
The Role of Indocyanine Green Fluorescence in Rectal Cancer Robotic Surgery: A Narrative Review


 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
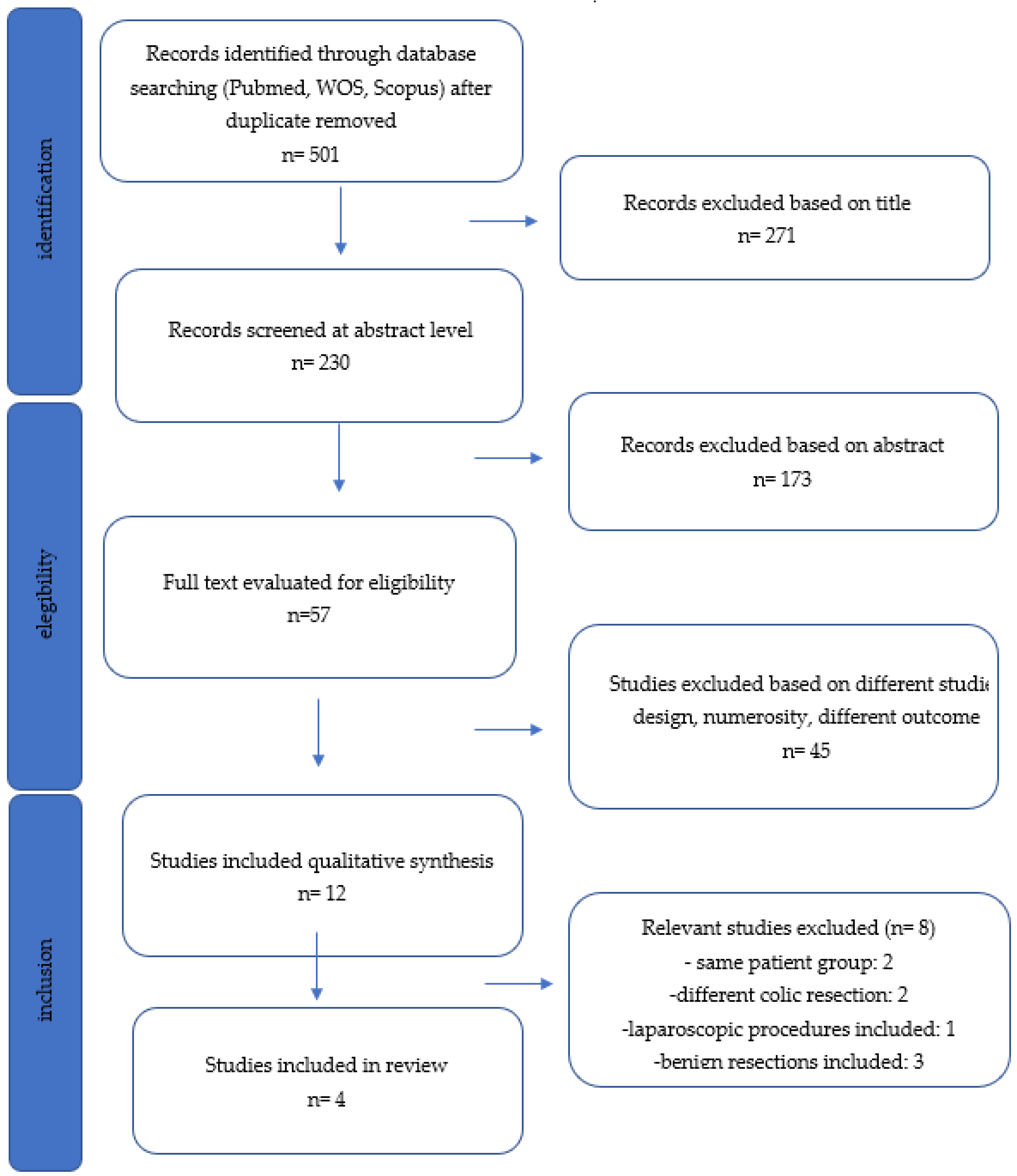
2. Materials and Methods
2.1. Study Selection
2.2. Data Extraction
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Outcomes of Interest
2.6. Statistical Analysis
3. Results
3.1. Included Studies
3.2. Patient Characteristics
3.3. Outcomes and ICG Application
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Keller, D.S.; Berho, M.; Perez, R.O.; Wexner, S.D.; Chand, M. The multidisciplinary management of rectal cancer. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 414–429. [Google Scholar] [CrossRef] [PubMed]
- Gessler, B.; Eriksson, O.; Angenete, E. Diagnosis, treatment, and consequences of anastomotic leakage in colorectal surgery. Int. J. Colorectal Dis. 2017, 32, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Spinelli, A.; Anania, G.; Arezzo, A.; Berti, S.; Bianco, F.; Bianchi, P.P.; De Giuli, M.; De Nardi, P.; de Paolis, P.; Foppa, C.; et al. Italian multi-society modified Delphi consensus on the definition and management of anastomotic leakage in colorectal surgery. Updates Surg. 2020, 72, 781–792. [Google Scholar] [CrossRef]
- Lee, W.-S.; Yun, S.H.; Roh, Y.-N.; Yun, H.-R.; Lee, W.Y.; Cho, Y.B.; Chun, H.-K. Risk factors and clinical outcome for anastomotic leakage after total mesorectal excision for rectal cancer. World J. Surg. 2008, 32, 1124–1129. [Google Scholar] [CrossRef]
- Baiocchi, G.L.; Diana, M.; Boni, L. Indocyanine green-based fluorescence imaging in visceral and hepatobiliary and pancreatic surgery: State of the art and future directions. World J. Gastroenterol. 2018, 24, 2921–2930. [Google Scholar] [CrossRef]
- Spota, A.; Al-Taher, M.; Felli, E.; Morales Conde, S.; Dal Dosso, I.; Moretto, G.; Spinoglio, G.; Baiocchi, G.; Vilallonga, R.; Impellizzeri, H.; et al. Fluorescence-based bowel anastomosis perfusion evaluation: Results from the IHU-IRCAD-EAES EURO-FIGS registry. Surg. Endosc. 2021, 35, 7142–7153. [Google Scholar] [CrossRef]
- Kowalewski, K.F.; Seifert, L.; Ali, S.; Schmidt, M.W.; Seide, S.; Haney, C.; Tapking, C.; Shamiyeh, A.; Kulu, Y.; Hackert, T.; et al. Functional outcomes after laparoscopic versus robotic-assisted rectal resection: A systematic review and meta-analysis. Surg. Endosc. 2021, 35, 81–95. [Google Scholar] [CrossRef] [Green Version]
- Moletta, L.; Pierobon, E.S.; Capovilla, G.; Costantini, M.; Salvador, R.; Merigliano, S.; Valmasoni, M. International guidelines and recommendations for surgery during COVID-19 pandemic: A Systematic Review. Int. J. Surg. 2020, 79, 180–188. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Dripps, R.D.; Lamont, A.; Eckenhoff, J.E. The role of anesthesia in surgical mortality. JAMA 1961, 178, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Jafari, M.D.; Lee, K.H.; Halabi, W.J.; Mills, S.F.; Carmichael, J.C.; Stamos, M.J.; Pigazzi, A. The use of indocyanine green fluorescence to assess anastomotic perfusion during robotic assisted laparoscopic rectal surgery. Surg. Endosc. 2013, 27, 3003–3008. [Google Scholar] [CrossRef] [PubMed]
- Somashekhar, S.P.; Reddy, R.G.; Kumar, C.R.; Ashwin, K.R. Prospective Study Comparing Clinical vs Indocyanine Green Fluorescence-Based Assessment of Line of Transection in Robotic Rectal Cancer Surgery-Indian Study. Indian J. Surg. Oncol. 2020, 11, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.U.; Min, B.S.; Kim, N.K. Robotic Low Ligation of the Inferior Mesenteric Artery for Rectal Cancer Using the Firefly Technique. Yonsei Med. J. 2015, 56, 1028–1035. [Google Scholar] [CrossRef]
- Kim, J.C.; Lee, J.L.; Yoon, Y.S.; Alotaibi, A.M.; Kim, J. Utility of indocyanine-green fluorescent imaging during robot-assisted sphincter-saving surgery on rectal cancer patients. Int. J. Med. Robot. Comput. Assist. Surg. 2015, 12, 710–717. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Cammà, C.; Giunta, M.; Fiorica, F.; Pagliaro, L.; Craxì, A.; Cottone, M. Preoperative radiotherapy for resectable rectal cancer: A meta-analysis. JAMA 2000, 284, 1008–1015. [Google Scholar] [CrossRef]
- Rubio, J.; Cristóbal, I.; Santos, A.; Caramés, C.; Luque, M.; Sanz-Alvarez, M.; Zazo, S.; Madoz-Gúrpide, J.; Rojo, F.; García-Foncillas, J. Low MicroRNA-19b Expression Shows a Promising Clinical Impact in Locally Advanced Rectal Cancer. Cancers 2021, 13, 1456. [Google Scholar] [CrossRef]
- Park, J.S.; Choi, G.-S.; Kim, S.H.; Kim, H.R.; Kim, N.K.; Lee, K.Y.; Kang, S.B.; Kim, J.Y.; Lee, K.Y.; Kim, B.C.; et al. Multicenter Analysis of Risk Factors for Anastomotic Leakage After Laparoscopic Rectal Cancer Excision: The Korean Laparoscopic Colorectal Surgery Study Group. Ann. Surg. 2013, 257, 665–671. [Google Scholar] [CrossRef]
- Meyer, J.; Naiken, S.; Christou, N.; Liot, E.; Toso, C.; Buchs, N.C.; Ris, F. Reducing anastomotic leak in colorectal surgery: The old dogmas and the new challenges. World J. Gastroenterol. 2019, 25, 5017–5025. [Google Scholar] [CrossRef]
- Pommergaard, H.C.; Gessler, B.; Burcharth, J.; Angenete, E.; Haglind, E.; Rosenberg, J. Preoperative risk factors for anastomotic leakage after resection for colorectal cancer: A systematic review and meta-analysis. Color. Dis. 2014, 16, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Karliczek, A.; Harlaar, N.J.; Zeebregts, C.J.; Wiggers, T.; Baas, P.C.; van Dam, G.M. Surgeons lack predictive accuracy for anastomotic leakage in gastrointestinal surgery. Int. J. Colorectal Dis. 2009, 24, 569–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.Q.; Elnahas, A.; Tang, E.; Alkhamesi, N.A.; Hawel, J.; Alnumay, A.; Schlachta, C.M. Cost analysis of indocyanine green fluorescence angiography for prevention of anastomotic leakage in colorectal surgery. Surg. Endosc. 2022, 15, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Skrovina, M.; Bencurik, V.; Martinek, L.; Machackova, M.; Bartos, J.; Andel, P.; Stepanova, E.; Bunakova, M.; Vomackova, K. The significance of intraoperative fluorescence angiography in miniinvasive low rectal resections. Videosurgery Other Miniinvasive Tech. 2020, 15, 43–48. [Google Scholar] [CrossRef] [PubMed]
- van den Bos, J.; Jongen, A.C.H.M.; Melenhorst, J.; Breukink, S.O.; Lenaerts, K.; Schols, R.M.; Bouvy, N.D.; Stassen, L.P.S. Near-infrared fluorescence image-guidance in anastomotic colorectal cancer surgery and its relation to serum markers of anastomotic leakage: A clinical pilot study. Surg. Endosc. 2019, 33, 3766–3774. [Google Scholar] [CrossRef] [Green Version]
- Mangano, A.; Fernandes, E.; Gheza, F.; Bustos, R.; Chen, L.L.; Masrur, M.; Giulianotti, P.C. Near-Infrared Indocyanine Green-Enhanced Fluorescence and Evaluation of the Bowel Microperfusion During Robotic Colorectal Surgery: A Retrospective Original Paper. Surg. Technol. Int. 2019, 34, 93–100. [Google Scholar]
- Ris, F.; Hompes, R.; Cunningham, C.; Lindsey, I.; Guy, R.; Jones, O.; George, B.; Cahill, R.A.; Mortensen, N.J. Near-infrared (NIR) perfusion angiography in minimally invasive colorectal surgery. Surg. Endosc. 2014, 28, 2221–2226. [Google Scholar] [CrossRef] [Green Version]
- Eltair, M.; Hajibandeh, S.; Hajibandeh, S.; Nuno, A.; Abdullah, K.H.; Alkaili-Alyamani, A.; Aslam, M.I.; Sinha, A.; Agarwal, T. Meta-analysis and trial sequential analysis of robotic versus laparoscopic total mesorectal excision in management of rectal cancer. Int. J. Colorectal Dis. 2020, 35, 1423–1438. [Google Scholar] [CrossRef]
- van der Pas, M.H.; Haglind, E.; Cuesta, M.A.; Fürst, A.; Lacy, A.M.; Hop, W.C.; Bonjer, H.J. Laparoscopic versus open surgery for rectal cancer (COLOR II): Short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 2013, 14, 210–218. [Google Scholar] [CrossRef]
- Jayne, D.; Pigazzi, A.; Marshall, H.; Croft, J.; Corrigan, N.; Copeland, J.; Quirke, P.; West, N.; Rautio, T.; Thomassen, N.; et al. Effect of Robotic-Assisted vs Conventional Laparoscopic Surgery on Risk of Conversion to Open Laparotomy Among Patients Undergoing Resection for Rectal Cancer: The ROLARR Randomized Clinical Trial. JAMA 2017, 318, 1569–1580. [Google Scholar] [CrossRef]
- Blanco-Colino, R.; Espin-Basany, E. Intraoperative use of ICG fluorescence imaging to reduce the risk of anastomotic leakage in colorectal surgery: A systematic review and meta-analysis. Tech. Coloproctol. 2018, 22, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Jafari, M.D.; Pigazzi, A.; McLemore, E.C.; Mutch, M.G.; Haas, E.; Rasheid, S.H.; Wait, A.D.; Paquette, I.M.; Bardakcioglu, O.; Safar, B.; et al. Perfusion Assessment in Left-Sided/Low Anterior Resection (PILLAR III): A Randomized, Controlled, Parallel, Multicenter Study Assessing Perfusion Outcomes With PINPOINT Near-Infrared Fluorescence Imaging in Low Anterior Resection. Dis. Colon Rectum 2021, 64, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- De Nardi, P.; Elmore, U.; Maggi, G.; Maggiore, R.; Boni, L.; Cassinotti, E.; Fumagalli, U.; Gardani, M.; De Pascale, S.; Parise, P.; et al. Intraoperative angiography with indocyanine green to assess anastomosis perfusion in patients undergoing laparoscopic colorectal resection: Results of a multicenter randomized controlled trial. Surg. Endosc. 2020, 34, 53–60. [Google Scholar] [CrossRef] [PubMed]
- EURO-FIGS. Available online: https://www.euro-figs.eu/login/ (accessed on 10 April 2022).
- Dosing and Timing Chart on How to Use Indocyanine Green (Icg) by Procedure. Available online: https://isfgs.org/physician-resources/photo-library/ (accessed on 10 April 2022).
- D’Urso, A.; Agnus, V.; Barberio, M.; Seeliger, B.; Marchegiani, F.; Charles, A.-L.; Geny, B.; Marescaux, J.; Mutter, D.; Diana, M. Computer-assisted quantification and visualization of bowel perfusion using fluorescence-based enhanced reality in left-sided colonic resections. Surg. Endosc. 2021, 35, 4321–4331. [Google Scholar] [CrossRef]
- Diana, M.; Agnus, V.; Halvax, P.; Liu, Y.-Y.; Dallemagne, B.; Schlagowski, A.-I.; Geny, B.; Diemunsch, P.; Lindner, V.; Marescaux, J. Intraoperative fluorescence-based enhanced reality laparoscopic real-time imaging to assess bowel perfusion at the anastomotic site in an experimental model. Br. J. Surg. 2015, 102, e169–e176. [Google Scholar] [CrossRef]
- Heald, R.J.; Husband, E.M.; Ryall, R.D. The mesorectum in rectal cancer surgery—The clue to pelvic recurrence? Br. J. Surg. 1982, 69, 613–616. [Google Scholar] [CrossRef]
- Stornes, T.; Wibe, A.; Nesbakken, A.; Myklebust, T.Å.; Endreseth, B.H. National Early Rectal Cancer Treatment Revisited. Dis. Colon Rectum 2016, 59, 623–629. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Milone, M.; Manigrasso, M.; Velotti, N.; Torino, S.; Vozza, A.; Sarnelli, G.; Aprea, G.; Maione, F.; Gennarelli, N.; Musella, M.; et al. Completeness of total mesorectum excision of laparoscopic versus robotic surgery: A review with a meta-analysis. Int. J. Colorectal Dis. 2019, 34, 983–991. [Google Scholar] [CrossRef]
- Prete, F.P.; Pezzolla, A.; Prete, F.; Testini, M.; Marzaioli, R.; Patriti, A.; Jimenez-Rodriguez, R.M.; Gurrado, A.; Strippoli, G.F.M. Robotic Versus Laparoscopic Minimally Invasive Surgery for Rectal Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Ann. Surg. 2018, 267, 1034–1046. [Google Scholar] [CrossRef]
- Jeong, S.-Y.; Park, J.W.; Nam, B.H.; Kim, S.; Kang, S.-B.; Lim, S.-B.; Choi, H.S.; Kim, D.-W.; Chang, H.J.; Kim, D.Y.; et al. Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): Survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol. 2014, 15, 767–774. [Google Scholar] [CrossRef]
- Kayano, H.; Okuda, J.; Tanaka, K.; Kondo, K.; Tanigawa, N. Evaluation of the learning curve in laparoscopic low anterior resection for rectal cancer. Surg. Endosc. 2011, 25, 2972–2979. [Google Scholar] [CrossRef] [PubMed]
- Simillis, C.; Lal, N.; Thoukididou, S.N.; Kontovounisios, C.; Smith, J.J.; Hompes, R.; Adamina, M.; Tekkis, P.P. Open Versus Laparoscopic Versus Robotic Versus Transanal Mesorectal Excision for Rectal Cancer: A Systematic Review and Network Meta-analysis. Ann. Surg. 2019, 270, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Guillou, P.J.; Quirke, P.; Thorpe, H.; Walker, J.; Jayne, D.G.; Smith, A.M.H.; Heath, R.M.; Brown, J.M. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): Multicentre, randomised controlled trial. Lancet 2005, 365, 1718–1726. [Google Scholar] [CrossRef]
- Kim, M.J.; Park, S.C.; Park, J.W.; Chang, H.J.; Kim, D.Y.; Nam, B.-H.; Sohn, D.K.; Oh, J.H. Robot-assisted Versus Laparoscopic Surgery for Rectal Cancer: A Phase II Open Label Prospective Randomized Controlled Trial. Ann. Surg. 2018, 267, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Wang, Z.; Jiang, Z.; Liu, J.; Zhao, J.; Li, J. Male urinary and sexual function after robotic pelvic autonomic nerve-preserving surgery for rectal cancer. Int. J. Med. Robot. 2017, 13, e1725. [Google Scholar] [CrossRef] [PubMed]
- Achilli, P.; Grass, F.; Larson, D.W. Robotic surgery for rectal cancer as a platform to build on: Review of current evidence. Surg. Today 2021, 51, 44–51. [Google Scholar] [CrossRef]
- Cleary, R.K.; Mullard, A.J.; Ferraro, J.; Regenbogen, S.E. The cost of conversion in robotic and laparoscopic colorectal surgery. Surg. Endosc. 2018, 32, 1515–1524. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Country | ICG | No ICG | Age | Gender (M/F) | BMI | Neoadjuvant Therapy |
|---|---|---|---|---|---|---|---|---|
| Jafari | 2013 | USA | 16 | 22 | 60.5 | 28/10 | 27 | 25 |
| Bae | 2015 | South Korea | 11 | NR | 42 | 6/5 | 22.9 | 7 |
| Kim | 2019 | South Korea | 609 | 359 | 57 | 586/382 | 23.5 | 287 |
| Somashekhar | 2020 | India | 50 | NR | 54.5 | 32/18 | 30 > 25 | 41 |
| Author | ICG Dosage | Timing | Change of Plan | Anastomotic Leak ICG (%) | Anastomotic Leak No ICG (%) |
|---|---|---|---|---|---|
| Jafari | 6–8 mg | Before | 3 (19%) | 1 (4.5%) | 4 (18%) |
| Bae | 5 mg | Before | NR | 0 (0%) | NR |
| Kim | 10 mg | Before and After | NR | 15 (2.4%) | 19 (5.3%) |
| Somashekhar | 0.1–0.5 mg/mL/kg | Before and After | 44 (88%) | 1 (2%) | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belloni, E.; Muttillo, E.M.; Di Saverio, S.; Gasparrini, M.; Brescia, A.; Nigri, G. The Role of Indocyanine Green Fluorescence in Rectal Cancer Robotic Surgery: A Narrative Review. Cancers 2022, 14, 2411. https://doi.org/10.3390/cancers14102411
Belloni E, Muttillo EM, Di Saverio S, Gasparrini M, Brescia A, Nigri G. The Role of Indocyanine Green Fluorescence in Rectal Cancer Robotic Surgery: A Narrative Review. Cancers. 2022; 14(10):2411. https://doi.org/10.3390/cancers14102411
Chicago/Turabian StyleBelloni, Elena, Edoardo Maria Muttillo, Salomone Di Saverio, Marcello Gasparrini, Antonio Brescia, and Giuseppe Nigri. 2022. "The Role of Indocyanine Green Fluorescence in Rectal Cancer Robotic Surgery: A Narrative Review" Cancers 14, no. 10: 2411. https://doi.org/10.3390/cancers14102411
APA StyleBelloni, E., Muttillo, E. M., Di Saverio, S., Gasparrini, M., Brescia, A., & Nigri, G. (2022). The Role of Indocyanine Green Fluorescence in Rectal Cancer Robotic Surgery: A Narrative Review. Cancers, 14(10), 2411. https://doi.org/10.3390/cancers14102411