
In Early Breast Cancer, the Ratios of Neutrophils, Platelets and Monocytes to Lymphocytes Significantly Correlate with the Presence of Subsets of Circulating Tumor Cells but Not with Disseminated Tumor Cells


Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Clinical Characteristics of Patients
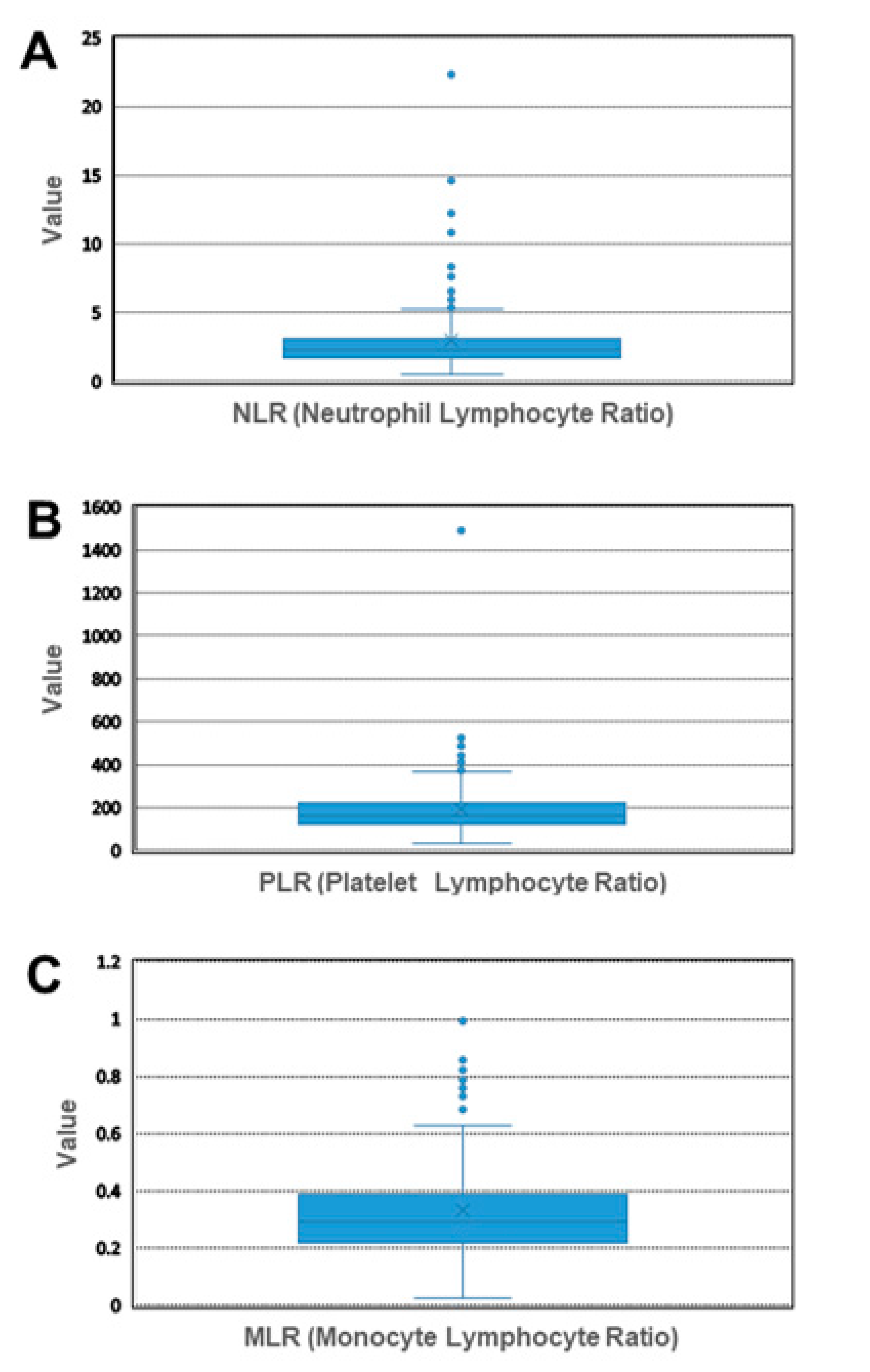
2.2. Establishment of Cut-Off Values
2.3. Correlation of NLR, PLR and MLR with Clinical Characteristics
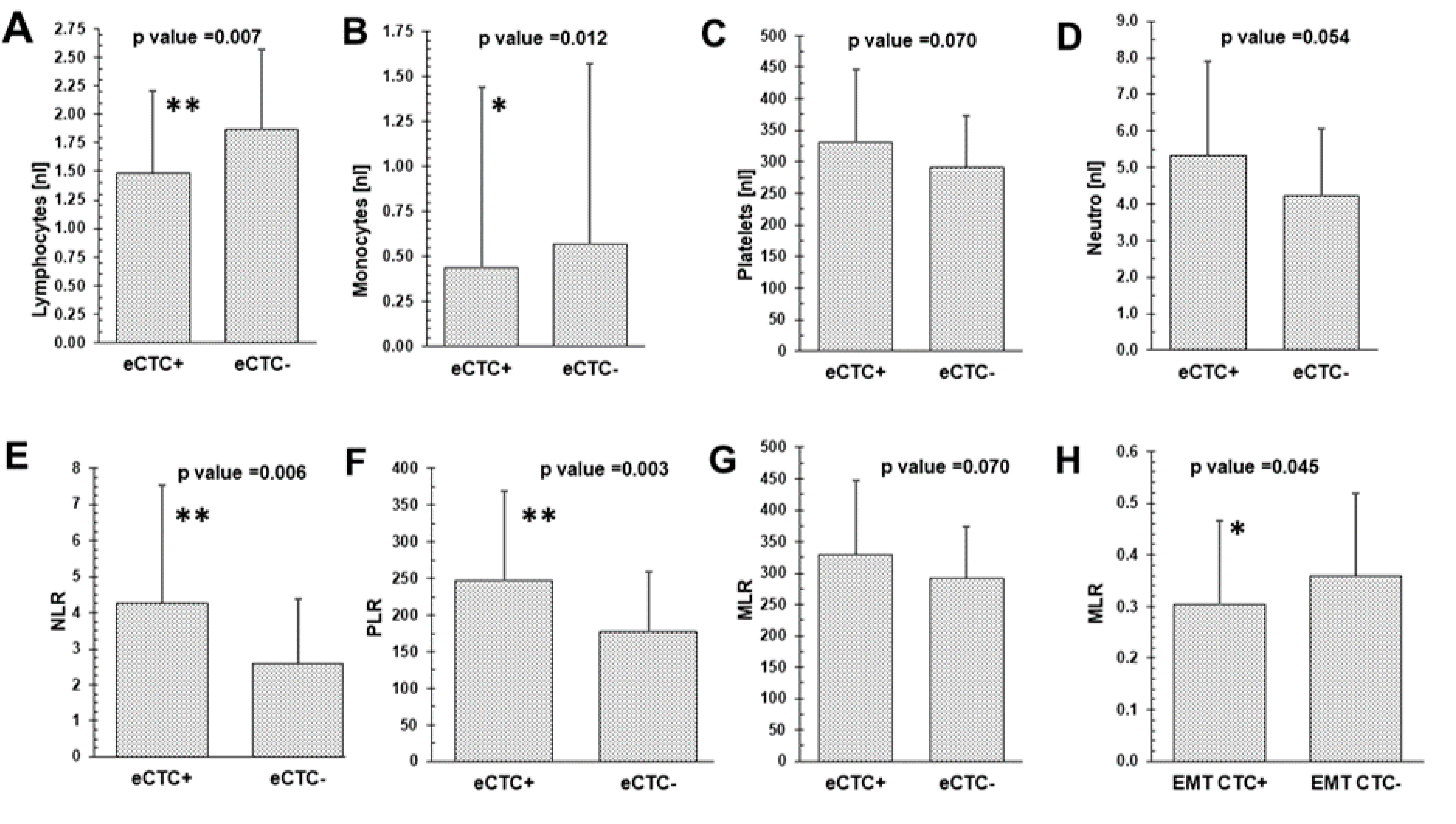
2.4. Mean Differences of CTC Subtypes, DTCs and Blood Values
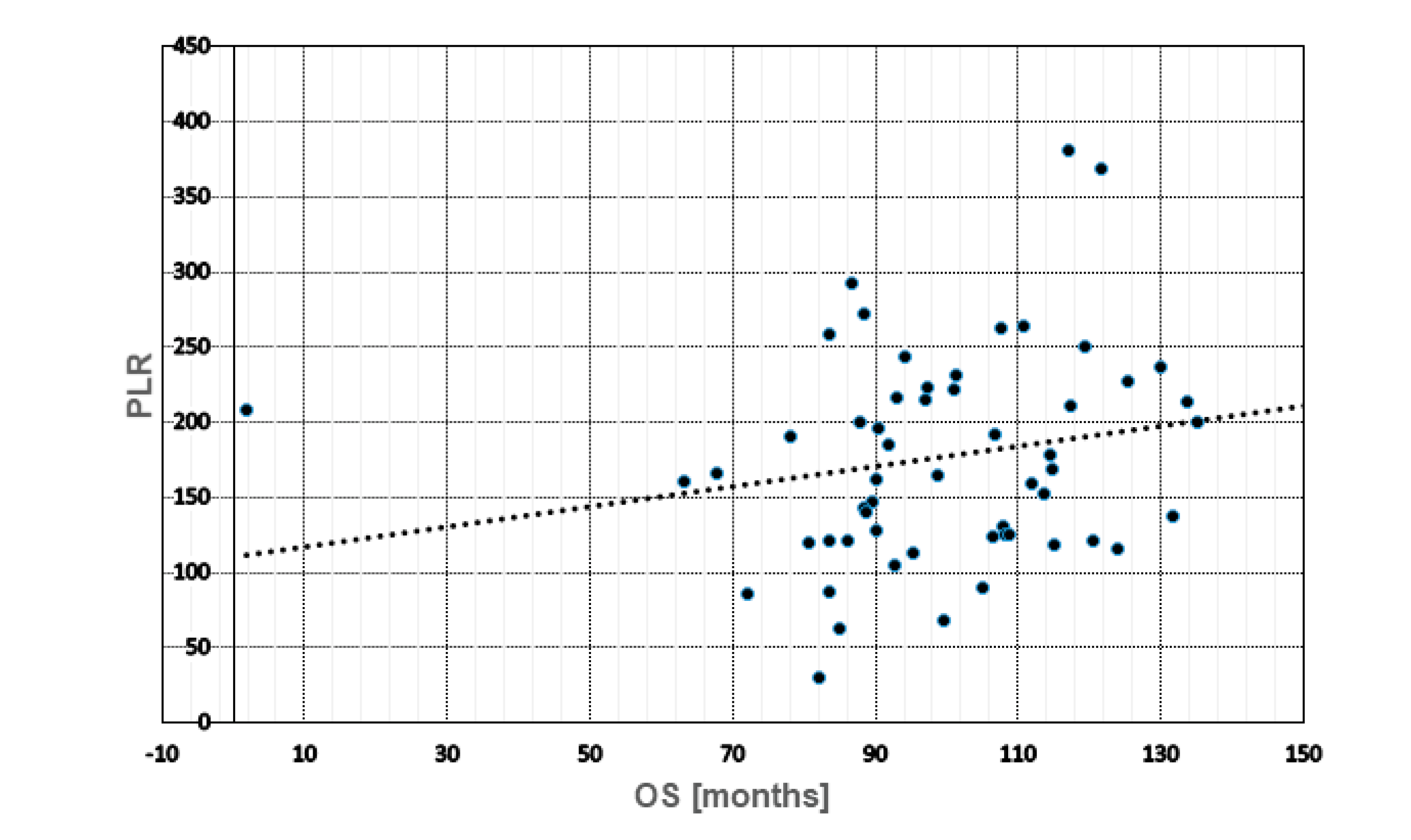
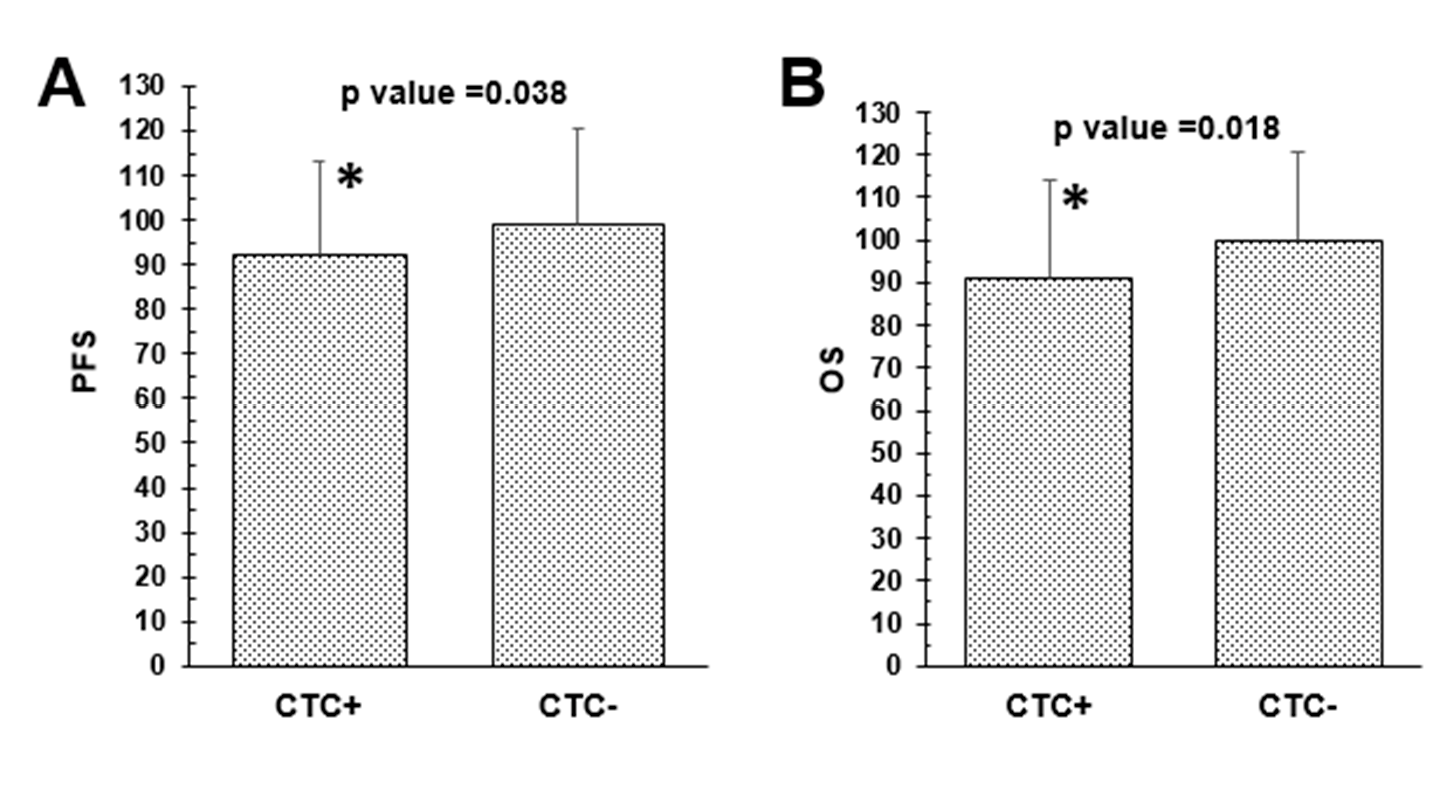
2.5. Prognostic Role of Blood Cell Counts, Ratios, CTCs and DTCs
2.6. Prognostic Value of CTCs, DTCs in Combination with NLR, PLR and MLR
2.7. Univariate and Multivariate Analysis
3. Discussion
4. Patients and Methods
4.1. Study Population
4.2. Selection and Detection of CTCs
4.3. Selection and Detection of DTCs
4.4. Statistical Analysis
5. Limitations of the Study and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harbeck, N.; Gnant, M. Breast cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef]
- Hosseini, H.; Obradović, M.M.S.; Hoffmann, M.; Harper, K.L.; Sosa, M.S.; Werner-Klein, M.; Nanduri, S.L.K.; Werno, C.; Ehrl, C.; Maneck, M.; et al. Early dissemination seeds metastasis in breast cancer. Nature 2016, 540, 552–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantel, K.; Hayes, D.F. Disseminated breast tumour cells: Biological and clinical meaning. Nat. Rev. Clin. Oncol. 2017, 15, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Hartkopf, A.D.; Brucker, S.Y.; Taran, F.-A.; Harbeck, N.; von Au, A.; Naume, B.; Pierga, J.-Y.; Hoffmann, O.; Beckmann, M.W.; Rydén, L.; et al. Disseminated tumour cells from the bone marrow of early breast cancer patients: Results from an international pooled analysis. Eur. J. Cancer 2021, 154, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Schochter, F.; Friedl, T.W.P.; Degregorio, A.; Krause, S.; Huober, J.; Rack, B.; Janni, W. Are Circulating Tumor Cells (CTCs) Ready for Clinical Use in Breast Cancer? An Overview of Completed and Ongoing Trials Using CTCs for Clinical Treatment Decisions. Cells 2019, 8, 1412. [Google Scholar] [CrossRef] [Green Version]
- Vasseur, A.; Kiavue, N.; Bidard, F.-C.; Pierga, J.-Y.; Cabel, L. Clinical utility of circulating tumor cells: An update. Mol. Oncol. 2021, 15, 1647–1666. [Google Scholar] [CrossRef]
- Cortés-Hernández, L.E.; Eslami, S.Z.; Alix-Panabières, C. Circulating tumor cell as the functional aspect of liquid biopsy to understand the metastatic cascade in solid cancer. Mol. Asp. Med. 2019, 72, 100816. [Google Scholar] [CrossRef]
- Balic, M.; Lin, H.; Young, L.; Hawes, D.; Giuliano, A.; McNamara, G.; Datar, R.H.; Cote, R.J. Most Early Disseminated Cancer Cells Detected in Bone Marrow of Breast Cancer Patients Have a Putative Breast Cancer Stem Cell Phenotype. Clin. Cancer Res. 2006, 12, 5615–5621. [Google Scholar] [CrossRef] [Green Version]
- Reuben, J.M.; Lee, B.-N.; Gao, H.; Cohen, E.N.; Mego, M.; Giordano, A.; Wang, X.; Lodhi, A.; Krishnamurthy, S.; Hortobagyi, G.N.; et al. Primary breast cancer patients with high risk clinicopathologic features have high percentages of bone marrow epithelial cells with ALDH activity and CD44+CD24lo cancer stem cell phenotype. Eur. J. Cancer 2011, 47, 1527–1536. [Google Scholar] [CrossRef] [Green Version]
- Kallergi, G.; Hoffmann, O.; Bittner, A.-K.; Papadimitriou, L.; Katsarou, S.D.; Zacharopoulou, N.; Zervakis, M.; Sfakianakis, S.; Stournaras, C.; Georgoulias, V.; et al. CXCR4 and JUNB double-positive disseminated tumor cells are detected frequently in breast cancer patients at primary diagnosis. Ther. Adv. Med Oncol. 2020, 12, 1758835919895754. [Google Scholar] [CrossRef]
- Kolb, A.D.; Shupp, A.B.; Mukhopadhyay, D.; Marini, F.C.; Bussard, K.M. Osteoblasts are “educated” by crosstalk with metastatic breast cancer cells in the bone tumor microenvironment. Breast Cancer Res. 2019, 21, 31. [Google Scholar] [CrossRef] [Green Version]
- Corbeau, I.; Jacot, W.; Guiu, S. Neutrophil to Lymphocyte Ratio as Prognostic and Predictive Factor in Breast Cancer Patients: A Systematic Review. Cancers 2020, 12, 958. [Google Scholar] [CrossRef]
- Ng, M.S.F.; Tan, L.; Wang, Q.; Mackay, C.R.; Ng, L.G. Neutrophils in cancer—unresolved questions. Sci. China Life Sci. 2021, 64, 1829–1841. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; Dong, L.; Cheng, L. Neutrophils in cancer carcinogenesis and metastasis. J. Hematol. Oncol. 2021, 14, 173. [Google Scholar] [CrossRef] [PubMed]
- Morimoto-Kamata, R.; Yui, S. Insulin-like growth factor-1 signaling is responsible for cathepsin G-induced aggregation of breast cancer MCF -7 cells. Cancer Sci. 2017, 108, 1574–1583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczerba, B.M.; Castro-Giner, F.; Vetter, M.; Krol, I.; Gkountela, S.; Landin, J.; Scheidmann, M.C.; Donato, C.; Scherrer, R.; Singer, J.; et al. Neutrophils escort circulating tumour cells to enable cell cycle progression. Nature 2019, 566, 553–557. [Google Scholar] [CrossRef]
- Najmeh, S.; Cools-Lartigue, J.; Rayes, R.F.; Gowing, S.; Vourtzoumis, P.; Bourdeau, F.; Giannias, B.; Berube, J.; Rousseau, S.; Ferri, L.E.; et al. Neutrophil extracellular traps sequester circulating tumor cells via β1-integrin mediated interactions. Int. J. Cancer 2017, 140, 2321–2330. [Google Scholar] [CrossRef] [Green Version]
- Albrengues, J.; Shields, M.A.; Ng, D.; Park, C.G.; Ambrico, A.; Poindexter, M.E.; Upadhyay, P.; Uyeminami, D.L.; Pommier, A.; Küttner, V.; et al. Neutrophil extracellular traps produced during inflammation awaken dormant cancer cells in mice. Science 2018, 361, 4227. [Google Scholar] [CrossRef] [Green Version]
- De Giorgi, U.; Mego, M.; Scarpi, E.; Giordano, A.; Giuliano, M.; Valero, V.; Alvarez, R.H.; Ueno, N.T.; Cristofanilli, M.; Reuben, J.M. Association between circulating tumor cells and peripheral blood monocytes in metastatic breast cancer. Ther. Adv. Med Oncol. 2019, 11, 1758835919866065. [Google Scholar] [CrossRef] [Green Version]
- Miklikova, S.; Minarik, G.; Sedlackova, T.; Plava, J.; Cihova, M.; Jurisova, S.; Kalavska, K.; Karaba, M.; Benca, J.; Smolkova, B.; et al. Inflammation-Based Scores Increase the Prognostic Value of Circulating Tumor Cells in Primary Breast Cancer. Cancers 2020, 12, 1134. [Google Scholar] [CrossRef]
- Thery, L.; Meddis, A.; Cabel, L.; Proudhon, C.; Latouche, A.; Pierga, J.-Y.; Bidard, F.-C. Circulating Tumor Cells in Early Breast Cancer. JNCI Cancer Spectr. 2019, 3, pkz026. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, O.; Aktas, B.; Goldnau, C.; Heubner, M.; Oberhoff, C.; Kimmig, R.; Kasimir-Bauer, S. Effect of ibandronate on disseminated tumor cells in the bone marrow of patients with primary breast cancer: A pilot study. Anticancer Res. 2011, 31, 3623–3628. [Google Scholar] [PubMed]
- Hoffmann, O.; Schroer-Zuendorf, I.A.; Kasimir-Bauer, S.; Oberhoff, C.; Kimmig, R.; Heubner, M. Evaluation of the prognostic significance of disseminated tumor cells in the bone marrow of primary, non-metastatic breast cancer patients after a 7-year follow-up. Arch. Gynecol. Obstet. 2015, 292, 1117–1125. [Google Scholar] [CrossRef] [PubMed]
- Kasimir-Bauer, S.; Bittner, A.-K.; König, L.; Reiter, K.; Keller, T.; Kimmig, R.; Hoffmann, O. Does primary neoadjuvant systemic therapy eradicate minimal residual disease? Analysis of disseminated and circulating tumor cells before and after therapy. Breast Cancer Res. 2016, 18, 1–15. [Google Scholar] [CrossRef]
- Kasimir-Bauer, S.; Reiter, K.; Aktas, B.; Bittner, A.-K.; Weber, S.; Keller, T.; Kimmig, R.; Hoffmann, O. Different prognostic value of circulating and disseminated tumor cells in primary breast cancer: Influence of bisphosphonate intake? Sci. Rep. 2016, 6, 26355. [Google Scholar] [CrossRef] [Green Version]
- Heeke, S.; Mograbi, B.; Alix-Panabières, C.; Hofman, P. Never Travel Alone: The Crosstalk of Circulating Tumor Cells and the Blood Microenvironment. Cells 2019, 8, 714. [Google Scholar] [CrossRef] [Green Version]
- Leone, K.; Poggiana, C.; Zamarchi, R. The Interplay between Circulating Tumor Cells and the Immune System: From Immune Escape to Cancer Immunotherapy. Diagnostics 2018, 8, 59. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Deng, Q.; Pan, Y.; He, B.; Ying, H.; Sun, H.; Liu, X.; Wang, S. Prognostic value of neutrophil-to-lymphocyte ratio in breast cancer. FEBS Open Bio. 2015, 5, 502–507. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Qu, J.-K.; Zhang, J.; Yan, Y.; Zhao, X.-X.; Wang, J.-Z.; Qu, H.-Y.; Liu, L.; Wang, J.-S.; Duan, X.-Y. Prognostic role of pretreatment neutrophil to lymphocyte ratio in breast cancer patients: A meta-analysis. Medicine 2017, 96, e8101. [Google Scholar] [CrossRef]
- Hernández, C.M.; Madrona, A.P.; Gil Vázquez, P.J.; Fernández, P.J.G.; Merino, G.R.; Romero, J.L.A.; Paricio, P.P. Usefulness of lymphocyte-to-monocyte, neutrophil-to-monocyte and neutrophil-to-lymphocyte ratios as prognostic markers in breast cancer patients treated with neoadjuvant chemotherapy. Clin. Transl. Oncol. 2017, 20, 476–483. [Google Scholar] [CrossRef]
- Peng, Y.; Chen, R.; Qu, F.; Ye, Y.; Fu, Y.; Tang, Z.; Wang, Y.; Zong, B.; Yu, H.; Luo, F.; et al. Low pretreatment lymphocyte/monocyte ratio is associated with the better efficacy of neoadjuvant chemotherapy in breast cancer patients. Cancer Biol. Ther. 2019, 21, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Zhang, J.; Chen, X. Lymphocyte-to-Monocyte Ratio is Associated with the Poor Prognosis of Breast Cancer Patients Receiving Neoadjuvant Chemotherapy. Cancer Manag. Res. 2021, 13, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Dong, J.; Sun, Q.; Lu, N.; Pan, Y.; Han, X. Role of neutrophil-to-lymphocyte ratio as a prognostic biomarker in patients with breast cancer receiving neoadjuvant chemotherapy: A meta-analysis. BMJ Open 2021, 11, e047957. [Google Scholar] [CrossRef]
- Ethier, J.-L.; Desautels, D.; Templeton, A.; Shah, P.S.; Amir, E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: A systematic review and meta-analysis. Breast Cancer Res. 2017, 19, 2. [Google Scholar] [CrossRef] [Green Version]
- Geng, S.-K.; Fu, S.-M.; Fu, Y.-P.; Zhang, H.-W. Neutrophil to lymphocyte ratio is a prognostic factor for disease free survival in patients with breast cancer underwent curative resection. Medicine 2018, 97, e11898. [Google Scholar] [CrossRef] [PubMed]
- Orditura, M.; Galizia, G.; Diana, A.; Saccone, C.; Cobellis, L.; Ventriglia, J.; Iovino, F.; Romano, C.; Morgillo, F.; Mosca, L.; et al. Neutrophil to lymphocyte ratio (NLR) for prediction of distant metastasis-free survival (DMFS) in early breast cancer: A propensity score-matched analysis. ESMO Open 2016, 1, e000038. [Google Scholar] [CrossRef] [Green Version]
- Huszno, J.; Kolosza, Z. Prognostic value of the neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratio in breast cancer patients. Oncol. Lett. 2019, 18, 6275–6283. [Google Scholar] [CrossRef]
- Koh, C.-H.; Bhoopathy, N.; Ng, K.-L.; Jabir, R.S.; Tan, G.-H.; See, M.H.; Jamaris, S.; Taib, N.A. Utility of pre-treatment neutrophil–lymphocyte ratio and platelet–lymphocyte ratio as prognostic factors in breast cancer. Br. J. Cancer 2015, 113, 150–158. [Google Scholar] [CrossRef]
- Wen, J.; Ye, F.; Huang, X.; Li, S.; Yang, L.; Xiao, X.; Xie, X. Prognostic Significance of Preoperative Circulating Monocyte Count in Patients with Breast Cancer: Based on a Large Cohort Study. Medicine 2015, 94, e2266. [Google Scholar] [CrossRef]
- Zheng, L.; Zou, K.; Yang, C.; Chen, F.; Guo, T.; Xiong, B. Inflammation-based indexes and clinicopathologic features are strong predictive values of preoperative circulating tumor cell detection in gastric cancer patients. Clin. Transl. Oncol. 2017, 19, 1125–1132. [Google Scholar] [CrossRef]
- Baccelli, I.; Schneeweiss, A.; Riethdorf, S.; Stenzinger, A.; Schillert, A.; Vogel, V.; Klein, C.; Saini, M.; Baeuerle, T.; Wallwiener, M.; et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat. Biotechnol. 2013, 31, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Mazel, M.; Jacot, W.; Pantel, K.; Bartkowiak, K.; Topart, D.; Cayrefourcq, L.; Rossille, D.; Maudelonde, T.; Fest, T.; Alix-Panabières, C. Frequent expression of PD-L1 on circulating breast cancer cells. Mol. Oncol. 2015, 9, 1773–1782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadaki, M.A.; Koutsopoulos, A.V.; Tsoulfas, P.G.; Lagoudaki, E.; Aggouraki, D.; Monastirioti, A.; Koutoulaki, C.; Apostolopoulou, C.A.; Merodoulaki, A.C.; Papadaki, C.; et al. Clinical Relevance of Immune Checkpoints on Circulating Tumor Cells in Breast Cancer. Cancers 2020, 12, 376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Y.; Fang, F.; Zhang, Q. Circulating tumor cell clusters: What we know and what we expect (Review). Int. J. Oncol. 2016, 49, 2206–2216. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Lian, S.; Ye, Y.; Yu, T.; Liang, H.; Cheng, Y.; Xie, J.; Zhu, Y.; Xie, X.; Yu, S.; et al. S-Nitrosocaptopril prevents cancer metastasis in vivo by creating the hostile bloodstream microenvironment against circulating tumor cells. Pharmacol. Res. 2018, 139, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhou, N.; Yu, X.; Zhang, X.; Li, S.; Lei, Z.; Hu, R.; Li, H.; Mao, Y.; Wang, X.; et al. Tumacrophage: Macrophages transformed into tumor stem-like cells by virulent genetic material from tumor cells. Oncotarget 2017, 8, 82326–82343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ören, B.; Urosevic, J.; Mertens, C.; Mora, J.; Guiu, M.; Gomis, R.R.; Weigert, A.; Schmid, T.; Grein, S.; Brüne, B.; et al. Tumour stroma-derived lipocalin-2 promotes breast cancer metastasis. J. Pathol. 2016, 239, 274–285. [Google Scholar] [CrossRef] [Green Version]
- Cabioglu, N.; Sahin, A.A.; Morandi, P.; Meric-Bernstam, F.; Islam, R.; Lin, H.Y.; Bucana, C.D.; Gonzalez-Angulo, A.M.; Hortobagyi, G.N.; Cristofanilli, M. Chemokine receptors in advanced breast cancer: Differential expression in metastatic disease sites with diagnostic and therapeutic implications. Ann. Oncol. 2009, 20, 1013–1019. [Google Scholar] [CrossRef]
- Gareau, A.J.; Brien, C.; Gebremeskel, S.; Liwski, R.S.; Johnston, B.; Bezuhly, M. Ticagrelor inhibits platelet–tumor cell interactions and metastasis in human and murine breast cancer. Clin. Exp. Metastasis 2018, 35, 25–35. [Google Scholar] [CrossRef]
- Yang, L.; Lv, Z.; Xia, W.; Zhang, W.; Xin, Y.; Yuan, H.; Chen, Y.; Hu, X.; Lv, Y.; Xu, Q.; et al. The effect of aspirin on circulating tumor cells in metastatic colorectal and breast cancer patients: A phase II trial study. Clin. Transl. Oncol. 2017, 20, 912–921. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | % | |
|---|---|---|
| Age (years) | ||
| Median | 61 | |
| Range | 31–83 | |
| Menopausal Status | ||
| Premenopausal | 32 | 18.7 |
| Perimenopausal | 16 | 9.4 |
| Postmenopausal | 123 | 71.9 |
| Histology | ||
| Ductal | 134 | 78.4 |
| Lobular | 17 | 9.9 |
| Others | 20 | 11.7 |
| Tumor Size | ||
| pT1 | 102 | 59.6 |
| pT2 | 64 | 37.4 |
| >pT2 | 5 | 2.9 |
| Nodal Status | ||
| pN0 | 101 | 59.1 |
| pN1 | 66 | 38.6 |
| pN2 and pN3 | 4 | 2.3 |
| Grading | ||
| I | 11 | 6.4 |
| II | 100 | 58.5 |
| III | 60 | 35.1 |
| ER Status | ||
| Negative | 37 | 21.6 |
| Positive | 134 | 78.4 |
| PR Status | ||
| Negative | 52 | 30.4 |
| Positive | 119 | 69.6 |
| HER2 Status | ||
| Negative | 144 | 84.2 |
| Positive | 27 | 15.8 |
| Immunohistochemical Subtype | ||
| (ER−, PR−, HER2−) | 26 | 15.2 |
| (ER−, PR−, HER2+) | 8 | 4.7 |
| (ER+ and/or PR+, HER2−) | 118 | 69 |
| (ER+ and/or PR+, HER2+) | 19 | 11.1 |
| DTC | ||
| Negative | 112 | 65.9 |
| Positive | 58 | 34.1 |
| n.d. | 1 | |
| CTC | ||
| Negative | 111 | 72 |
| Positive | 44 | 28 |
| n.d. | 16 | |
| NLR | ||
| >3.13 | 42 | 25 |
| <3.13 | 127 | 75 |
| n.d. | 2 | |
| PLR | ||
| >222.3 | 42 | 25 |
| <222.3 | 129 | 75 |
| MLR | ||
| >0.39 | 47 | 28 |
| <0.39 | 122 | 72 |
| n.d. | 2 | |
| Recurrent | 10 | 6 |
| Deceased | 15 | 9 |
| n | Mean | Median | Perc 25 | Perc 75 | SD | Min | Max | |
|---|---|---|---|---|---|---|---|---|
| NLR | 169 | 2.97 | 2.24 | 1.68 | 3.13 | 2.6 | 0.45 | 22.37 |
| PLR | 170 | 193.6 | 161 | 124.5 | 222.3 | 135 | 30.2 | 1492.7 |
| MLR | 169 | 0.33 | 0.29 | 0.22 | 0.39 | 0.17 | 0.03 | 0.99 |
| Neutrophils (nL) | 169 | 4.45 | 4.03 | 3.13 | 5.31 | 2 | 0.25 | 11.8 |
| Lymphocytes (nL) | 170 | 1.81 | 1.7 | 1.34 | 2.2 | 0.71 | 0.41 | 4.3 |
| Platelets (nL) | 171 | 296.6 | 283 | 237 | 336 | 87.3 | 52 | 612 |
| Monocytes (nL) | 169 | 0.55 | 0.53 | 0.4 | 0.67 | 0.23 | 0.02 | 1.36 |
| Age (y) | 171 | 58.6 | 61 | 50 | 68 | 11.3 | 31 | 83 |
| NLR (Cut-Off) | Sig $ | PLR (Cut-Off) | Sig $ | MLR (Cut-Off) | Sig $ | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≥3.13 | <3.13 | ≥222.3 | <222.3 | ≥0.39 | <0.39 | |||||||||||
| n | % | n | % | p-Value | n | % | n | % | p-Value | n | % | n | % | p-Value | ||
| Age Grouped (60 y) | <60 | 25 | 58.1 | 66 | 52.4 | 0.513 | 25 | 58.1 | 67 | 52.8 | 0.54 | 26 | 61.9 | 65 | 51.2 | 0.227 |
| ≥60 | 18 | 41.9 | 60 | 47.6 | 18 | 41.9 | 60 | 47.2 | 16 | 38.1 | 62 | 48.8 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| Menopausal Status | Premenopausal | 9 | 20.9 | 22 | 17.5 | 0.399 | 8 | 18.6 | 23 | 18.1 | 0.997 | 7 | 16.7 | 24 | 18.9 | 0.426 |
| Perimenopausal | 6 | 14 | 10 | 7.9 | 4 | 9.3 | 12 | 9.4 | 2 | 4.8 | 14 | 11 | ||||
| Postmenopausal | 28 | 65.1 | 94 | 74.6 | 31 | 72.1 | 92 | 72.4 | 33 | 78.6 | 89 | 70.1 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| Histology | Ductal | 30 | 69.8 | 102 | 83.6 | 0.128 | 31 | 73.8 | 102 | 82.3 | 0.478 | 30 | 75 | 102 | 81.6 | 0.657 |
| Lobular | 6 | 14 | 11 | 9 | 6 | 14.3 | 11 | 8.9 | 5 | 12.5 | 12 | 9.6 | ||||
| Other | 7 | 16.3 | 9 | 7.4 | 5 | 11.9 | 11 | 8.9 | 5 | 12.5 | 11 | 8.8 | ||||
| Total | 43 | 100 | 122 | 100 | 42 | 100 | 124 | 100 | 40 | 100 | 125 | 100 | ||||
| pT | pT1 | 26 | 60.5 | 74 | 58.7 | 0.951 | 27 | 62.8 | 74 | 58.3 | 0.86 | 21 | 50 | 79 | 62.2 | 0.107 |
| pT2 | 16 | 37.2 | 48 | 38.1 | 15 | 34.9 | 49 | 38.6 | 18 | 42.9 | 46 | 36.2 | ||||
| pT3 pT4 | 1 | 2.3 | 4 | 3.2 | 1 | 2.3 | 4 | 3.1 | 3 | 7.1 | 2 | 1.6 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| pN | pN0 | 22 | 51.2 | 78 | 61.9 | 0.45 | 18 | 41.9 | 82 | 64.6 | 0.029 | 18 | 42.9 | 82 | 64.6 | 0.041 |
| pN1 | 20 | 46.5 | 45 | 35.7 | 24 | 55.8 | 42 | 33.1 | 23 | 54.8 | 42 | 33.1 | ||||
| pN2 pN3 | 1 | 2.3 | 3 | 2.4 | 1 | 2.3 | 3 | 2.4 | 1 | 2.4 | 3 | 2.4 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| Grading | G1 | 1 | 2.3 | 9 | 7.1 | 0.254 | 2 | 4.7 | 8 | 6.3 | 0.568 | 1 | 2.4 | 9 | 7.1 | 0.338 |
| G2 | 23 | 53.5 | 76 | 60.3 | 23 | 53.5 | 77 | 60.6 | 23 | 54.8 | 76 | 59.8 | ||||
| G3 | 19 | 44.2 | 41 | 32.5 | 18 | 41.9 | 42 | 33.1 | 18 | 42.9 | 42 | 33.1 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| ER Status | No | 13 | 30.2 | 23 | 18.3 | 0.098 | 10 | 23.3 | 27 | 21.3 | 0.784 | 9 | 21.4 | 27 | 21.3 | 0.982 |
| Yes | 30 | 69.8 | 103 | 81.7 | 33 | 76.7 | 100 | 78.7 | 33 | 78.6 | 100 | 78.7 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| PR Status | No | 15 | 34.9 | 36 | 28.6 | 0.436 | 14 | 32.6 | 38 | 29.9 | 0.746 | 12 | 28.6 | 39 | 30.7 | 0.794 |
| Yes | 28 | 65.1 | 90 | 71.4 | 29 | 67.4 | 89 | 70.1 | 30 | 71.4 | 88 | 69.3 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| HER2 Status | No | 35 | 81.4 | 107 | 84.9 | 0.586 | 33 | 76.7 | 110 | 86.6 | 0.126 | 33 | 78.6 | 109 | 85.8 | 0.266 |
| Yes | 8 | 18.6 | 19 | 15.1 | 10 | 23.3 | 17 | 13.4 | 9 | 21.4 | 18 | 14.2 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| ER– PR– HER2– | No | 34 | 79.1 | 110 | 87.3 | 0.189 | 35 | 81.4 | 109 | 85.8 | 0.489 | 36 | 85.7 | 108 | 85 | 0.915 |
| Yes | 9 | 20.9 | 16 | 12.7 | 8 | 18.6 | 18 | 14.2 | 6 | 14.3 | 19 | 15 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| ER– PR– HER2+ | No | 40 | 93 | 121 | 96 | 0.422 | 41 | 95.3 | 121 | 95.3 | 0.984 | 39 | 92.9 | 122 | 96.1 | 0.396 |
| Yes | 3 | 7 | 5 | 4 | 2 | 4.7 | 6 | 4.7 | 3 | 7.1 | 5 | 3.9 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| ER + AND (PR + OR Her2–) | No | 13 | 30.2 | 29 | 23 | 0.344 | 11 | 25.6 | 32 | 25.2 | 0.96 | 10 | 23.8 | 32 | 25.2 | 0.857 |
| Yes | 30 | 69.8 | 97 | 77 | 32 | 74.4 | 95 | 74.8 | 32 | 76.2 | 95 | 74.8 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| ER + AND (PR + OR Her2+) | No | 16 | 37.2 | 32 | 25.4 | 0.138 | 13 | 30.2 | 36 | 28.3 | 0.813 | 11 | 26.2 | 37 | 29.1 | 0.714 |
| Yes | 27 | 62.8 | 94 | 74.6 | 30 | 69.8 | 91 | 71.7 | 31 | 73.8 | 90 | 70.9 | ||||
| Total | 43 | 100 | 126 | 100 | 43 | 100 | 127 | 100 | 42 | 100 | 127 | 100 | ||||
| DTC Status | Neg | 29 | 67.4 | 82 | 65.6 | 0.826 | 28 | 65.1 | 84 | 66.7 | 0.853 | 24 | 57.1 | 87 | 69 | 0.158 |
| Pos | 14 | 32.6 | 43 | 34.4 | 15 | 34.9 | 42 | 33.3 | 18 | 42.9 | 39 | 31 | ||||
| Total | 43 | 100 | 125 | 100 | 43 | 100 | 126 | 100 | 42 | 100 | 126 | 100 | ||||
| CTC Status | Neg | 23 | 57.5 | 86 | 76.1 | 0.025 | 26 | 61.9 | 84 | 75 | 0.109 | 25 | 67.6 | 84 | 72.4 | 0.571 |
| Pos | 17 | 42.5 | 27 | 23.9 | 16 | 38.1 | 28 | 25 | 12 | 32.4 | 32 | 27.6 | ||||
| Total | 40 | 100 | 113 | 100 | 42 | 100 | 112 | 100 | 37 | 100 | 116 | 100 | ||||
| NLR | PLR | MLR | Neutrophils (nL) | Lymphocytes (nL) | Platelets (nL) | Monocytes (nL) | ||
|---|---|---|---|---|---|---|---|---|
| PFS | r | 0.073 | 0.143 | −0.067 | −0.096 | −0.130 | 0.101 | 0.144 |
| p | 0.350 | 0.066 | 0.392 | 0.221 | 0.094 | 0.193 | 0.065 | |
| n | 165 | 166 | 165 | 165 | 166 | 167 | 165 | |
| OS | r | 0.053 | 0.150 | −0.085 | −0.085 | −0.146 | 0.083 | −0.163 |
| p | 0.497 | 0.050 | 0.271 | 0.164 | 0.058 | 0.283 | 0.034 | |
| n | 169 | 170 | 169 | 169 | 170 | 171 | 169 |
| OS | PFS | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Age (years) | ||||||||
| < vs. > 60 | 4.195 (1.182–14.892) | 0.027 | 2.801 (0.552–14.203) | 0.214 | 4.784 (1.032–22.181) | 0.046 | 2.355 (0.375–14.782) | 0.361 |
| Tumor size | ||||||||
| T1 vs. >T1 | 2.182 (0.775–6.139) | 0.139 | 2.159 (0.672–6.932) | 0.196 | 2.533 (0.740–8.674) | 0.137 | 2.916 (0.669–12.705) | 0.154 |
| Lymph node involvement | ||||||||
| N0 vs. N+ | 3.889 (1.238–12.216) | 0.020 | 3.423 (0.999–11.730) | 0.050 | 3.836 (1.017–14.465) | 0.047 | 3.216 (0.752–13.746) | 0.115 |
| Menopausal Status | ||||||||
| Pre- and peri vs. postmenopausal | 2.785 (0.627–12.359) | 0.178 | 1.181 (0.169–8.235) | 0.866 | 4.266 (0.545–33.369) | 0.167 | 2.165 (0.185–25.378) | 0.538 |
| NLR | ||||||||
| < vs. ≥3.13 | 1.909 (0.678–5.373) | 0.221 | 2.073 (0.546–7.870) | 0.284 | 2.336 (0.711–7.667) | 0.162 | 2.696 (0.555–13.089) | 0.219 |
| PLR | ||||||||
| < vs. ≥222.3 | 0.671 (0.189–2.382) | 0.537 | 0.303 (0.069–1.326) | 0.113 | 0.608 (0.131–2.820) | 0.525 | 0.281 (0.049–1.618) | 0.155 |
| MLR | ||||||||
| < vs. ≥0.39 | 1.639 (0.559–4.805) | 0.368 | 1.500 (0.419–5.367) | 0.533 | 1.964 (0.572–6.745) | 0.284 | 1.575 (0.354–7.013) | 0.551 |
| CTCs | ||||||||
| Pos. vs. Neg. | 1.151 (0.360–3.677) | 0.813 | 0.981 (0.294–3.269) | 0.975 | 1.194 (0.308–4.628) | 0.797 | 0.904 (0.218–3.751) | 0.890 |
| DTCs | ||||||||
| Pos. Vs. neg. | 1.172 (0.416–3.305) | 0.764 | 0.825 (0.251–2.716) | 0.752 | 1.467 (0.446–4.828) | 0.528 | 0.959 (0.240–3.833) | 0.953 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasimir-Bauer, S.; Karaaslan, E.; Hars, O.; Hoffmann, O.; Kimmig, R. In Early Breast Cancer, the Ratios of Neutrophils, Platelets and Monocytes to Lymphocytes Significantly Correlate with the Presence of Subsets of Circulating Tumor Cells but Not with Disseminated Tumor Cells. Cancers 2022, 14, 3299. https://doi.org/10.3390/cancers14143299
Kasimir-Bauer S, Karaaslan E, Hars O, Hoffmann O, Kimmig R. In Early Breast Cancer, the Ratios of Neutrophils, Platelets and Monocytes to Lymphocytes Significantly Correlate with the Presence of Subsets of Circulating Tumor Cells but Not with Disseminated Tumor Cells. Cancers. 2022; 14(14):3299. https://doi.org/10.3390/cancers14143299
Chicago/Turabian StyleKasimir-Bauer, Sabine, Ebru Karaaslan, Olaf Hars, Oliver Hoffmann, and Rainer Kimmig. 2022. "In Early Breast Cancer, the Ratios of Neutrophils, Platelets and Monocytes to Lymphocytes Significantly Correlate with the Presence of Subsets of Circulating Tumor Cells but Not with Disseminated Tumor Cells" Cancers 14, no. 14: 3299. https://doi.org/10.3390/cancers14143299
APA StyleKasimir-Bauer, S., Karaaslan, E., Hars, O., Hoffmann, O., & Kimmig, R. (2022). In Early Breast Cancer, the Ratios of Neutrophils, Platelets and Monocytes to Lymphocytes Significantly Correlate with the Presence of Subsets of Circulating Tumor Cells but Not with Disseminated Tumor Cells. Cancers, 14(14), 3299. https://doi.org/10.3390/cancers14143299