
Incidence, Mortality, and Trends of Prostate Cancer in Mexico from 2000 to 2019: Results from the Global Burden of Disease Study 2019

 , , , ,
, , , , 
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Data Input Sources and Case Definition
2.2. Estimation of Prostate Cancer Incidence and Mortality
2.3. Reporting Standards
2.4. Analysis of Prostate Cancer Trends
2.5. Analysis of Prostate Cancer Burden by Age Group
2.6. Association of Prostate Cancer Burden with Sociodemographic Index
3. Results
3.1. National Incidence and Mortality of Prostate Cancer in 2019
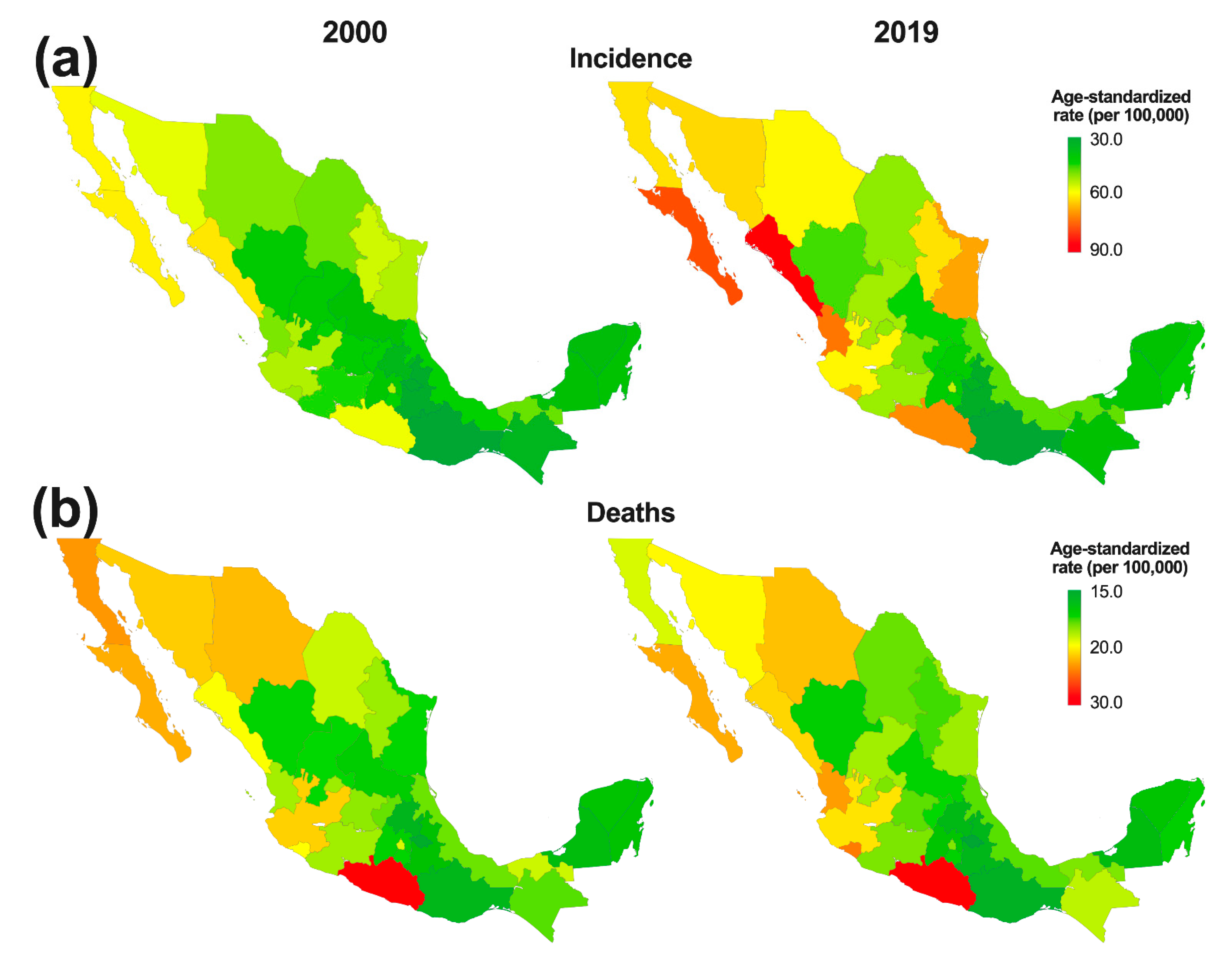
3.2. Subnational Incidence and Mortality of Prostate Cancer in 2019
3.3. National Burden of Prostate Cancer by Age Group
3.4. National Trends of Prostate Cancer Burden from 2000 to 2019
3.5. Subnational Trends of Prostate Cancer Burden from 2000 to 2019
3.6. National Annual Percentage Changes of Age-Standardized Incidence and Mortality of Prostate Cancer from 2000 to 2019
3.7. Association of the Sociodemographic Index with the Burden of Prostate Cancer at the Subnational Level in 2019
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Available online: https://gco.iarc.fr/today/home (accessed on 12 January 2022).
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Global Burden of Disease 2019 Cancer Collaboration; Kocarnik, J.M.; Compton, K.; Dean, F.E.; Fu, W.; Gaw, B.L.; Harvey, J.D.; Henrikson, H.J.; Lu, D.; Pennini, A.; et al. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef] [PubMed]
- Lajous, M.; Cooperberg, M.R.; Rider, J.; Manzanilla-Garcia, H.A.; Gabilondo-Navarro, F.B.; Rodriguez-Covarrubias, F.T.; Lopez-Ridaura, R.; Torres-Sanchez, L.E.; Mohar, A. Prostate cancer screening in low- and middle-income countries: The Mexican case. Salud Pública De México 2019, 61, 542–544. [Google Scholar] [CrossRef] [PubMed]
- Sierra, M.S.; Soerjomataram, I.; Forman, D. Prostate cancer burden in Central and South America. Cancer Epidemiol. Prev. Biomark. 2016, 44 (Suppl. S1), S131–S140. [Google Scholar] [CrossRef]
- Reis, R.B.D.; Alias-Melgar, A.; Martinez-Cornelio, A.; Neciosup, S.P.; Sade, J.P.; Santos, M.; Villoldo, G.M. Prostate Cancer in Latin America: Challenges and Recommendations. Cancer Control 2020, 27, 1073274820915720. [Google Scholar] [CrossRef]
- Adame González, C.; Álvarez Romero, J.T.; Morachel y Rodríguez, M.; Félix Leyva, A.; Ponce Viveros, M.; Villavicencio Queijeiro, M.A.; Bautista Hernández, M.Y.B.; Gracia-Medrano Valdemar, L. Biochemical relapse free survival rate in patients with prostate cancer treated with external radiotherapy: Outcomes obtained at the CMN Siglo XXI Hospital de Oncología, CMN 20 de Noviembre and Hospital General de México of the México City. Rep. Pract. Oncol. Radiother. 2020, 25, 276–281. [Google Scholar] [CrossRef]
- Torres-Sánchez, L.E.; Espinoza-Giacinto, R.; Rojas-Martínez, R.; Escamilla-Nuñez, C.; Vázquez-Salas, R.A.; Campuzano, J.C.; Lazcano-Ponce, E. Comportamiento de la mortalidad por cáncer de próstata en México de acuerdo al índice de marginación estatal, de 1980 a 2013. Salud Pública De México 2016, 58, 179–186. [Google Scholar] [CrossRef]
- Gomez-Dantes, H.; Lamadrid-Figueroa, H.; Cahuana-Hurtado, L.; Silverman-Retana, O.; Montero, P.; Gonzalez-Robledo, M.C.; Fitzmaurice, C.; Pain, A.; Allen, C.; Dicker, D.J.; et al. The burden of cancer in Mexico, 1990-2013. Salud Pública De México 2016, 58, 118–131. [Google Scholar] [CrossRef]
- Castillejos-Molina, R.A.; Gabilondo-Navarro, F.B. Prostate cancer. Salud Pública De México 2016, 58, 279–284. [Google Scholar] [CrossRef]
- Global Burden of Disease Cancer, C.; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, T.; Zhang, H.; Sang, S.; Chen, H.; Zuo, X. Temporal trend of gastric cancer burden along with its risk factors in China from 1990 to 2019, and projections until 2030: Comparison with Japan, South Korea, and Mongolia. Biomark. Res. 2021, 9, 84. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Chan, W.C.; Ngai, C.H.; Lok, V.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.-J.; Elcarte, E.; Withers, M. Worldwide Burden, Risk Factors, and Temporal Trends of Ovarian Cancer: A Global Study. Cancers 2022, 14, 2230. [Google Scholar] [CrossRef] [PubMed]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Chatenoud, L.; Bertuccio, P.; Bosetti, C.; Malvezzi, M.; Levi, F.; Negri, E.; La Vecchia, C. Trends in mortality from major cancers in the Americas: 1980-2010. Ann. Oncol. 2014, 25, 1843–1853. [Google Scholar] [CrossRef]
- Pow-Sang, M.; Destefano, V.; Astigueta, J.C.; Castillo, O.; Gaona, J.L.; Santaella, F.; Sotelo, R. Cáncer de próstata en Latinoamérica. Actas Urológicas Españolas 2009, 33, 1057–1061. [Google Scholar] [CrossRef][Green Version]
- Center, M.M.; Jemal, A.; Lortet-Tieulent, J.; Ward, E.; Ferlay, J.; Brawley, O.; Bray, F. International variation in prostate cancer incidence and mortality rates. Eur. Urol. 2012, 61, 1079–1092. [Google Scholar] [CrossRef]
- Bishop, S.K.; Hsiu-Juei Kao, C.; Yeo Han, D.; Ferguson, R.L. Prostate Cancer Prevention in the Developing World—What are we Waiting for? Curr. Pharm. Pers. Med. 2012, 10, 70–86. [Google Scholar] [CrossRef]
- Quinn, M.; Babb, P. Patterns and trends in prostate cancer incidence, survival, prevalence and mortality. Part I: International comparisons. BJU Int. 2002, 90, 162–173. [Google Scholar] [CrossRef]
- Hsing, A.W.; Devesa, S.S. Trends and patterns of prostate cancer: What do they suggest? Epidemiol. Rev. 2001, 23, 3–13. [Google Scholar] [CrossRef]
- Grozescu, T.; Popa, F. Prostate cancer between prognosis and adequate/proper therapy. J. Med. Life 2017, 10, 5. [Google Scholar]
- Dy, G.W.; Gore, J.L.; Forouzanfar, M.H.; Naghavi, M.; Fitzmaurice, C. Global Burden of Urologic Cancers, 1990–2013. Eur. Urol. 2017, 71, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Zheng, Y.; Li, N.; Deng, Y.; Zhou, L.; Tian, T.; Yang, S.; Hao, Q.; Song, D.; Wu, Y.; et al. Incidence and disease burden of prostate cancer from 1990 to 2017: Results from the Global Burden of Disease Study 2017. Cancer 2020, 126, 1969–1978. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Center, M.M.; DeSantis, C.; Ward, E.M. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1893–1907. [Google Scholar] [CrossRef] [PubMed]
- Taitt, H.E. Global trends and prostate cancer: A review of incidence, detection, and mortality as influenced by race, ethnicity, and geographic location. Am. J. Men’s Health 2018, 12, 1807–1823. [Google Scholar] [CrossRef]
- Baade, P.D.; Yu, X.Q.; Smith, D.P.; Dunn, J.; Chambers, S.K. Geographic disparities in prostate cancer outcomes--review of international patterns. Asian Pac. J. Cancer Prev. 2015, 16, 1259–1275. [Google Scholar] [CrossRef]
- Diaz, D.; Vazquez-Polanco, A.M.; Argueta-Donohue, J.; Stephens, C.R.; Jimenez-Trejo, F.; Ceballos-Liceaga, S.E.; Mantilla-Beniers, N. Incidence of Intestinal Infectious Diseases due to Protozoa and Bacteria in Mexico: Analysis of National Surveillance Records from 2003 to 2012. BioMed Res. Int. 2018, 2018, 2893012. [Google Scholar] [CrossRef]
- Pineros, M.; Znaor, A.; Mery, L.; Bray, F. A global cancer surveillance framework within noncommunicable disease surveillance: Making the case for population-based cancer registries. Epidemiol. Rev. 2017, 39, 161–169. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Estimate | Counts (95% UI) | % Change 2010 to 2019 | ASR (per 100,000) | ||
|---|---|---|---|---|---|
| 2000 | 2010 | 2019 | 2019 | ||
| Incidence | 11,444 (8883 to 14,016) | 17,784 (14,346 to 23,397) | 27,096 (20,602 to 36,016) | 52.4 (24.0 to 88.0) | 52.3 (40.0 to 70.1) |
| Deaths | 4812 (3795 to 6138) | 6864 (5674 to 9075) | 9256 (7077 to 12,678) | 34.8 (13.0 to 62.0) | 19.4 (14.7 to 26.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beltran-Ontiveros, S.A.; Fernandez-Galindo, M.A.; Moreno-Ortiz, J.M.; Contreras-Gutierrez, J.A.; Madueña-Molina, J.; Arambula-Meraz, E.; Leal-Leon, E.; Becerril-Camacho, D.M.; Picos-Cardenas, V.J.; Angulo-Rojo, C.; et al. Incidence, Mortality, and Trends of Prostate Cancer in Mexico from 2000 to 2019: Results from the Global Burden of Disease Study 2019. Cancers 2022, 14, 3184. https://doi.org/10.3390/cancers14133184
Beltran-Ontiveros SA, Fernandez-Galindo MA, Moreno-Ortiz JM, Contreras-Gutierrez JA, Madueña-Molina J, Arambula-Meraz E, Leal-Leon E, Becerril-Camacho DM, Picos-Cardenas VJ, Angulo-Rojo C, et al. Incidence, Mortality, and Trends of Prostate Cancer in Mexico from 2000 to 2019: Results from the Global Burden of Disease Study 2019. Cancers. 2022; 14(13):3184. https://doi.org/10.3390/cancers14133184
Chicago/Turabian StyleBeltran-Ontiveros, Saul A., Martha A. Fernandez-Galindo, Jose M. Moreno-Ortiz, Jose A. Contreras-Gutierrez, Jesus Madueña-Molina, Eliakym Arambula-Meraz, Emir Leal-Leon, Delia M. Becerril-Camacho, Veronica J. Picos-Cardenas, Carla Angulo-Rojo, and et al. 2022. "Incidence, Mortality, and Trends of Prostate Cancer in Mexico from 2000 to 2019: Results from the Global Burden of Disease Study 2019" Cancers 14, no. 13: 3184. https://doi.org/10.3390/cancers14133184
APA StyleBeltran-Ontiveros, S. A., Fernandez-Galindo, M. A., Moreno-Ortiz, J. M., Contreras-Gutierrez, J. A., Madueña-Molina, J., Arambula-Meraz, E., Leal-Leon, E., Becerril-Camacho, D. M., Picos-Cardenas, V. J., Angulo-Rojo, C., Velazquez, D. Z., Jimenez-Trejo, F., Gallardo-Vera, F., & Diaz, D. (2022). Incidence, Mortality, and Trends of Prostate Cancer in Mexico from 2000 to 2019: Results from the Global Burden of Disease Study 2019. Cancers, 14(13), 3184. https://doi.org/10.3390/cancers14133184