
The Identification and Clinical Applications of Mutated Antigens in the Era of Immunotherapy
 , , ,
, , ,  , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
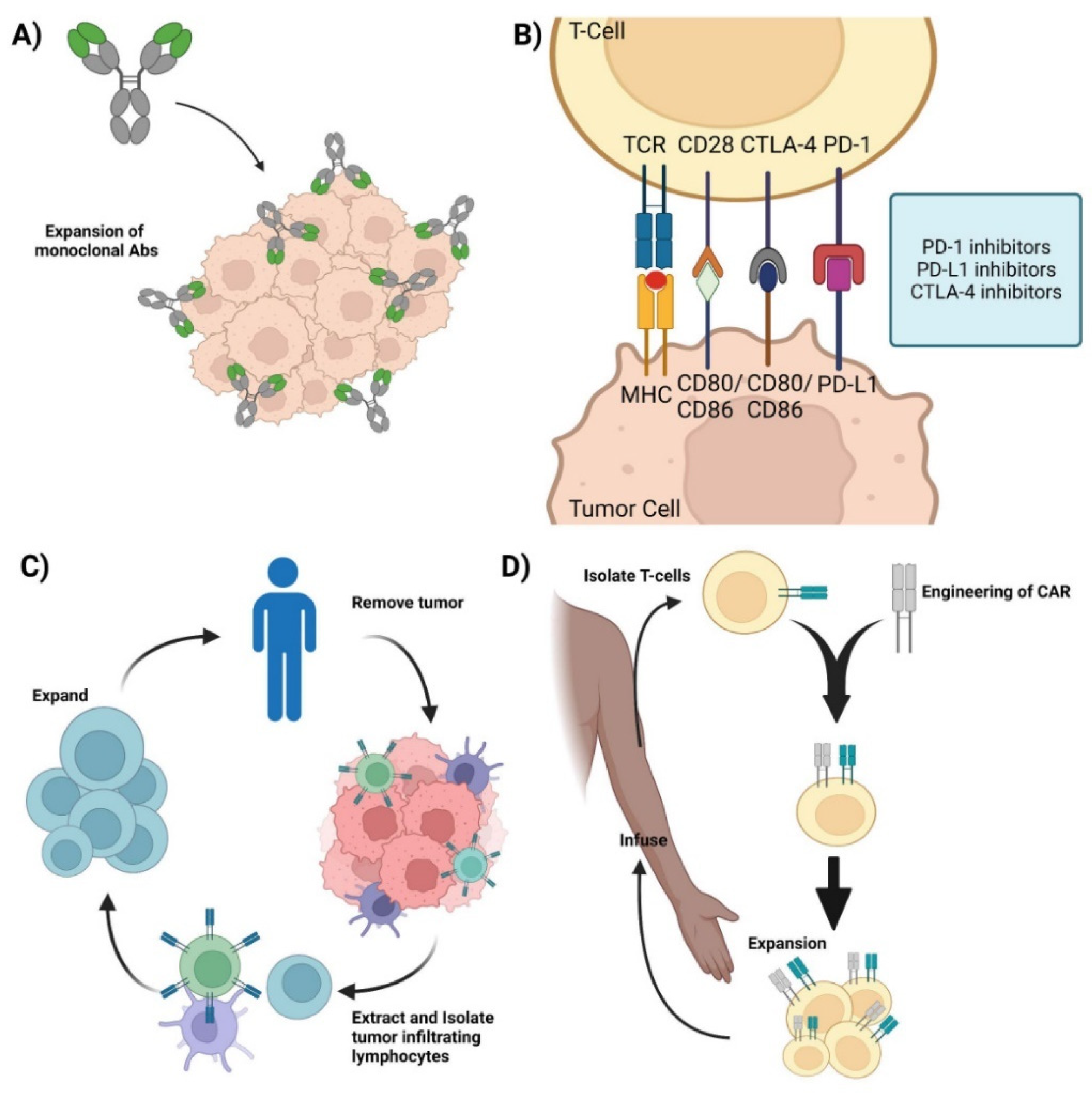
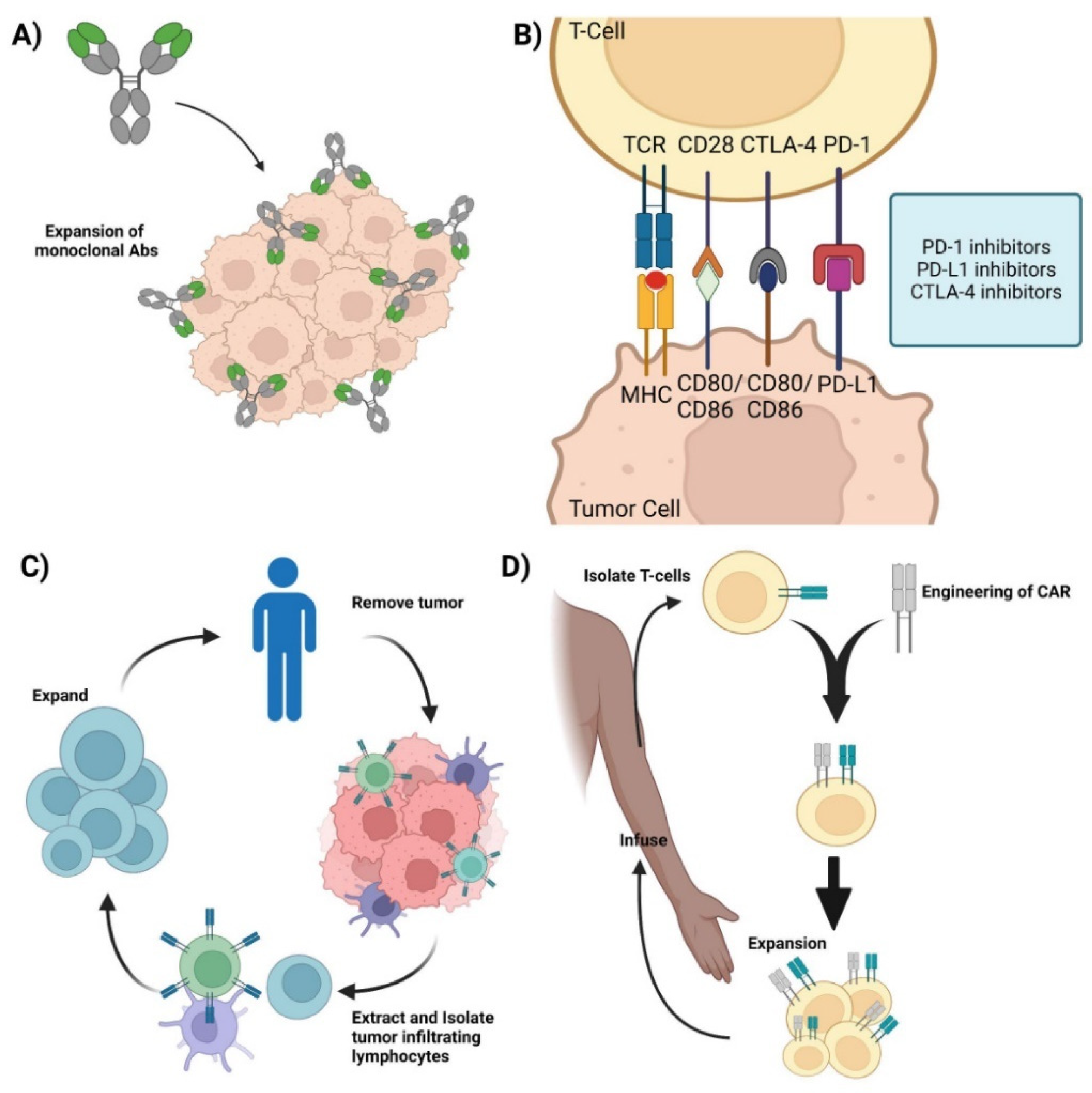
2. Cancer and Immunotherapy
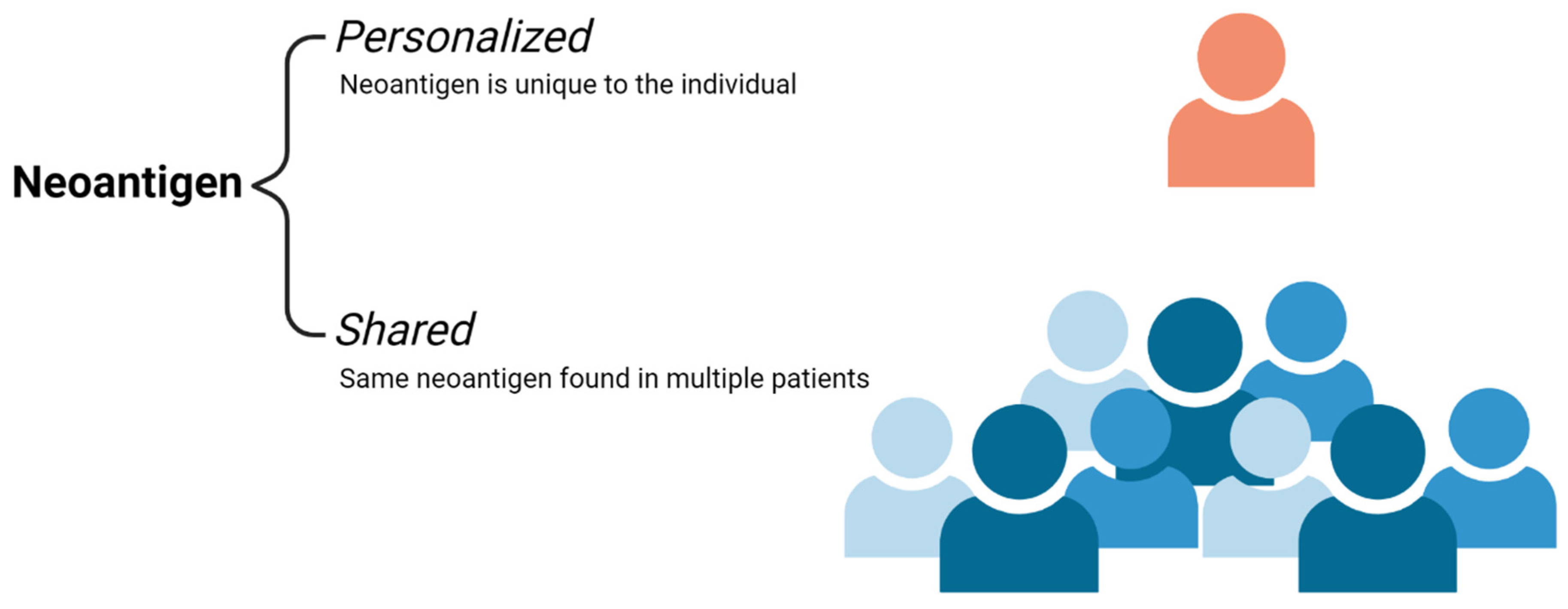
3. Neoantigens
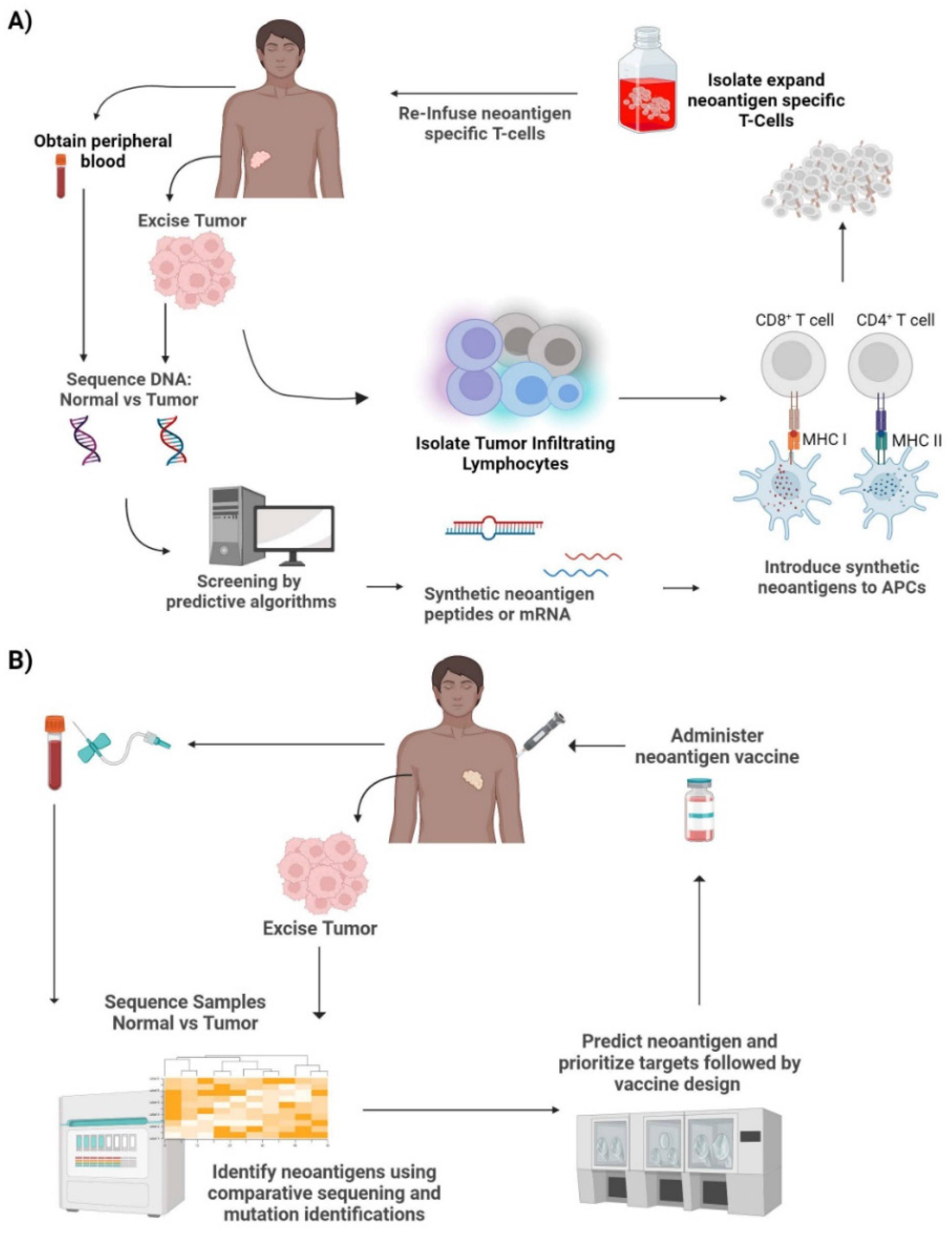
4. Identification of Neoantigens
5. Clinical Applications of Neoantigens
6. Neoantigen-Based Biomarkers
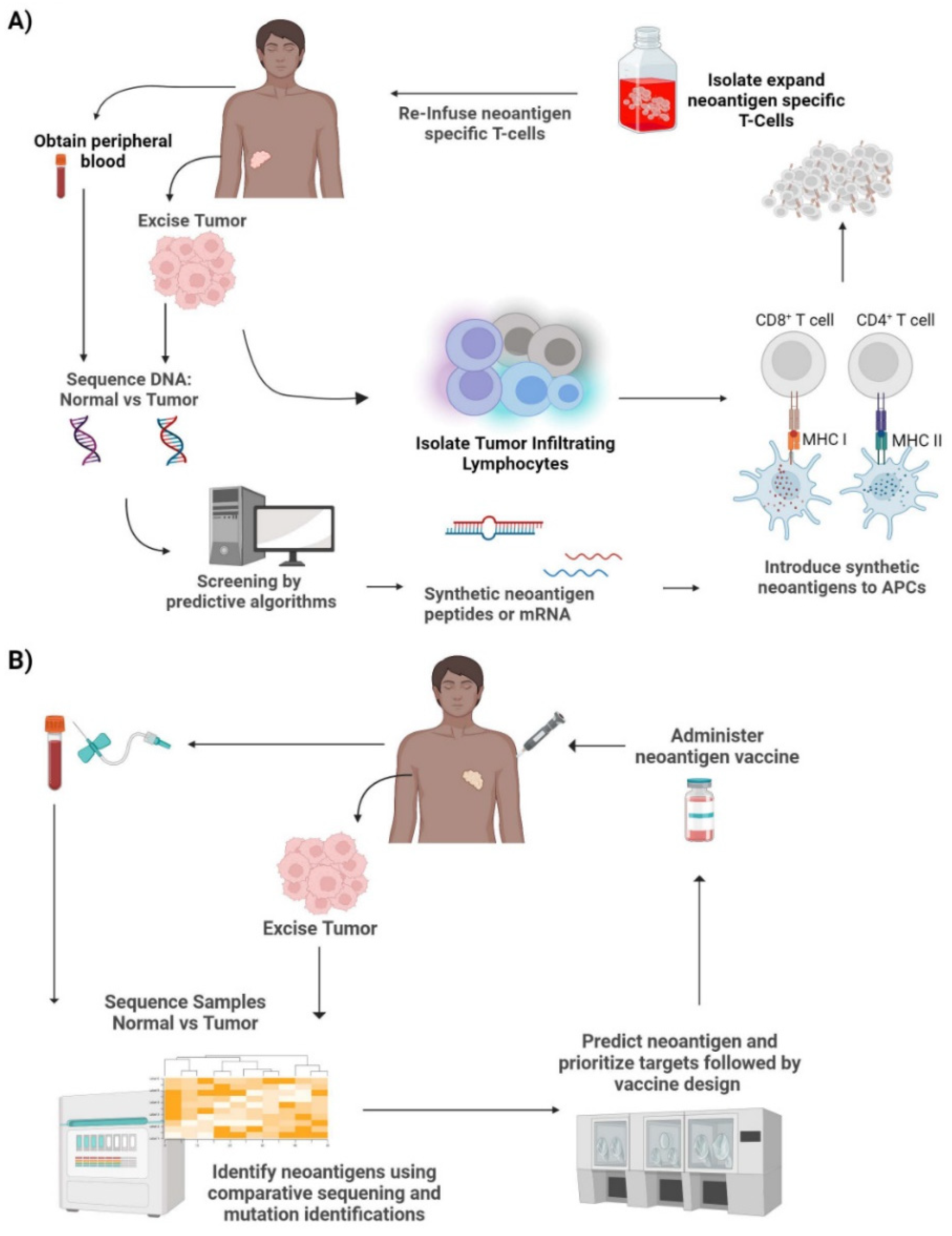
7. Neoantigen-Based Therapies
7.1. Neoantigen-Specific TCR-T Cell Therapy
7.2. Neoantigen Vaccines
8. Limitations and Challenges
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACT | Adoptive Cell Therapy |
| APC | Antigen Presenting Cell |
| CAR-T | Chimeric Antigen Receptor-T cell |
| CTA | Cancer Testis Antigens |
| DC | Dendritic Cell |
| HLA | Human Leukocyte Antigen |
| IFNγ | Interferon-gamma |
| ICI | Immune Checkpoint Inhibitors |
| irAEs | Immune-Related Adverse Events |
| KRAS | Kirsten rat sarcoma virus |
| mAb | monoclonal antibodies |
| MHC | Major Histocompatibility Complex |
| NK cell | Natural Killer cell |
| NGS | Next Generation Sequencing |
| NSCLC | Non-Small Cell Lung Carcinoma |
| TAA | Tumor Associated Antigens |
| TSA | Tumor Specific Antigen |
| TCR | T-Cell Receptor |
| TCRm | T-Cell Receptor Mimic Antibodies |
| TIL | Tumor Infiltrating Lymphocyte |
| TME | Tumor Microenvironment |
References
- Marrocco, I.; Romaniello, D.; Yarden, Y. Cancer Immunotherapy: The Dawn of Antibody Cocktails. In Human Monoclonal Antibodies; Steinitz, M., Ed.; Methods in Molecular Biology; Springer: New York, NY, USA, 2019; Volume 1904, pp. 11–51. [Google Scholar] [CrossRef]
- O’Donnell, J.S.; Teng, M.W.L.; Smyth, M.J. Cancer immunoediting and resistance to T cell-based immunotherapy. Nat. Rev. Clin. Oncol. 2019, 16, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Lei, X.; Lei, Y.; Li, J.-K.; Du, W.-X.; Li, R.-G.; Yang, J.; Li, J.; Li, F.; Tan, H.-B. Immune cells within the tumor microenvironment: Biological functions and roles in cancer immunotherapy. Cancer Lett. 2019, 470, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Lu, M.; Qin, Y.; Gao, W.; Tao, L.; Su, W.; Zhong, J. Neoantigen: A New Breakthrough in Tumor Immunotherapy. Front. Immunol. 2021, 12, 672356. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Shi, T.; Zhang, H.; Hu, J.; Song, Y.; Wei, J.; Ren, S.; Zhou, C. Tumor neoantigens: From basic research to clinical applications. J. Hematol. Oncol. 2019, 12, 1–13. [Google Scholar] [CrossRef]
- Zhang, Q.; Jia, Q.; Zhang, J.; Zhu, B. Neoantigens in precision cancer immunotherapy: From identification to clinical applications. Chin. Med. J. 2022; Publish Ah. [Google Scholar] [CrossRef]
- Peng, M.; Mo, Y.; Wang, Y.; Wu, P.; Zhang, Y.; Xiong, F.; Guo, C.; Wu, X.; Li, Y.; Li, X.; et al. Neoantigen vaccine: An emerging tumor immunotherapy. Mol. Cancer 2019, 18, 1–14. [Google Scholar] [CrossRef]
- Itoh, Y.; Nagase, H. Matrix metalloproteinases in cancer. Essays Biochem. 2002, 38, 21–36. [Google Scholar] [CrossRef]
- Garner, H.; de Visser, K.E. Immune crosstalk in cancer progression and metastatic spread: A complex conversation. Nat. Rev. Immunol. 2020, 20, 483–497. [Google Scholar] [CrossRef]
- Pelletier, J.P.R.; Mukhtar, F. Passive Monoclonal and Polyclonal Antibody Therapies. In Immunologic Concepts in Transfusion Medicine; Elsevier: Amsterdam, The Netherlands, 2020; pp. 251–348. [Google Scholar] [CrossRef]
- Zahavi, D.J.; Weiner, L.M. Targeting Multiple Receptors to Increase Checkpoint Blockade Efficacy. Int. J. Mol. Sci. 2019, 20, 158. [Google Scholar] [CrossRef]
- Ahmadzadeh, M.; Pasetto, A.; Jia, L.; Deniger, D.C.; Stevanović, S.; Robbins, P.F.; Rosenberg, S.A. Tumor-infiltrating human CD4 + regulatory T cells display a distinct TCR repertoire and exhibit tumor and neoantigen reactivity. Sci. Immunol. 2019, 4, eaao4310. [Google Scholar] [CrossRef]
- Pearlman, A.H.; Hwang, M.S.; Konig, M.F.; Hsiue, E.H.-C.; Douglass, J.; DiNapoli, S.R.; Mog, B.J.; Bettegowda, C.; Pardoll, D.M.; Gabelli, S.B.; et al. Targeting public neoantigens for cancer immunotherapy. Nat. Cancer 2021, 2, 487–497. [Google Scholar] [CrossRef]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Ghisoni, E.; Wicky, A.; Bouchaab, H.; Imbimbo, M.; Delyon, J.; Moura, B.G.; Gérard, C.; Latifyan, S.; Özdemir, B.; Caikovski, M.; et al. Late-onset and long-lasting immune-related adverse events from immune checkpoint-inhibitors: An overlooked aspect in immunotherapy. Eur. J. Cancer 2021, 149, 153–164. [Google Scholar] [CrossRef]
- Uhara, H.; Kiyohara, Y.; Uehara, J.; Fujisawa, Y.; Takenouchi, T.; Otsuka, M.; Uchi, H.; Fukushima, S.; Minami, H.; Hatsumichi, M.; et al. Five-year survival with nivolumab in previously untreated Japanese patients with advanced or recurrent malignant melanoma. J. Dermatol. 2021, 48, 592–599. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Yau, T.; Kang, Y.-K.; Kim, T.-Y.; El-Khoueiry, A.B.; Santoro, A.; Sangro, B.; Melero, I.; Kudo, M.; Hou, M.-M.; Matilla, A.; et al. Efficacy and Safety of Nivolumab Plus Ipilimumab in Patients With Advanced Hepatocellular Carcinoma Previously Treated With Sorafenib: The CheckMate 040 Randomized Clinical Trial. JAMA Oncol. 2020, 6, e204564. [Google Scholar] [CrossRef]
- Bagchi, S.; Yuan, R.; Engleman, E.G. Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance. Annu. Rev. Pathol. Mech. Dis. 2021, 16, 223–249. [Google Scholar] [CrossRef]
- El-Osta, H.; Jafri, S. Predictors for clinical benefit of immune checkpoint inhibitors in advanced non-small-cell lung cancer: A meta-analysis. Immunotherapy 2019, 11, 189–199. [Google Scholar] [CrossRef]
- Tsimberidou, A.-M.; Van Morris, K.; Vo, H.H.; Eck, S.; Lin, Y.-F.; Rivas, J.M.; Andersson, B.S. T-cell receptor-based therapy: An innovative therapeutic approach for solid tumors. J. Hematol. Oncol. 2021, 14, 1–22. [Google Scholar] [CrossRef]
- Ma, S.; Li, X.; Wang, X.; Cheng, L.; Li, Z.; Zhang, C.; Ye, Z.; Qian, Q. Current Progress in CAR-T Cell Therapy for Solid Tumors. Int. J. Biol. Sci. 2019, 15, 2548–2560. [Google Scholar] [CrossRef] [PubMed]
- Depil, S.; Duchateau, P.; Grupp, S.A.; Mufti, G.; Poirot, L. ‘Off-the-shelf’ allogeneic CAR T cells: Development and challenges. Nat. Rev. Drug Discov. 2020, 19, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Kunte, S.; Abraham, J.; Montero, A.J. Novel HER2–targeted therapies for HER2–positive metastatic breast cancer. Cancer 2020, 126, 4278–4288. [Google Scholar] [CrossRef] [PubMed]
- Binnewies, M.; Roberts, E.W.; Kersten, K.; Chan, V.; Fearon, D.F.; Merad, M.; Coussens, L.M.; Gabrilovich, D.I.; Ostrand-Rosenberg, S.; Hedrick, C.C.; et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat. Med. 2018, 24, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Buonaguro, L.; Tagliamonte, M. Selecting Target Antigens for Cancer Vaccine Development. Vaccines 2020, 8, 615. [Google Scholar] [CrossRef] [PubMed]
- Blass, E.; Ott, P.A. Advances in the development of personalized neoantigen-based therapeutic cancer vaccines. Nat. Rev. Clin. Oncol. 2021, 18, 215–229. [Google Scholar] [CrossRef]
- Kandoth, C.; McLellan, M.D.; Vandin, F.; Ye, K.; Niu, B.; Lu, C.; Xie, M.; Zhang, Q.; McMichael, J.F.; Wyczalkowski, M.A.; et al. Mutational landscape and significance across 12 major cancer types. Nature 2013, 502, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Roudko, V.; Greenbaum, B.; Bhardwaj, N. Computational Prediction and Validation of Tumor-Associated Neoantigens. Front. Immunol. 2020, 11, 27. [Google Scholar] [CrossRef]
- Sun, C.; Xu, S. Advances in personalized neoantigen vaccines for cancer immunotherapy. Biosci. Trends 2020, 14, 349–353. [Google Scholar] [CrossRef]
- Gopanenko, A.V.; Kosobokova, E.N.; Kosorukov, V.S. Main Strategies for the Identification of Neoantigens. Cancers 2020, 12, 2879. [Google Scholar] [CrossRef]
- Rosenthal, R.; Cadieux, E.L.; Salgado, R.; Bakir, M.A.; Moore, D.A.; Hiley, C.T.; Lund, T.; Tanić, M.; Reading, J.L.; Joshi, K.; et al. Neoantigen-directed immune escape in lung cancer evolution. Nature 2019, 567, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Luo, H.; Kong, Y.; Lai, W.-F.; Cui, L.; Zhu, X. Cancer neoantigen: Boosting immunotherapy. Biomed. Pharmacother. 2020, 131, 110640. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Salazar, G.T.; Zhang, N.; An, Z. T-cell receptor mimic (TCRm) antibody therapeutics against intracellular proteins. Antib. Ther. 2019, 2, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, P.; Pasetto, A.; Robbins, P.F.; Parkhurst, M.R.; Paria, B.C.; Jia, L.; Gartner, J.J.; Hill, V.; Yu, Z.; Restifo, N.P.; et al. Neoantigen screening identifies broad TP53 mutant immunogenicity in patients with epithelial cancers. J. Clin. Investig. 2019, 129, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Malekzadeh, P.; Yossef, R.; Cafri, G.; Paria, B.C.; Lowery, F.J.; Jafferji, M.; Good, M.L.; Sachs, A.; Copeland, A.R.; Kim, S.P.; et al. Antigen Experienced T Cells from Peripheral Blood Recognize p53 Neoantigens. Clin. Cancer Res. 2020, 26, 1267–1276. [Google Scholar] [CrossRef]
- Paria, B.C.; Levin, N.; Lowery, F.J.; Pasetto, A.; Deniger, D.C.; Parkhurst, M.R.; Yossef, R.; Kim, S.P.; Florentin, M.; Ngo, L.T.; et al. Rapid Identification and Evaluation of Neoantigen-reactive T-Cell Receptors From Single Cells. J. Immunother. 2020, 44, 1–8. [Google Scholar] [CrossRef]
- Wagner, S.; Mullins, C.S.; Linnebacher, M. Colorectal cancer vaccines: Tumor-associated antigens vs neoantigens. World J. Gastroenterol. 2018, 24, 5418–5432. [Google Scholar] [CrossRef]
- Samstein, R.M.; Lee, C.-H.; Shoushtari, A.N.; Hellmann, M.D.; Shen, R.; Janjigian, Y.Y.; Barron, D.A.; Zehir, A.; Jordan, E.J.; Omuro, A.; et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat. Genet. 2019, 51, 202–206. [Google Scholar] [CrossRef]
- Zhou, L.; Zou, F.; Sun, W. Prioritizing candidate peptides for cancer vaccines through predicting peptide presentation by HLA-I proteins. Biometrics 2022. [Google Scholar] [CrossRef]
- Ott, P.A.; Hu, Z.; Keskin, D.B.; Shukla, S.A.; Sun, J.; Bozym, D.J.; Zhang, W.; Luoma, A.; Giobbie-Hurder, A.; Peter, L.; et al. An immunogenic personal neoantigen vaccine for patients with melanoma. Nature 2017, 547, 217–221. [Google Scholar] [CrossRef]
- Lin, M.; Zhang, X.-L.; You, R.; Yang, Q.; Zou, X.; Yu, K.; Liu, Y.-P.; Zou, R.-H.; Hua, Y.-J.; Huang, P.-Y.; et al. Neoantigen landscape in metastatic nasopharyngeal carcinoma. Theranostics 2021, 11, 6427–6444. [Google Scholar] [CrossRef]
- Castle, J.C.; Kreiter, S.; Diekmann, J.; Löwer, M.; van de Roemer, N.; de Graaf, J.; Selmi, A.; Diken, M.; Boegel, S.; Paret, C.; et al. Exploiting the Mutanome for Tumor Vaccination. Cancer Res. 2012, 72, 1081–1091. [Google Scholar] [CrossRef]
- Siniard, R.C.; Harada, S. Immunogenomics: Using genomics to personalize cancer immunotherapy. Virchows Arch. 2017, 471, 209–219. [Google Scholar] [CrossRef]
- Sheinson, D.M.; Wong, W.B.; Meyer, C.S.; Stergiopoulos, S.; Lofgren, K.T.; Flores, C.; Adams, D.V.; Fleury, M.E. Trends in Use of Next-Generation Sequencing in Patients With Solid Tumors by Race and Ethnicity After Implementation of the Medicare National Coverage Determination. JAMA Netw. Open 2021, 4, e2138219. [Google Scholar] [CrossRef]
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer immunotherapy efficacy and patients’ sex: A systematic review and meta-analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef]
- Christian, L.S.; Wang, L.; Lim, B.; Deng, D.; Wu, H.; Wang, X.-F.; Li, Q.-J. Resident memory T cells in tumor-distant tissues fortify against metastasis formation. Cell Rep. 2021, 35, 109118. [Google Scholar] [CrossRef]
- Aldous, A.R.; Dong, J.Z. Personalized neoantigen vaccines: A new approach to cancer immunotherapy. Bioorganic Med. Chem. 2017, 26, 2842–2849. [Google Scholar] [CrossRef]
- Lozano-Rabella, M.; Gros, A. TCR Repertoire Changes during TIL Expansion: Clonal Selection or Drifting? Clin. Cancer Res. 2020, 26, 4177–4179. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Cancer | NCT No. | Status | Phase | Number of Patients Enrolled | Intervention |
|---|---|---|---|---|---|
| Non Small Cell Lung Cancer, Colorectal Cancer, Gastroesophageal Adenocarcinoma, Urothelial Carcinoma, Pancreatic Ductal Adenocarcinoma | NCT03794128 | Completed | Observational | 93 | Not Applicable |
| Ovarian Cancer, Endometrial Cancer, Colorectal Cancer, Cholangiocarcinoma, Non Small Cell Lung Cancer, Pancreatic Cancer | NCT05124743 | Recruiting | Observational | 2000 | Not Applicable |
| Metastatic Colorectal Cancer, Stage II/III Colon Cancer | NCT05158621 | Recruiting | Observational | 100 | Not Applicable |
| Colon Cancer | NCT04994093 | Recruiting | Observational | 100 | Not Applicable |
| Non-small Cell Lung Cancer | NCT04923802 | Recruiting | Observational | 400 | Not Applicable |
| Hematological Malignancies B | NCT02844491 | Terminated | Observational | 28 | Not Applicable |
| Solid Tumor | NCT03517917 | Recruiting | Observational | 400 | Not Applicable |
| Synovial Cell, Colorectal, Lung, Bladder Cancer, Melanoma | NCT00001823 | Recruiting | Observational | 7000 | Not Applicable |
| Acute Myeloid Leukemia | NCT03789981 | Recruiting | Observational | 75 | Not Applicable |
| Pancreatic Cancer | NCT02869802 | Recruiting | Observational | 190 | Not Applicable |
| Pancreatic Ductal Cancer | NCT02750657 | Active, not recruiting | Observational | 332 | Not Applicable |
| Cancer | NCT No. | Status | Phase | Number of Patients Enrolled | Intervention |
|---|---|---|---|---|---|
| Malignant Epithelial Tumors, Malignant Solid Tumors | NCT05141474 | Recruiting | Phase 1, early | 10 | Single Arm: NEXTGEN-TIL (Neoantigen-based TIL) |
| Advanced Non- Small Cell Lung Cancer | NCT04032847 | Recruiting | Phase 1,2 | 50 | Group 1) ATL001 (autologous clonal neoantigen reactive T cells) Group 2) ATL001 + Pembrolizumab |
| Solid Tumor | NCT03970382 | Active, not recruiting, suspended | Phase 1 | 21 | Sequential: NeoTCR-P1 adoptive cell therapy + nivolumab + IL-2 |
| Endocrine/Neuroendocrine, Non-Small Cell Lung Cancer, Breast Cancer, Gastrointestinal/Genitourinary Cancers, Ovarian Cancer | NCT04102436 | Recruiting | Phase 2 | 210 | Single Arm: Fludarabine + Cyclophosphamide + Aldesleukin + Sleeping Beauty Transposed PBL |
| Melanoma, Non-small Cell Lung Cancer, Squamous Cell Carcinoma of Head and Neck, Urothelial Carcinoma, Renal Cell Carcinoma, Small-cell Lung Cancer, Cutaneous Squamous Cell Carcinoma, Anal Squamous Cell Carcinoma, Merkel Cell Carcinoma | NCT04596033 | Terminated | Phase 1 | 49 | Group 1) GEN-011 (T cell therapy) + IL-2 Group 2) GEN-011 + IL-2 + Fludarabine + Cyclophosphamide |
| Gastrointestinal (GI) Neoplasms, GI Epithelial Cancer, Colorectal, Pancreatic, Gall Bladder, Colon, Esophageal, Stomach Cancer | NCT04426669 | Recruiting | Phase 1, 2 | 20 | Sequential: Cyclophosphamide + Fludarabine + TIL + Aldesleukin |
| Unresectable Melanoma Metastatic Melanoma | NCT04625205 | Recruiting | Phase 1 | 52 | Single Arm: NEO-PTC-01 (autologous personalized T cell) |
| Melanoma | NCT03997474 | Recruiting | Phase 1, 2 | 40 | Single Arm: ATL001 (autologous clonal neoantigen reactive T cells) + Checkpoint Inhibitor |
| Gynecologic Cancer, Colorectal Cancer, Pancreatic Cancer, Non-small Cell Lung Cancer, Cholangiocarcinoma, Endometrial Cancer, Ovarian Cancer, Neoplasm; Lung Adenocarcinoma, Lung Squamous Carcinoma, Lung Adenosquamous carcinoma | NCT05194735 | Recruiting | Phase 1,2 | 180 | Sequential: Neoantigen specific TCR-T cell drug product + Aldesleukin (IL-2) |
| Malignant Epithelial Neoplasms | NCT04520711 | Recruiting | Phase 1 | 24 | Single Arm: TCR-transduced T cells + CDX-1140 + Pembro |
| Cancer | NCT No. | Status | Phase | Number of Patients Enrolled | Intervention |
|---|---|---|---|---|---|
| Non Small Cell Lung Cancer | NCT04397926 | Recruiting | Phase 1 | 20 | Single Arm: Individualized neoantigen peptides vaccine |
| Triple Negative Breast Cancer | NCT04105582 | Completed | Phase 1 | 5 | Single Arm: Neo-antigen pulsed Dendritic cell |
| Non Small Cell Lung Cancer | NCT04487093 | Recruiting | Phase 1 | 20 | Group 1) neoantigen vaccine + EGFR-TKI; Group 2) neoantigen vaccine + anti- angiogenesis |
| Pancreatic Cancer | NCT03645148 | Completed | Phase 1 | 7 | Single Arm: iNeo-Vac-P01 (neoantigen peptides)+ GM-CSF |
| Gastric Cancer, Esophageal Cancer, Liver Cancer | NCT05192460 | Recruiting | Not applicable | 36 | Single Arm: neoantigen tumor vaccine + PD-1/L1 |
| Pancreatic Cancer | NCT03122106 | Active, not recruiting | Phase 1 | 15 | Single Arm: personalized neoantigen DNA vaccine |
| Resectable Pancreatic Cancer | NCT04810910 | Recruiting | Phase 1 | 20 | Single Arm: iNeo-Vac-P01 (neoantigen peptides) |
| Resectable Esophageal Cancer | NCT05307835 | Recruiting | Phase 1 | 40 | Group 1) iNeo-Vac-P01; Group 2) GM-CSF |
| Pancreatic Cancer | NCT03956056 | Active, not recruiting | Phase 1 | 12 | Single Arm: Neoantigen Peptide Vaccine + Poly ICLC |
| Neoplasms | NCT05475106 | Recruiting | Phase 1 | 100 | Single Arm: Multi-peptide neoantigen vaccine |
| Neoplasms | NCT04509167 | Completed | Phase 1 | 30 | Single Arm: Neoantigen peptides |
| Extensive-stage Small Cell Lung Cancer | NCT04397003 | Recruiting | Phase 1 | 27 | Single Arm: Carboplatin + etoposide + durvalumab + polyepitope neoantigen DNA vaccine |
| Pancreatic Cancer | NCT03558945 | Recruiting | Phase 1 | 60 | Group 1) Radical surgery and post-operative chemotherapy + personalized neoantigen vaccine; Group 2) Radical surgery and conventional post-operative chemotherapy |
| Triple Negative Breast Cancer | NCT03199040 | Active, not recruiting | Phase 1 | 18 | Group 1) Neoantigen DNA vaccine + Durvalumab; Group 2) Neoantigen DNA vaccine |
| Metastatic Hormone-Sensitive Prostate Cancer | NCT03532217 | Completed | Phase 1 | 19 | Single arm: PROSTVAC + ipilumumab + nivolumab neoantigen DNA vaccine |
| Colonic neoplasms | NCT05456165 | Recruiting | Phase 2 | 142 | Group 1) GRT-C901 (adenovirus vector) vaccine, GRT-R902 (self-amplifying mRNA vector) vaccine + Atezolizumab + Ipilimumab; Group 2) Adjuvant Chemotherapy |
| Advanced Malignant Solid Tumor | NCT03662815 | Active, not recruiting | Phase 1 | 30 | Single Arm: iNeo-Vac-P01 + GM-CSF |
| Kidney Cancer | NCT02950766 | Recruiting | Phase 1 | 19 | Single Arm: NeoVax (Poly-ICLC and Neoantigen Peptide) + Ipilimumab |
| Advanced Malignant Solid Tumor | NCT04864379 | Recruiting | Phase 1 | 30 | Group 1) RFA+PD-1+iNeo-Vac-P01; Group 2) RFA+iNeo-Vac-P01+PD-1 |
| Colorectal neoplasms | NCT05141721 | Recruiting | Phase 2, Phase 3 | 665 | Group 1) GRT-C901/GRT-C902 (neoantigen vaccine) + Fluoropyrimidine + Bevacizumab + Oxaliplatin + Atezolizumab + Ipilimumab; Group 2) Fluoropyrimidine + Bevacizumab + Oxaliplatin |
| Non Small Cell Lung Cancer, Colorectal Cancer, Pancreatic Cancer, Solid Tumor, Shared Neoantigen-Positive Solid Tumors | NCT03953235 | Recruiting | Phase 1, 2 | 144 | Sequential: GRT-C903 + GRT-R904 + ipilimumab + nivolumab |
| Non Small Cell Lung Cancer, Colorectal Cancer, Gastroesophageal Adenocarcinoma, Urothelial Carcinoma | NCT03639714 | Active, not recruiting | Phase 1,2 | 214 | Sequential: GRT-C901 + GRT-R902 + nivolumab + ipilimumab |
| Colorectal Cancer | NCT01885702 | Active, not recruiting | Phase 1, 2 | 25 | Group 1: Colorectal Cancer pts with DC Vaccine (Frameshift-derived neoantigen loaded onto DC); Group 2: Lynch syndrome pts with DC vaccine |
| Anatomic Stage IV Breast Cancer, Clinical Stage III, IV Cutaneous Melanoma, Hormone Receptor-Positive Breast Carcinoma, Locally Advanced Cutaneous Melanoma, Metastatic: Acral Lentiginous Melanoma, Conjunctival Melanoma, Cutaneous Melanoma, HER2-Negative Breast Carcinoma, Mucosal Melanoma, Pathologic Stage IIIC, IIID, IV Cutaneous Melanoma, Prognostic Stage IV Breast Cancer, Recurrent: Acral Lentiginous Melanoma, Cutaneous Melanoma, Mucosal Melanoma; Refractory HER2-Negative Breast Carcinoma, Unresectable: Acral Lentiginous Melanoma, Cutaneous Melanoma, Mucosal Melanoma | NCT05098210 | Recruiting | Phase 1 | 20 | Single Arm: Neoantigen Peptide Vaccine + Nivolumab + Poly ICLC |
| Melanoma, Colon Cancer, Gastrointestinal Cancer, Genitourinary Cancer, Hepatocellular Cancer | NCT03480152 | Terminated | Phase 1,2 | 5 | Single Arm: NCI-4650, a messenger ribonucleic acid (mRNA)-based, Personalized Cancer Vaccine |
| Urothelial/Bladder Cancer | NCT03359239 | Completed | Phase 1 | 10 | Single Arm: PGV001 (multipeptide personalized neoantigen vaccine) + Atezolizumab |
| Anatomic Stage IV Breast Cancer, Invasive Breast Carcinoma, Metastatic Triple-Negative Breast Carcinoma | NCT03606967 | Recruiting | Phase 2 | 70 | Group 1) nab-paclitaxel + durvalumab + tremelimumab + personalized synthetic long peptide vaccine; Group 2) nab-paclitaxel + durvalumab + tremelimumab |
| Gastric Cancer, Hepatocellular Carcinoma, Non-Small-Cell Lung Cancer, Colon Rectal Cancer | NCT04147078 | Recruiting | Phase 1 | 80 | Single Arm: tumor neoantigen primed DC vaccine |
| Melanoma, Gastrointestinal Cancer, Breast Cancer, Ovarian Cancer, Pancreatic Cancer | NCT03300843 | Terminated | Phase 2 | 1 | Single Arm: Peptide loaded dendritic cell vaccine |
| Myeloproliferative Neoplasms | NCT05444530 | Recruiting | Phase 1 | 60 | Sequential: VAC85135 (Neoantigen Vaccine) + Ipilimumab |
| Malignant Melanoma, Metastatic, Non Small Cell Lung Cancer Metastatic, Bladder Urothelial Carcinoma, Metastatic | NCT03715985 | Active, not recruiting | Phase 1,2 | 12 | Sequential: EVAX-01-CAF09b (personalised NPV-ds001 drug) |
| Anatomic Stage III, IIIA, IIIB, IIIC, IV Breast Cancer, Clinical Stage III, IV Cutaneous Melanoma, Clinical Stage III, IV, IVA, IVB, Gastric Cancer, Clinical Stage III, IV, IVA, IVB Gastroesophageal Junction (GEJ) Adenocarcinoma, Clinical Stage III, IV Merkel Cell Carcinoma, Locally Advanced and Metastatic: Cervical, Endometrial Carcinoma, Gastric Adenocarcinoma, GEJ Adenocarcinoma, Head and Neck Squamous Cell Carcinoma, Hepatocellular Carcinoma, Lung Non-Small Cell Carcinoma, Malignant Solid Neoplasm, Melanoma, Merkel Cell Carcinoma, Renal Cell Carcinoma, Skin Squamous Cell Carcinoma, TNBC, Unresectable Breast Carcinoma, Unresectable Cervical Carcinoma, | NCT05269381 | Recruiting | Phase 1 | 36 | Single Arm: Cyclophosphamide + Personalized Neoantigen vaccine + Pembrolizumab |
| Unresectable Gastric Adenocarcinoma, Unresectable GEJ Adenocarcinoma, Unresectable Renal Cell Carcinoma, Urothelial Carcinoma, Pathologic Stage III: Cutaneous Melanoma, Gastric Cancer, GEJ Adenocarcinoma, Merkel Cell Carcinoma; Pathologic Stage IIIA: Cutaneous Melanoma, Gastric Cancer, GEJ Adenocarcinoma; Pathologic Stage IIIB: Cutaneous Melanoma, Gastric Cancer, GEJ Adenocarcinoma; Pathologic Stage IIIC: Cutaneous Melanoma, Gastric Cancer; Pathologic Stage IIID Cutaneous Melanoma; Pathologic Stage IV Cutaneous Melanoma, Gastric Cancer, GEJ Adenocarcinoma, Merkel Cell Carcinoma; Pathologic Stage IVA, IVB GEJ Adenocarcinoma; Postneoadjuvant Therapy Stage III, IV Gastric Cancer; Postneoadjuvant Therapy Stage III, IIIA, IIIB, IVA, IVB GEJ Adenocarcinoma, Prognostic Stage III, IIIA, IIIB, IIIC, IV Breast Cancer, Skin Squamous Cell Carcinoma; Stage III: Cervical Cancer, Cutaneous Squamous Cell Carcinoma of the Head and Neck, Hepatocellular Carcinoma, Lung Cancer, Renal Cell Cancer, Uterine Corpus Cancer; Stage IIIA Cervical Cancer, Hepatocellular Carcinoma, Lung Cancer, Uterine Corpus Cancer; Stage IIIB Cervical Cancer, Hepatocellular Carcinoma, | NCT05269381 | Recruiting | Phase 1 | 36 | Single Arm: Cyclophosphamide + Personalized Neoantigen vaccine + Pembrolizumab |
| Lung Cancer, Uterine Corpus Cancer; Stage IIIC Lung Cancer; Stage IIIC IIIC1 IIIC2 Uterine Corpus Cancer; Stage IV Cutaneous Squamous Cell Carcinoma of the Head and Neck, Renal Cell Cancer; Stage IV IVA IVB Cervical Cancer, Hepatocellular Carcinoma, Lung Cancer, Uterine Corpus Cancer; Triple-Negative Breast Carcinoma, Unresectable: Cervical Carcinoma, Endometrial Carcinoma, Gastric Adenocarcinoma, GEJ Adenocarcinoma, Head and Neck Squamous Cell Carcinoma, Hepatocellular Carcinoma, Lung Non-Small Cell Carcinoma, Malignant Solid Neoplasm, Melanoma, Merkel Cell Carcinoma, Renal Cell Carcinoma, Skin Squamous Cell Carcinoma, Triple-Negative Breast Carcinoma, Urothelial Carcinoma | NCT05269381 | Recruiting | Phase 1 | 36 | Single Arm: Cyclophosphamide + Personalized Neoantigen vaccine + Pembrolizumab |
| Hepatocellular Cancer, Colorectal Cancer, Liver Metastases | NCT04912765 | Recruiting | Phase 2 | 60 | Single Arm: Neoantigen Dendritic Cell Vaccine + Nivolumab |
| Biochemically Recurrent Prostate Carcinoma, Prostate Adenocarcinoma | NCT04336943 | Recruiting | Phase 2 | 30 | Single Arm: Durvalumab + Olaparib against pts with a predicted high neoantigen load |
| Breast Cancer, Cutaneous melanoma | NCT02831634 | Completed | Not applicable | 25 | Not Applicable |
| Advanced Solid Tumor | NCT05020119 | Recruiting | Phase 1 | 9 | Sequential Neoantigen-expanded cell therapy |
| Endocrine Tumors, Non-Small Cell Lung Cancer, Ovarian Cancer, Breast Cancer, Gastrointestinal/Genitourinary Cancers, Neuroendocrine Tumors, Multiple Myeloma | NCT03412877 | Recruiting | Phase 2 | 270 | Group 1) cyclophosphamide + fludarabine + Individual Patient TCR-Transduced PBL + high- or low-dose aldesleukin; Group 2) cyclophosphamide + fludarabine + Individual Patient TCR-Transduced PBL + high- or low-dose aldesleukin + pembrolizumab |
| Melanoma | NCT01970358 | Completed | Phase 1 | 20 | Single Arm: NeoVax (peptides + poly-ICLC) |
| Ovarian Cancer | NCT04024878 | Recruiting | Phase 1 | 30 | Group 1) Nivolumab + NeoVax; Group 2) Nivolumab + NeoVax + Core Needle Bx upon recurrence |
| Melanoma | NCT04072900 | Recruiting | Phase 1 | 30 | Single Arm: Personalized NeoAntigen Cancer Vaccine- Neo-Vac-Mn (peptides + rhGM-CSF + anti-PD1 + Imiquimod 5% Topical Cream) |
| Pancreatic Cancer | NCT04161755 | Active, not recruiting | Phase 1 | 29 | Single Arm: Atezolizumab + RO7198457 (personalized vaccine) + mFOLFIRINOX |
| Glioblastoma | NCT02287428 | Recruiting | Phase 1 | 56 | Group 1) Standard Radiation (Std RT) + NeoVax; Group 2) Pembrolizumab/Std RT + NeoVax + Pembrolizumab; Group 3) Std RT + NeoVax + Pembrolizumab (Pembro); Group 4) Std RT (+ 1 dose Pembro) + NeoVax + Pembro; Group 5) Std RT + Temozolomide + NeoVax + Pembro |
| Lymphocytic Leukemia | NCT03219450 | Recruiting | Phase 1 | 15 | Sequential: NeoVax + Cyclophosphamide + Pembrolizumab |
| Follicular Lymphoma | NCT03361852 | Recruiting | Phase 1 | 20 | Single Arm: Rituximab + NeoVax + Pembro |
| Advanced Cancer | NCT02992977 | Terminated | Phase 1 | 3 | Single Arm: AutoSynVax™ (personalized neoantigen) vaccine |
| Breast Cancer Female | NCT04879888 | Completed | Phase 1 | 9 | Single Arm: Peptide pulsed Dendritic cell |
| Advanced Cancer | NCT03568058 | Active, not recruiting | Phase 1 | 30 | Group 1) Personalized Vaccine + Pembro; Group 2) Pembro then personalized vaccine; Group 3) Pembro + personalized vaccine; Group 4) Personalized vaccine |
| Solid Tumors, Adult | NCT05354323 | Recruiting | Phase 1 | 6 | Single Arm: NECVAX-NEO1 (Personalized patient-individual oral DNA vaccine) |
| Solid Tumor, Adult | NCT03673020 | Completed | Phase 1 | 3 | Single Arm: ASV® AGEN2017 + QS-21 Stimulon® adjuvant (Neoantigen vaccine) |
| High Risk Cancer, Pancreatic Cancer | NCT05013216 | Recruiting | Phase 1 | 25 | Single Arm: pooled mutant-KRAS peptide vaccine with poly-ICLC adjuvant |
| Cutaneous Melanoma, Non-small Cell Lung Cancer, Squamous Cell Carcinoma of the Head and Neck, Urothelial, Renal Cell Carcinoma | NCT03633110 | Completed | Phase 1, 2 | 24 | Single Arm: GEN-009 (Personalized adjuvanted vaccine) + Nivolumab + Pembro |
| Colorectal Cancer | NCT05238558 | Active, not recruiting | Phase 1 | 16 | Single Arm: FMPV-1 + GM-CSF (as adjuvant) |
| Melanoma, Non-Small-Cell Lung Carcinoma | NCT04990479 | Recruiting | Phase 1 | 34 | Single Arm: Nous-PEV (Personalized vaccine GAd-PEV + MVA-PEV) |
| Diffuse Intrinsic Pontine Glioma (DIPG) or Glioblastoma (GBM) | NCT03914768 | Enrolling by invitation | Phase 1 | 10 | Single Arm: Immunomodulatory DC vaccine to target DIPG and GBM |
| Non-Small-Cell Lung Cancer, Lung cancer, Nonsquamous nonsmall Lung Cancer | NCT03380871 | Completed | Phase 1 | 38 | Single Arm: NEO-PV-01/Adjuvant (personalized vaccine) + pembrolizumab + chemotherapy |
| Colorectal Cancer, Pancreatic Cancer | NCT04117087 | Recruiting | Phase 1 | 30 | Single Arm: KRAS peptide vaccine + Nivolumab + Ipilimumab |
| Melanoma, Non-Small Cell Lung Cancer, Bladder Cancer, Colorectal Cancer, TNBC, Renal Cancer, Head and Neck cancer, Other solid cancers | NCT03289962 | Active, not recruiting | Phase 1 | 272 | Sequential: Autogene Cevumeran + Atezolizumab |
| Diffuse Intrinsic Pontine Glioma, Diffuse Midline Glioma, H3 K27M- Mutant | NCT04943848 | Recruiting | Phase 1 | 36 | Sequential: rHSC-DIPGVax (neoantigen heat shock protein) + Balstilimab + Zalifrelimab |
| Acute Myelogenous Leukemia, Acute Lymphocytic Leukemia, Chronic Myelogenous Leukemia, Myelodysplastic Syndrome, Non-Hodgkin’s lymphoma | NCT00923910 | Completed | Phase 1, 2 | 10 | Single Arm: WT1 Peptide-Pulsed Dendritic Cells + Donor Lymphocytes + IL-4 + KLH + WT1 Peptides + Endotoxin + Diphenydramine + Acetaminophen |
| Metastatic: Colorectal Adenocarcinoma, Pancreatic Ductal Adenocarcinoma; Stage IV: Colorectal Cancer, Pancreatic Cancer; Stage IVA, IVB Colorectal Cancer | NCT02600949 | Recruiting | Phase 1 | 150 | Group 1) personalized vaccine, imiquimod; Group 2) personalized vaccine, imiquimod, pembrolizumab; Group 3,4) personalized vaccine, imiquimod, pembrolizumab, sotigalimab |
| Urinary Bladder Cancer, Transitional Cell Carcinoma of the Bladder. Malignant Melanoma, Melanoma, Skin Cancer, Non Small Cell Lung Cancer, Lung cancer | NCT02897765 | Completed | Phase 1 | 34 | Single Arm: NEO-PV-01 + Nivolumab + Adjuvant |
| Diffuse Intrinsic Pontine Glioma | NCT04749641 | Recruiting | Phase 1 | 30 | Group 1: Stereotactic Biopsy + Histone H3.3-K27M Neoantigen Vaccine; Group 2: Open Biopsy + Histone H3.3-K27M Neoantigen Vaccine |
| Glioblastoma | NCT04015700 | Recruiting | Phase 1 | 12 | Single Arm: Personalized neoantigen DNA vaccine supplied by Geneos Therapeutics + Plasmid encoded IL-12 |
| Glioblastoma | NCT03422094 | Terminated | Phase 1 | 3 | Sequential: NeoVax + Nivolumab + Ipilimumab |
| Melanoma | NCT03929029 | Recruiting | Phase 1 | 20 | Single Arm: Nivolumab + NeoVax plus Montanide + Ipilimumab |
| Melanoma, Ocular Melanoma, Uveal Melanoma | NCT04364230 | Recruiting | Phase 1, 2 | 44 | Single Arm: 6MHP + NeoAg-mBRAF + PolyICLC + CDX-1140 |
| Metastatic Melanoma | NCT03597282 | Terminated | Phase 1 | 22 | Group 1) NEO-PV-01 + adjuvant + nivolumab; Group 2) Nivolumab + adjuvant; Group 3) NEO-PV-01 + adjuvant + nivolumab on alternate schedule; Group 4) NEO-PV-01 + adjuvant + nivolumab + APX005M; Group 5) Nivolumab + APX005M; Group 6) NEO-PV-01 + adjuvant + nivolumab + ipilimumab; Group 7) Nivolumab + ipilimumab |
| Glioblastoma Multiforme of Brain | NCT04968366 | Recruiting | Phase 1 | 10 | Single Arm: Autologous dendritic cells pulsed with multiple neoantigen peptides + Temozolomide adjuvant chemotherapy |
| Melanoma, Metastatic Melanoma | NCT04930783 | Recruiting | Phase 1 | 20 | Single Arm: NEOVAX + CDX-301 + Nivolumab |
| Glioblastoma Multiforme, Astrocytoma, Grade IV | NCT02510950 | Terminated | Phase 1 | 1 | Single Arm: Personalized peptide vaccine + Poly-ICLC + Temozolomide |
| Malignant, Recurrent Glioma | NCT04943718 | Recruiting | Phase 1 | 10 | Single Arm: personalized vaccine |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kye, Y.; Nagineni, L.; Gadad, S.; Ramirez, F.; Riva, H.; Fernandez, L.; Samaniego, M.; Holland, N.; Yeh, R.; Takigawa, K.; et al. The Identification and Clinical Applications of Mutated Antigens in the Era of Immunotherapy. Cancers 2022, 14, 4255. https://doi.org/10.3390/cancers14174255
Kye Y, Nagineni L, Gadad S, Ramirez F, Riva H, Fernandez L, Samaniego M, Holland N, Yeh R, Takigawa K, et al. The Identification and Clinical Applications of Mutated Antigens in the Era of Immunotherapy. Cancers. 2022; 14(17):4255. https://doi.org/10.3390/cancers14174255
Chicago/Turabian StyleKye, Yae, Lokesh Nagineni, Shrikanth Gadad, Fabiola Ramirez, Hannah Riva, Lorena Fernandez, Michelle Samaniego, Nathan Holland, Rose Yeh, Kei Takigawa, and et al. 2022. "The Identification and Clinical Applications of Mutated Antigens in the Era of Immunotherapy" Cancers 14, no. 17: 4255. https://doi.org/10.3390/cancers14174255
APA StyleKye, Y., Nagineni, L., Gadad, S., Ramirez, F., Riva, H., Fernandez, L., Samaniego, M., Holland, N., Yeh, R., Takigawa, K., Dhandayuthapani, S., & Chacon, J. (2022). The Identification and Clinical Applications of Mutated Antigens in the Era of Immunotherapy. Cancers, 14(17), 4255. https://doi.org/10.3390/cancers14174255