
Clinical Outcomes Following Proton and Photon Stereotactic Body Radiation Therapy for Early-Stage Lung Cancer

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Stereotactic Body Radiation Therapy
2.3. Assessments
2.4. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
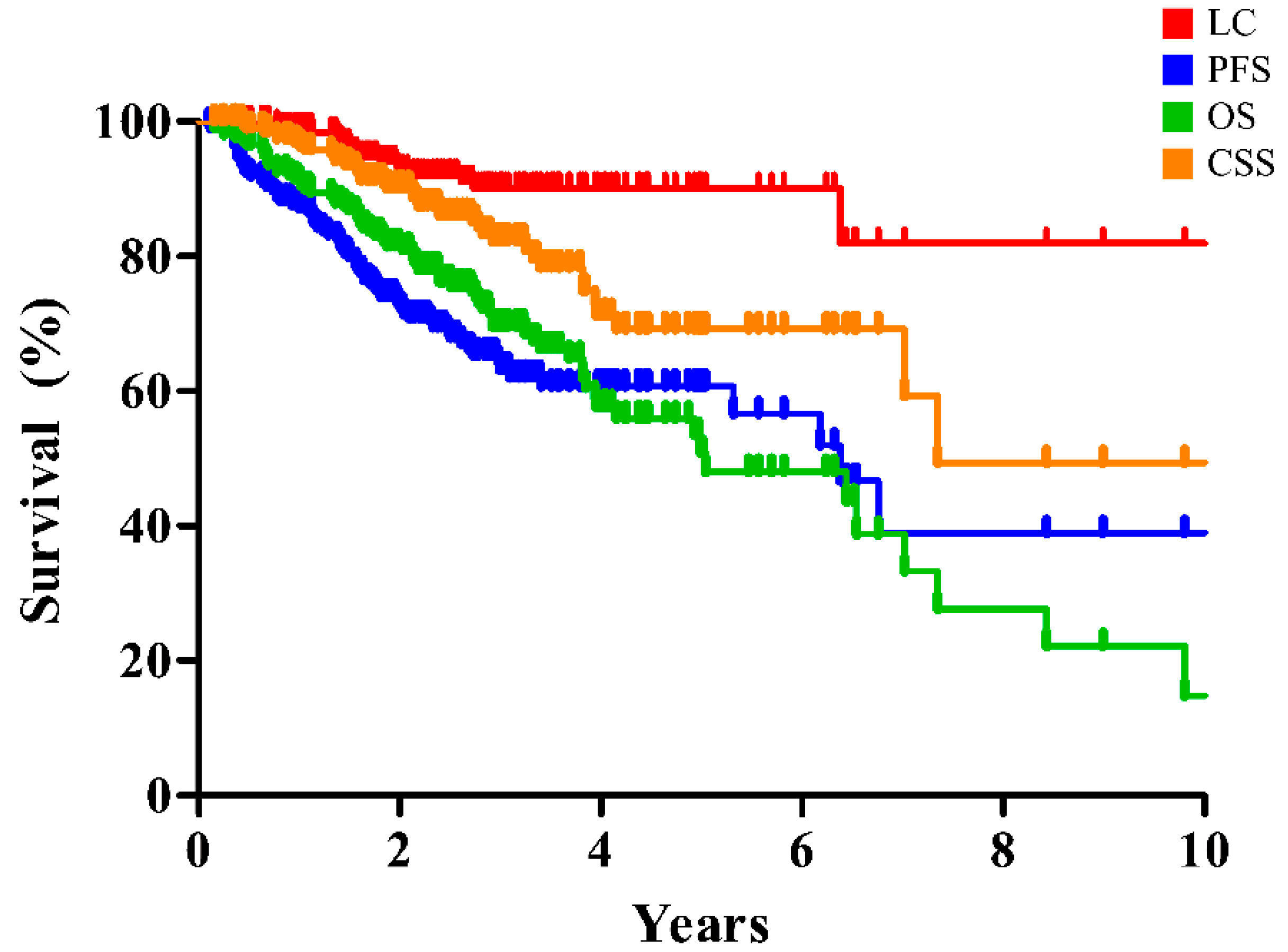
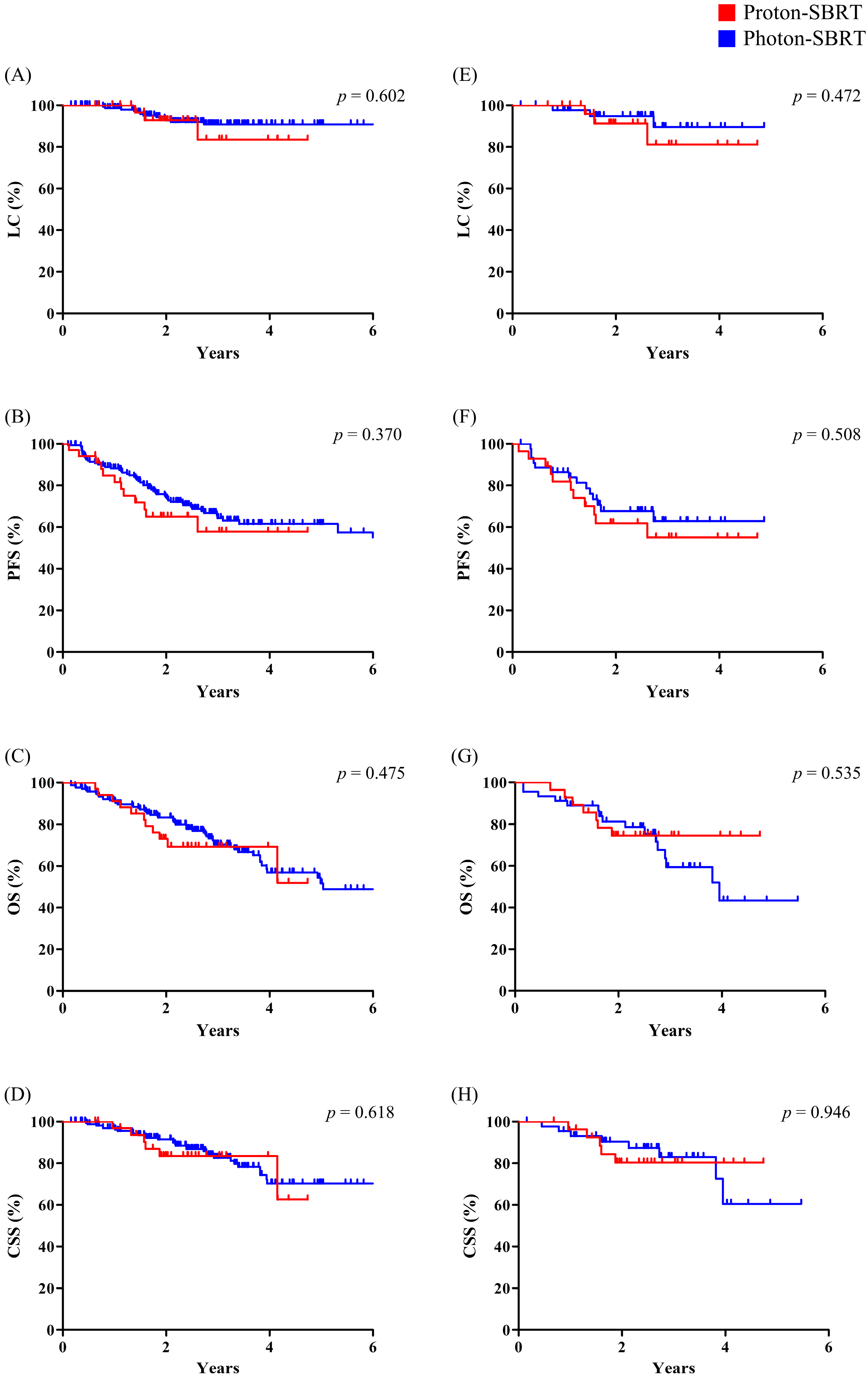
3.2. Survivals
3.3. Toxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bade, B.C.; Cruz, C.S.D. Lung cancer 2020: Epidemiology, etiology, and prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Cilleruelo-Ramos, A.; Cladellas-Gutiérrez, E.; de la Pinta, C.; Quintana-Cortés, L.; Sosa-Fajardo, P.; Couñago, F.; Mielgo-Rubio, X.; Trujillo-Reyes, J.C. Advances and controversies in the management of early stage non-small cell lung cancer. World J. Clin. Oncol. 2021, 12, 1089. [Google Scholar] [CrossRef] [PubMed]
- Shinde, A.; Li, R.; Kim, J.; Salgia, R.; Hurria, A.; Amini, A. Stereotactic body radiation therapy (SBRT) for early-stage lung cancer in the elderly. Semin. Oncol. 2018, 45, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Videtic, G.M.; Donington, J.; Giuliani, M.; Heinzerling, J.; Karas, T.Z.; Kelsey, C.R.; Lally, B.E.; Latzka, K.; Lo, S.S.; Moghanaki, D. Stereotactic body radiation therapy for early-stage non-small cell lung cancer: Executive Summary of an ASTRO Evidence-Based Guideline. Pract. Radiat. Oncol. 2017, 7, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Guckenberger, M.; Andratschke, N.; Dieckmann, K.; Hoogeman, M.S.; Hoyer, M.; Hurkmans, C.; Tanadini-Lang, S.; Lartigau, E.; Mendez Romero, A.; Senan, S.; et al. ESTRO ACROP consensus guideline on implementation and practice of stereotactic body radiotherapy for peripherally located early stage non-small cell lung cancer. Radiother Oncol. 2017, 124, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Liu, K.; Hou, Y.; Cheng, J.; Zhang, J. The evolution of proton beam therapy: Current and future status. Mol. Clin. Oncol. 2018, 8, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Seco, J.; Panahandeh, H.R.; Westover, K.; Adams, J.; Willers, H. Treatment of non-small cell lung cancer patients with proton beam-based stereotactic body radiotherapy: Dosimetric comparison with photon plans highlights importance of range uncertainty. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 354–361. [Google Scholar] [CrossRef]
- Kadoya, N.; Obata, Y.; Kato, T.; Kagiya, M.; Nakamura, T.; Tomoda, T.; Takada, A.; Takayama, K.; Fuwa, N. Dose–volume comparison of proton radiotherapy and stereotactic body radiotherapy for non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1225–1231. [Google Scholar] [CrossRef]
- Georg, D.; Hillbrand, M.; Stock, M.; Dieckmann, K.; Pötter, R. Can protons improve SBRT for lung lesions? Dosimetric considerations. Radiother. Oncol. 2008, 88, 368–375. [Google Scholar] [CrossRef]
- Harada, H.; Murayama, S. Proton beam therapy in non-small cell lung cancer: State of the art. Lung Cancer Targets Ther. 2017, 8, 141. [Google Scholar] [CrossRef] [PubMed]
- Kocak, Z.; Evans, E.S.; Zhou, S.-M.; Miller, K.L.; Folz, R.J.; Shafman, T.D.; Marks, L.B. Challenges in defining radiation pneumonitis in patients with lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 635–638. [Google Scholar] [CrossRef] [PubMed]
- Westover, K.D.; Seco, J.; Adams, J.A.; Lanuti, M.; Choi, N.C.; Engelsman, M.; Willers, H. Proton SBRT for medically inoperable stage I NSCLC. J. Thorac. Oncol. 2012, 7, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.M.; Wang, S. Nondosimetric risk factors for radiation-induced lung toxicity. Semin. Radiat. Oncol. 2015, 25, 100–109. [Google Scholar] [CrossRef]
- Nantavithya, C.; Gomez, D.R.; Wei, X.; Komaki, R.; Liao, Z.; Lin, S.H.; Jeter, M.; Nguyen, Q.-N.; Li, H.; Zhang, X. Phase 2 study of stereotactic body radiation therapy and stereotactic body proton therapy for high-risk, medically inoperable, early-stage non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 558–563. [Google Scholar] [CrossRef]
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef]
- Oh, D.; Ahn, Y.C.; Seo, J.M.; Shin, E.H.; Park, H.C.; Lim, D.H.; Pyo, H. Potentially curative stereotactic body radiation therapy (SBRT) for single or oligometastasis to the lung. Acta. Oncol. 2012, 51, 596–602. [Google Scholar] [CrossRef]
- Hoyer, M.; Roed, H.; Traberg Hansen, A.; Ohlhuis, L.; Petersen, J.; Nellemann, H.; Kiil Berthelsen, A.; Grau, C.; Aage Engelholm, S.; Von der Maase, H. Phase II study on stereotactic body radiotherapy of colorectal metastases. Acta. Oncol. 2006, 45, 823–830. [Google Scholar] [CrossRef]
- Fakiris, A.J.; McGarry, R.C.; Yiannoutsos, C.T.; Papiez, L.; Williams, M.; Henderson, M.A.; Timmerman, R. Stereotactic body radiation therapy for early-stage non-small-cell lung carcinoma: Four-year results of a prospective phase II study. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 677–682. [Google Scholar] [CrossRef]
- Baumann, P.; Nyman, J.; Hoyer, M.; Wennberg, B.; Gagliardi, G.; Lax, I.; Drugge, N.; Ekberg, L.; Friesland, S.; Johansson, K.A.; et al. Outcome in a prospective phase II trial of medically inoperable stage I non-small-cell lung cancer patients treated with stereotactic body radiotherapy. J. Clin. Oncol. 2009, 27, 3290–3296. [Google Scholar] [CrossRef]
- Timmerman, R.; Paulus, R.; Galvin, J.; Michalski, J.; Straube, W.; Bradley, J.; Fakiris, A.; Bezjak, A.; Videtic, G.; Johnstone, D.; et al. Stereotactic body radiation therapy for inoperable early stage lung cancer. JAMA 2010, 303, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, R.D.; Paulus, R.; Pass, H.I.; Gore, E.M.; Edelman, M.J.; Galvin, J.; Straube, W.L.; Nedzi, L.A.; McGarry, R.C.; Robinson, C.G.; et al. Stereotactic Body Radiation Therapy for Operable Early-Stage Lung Cancer: Findings From the NRG Oncology RTOG 0618 Trial. JAMA Oncol. 2018, 4, 1263–1266. [Google Scholar] [CrossRef] [PubMed]
- Nagata, Y.; Kimura, T. Stereotactic body radiotherapy (SBRT) for Stage I lung cancer. Jpn. J. Clin. Oncol. 2018, 48, 405–409. [Google Scholar] [CrossRef]
- Videtic, G.M.; Hu, C.; Singh, A.K.; Chang, J.Y.; Parker, W.; Olivier, K.R.; Schild, S.E.; Komaki, R.; Urbanic, J.J.; Timmerman, R.D.; et al. A Randomized Phase 2 Study Comparing 2 Stereotactic Body Radiation Therapy Schedules for Medically Inoperable Patients With Stage I Peripheral Non-Small Cell Lung Cancer: NRG Oncology RTOG 0915 (NCCTG N0927). Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 757–764. [Google Scholar] [CrossRef]
- Bayasgalan, U.; Moon, S.H.; Kim, T.H.; Kim, T.Y.; Lee, S.H.; Suh, Y.G. Dosimetric Comparisons between Proton Beam Therapy and Modern Photon Radiation Techniques for Stage I Non-Small Cell Lung Cancer According to Tumor Location. Cancers 2021, 13, 6356. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Jabbour, S.K.; De Ruysscher, D.; Schild, S.E.; Simone, C.B., 2nd; Rengan, R.; Feigenberg, S.; Khan, A.J.; Choi, N.C.; Bradley, J.D.; et al. Consensus Statement on Proton Therapy in Early-Stage and Locally Advanced Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 505–516. [Google Scholar] [CrossRef]
- Berg, J.; Ramberg, C.; Haugstvedt, J.O.S.; Bengtson, M.-B.; Gabrielsen, A.-M.; Brustugun, O.T.; Halvorsen, A.R.; Helland, Å. Lung function after stereotactic body radiation therapy for early-stage non-small cell lung cancer, changes and predictive markers. Front. Oncol. 2021, 11, 1829. [Google Scholar] [CrossRef]
- Zhang, X.-J.; Sun, J.-G.; Sun, J.; Ming, H.; Wang, X.-X.; Wu, L.; Chen, Z.-T. Prediction of radiation pneumonitis in lung cancer patients: A systematic review. J. Cancer Res. Clin. Oncol. 2012, 138, 2103–2116. [Google Scholar] [CrossRef]
- Welsh, J.; Thomas, J.; Shah, D.; Allen, P.K.; Wei, X.; Mitchell, K.; Gao, S.; Balter, P.; Komaki, R.; Chang, J.Y. Obesity increases the risk of chest wall pain from thoracic stereotactic body radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 91–96. [Google Scholar] [CrossRef]
- Welsh, J.; Amini, A.; Ciura, K.; Nguyen, N.; Palmer, M.; Soh, H.; Allen, P.K.; Paolini, M.; Liao, Z.; Bluett, J. Evaluating proton stereotactic body radiotherapy to reduce chest wall dose in the treatment of lung cancer. Med. Dosim. 2013, 38, 442–447. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Entire Cohort (N = 202) | Matched Cohort (N = 74) | ||||||
|---|---|---|---|---|---|---|---|
| Overall (n = 202) | Photon SBRT (n = 168) | Proton SBRT (n = 34) | p value | Photon SBRT (n = 46) | Proton SBRT (n = 28) | p value | |
| Age (years, median, IQR) | 75 (70–79) | 76 (70–79) | 72.5 (68–76) | 0.288 | 75 (70–78) | 73 (68–76) | 0.411 |
| Sex | 0.963 | 0.667 | |||||
| Male | 161 (79.7%) | 134 (79.8%) | 27 (79.4%) | 38 (82.6%) | 22 (78.6%) | ||
| Female | 41 (20.3%) | 34 (20.2%) | 7 (20.6%) | 8 (17.4%) | 6 (21.4%) | ||
| ECOG PS | 0.151 | 0.113 | |||||
| 0–1 | 167 (82.7%) | 136 (81.0%) | 31 (91.2%) | 35 (76.1%) | 26 (92.9%) | ||
| 2- | 35 (17.3%) | 32 (19.0%) | 3 (8.8%) | 11 (23.9%) | 2 (7.1%) | ||
| Pathology | 0.241 | 0.589 | |||||
| Adenocarcinoma | 77 (38.1%) | 66 (39.3%) | 11 (32.4%) | 16 (34.8%) | 10 (35.7%) | ||
| Squamous cell carcinoma | 47 (23.3%) | 38 (22.6%) | 9 (26.5%) | 12 (26.1%) | 8 (28.6%) | ||
| Other | 13 (6.4%) | 13 (7.7%) | 0 (0.0%) | 3 (6.5%) | 0 (0.0%) | ||
| Unproven | 65 (32.2%) | 51 (30.4%) | 14 (41.2%) | 15 (32.6%) | 10 (35.7%) | ||
| Location | 0.176 | 0.479 | |||||
| LLL | 34 (16.8%) | 25 (14.9%) | 9 (26.5%) | 5 (10.9%) | 7 (25.0%) | ||
| LUL | 55 (27.2%) | 48 (28.6%) | 7 (20.6%) | 12 (26.1%) | 6 (21.4%) | ||
| RLL | 41 (20.3%) | 31 (18.5%) | 10 (29.4%) | 11 (23.9%) | 8 (28.6%) | ||
| RML | 7 (3.5%) | 6 (3.6%) | 1 (2.9%) | 3 (6.5%) | 1 (3.6%) | ||
| RUL | 65 (32.2%) | 58 (34.5%) | 7 (20.6%) | 15 (32.6%) | 6 (21.4%) | ||
| Tumor size (mm, mean ± SD) | 21.77 ± 8.52 | 21.62 ± 8.22 | 22.50 ± 10.00 | 0.584 | 22.00 ± 9.60 | 23.32 ± 9.96 | 0.573 |
| T stage | 0.178 | 0.667 | |||||
| T1 | 170 (84.2%) | 144 (85.7%) | 26 (76.5%) | 38 (82.6%) | 22 (78.6%) | ||
| T2 | 32 (15.8%) | 24 (14.3%) | 8 (23.5%) | 8 (17.4%) | 6 (21.4%) | ||
| COPD | 85 (42.1%) | 61 (36.3%) | 24 (70.6%) | <0.001 | 25 (54.3%) | 18 (64.3%) | 0.401 |
| COPD GOLD grade | 0.001 | 0.645 | |||||
| Grade 1 | 22 (10.8%) | 18 (10.7%) | 4 (11.8%) | 6 (13.0%) | 3 (10.7%) | ||
| Grade 2 | 46 (22.7%) | 33 (19.6%) | 13 (38.2%) | 13 (28.3%) | 12 (42.9%) | ||
| Grade 3 | 16 (7.9%) | 9 (5.4%) | 7 (20.6%) | 6 (13.0%) | 3 (10.7%) | ||
| Grade 4 | 1 (0.5%) | 1 (0.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | ||
| ILD | 25 (12.4%) | 18 (10.7%) | 7 (20.6%) | 0.149 | 9 (19.6%) | 6 (21.4%) | 0.847 |
| ILD GAP stage | 0.065 | 0.845 | |||||
| Stage 1 | 6 (3.0%) | 6 (3.6%) | 0 (0.0%) | 1 (2.2%) | 0 (0.0%) | ||
| Stage 2 | 17 (8.4%) | 11 (6.5%) | 6 (17.7%) | 7 (15.2%) | 5 (17.9%) | ||
| Stage 3 | 2 (1.0%) | 1 (0.6%) | 1 (2.9%) | 1 (2.2%) | 1 (3.6%) | ||
| Baseline FEV1 (% predicted, mean ± SD) | 77.85 ± 24.74 | 80.19 ± 25.24 | 67.38 ± 19.44 | 0.006 | 71.46 ± 22.71 | 71.25 ± 16.45 | 0.967 |
| Baseline DLCO (% predicted, mean ± SD) | 68.98 ± 22.82 | 72.42 ± 21.87 | 54.52 ± 21.29 | <0.001 | 60.28 ± 17.51 | 57.68 ± 21.40 | 0.571 |
| Operability | <0.001 | 0.001 | |||||
| Operable | 47 (23.3%) | 47 (28.0%) | 0 (0.0%) | 13 (28.3%) | 0 (0.0%) | ||
| Inoperable | 155 (76.7%) | 121 (72.0%) | 34 (100.0%) | 33 (71.7%) | 28 (100.0%) | ||
| SBRT technique | <0.001 | <0.001 | |||||
| 3D-CRT | 130 (64.4%) | 130 (77.4%) | 0 (0.0%) | 29 (63.0%) | 0 (0.0%) | ||
| IMRT | 38 (18.8%) | 38 (22.6%) | 0 (0.0%) | 17 (37.0%) | 0 (0.0%) | ||
| Passive scattering | 4 (2.0%) | 0 (0.0%) | 4 (11.8%) | 0 (0.0%) | 4 (14.3%) | ||
| IMPT | 30 (14.8%) | 0 (0.0%) | 30 (88.2%) | 0 (0.0%) | 24 (85.7%) | ||
| Respiratory motion control | <0.001 | <0.001 | |||||
| Free breathing | 187 (92.6%) | 167 (99.4%) | 20 (58.8%) | 46 (100.0%) | 16 (57.1%) | ||
| Gating | 1 (0.5%) | 0 (0.0%) | 1 (2.9%) | 0 (0.0%) | 1 (3.6%) | ||
| DIBH | 14 (6.9%) | 1 (0.6%) | 13 (38.2%) | 0 (0.0%) | 11 (39.3%) | ||
| Dosimetric parameters | |||||||
| ITV (cc, mean ± SD) | 14.44 ± 18.73 | 13.39 ± 15.07 | 19.44 ± 30.55 | 0.274 | 12.48 ± 13.63 | 19.68 ± 32.38 | 0.189 |
| PTV (cc, mean ± SD) | 38.57 ± 34.74 | 36.00 ± 29.07 | 51.28 ± 53.62 | 0.115 | 34.38 ± 27.77 | 52.61 ± 55.59 | 0.064 |
| Lung V40Gy (%, mean ± SD) | 4.07 ± 2.66 | 4.06 ± 2.72 | 4.12 ± 2.38 | 0.907 | 4.16 ± 3.68 | 4.49 ± 2.40 | 0.674 |
| Lung V20Gy (%, mean ± SD) | 8.74 ± 4.33 | 8.90 ± 4.45 | 7.93 ± 3.61 | 0.233 | 9.28 ± 5.51 | 8.51 ± 3.45 | 0.513 |
| Lung V10Gy (%, mean ± SD) | 13.78 ± 5.52 | 14.28 ± 5.52 | 11.33 ± 4.90 | 0.004 | 14.72 ± 6.09 | 12.07 ± 4.68 | 0.053 |
| Lung V5Gy (%, mean ± SD) | 20.40 ± 7.90 | 21.69 ± 7.61 | 14.04 ± 6.09 | <0.001 | 22.02 ± 7.79 | 14.90 ± 5.86 | <0.001 |
| Entire Cohort (N = 202) | Matched Cohort (N = 74) | |||||||
|---|---|---|---|---|---|---|---|---|
| Overall (n = 202) | Photon SBRT (n = 168) | Proton SBRT (n = 34) | p value | Photon SBRT (n = 46) | Proton SBRT (n = 28) | p value | ||
| LC | 2-year | 92.7% | 92.8% | 92.8% | 0.602 | 94.9% | 91.3% | 0.472 |
| 5-year | 90.1% | 90.8% | 83.6% | 89.6% | 81.1% | |||
| PFS | 2-year | 72.8% | 74.4% | 65.0% | 0.370 | 67.7% | 61.9% | 0.508 |
| 5-year | 60.7% | 61.6% | 57.8% | 62.9% | 55.0% | |||
| OS | 2-year | 81.5% | 83.3% | 73.1% | 0.475 | 81.3% | 74.5% | 0.535 |
| 5-year | 50.8% | 51.7% | 51.9% | 43.4% | 74.5% | |||
| CSS | 2-year | 90.1% | 91.5% | 83.5% | 0.618 | 90.4% | 80.4% | 0.946 |
| 5-year | 69.2% | 70.3% | 62.6% | 60.5% | 80.4% | |||
| Entire Cohort (N = 202) | Matched Cohort (N = 74) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Photon SBRT (n = 168) | Proton SBRT (n = 34) | p value | Photon SBRT (n = 46) | Proton SBRT (n = 28) | p value | |||||||||
| G2 | G3 | G4 | G2 | G3 | G4 | G2 | G3 | G4 | G2 | G3 | G4 | |||
| Radiation pneumonitis | 13 (7.7%) | 20 (11.9%) | 0 (0.0%) | 3 (8.8%) | 6 (17.6%) | 0 (0.0%) | 0.371 * | 3 (6.5%) | 11 (23.9%) | 0 (0.0%) | 3 (10.7%) | 3 (10.7%) | 0 (0.0%) | 0.398 * |
| Musculoskeletal | 17 (10.1%) | 6 (3.6%) | 0 (0.0%) | 2 (5.9%) | 0 (0.0%) | 0 (0.0%) | 0.264 ** | 6 (13.0%) | 1 (2.2%) | 0 (0.0%) | 2 (7.1%) | 0 (0.0%) | 0 (0.0%) | 0.285 ** |
| Skin | 3 (1.8%) | 3 (1.8%) | 1 (0.6%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.604 ** | 2 (4.3%) | 1 (2.2%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.468 ** |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| Sex (Male) | 7.606 (1.002–57.709) | 0.054 | ||
| Age (>70) | 1.400 (0.498–3.934) | 0.523 | ||
| ECOG PS (2 or higher) | 3.054 (1.231–7.580) | 0.016 | 3.162 (1.215–8.226) | 0.018 |
| Smoking History (Yes) | 2.349 (0.669–8.252) | 0.183 | ||
| COPD (Yes) | 1.444 (0.633–3.297) | 0.383 | ||
| ILD (Yes) | 2.479 (0.886–6.937) | 0.084 | ||
| T stage (T2) | 1.731 (0.635–4.718) | 0.284 | ||
| Operability (Inoperable) | 8.846 (1.165–67.144) | 0.035 | 7.204 (0.929–55.863) | 0.059 |
| Baseline FEV1 (<40%) | 3.818 (1.062–13.731) | 0.040 | ||
| Baseline DLCO (<40%) | 4.980 (1.636–15.162) | 0.005 | 3.995 (1.259–12.675) | 0.019 |
| Respiratory motion control (No) | 0.611 (0.162–2.310) | 0.468 | ||
| Treatment modality (Photon) | 0.631 (0.233–1.710) | 0.365 | ||
| Article | Patients | Stage | Dose | Follow-up | LC | OS | Toxicity |
|---|---|---|---|---|---|---|---|
| Hoyer et al. [18] | 40 | Stage I | 45 Gy in 3 fractions | 29 months | 2-year, 85% | 2-year, 47% | Grade ≥ 2, 48% |
| Fakiris et al. [19] | 70 | T1-T2 | 60–66 Gy in 3 fractions | 50 months | 3-year, 88.1% | 3-year, 42.7% | Grade ≥ 3, 15.7% |
| Baumann et al. [20] | 57 | T1-T2 | 45 Gy in 3 fractions | 35 months | 3-year, 92% | 3-year, 60% | Grade ≥ 3, 28% |
| Timmerman et al. [21] | 55 | T1-T2 | 54 Gy in 3 fractions | 34 months | 3-year, 91% | 3-year, 56% | Grade ≥ 3, 16% |
| Timmerman et al. [22] | 33 | T1-T2 | 54 Gy in 3 fractions | 48.1 months | 4-year, 96% | 4-year, 57% | Grade ≥ 3, 8% |
| Nagata et al. [23] | 100 (inoperable) | T1 | 48 Gy in 4 fractions | 47 months | 3-year, 87.3% | 3-year, 59.9% | Grade ≥ 3, 12.5% |
| 64 (operable) | T1 | 48 Gy in 4 fractions | 67 months | 3-year, 85.4% | 3-year, 76.5% | Grade ≥ 3, 6.2% | |
| Videtic et al. [24] | 39 | T1-T2 | 34 Gy in 1 fraction | 3.5 years | 5-year, 89.4% | 5-year, 29.6% | Grade ≥ 3, 2.6% |
| 45 | T1-T2 | 48 Gy in 4 fractions | 4.0 years | 5-year, 93.2% | 5-year, 41.1% | Grade ≥ 3, 11.1% | |
| Current study | 168 (Photon) | T1-T2 | 60 Gy in 4 fractions | 2.7 years | 5-year, 90.8% | 5-year. 51.7% | Grade ≥ 3, 16.7% |
| 34 (Proton) | T1-T2 | 60 Gy in 4 fractions | 2.2 years | 5-year, 83.6% | 5-year, 51.9% | Grade ≥ 3, 17.6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, B.K.; Yang, K.; Noh, J.M.; Pyo, H.; Ahn, Y.C. Clinical Outcomes Following Proton and Photon Stereotactic Body Radiation Therapy for Early-Stage Lung Cancer. Cancers 2022, 14, 4152. https://doi.org/10.3390/cancers14174152
Bae BK, Yang K, Noh JM, Pyo H, Ahn YC. Clinical Outcomes Following Proton and Photon Stereotactic Body Radiation Therapy for Early-Stage Lung Cancer. Cancers. 2022; 14(17):4152. https://doi.org/10.3390/cancers14174152
Chicago/Turabian StyleBae, Bong Kyung, Kyungmi Yang, Jae Myung Noh, Hongryull Pyo, and Yong Chan Ahn. 2022. "Clinical Outcomes Following Proton and Photon Stereotactic Body Radiation Therapy for Early-Stage Lung Cancer" Cancers 14, no. 17: 4152. https://doi.org/10.3390/cancers14174152
APA StyleBae, B. K., Yang, K., Noh, J. M., Pyo, H., & Ahn, Y. C. (2022). Clinical Outcomes Following Proton and Photon Stereotactic Body Radiation Therapy for Early-Stage Lung Cancer. Cancers, 14(17), 4152. https://doi.org/10.3390/cancers14174152