Cancer 2011, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, L.; Wang, H.; Ma, J.-X.; Sun, J.-Z. Curcumin inhibits lung cancer progression and metastasis through induction of FOXO1. Tumor. Biol. 2014, 35, 111. [Google Scholar] [CrossRef]
- Zhou, D.Y.; Ding, N.; Du, Z.Y.; Cui, X.X.; Wang, H.; Wei, X.C.; Conney, A.H.; Zhang, K.; Zheng, X. Curcumin analogues with high activity for inhibiting human prostate cancer cell growth and androgen receptor activation. Mol. Med. Rep. 2014, 10, 1315–1322. [Google Scholar] [CrossRef] [PubMed]
- Dorai, T.; Diouri, J.; O’Shea, O.; Doty, S.B. Curcumin inhibits prostate cancer bone metastasis by up-regulating bone morphogenic protein-7 in vivo. J. Cancer Ther. 2014, 5, 369–386. [Google Scholar] [CrossRef]
- Du, Y.; Long, Q.; Zhang, L.; Shi, Y.; Liu, X.; Li, X.; Guan, B.; Tian, Y.; Wang, X.; Li, L.; et al. Curcumin inhibits cancer-associated fibroblast-driven prostate cancer invasion through MAOA/mTOR/HIF-1α signaling. Int. J. Oncol. 2015, 47, 2064–2072. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Shishodia, S.; Takada, Y.; Banerjee, S.; Newman, R.A.; Buesos-Ramos, C.E.; Price, J.E. Curcumin suppresses the paclitaxel-induced nuclear factor-kappaB pathway in breast cancer cells and inhibits lung metastasis of human breast cancer in nude mice. Clin. Cancer Res. 2005, 11, 7490–7498. [Google Scholar] [CrossRef]
- Huang, M.T.; Wang, Z.Y.; Georgiadis, C.A.; Laskin, J.D.; Conney, A.H. Inhibitory effects of curcumin on tumor initiation by benzo[a]pyrene and 7, 12 dimethylbenz[a]anthracene. Carcinogenesis 1992, 13, 2183–2186. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Drummond, P.D. Efficacy of curcumin, and a saffron/curcumin combination for the treatment of major depression: A randomised, double-blind, placebo-controlled study. J. Affect. Disord. 2017, 207, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Maes, M.; Maker, G.L.; Hood, S.D.; Drummond, P.D. Curcumin for the treatment of major depression: A randomised, double-blind, placebo controlled study. J. Affect. Disord. 2014, 167, 368–375. [Google Scholar] [CrossRef]
- Hao, E.; Mukhopadhyay, P.; Cao, Z.; Erdélyi, K.; Holovac, E.; Liaudet, L.; Lee, W.-S.; Haskó, G.; Mechoulam, R.; Pacher, P. Cannabidiol Protects against Doxorubicin-Induced Cardiomyopathy by Modulating Mitochondrial Function and Biogenesis. Mol. Med. 2015, 21, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.; Mukhopadhyay, P.; Rajesh, M.; Patel, V.; Mukhopadhyay, B.; Gao, B.; Haskó, G.; Pacher, P. Cannabidiol Attenuates Cisplatin-Induced Nephrotoxicity by Decreasing Oxidative/Nitrosative Stress, Inflammation, and Cell Death. J. Pharmacol. Exp. Ther. 2008, 328, 708–714. [Google Scholar] [CrossRef]
- Ward, S.J.; McAllister, S.D.; Kawamura, R.; Murase, Y.; Neelakantan, H.; Walker, E.A. Cannabidiol inhibits paclitaxel-induced neuropathic pain through 5-HT 1A receptors without diminishing nervous system function or chemotherapy efficacy. J. Cereb. Blood Flow. Metab. 2014, 171, 636–645. [Google Scholar] [CrossRef]
- Taha, T.; Meiri, D.; Talhamy, S.; Wollner, M.; Peer, A.; Bar-Sela, G. Cannabis Impacts Tumor Response Rate to Nivolumab in Patients with Advanced Malignancies. Oncol. 2019, 24, 549–554. [Google Scholar] [CrossRef]
- Cao, Y.; Xu, X.; Liu, S.; Huang, L.; Gu, J. Ganoderma: A cancer immunotherapy review. Front. Pharmacol. 2018, 9, 1217. [Google Scholar] [CrossRef]
- Wachtel-Galor, S.; Yuen, J.; Buswell, J.A.; Benzie, I.F.F. Ganoderma lucidum (Lingzhi or Reishi): A medicinal mushroom. In Herbal Medicine: Biomolecular and Clinical Aspects, 2nd ed.; CRC Press: Boca Raton, FL, USA; Taylor & Francis: Boca Raton, FL, USA, 2011. [Google Scholar]
- Liu, J.; Shimizu, K.; Konishi, F.; Noda, K.; Kumamoto, S.; Kurashiki, K.; Kondo, R. Anti-androgenic activities of the triterpenoids fraction of Ganoderma lucidum. Food Chem. 2007, 100, 1691–1696. [Google Scholar] [CrossRef]
- Liu, J.; Shimizu, K.; Konishi, F.; Kumamoto, S.; Kondo, R. The anti-androgen effect of ganoderol B isolated from the fruiting body of Ganoderma lucidum. Bioorganic Med. Chem. 2007, 15, 4966–4972. [Google Scholar] [CrossRef]
- Gao, Y.; Zhou, S.; Jiang, W.; Huang, M.; Dai, X. Effects of ganopoly (a Ganoderma lucidum polysaccharide extract) on the immune functions in advanced-stage cancer patients. Immunol. Invest. 2003, 32, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Beguerie, J.R.; Sze, D.M.-Y.; Chan, G.C. Ganoderma lucidum (Reishi mushroom) for cancer treatment. Cochrane Database Syst. Rev. 2012, CD007731. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Li, L.; Li, Y.; Wang, J.; Wang, Q. Chinese Herbal Medicine as an Adjunctive Therapy for Breast Cancer: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2016, 2016, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; So, T.-H.; Tang, G.; Tan, H.-Y.; Wang, N.; Ng, B.F.L.; Chan, C.K.W.; Yu, E.C.-L.; Feng, Y. Chinese herbal medicine for reducing chemotherapy-associated side-effects in breast cancer patients: A systematic review and meta-analysis. Front. Oncol. 2020, 10, 599073. [Google Scholar] [CrossRef]
- O’Brien, K.; Weber, D. Insomnia in Chinese medicine: The Heart of the Matter. JACM 2016, 22, 684–694. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.; O’Brien, K. Cancer and Cancer-Related Fatigue and the Interrelationships With Depression, Stress, and Inflammation. J. Evid. Based Integr. Med. 2016, 22, 502–512. [Google Scholar] [CrossRef]
- Lu, W.; Dean-Clower, E.; Doherty-Gilman, A.; Rosenthal, D.S. The value of acupuncture in cancer care. Hematol. Oncol. Clin. North Am. 2008, 22, 631–648. [Google Scholar] [CrossRef]
- Meng, Z.; Barcia, M.K.; Hu, C.; Chiang, J.; Chambers, M.; Rosenthal, D.I.; Peng, H.; Zhang, Y.; Zhao, Q.; Zhao, G.; et al. Randomized controlled trial of acupuncture for prevention of radiation-induced xerostomia among patients with nasopharyngeal carcinoma. Cancer 2012, 118, 3337–3344. [Google Scholar] [CrossRef]
- Shen, J.; Wenger, N.; Glaspy, J.; Hays, R.D.; Albert, P.S.; Choi, C.; Shekelle, P.G. Electroacupuncture for control of myeloablative chemotherapy-induced emesis: A randomized controlled trial. JAMA 2000, 284, 2755–2761. [Google Scholar] [CrossRef]
- Tas, D.; Uncu, D.; Sendur, M.A.; Koca, N.; Zengin, N. Acupuncture as a complementary treatment for cancer patients receiving chemotherapy. Asian Pac. J. Cancer Prev. 2014, 15, 3139–3144. [Google Scholar] [CrossRef]
- Yang, J.; Wahner-Roedler, D.L.; Zhou, X.A.; Johnson, L.; Do, A.; Pachman, D.R.; Chon, T.Y.; Salinas, M.; Millstine, D.A.; Bauer, B. Acupuncture for palliative cancer pain management: Systematic review. BMJ Support. Palliat. Care 2021, 11, 264–270. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, L.; Li, H.; Hu, Y.; Tian, L. Effects of acupuncture on cancer-related fatigue: A meta-analysis. Support. Care Cancer 2018, 26, 415–425. [Google Scholar] [CrossRef] [PubMed]
- Cancer Council NSW. Massage. Available online: https://www.cancercouncil.com.au/cancer-information/living-well/complementary-therapies/body-based-practices/massage/ (accessed on 12 October 2022).
- Campeau, M.P.; Gaboriault, R.; Drapeau, M.; Nguyen, T.V.; Roy, I.; Fortin, B.; Marois, M.; Nguyen-Tan, P.F. The impact of massage therapy on anxiety levels in patients undergoing radiation therapy: A randomized controlled trial. J Soc Integr. Oncol. 2007, 5, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Khiewkhern, S.; Promthet, S.; Sukprasert, A.; Eunhpinitpong, W.; Bradshaw, P. Effectiveness of Aromatherapy with Light Thai Massage for Cellular Immunity Improvement in Colorectal Cancer Patients Receiving Chemotherapy. Asian Pac. J. Cancer Prev. 2013, 14, 3903–3907. [Google Scholar] [CrossRef] [PubMed]
- Sagar, S.; Dryden, T.; Wong, R.K. Massage Therapy for Cancer Patients: A Reciprocal Relationship between Body and Mind. Curr. Oncol. 2007, 14, 45–56. [Google Scholar] [CrossRef]
- McIntyre, J.; Conroy, S.; Avery, A.; Corns, H.; Choonara, I. Unlicensed and off label prescribing of drugs in general practice. Arch. Dis. Child. 2000, 83, 498–501. [Google Scholar] [CrossRef]
- Gupta, S.K.; Nayak, R.P. Off-label use of medicine: Perspective of physicians, patients, pharmaceutical companies and regulatory authorities. J. Pharmacol. Pharmacother. 2014, 5, 88–92. [Google Scholar] [CrossRef]
- Soeters, P.B.; Grimble, R.F. The conditional role of inflammation in pregnancy and cancer. Clin. Nutr. 2013, 32, 460–465. [Google Scholar] [CrossRef]
- Heckman-Stoddard, B.M.; DeCensi, A.; Sahasrabuddhe, V.V.; Ford, L.G. Repurposing metformin for the prevention of cancer and cancer recurrence. Diabetologia 2017, 60, 1639–1647. [Google Scholar] [CrossRef]
- Chae, Y.K.; Arya, A.; Malecek, M.-K.; Shin, D.S.; Carneiro, B.; Chandra, S.; Kaplan, J.; Kalyan, A.; Altman, J.K.; Platanias, L.; et al. Repurposing metformin for cancer treatment: Current clinical studies. Oncotarget 2016, 7, 40767–40780. [Google Scholar] [CrossRef]
- Zhang, Z.-J.; Li, S. The prognostic value of metformin for cancer patients with concurrent diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2014, 16, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Liubchenko, K.; Kordbacheh, K.; Khajehdehi, N.; Visnjevac, T. Naltrexone’s impact on cancer progression and mortality: A systematic review of studies in humans, animal models, and cell cultures. Adv. Ther. 2021, 38, 904–924. [Google Scholar] [CrossRef] [PubMed]
- Farhood, B.; Goradel, N.H.; Mortezaee, K.; Khanlarkhani, N.; Salehi, E.; Nashtaei, M.S.; Mirtavoos-Mahyari, H.; Motevaseli, E.; Shabeeb, D.; Musa, A.E.; et al. Melatonin as an adjuvant in radiotherapy for radioprotection and radiosensitization. Clin. Transl. Oncol. 2018, 21, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Latocha, M.; Zyrek, L. Anti-cancer properties of dichloroacetate. Pol. Merkur. Lekarski. 2022, 50, 145–147. [Google Scholar] [PubMed]
- Wise, D.R.; Thompson, C.B. Glutamine addiction: A new therapeutic target in cancer. Trends Biochem. Sci. 2010, 35, 427–433. [Google Scholar] [CrossRef]
- Iannitti, T.; Palmieri, B. Clinical and experimental applications of sodium phenylbutyrate. Drugs R D 2011, 11, 227–249. [Google Scholar] [CrossRef]
- Gore, S.D.A.; Carducci, M. Modifying histones to tame cancer: Clinical development of sodium phenylbutyrate and other histone deacetylase inhibitors. Expert Opin. Investig. Drugs 2000, 9, 2923–2934. [Google Scholar] [CrossRef]
- Meade, B.; Sali, A.; Stephens, A.; Rainczuk, A.; Murphy, D.L. An investigation of metronomic photodynamic therapies for local prostate cancer: Supplementary fluorescent photography and proteomic studies, as measurable parameters of this treatment. J. Cancer Sci. Therap. 2018, 1, 8. [Google Scholar]
- Dery, M. Pharmacists Key to Safe Complementary Medicine Use, Australian Pharmacist. 2019. Available online: https://www.australianpharmacist.com.au/pharmacists-key-to-ensuring-safety-with-complementary-medicine/ (accessed on 22 March 2019).
- Gurley, B.; Fifer, E.; Gardner, Z. Pharmacokinetic Herb-Drug Interactions (Part 2): Drug Interactions Involving Popular Botanical Dietary Supplements and Their Clinical Relevance. Planta Med. 2012, 78, 1490–1514. [Google Scholar] [CrossRef]
- Izzo, A.A.; Ernst, E. Interactions between herbal medicines and prescribed drugs. Drugs 2009, 69, 1777–1798. [Google Scholar] [CrossRef]
- Yue, Q.Y.; Strandell, J.; Myrberg, O. Concomitant use of glucosamine may potentiate the effect of warfarin. Drug Saf. 2006, 29, 911–1010. [Google Scholar] [CrossRef]
- Tsai, Y.-T.; Lai, J.-N.; Wu, C.-T. The use of Chinese herbal products and its use on tamoxifam-induced endometrial cancer risk among female breast cancer patients: A population based study. J. Ethnopharm. 2014, 155, 1256–1262. [Google Scholar] [CrossRef]
- Jou, J.; Johnson, P.J. Nondisclosure of complementary and alternative medicine use to primary care physicians findings from the 2012 National Health Interview Survey. JAMA Intern. Med. 2016, 176, 545–546. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Type of Therapy | Some Key Benefits | References |
|---|---|---|
| Meditation | Significantly less tumours compared with non-meditators; fewer admissions for cancer; decreased mortality from cancer; cancer regression | [54,55,56] |
| Tai Chi and Qi Gong | Positive effects on cancer-specific quality of life, as well as fatigue, anxiety, immune function and cortisol levels | [57] |
| Pet therapy | Significant improvements in social and emotional wellbeing despite high symptom burden and expected decreases in physical and functional wellbeing associated with radiation-chemotherapy treatment [58]; pet therapy during chemotherapy associated with significant decrease in depression and increase in oxygen saturation [44] | [58,59] |
| Art therapy | Decreased anxiety, depression and pain in patients with cancer; decreasing anxiety in those receiving cancer therapy; improvement in wellbeing | [60,61,62,63,64] |
| Music therapy | Reduction of anxiety, pain, fatigue and improved mood and quality of life | [65,66] |
| Writing therapy | Improved quality of life | [67] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Brien, K.; Ried, K.; Binjemain, T.; Sali, A. Integrative Approaches to the Treatment of Cancer. Cancers 2022, 14, 5933. https://doi.org/10.3390/cancers14235933
O’Brien K, Ried K, Binjemain T, Sali A. Integrative Approaches to the Treatment of Cancer. Cancers. 2022; 14(23):5933. https://doi.org/10.3390/cancers14235933
Chicago/Turabian StyleO’Brien, Kylie, Karin Ried, Taufiq Binjemain, and Avni Sali. 2022. "Integrative Approaches to the Treatment of Cancer" Cancers 14, no. 23: 5933. https://doi.org/10.3390/cancers14235933
APA StyleO’Brien, K., Ried, K., Binjemain, T., & Sali, A. (2022). Integrative Approaches to the Treatment of Cancer. Cancers, 14(23), 5933. https://doi.org/10.3390/cancers14235933