
Contraception and Hormone Replacement Therapy in Healthy Carriers of Germline BRCA1/2 Genes Pathogenic Variants: Results from an Italian Survey

 , , ,
, , ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
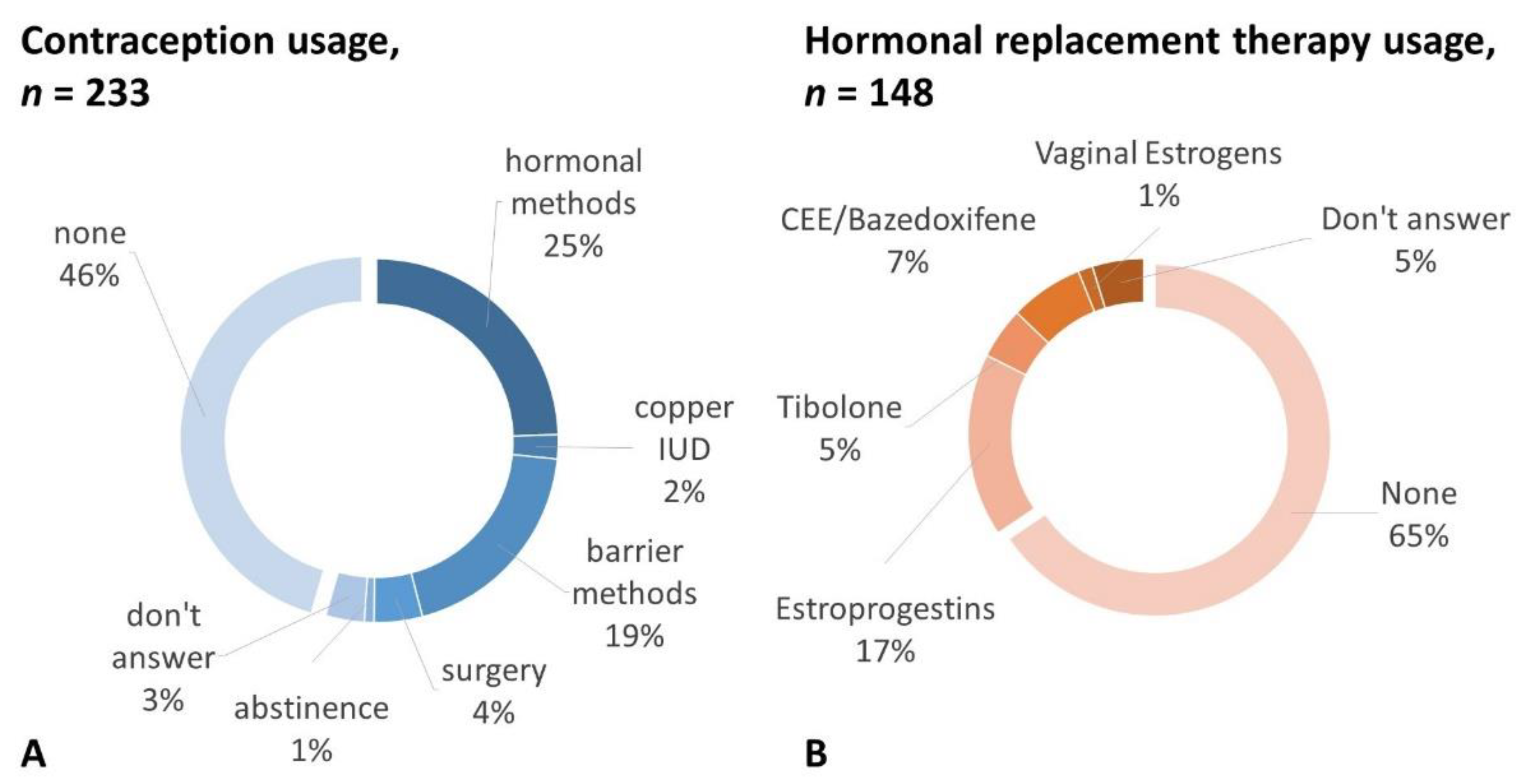
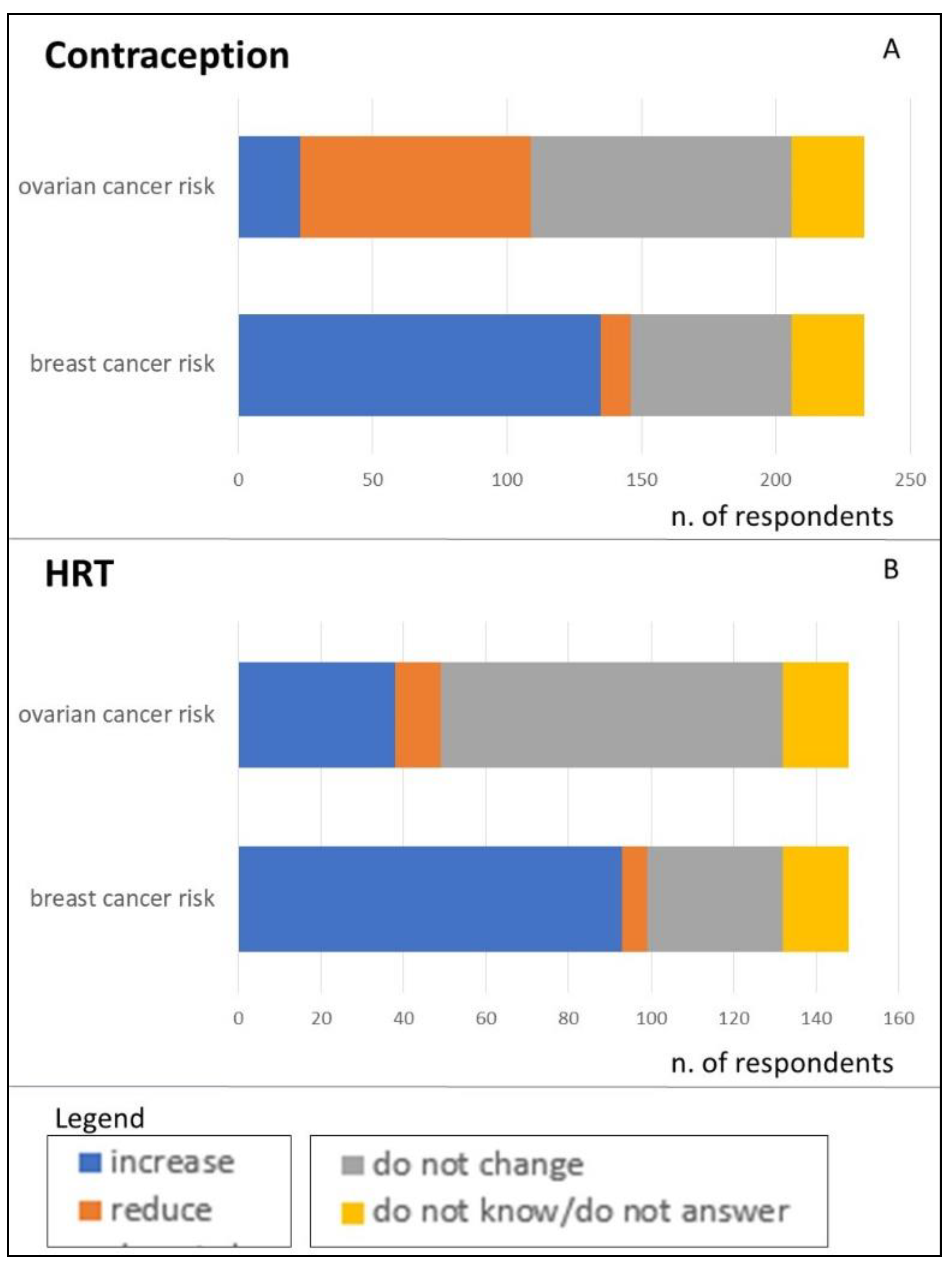
3.2. Contraception
3.3. Menopause
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; Van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paluch-Shimon, S.; Cardoso, F.; Sessa, C.; Balmana, J.; Cardoso, M.J.; Gilbert, F.; Senkus, E. ESMO Guidelines Committee. Prevention and screening in BRCA mutation carriers and other breast/ovarian hereditary cancer syndromes: ESMO Clinical Practice Guidelines for cancer prevention and screening. Ann. Oncol. 2016, 27, v103–v110. [Google Scholar] [CrossRef] [PubMed]
- González-Santiago, S.E.; Ramon y Cajal, T.; Aguirre, E.; Alés-Martínez, J.E.; Andrés, R.; Balmaña, J.; Graña, B.; Herrero, A.; Llort, G.; González-del-Alba, A.; et al. SEOM clinical guidelines in hereditary breast and ovarian cancer (2019). Clin. Transl. Oncol. 2020, 22, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Practice Bulletin No 182: Hereditary Breast and Ovarian Cancer Syndrome. Obstet. Gynecol. 2017, 130, e110–e126. [CrossRef] [PubMed]
- Buonomo, B.; Massarotti, C.; Dellino, M.; Anserini, P.; Ferrari, A.; Campanella, M.; Magnotti, M.; De Stefano, C.; Peccatori, F.A.; Lambertini, M.; et al. Reproductive issues in carriers of germline pathogenic variants in the BRCA1/2 genes: An expert meeting. BMC Med. 2021, 19, 205. [Google Scholar] [CrossRef]
- Grandi, G.; Caroli, M.; Cortesi, L.; Toss, A.; Tazzioli, G.; Facchinetti, F. Postmenopausal hormone therapy in BRCA gene mutation carriers: To whom and which? Expert Opin. Drug Saf. 2020, 19, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Doren, A.; Vecchiola, A.; Aguirre, B.; Villaseca, P. Gynecological–endocrinological aspects in women carriers of BRCA1/2 gene mutations. Climacteric 2018, 21, 529–535. [Google Scholar] [CrossRef]
- Huber, D.; Seitz, S.; Kast, K.; Emons, G.; Ortmann, O. Use of oral contraceptives in BRCA mutation carriers and risk for ovarian and breast cancer: A systematic review. Arch. Gynecol. Obstet. 2020, 301, 875–884. [Google Scholar] [CrossRef]
- European Society for Human Reproduction and Embryology (ESHRE) Guideline Group on POI; Webber, L.; Davies, M.; Anderson, R.; Bartlett, J.; Braat, D.; Cartwright, B.; Cifkova, R.; de Muinck Keizer-Schrama, S.; Hogervorst, E.; et al. ESHRE Guideline: Management of women with premature ovarian insufficiency. Hum. Reprod. 2016, 31, 926–937. [Google Scholar]
- Rocca, W.A.; Grossardt, B.R.; de Andrade, M.; Malkasian, G.D.; Melton, L.J., 3rd. Survival patterns after oophorectomy in premenopausal women: A population-based cohort study. Lancet Oncol. 2006, 7, 821–828. [Google Scholar] [CrossRef]
- Smith, M.J.; Gerber, D.; Olsen, A.; Khouri, O.R.; Wang, Y.; Liu, M.; Smith, J.; Pothuri, B. Uptake and timing of risk-reducing salpingo-oophorectomy among patients with BRCA1 and BRCA2 mutations. Am. J. Obstet. Gynecol. 2021, 225, 508.e1–508.e10. [Google Scholar] [CrossRef] [PubMed]
- Huber, D.; Seitz, S.; Kast, K.; Emons, G.; Ortmann, O. Hormone replacement therapy in BRCA mutation carriers and risk of ovarian, endometrial, and breast cancer: A systematic review. J. Cancer Res. Clin. Oncol. 2021, 147, 2035–2045. [Google Scholar] [CrossRef] [PubMed]
- Eisen, A.; Lubinski, J.; Gronwald, J.; Moller, P.; Lynch, H.T.; Klijn, J.; Kim-Sing, C.; Neuhausen, S.L.; Gilbert, L.; Ghadirian, P.; et al. Hormone therapy and the risk of breast cancer in BRCA1 mutation carriers. J. Natl. Cancer Inst. 2008, 100, 1361–1367. [Google Scholar] [CrossRef] [Green Version]
- Johansen, N.; Liavaag, A.H.; Iversen, O.E.; Dørum, A.; Braaten, T.; Michelsen, T.M. Use of hormone replacement therapy after risk-reducing salpingo-oophorectomy. Acta Obstet. Gynecol. Scand. 2017, 96, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Borrego, R.; Sánchez-Prieto, M. What are the mechanisms of action of the different contraceptive methods to reduce the risk of ovarian cancer? Eur. J. Contracept. Reprod. Health Care 2021, 26, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Moorman, P.G.; Havrilesky, L.J.; Gierisch, J.M.; Coeytaux, R.R.; Lowery, W.J.; Peragallo Urrutia, R.; Dinan, M.; McBroom, A.J.; Hasselblad, V.; Sanders, G.D.; et al. Oral contraceptives and risk of ovarian cancer and breast cancer among high-risk women: A systematic review and meta-analysis. J. Clin. Oncol. 2013, 31, 4188–4198. [Google Scholar] [CrossRef] [PubMed]
- Kotsopoulos, J.; Gronwald, J.; Karlan, B.Y.; Huzarski, T.; Tung, N.; Moller, P.; Armel, S.; Lynch, H.T.; Senter, L.; Eisen, A.; et al. Hormone replacement therapy after oophorectomy and breast cancer risk among BRCA1 mutation carriers. JAMA Oncol. 2018, 4, 1059–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebbeck, T.R.; Friebel, T.; Wagner, T.; Lynch, H.T.; Garber, J.E.; Daly, M.B.; Isaacs, C.; Olopade, O.I.; Neuhausen, S.L.; Eeles, R.; et al. Effect of short-term hormone replacement therapy on breast cancer risk reduction after bilateral prophylactic oophorectomy in BRCA1 and BRCA2 mutation carriers: The PROSE Study Group. J. Clin. Oncol. 2005, 23, 7804–7810. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, C.; De Felice, F.; Boccia, S.; Sassu, C.; Di Donato, V.; Perniola, G.; Palaia, I.; Monti, M.; Muzii, L.; Tombolini, V.; et al. Hormone replacement therapy after prophylactic risk-reducing salpingo-oophorectomy and breast cancer risk in BRCA1 and BRCA2 mutation carriers: A meta-analysis. Crit. Rev. Oncol. Hematol. 2018, 132, 111–115. [Google Scholar] [CrossRef]
- Cagnacci, A.; Gambacciani, M.; Gallo, M.; Lello, S.; Executive Committee of the Italian Society of Menopause (SIM) and of the Italian Society of Gynecology of the Third Age (SIGiTE). Recommendations on menopausal hormone replacement therapy. Minerva Ginecol. 2019, 71, 395–403. [Google Scholar] [CrossRef]
- Somboonporn, W.; Panna, S.; Temtanakitpaisan, T.; Kaewrudee, S.; Soontrapa, S. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal women: Systematic review and meta-analysis. Menopause 2011, 18, 1060–1066. [Google Scholar] [CrossRef] [PubMed]
- Gordhandas, S.; Norquist, B.M.; Pennington, K.P.; Yung, R.L.; Laya, M.B.; Swisher, E.M. Hormone replacement therapy after risk reducing salpingo-oophorectomy in patients with BRCA1 or BRCA2 mutations; a systematic review of risks and benefits. Gynecol. Oncol. 2019, 153, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Henry, D.A.; Lee, M.C.; Almanza, D.; Ahmed, K.A.; Sun, W.; Boulware, D.C.; Laronga, C. Trends in use of bilateral prophylactic mastectomy vs high-risk surveillance in unaffected carriers of inherited breast cancer syndromes in the Inherited Cancer Registry (ICARE). Breast Cancer Res. Treat. 2019, 174, 39–45. [Google Scholar] [CrossRef] [PubMed]
- European Parliamentary Forum for Sexual & Reproductive Rights (EPF). European Contraception Policy Atlas. 2020. Available online: https://www.epfweb.org/node/669 (accessed on 15 November 2021).
- Istituto Superiore di Sanità (ISS). Terapia Ormonale Post-Menopausale e Informazione alle Donne: Risultato di un Percorso di Ricerca. 2011. Available online: https://www.epicentro.iss.it/focus/ormoni/ConMe2011 (accessed on 8 July 2022).



{kind=link}
{kind=link}
| Age, years | 40.8 ± 8.6 (18–62) |
| Education, n (%) | |
| < High school | 16 (6.8) |
| High school degree | 90 (38.1) |
| University or higher | 130 (55.1) |
| Having children, n (%) | |
| Yes | 163 (69.1) |
| No | 73 (30.9) |
| Age at healthy carrier status diagnosis, years | 35.8 ± 8.8 (17–56) |
| BRCA1, n. (%) | 137 (58.1) |
| BRCA2, n. (%) | 99 (41.9) |
| Region, n. (%) | |
| North Italy | 124 (52.5) |
| Central Italy | 59 (25) |
| South Italy | 36 (15.3) |
| Islands | 17 (7.2) |
| Access to a fertility unit, n. (%) | |
| Yes | 124 (54.5) |
| No | 83 (35.2) |
| Don’t know/no answer | 29 (12.3) |
| Risk-reducing surgery, n. (%) | |
| Mastectomy only | 43 (18.2) |
| RRSO only | 42 (17.8) |
| Both | 89 (37.7) |
| None | 62 (26.3) |
| Age at mastectomy, years | 39.6 ± 6.8 (22–57) |
| Age at RRSO, years | 42.9 ± 5.5 (28–57) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massarotti, C.; Buonomo, B.; Dellino, M.; Campanella, M.; De Stefano, C.; Ferrari, A.; Anserini, P.; Lambertini, M.; Peccatori, F.A. Contraception and Hormone Replacement Therapy in Healthy Carriers of Germline BRCA1/2 Genes Pathogenic Variants: Results from an Italian Survey. Cancers 2022, 14, 3457. https://doi.org/10.3390/cancers14143457
Massarotti C, Buonomo B, Dellino M, Campanella M, De Stefano C, Ferrari A, Anserini P, Lambertini M, Peccatori FA. Contraception and Hormone Replacement Therapy in Healthy Carriers of Germline BRCA1/2 Genes Pathogenic Variants: Results from an Italian Survey. Cancers. 2022; 14(14):3457. https://doi.org/10.3390/cancers14143457
Chicago/Turabian StyleMassarotti, Claudia, Barbara Buonomo, Miriam Dellino, Maria Campanella, Cristofaro De Stefano, Alberta Ferrari, Paola Anserini, Matteo Lambertini, and Fedro A. Peccatori. 2022. "Contraception and Hormone Replacement Therapy in Healthy Carriers of Germline BRCA1/2 Genes Pathogenic Variants: Results from an Italian Survey" Cancers 14, no. 14: 3457. https://doi.org/10.3390/cancers14143457
APA StyleMassarotti, C., Buonomo, B., Dellino, M., Campanella, M., De Stefano, C., Ferrari, A., Anserini, P., Lambertini, M., & Peccatori, F. A. (2022). Contraception and Hormone Replacement Therapy in Healthy Carriers of Germline BRCA1/2 Genes Pathogenic Variants: Results from an Italian Survey. Cancers, 14(14), 3457. https://doi.org/10.3390/cancers14143457