
Validating an Instrument for Direct Patient Reporting of Distress and Chemotherapy-Related Toxicity among South African Cancer Patients

 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient-Reported Symptoms-South Africa Instrument Design
2.2. Additional Study Instruments
2.3. Setting and Participants
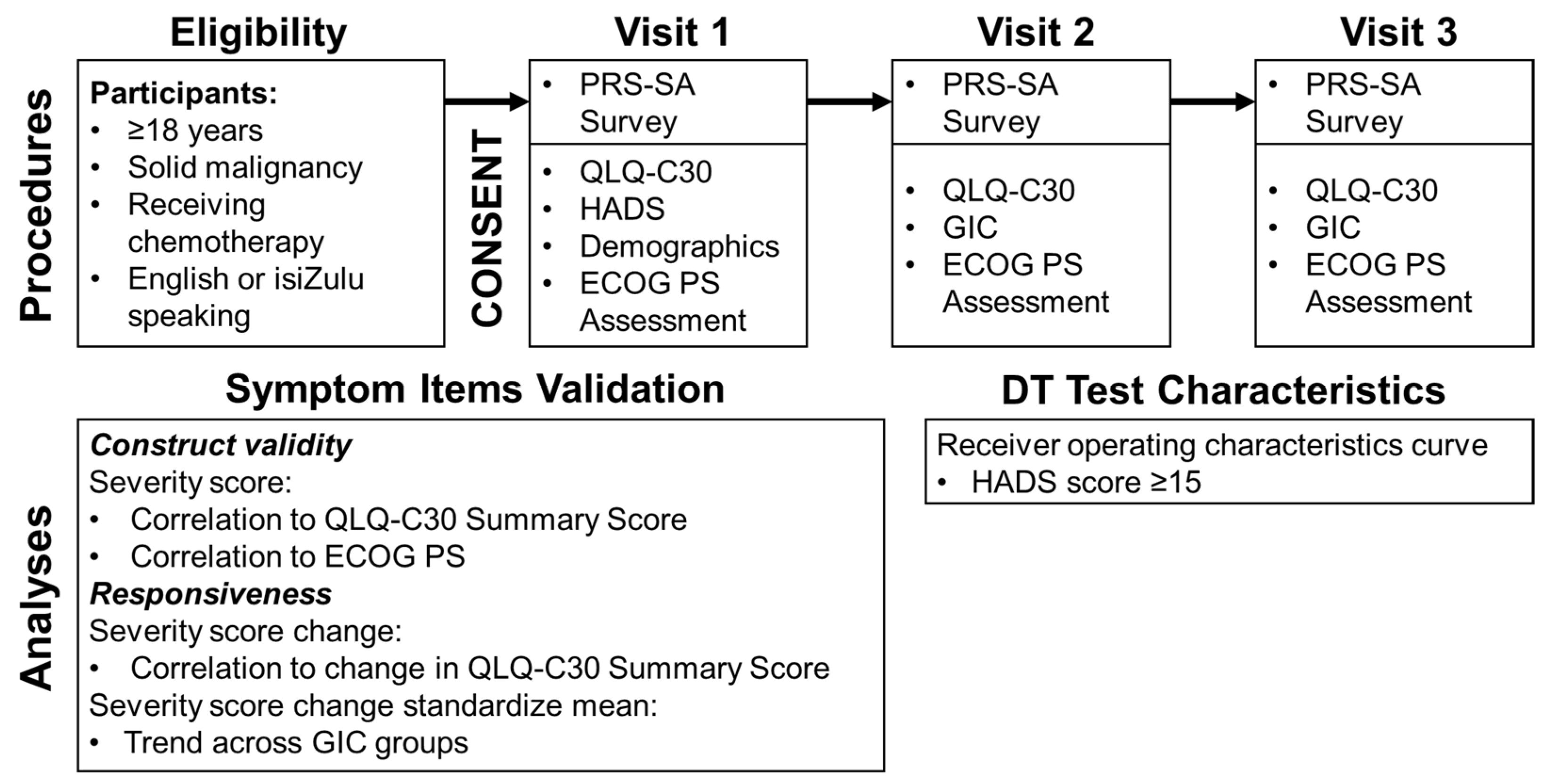
2.4. Study Procedures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leblanc, T.W.; Abernethy, A.P. Patient-Reported Outcomes in Cancer Care—Hearing the Patient Voice at Greater Volume. Nat. Rev. Clin. Oncol. 2017, 14, 763–772. [Google Scholar] [CrossRef] [PubMed]
- Holch, P.; Warrington, L.; Bamforth, L.C.A.; Keding, A.; Ziegler, L.E.; Absolom, K.; Hector, C.; Harley, C.; Johnson, O.; Hall, G.; et al. Development of an Integrated Electronic Platform for Patient Self-Report and Management of Adverse Events during Cancer Treatment. Ann. Oncol. 2017, 28, 2305–2311. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Artz, D.; Iasonos, A.; Speakman, J.; Shannon, K.; Lin, K.; Pun, C.; Yong, H.; Fearn, P.; Barz, A.; et al. Evaluation of an Online Platform for Cancer Patient Self-Reporting of Chemotherapy Toxicities. J. Am. Med. Inform. Assoc. 2007, 14, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Ou, L.; Hollis, S.J. A Systematic Review of the Impact of Routine Collection of Patient Reported Outcome Measures on Patients, Providers and Health Organisations in an Oncologic Setting. BMC Health Serv. Res. 2013, 13, 211. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, F.; Mittica, G.; Cagnazzo, C.; Longo, V.; Berchialla, P.; Solinas, G.; Culotta, P.; Martinello, R.; Foresto, M.; Gallizioli, S.; et al. Self-Evaluation of Adjuvant Chemotherapy-Related Adverse Effects by Patients with Breast Cancer. JAMA Oncol. 2016, 2, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Kotronoulas, G.; Kearney, N.; Maguire, R.; Harrow, A.; Di Domenico, D.; Croy, S.; MacGillivray, S. What Is the Value of the Routine Use of Patient-Reported Outcome Measures Toward Improvement of Patient Outcomes, Processes of Care, and Health Service Outcomes in Cancer Care? A Systematic Review of Controlled Trials. J. Clin. Oncol. 2014, 32, 1480–1501. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Kris, M.G.; Scher, H.I.; Hudis, C.A.; Sabbatini, P.; Rogak, L.; Bennett, A.V.; Dueck, A.C.; Atkinson, T.M.; et al. Symptom Monitoring With Patient-Reported Outcomes During Routine Cancer Treatment: A Randomized Controlled Trial. JCO 2015, 34, 557–565. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197–198. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of Depression, Anxiety, and Adjustment Disorder in Oncological, Haematological, and Palliative-Care Settings: A Meta-Analysis of 94 Interview-Based Studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef]
- Batty, G.D.; Russ, T.C.; Stamatakis, E.; Kivimäki, M. Psychological Distress in Relation to Site Specific Cancer Mortality: Pooling of Unpublished Data from 16 Prospective Cohort Studies. BMJ 2017, 356, j108. [Google Scholar] [CrossRef]
- Carlson, L.E.; Groff, S.L.; Maciejewski, O.; Bultz, B.D. Screening for Distress in Lung and Breast Cancer Outpatients: A Randomized Controlled Trial. J. Clin. Oncol. 2010, 28, 4884–4891. [Google Scholar] [CrossRef]
- Mustafa, M.; Carson-Stevens, A.; Gillespie, D.; Edwards, A.G.K. Psychological Interventions for Women with Metastatic Breast Cancer. Cochrane Database Syst. Rev. 2013, 6, CD004253. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Distress Management (Version 1.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/distress.pdf (accessed on 23 December 2021).
- Roth, A.J.; Kornblith, A.B.; Batel-Copel, L.; Peabody, E.; Scher, H.I.; Holland, J.C. Rapid Screening for Psychologic Distress in Men with Prostate Carcinoma. Cancer 1998, 82, 1904–1908. [Google Scholar] [CrossRef]
- Donovan, K.A.; Grassi, L.; McGinty, H.L.; Jacobsen, P.B. Validation of the Distress Thermometer Worldwide: State of the Science. Psycho-Oncology 2014, 23, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Artz, D.; Dulko, D.; Scher, K.; Sabbatini, P.; Hensley, M.; Mitra, N.; Speakman, J.; McCabe, M.; Schrag, D. Patient Online Self-Reporting of Toxicity Symptoms During Chemotherapy. J. Clin. Oncol. 2005, 23, 3552–3561. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 23 December 2021).
- Dueck, A.C.; Mendoza, T.R.; Mitchell, S.A.; Reeve, B.B.; Castro, K.M.; Rogak, L.J.; Atkinson, T.M.; Bennett, A.V.; Denicoff, A.M.; O’Mara, A.M.; et al. Validity and Reliability of the US National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). JAMA Oncol. 2015, 1, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Osoba, D.; Rodrigues, G.; Myles, J.; Zee, B.; Pater, J. Interpreting the Significance of Changes in Health-Related Quality-of-Life Scores. J. Clin. Oncol. 1998, 16, 139–144. [Google Scholar] [CrossRef]
- ECOG-ACRIN Cancer Research Group. ECOG Performance Status. Available online: https://ecog-acrin.org/resources/ecog-performance-status (accessed on 19 August 2021).
- Gundy, C.M.; Fayers, P.M.; Groenvold, M.; Petersen, M.A.; Scott, N.W.; Sprangers, M.A.G.; Velikova, G.; Aaronson, N.K. Comparing Higher Order Models for the EORTC QLQ-C30. Qual. Life Res. 2012, 21, 1607–1617. [Google Scholar] [CrossRef]
- Giesinger, J.M.; Kieffer, J.M.; Fayers, P.M.; Groenvold, M.; Petersen, M.A.; Scott, N.W.; Sprangers, M.A.G.; Velikova, G.; Aaronson, N.K. Replication and Validation of Higher Order Models Demonstrated That a Summary Score for the EORTC QLQ-C30 Is Robust. J. Clin. Epidemiol. 2016, 69, 79–88. [Google Scholar] [CrossRef]
- Shaik, F.; Uldrick, T.S.; Esterhuizen, T.; Mosam, A. Health-Related Quality of Life in Patients Treated With Antiretroviral Therapy Only Versus Chemotherapy and Antiretroviral Therapy for HIV-Associated Kaposi Sarcoma: A Randomized Control Trial. JGO 2018, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jeppe, C.Y.; Becker, P.; Smith, M.D. Post-Frey Procedure Quality of Life in South African Patients with Painful Chronic Pancreatitis. JOP J. Pancreas 2013, 14, 21–30. [Google Scholar]
- Jacobsen, P.B.; Donovan, K.A.; Trask, P.C.; Fleishman, S.B.; Zabora, J.; Baker, F.; Holland, J.C. Screening for Psychologic Distress in Ambulatory Cancer Patients: A Multicenter Evaluation of the Distress Thermometer. Cancer 2005, 103, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Wouters, E.; le Roux Booysen, F.; Ponnet, K.; Loon, F.B.V. Wording Effects and the Factor Structure of the Hospital Anxiety & Depression Scale in HIV/AIDS Patients on Antiretroviral Treatment in South Africa. PLoS ONE 2012, 7, e34881. [Google Scholar] [CrossRef]
- Central Intelligence Agency. The World Factbook 2018; Central Intelligence Agency: Washington, DC, USA, 2018. [Google Scholar]
- Grimes, B.F. Ethnologue: Languages of the World, 14th ed.; SIL International: Dallas, TX, USA, 2000. [Google Scholar]
- Khuluvhe, M. Fact Sheet: Adult Literacy in South Africa; Department of Higher Education and Training: Pretoria, South Africa, 2021. [Google Scholar]
- Coovadia, H.; Jewkes, R.; Barron, P.; Sanders, D.; McIntyre, D. The Health and Health System of South Africa: Historical Roots of Current Public Health Challenges. Lancet 2009, 374, 817–834. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research Electronic Data Capture (REDCap)—A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Sachs, M.C. Generate ROC Curve Charts for Print and Interactive Use. Available online: https://cran.r-project.org/web/packages/plotROC/vignettes/examples.html (accessed on 24 September 2021).
- Belachew, S.A.; Erku, D.A.; Mekuria, A.B.; Gebresillassie, B.M. Pattern of Chemotherapy-Related Adverse Effects among Adult Cancer Patients Treated at Gondar University Referral Hospital, Ethiopia: A Cross-Sectional Study. DHPS 2016, 8, 83–90. [Google Scholar] [CrossRef]
- Dano, D.; Hénon, C.; Sarr, O.; Ka, K.; Ba, M.; Badiane, A.; Thiam, I.; Diene, P.; Diop, M.; Dem, A.; et al. Quality of Life During Chemotherapy for Breast Cancer in a West African Population in Dakar, Senegal: A Prospective Study. JGO 2019, 5, 1–9. [Google Scholar] [CrossRef]
- Wang, T.Q.; Samuel, J.N.; Brown, M.C.; Vennettilli, A.; Solomon, H.; Eng, L.; Liang, M.; Gill, G.; Merali, Z.; Tian, C.; et al. Routine Surveillance of Chemotherapy Toxicities in Cancer Patients Using the Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE). Oncol. Ther. 2018, 6, 189–201. [Google Scholar] [CrossRef]
- Pearce, A.; Haas, M.; Viney, R.; Pearson, S.-A.; Haywood, P.; Brown, C.; Ward, R. Incidence and Severity of Self-Reported Chemotherapy Side Effects in Routine Care: A Prospective Cohort Study. PLoS ONE 2017, 12, e0184360. [Google Scholar] [CrossRef] [PubMed]
- Nakaganda, A.; Solt, K.; Kwagonza, L.; Driscoll, D.; Kampi, R.; Orem, J. Challenges Faced by Cancer Patients in Uganda: Implications for Health Systems Strengthening in Resource Limited Settings. J. Cancer Policy 2021, 27, 100263. [Google Scholar] [CrossRef]
- Adisa, A.O.; Lawal, O.O.; Adesunkanmi, A.R.K. Evaluation of Patients\’ Adherence to Chemotherapy for Breast Cancer. Afr. J. Health Sci. 2008, 15, 22–27. [Google Scholar] [CrossRef][Green Version]
- Ingwu, J.-A.; Idoko, C.; Israel, C.-E.; Maduakolam, I.; Madu, O. Factors Influencing Non–Adherence to Chemotherapy: Perspective of Nigerian Breast Cancer Survivors. Nurs. Pract. Today 2019, 6. [Google Scholar] [CrossRef]
- O’Neil, D.S.; Nxumalo, S.; Ngcamphalala, C.; Tharp, G.; Jacobson, J.S.; Nuwagaba-Biribonwoha, H.; Dlamini, X.; Pace, L.E.; Neugut, A.I.; Harris, T.G. Breast Cancer Early Detection in Eswatini: Evaluation of a Training Curriculum and Patient Receipt of Recommended Follow-Up Care. JCO Glob. Oncol. 2021, 7, 1349–1357. [Google Scholar] [CrossRef]
- Lambert, M.; Mendenhall, E.; Kim, A.W.; Cubasch, H.; Joffe, M.; Norris, S.A. Health System Experiences of Breast Cancer Survivors in Urban South Africa. Womens Health 2020, 16, 1745506520949419. [Google Scholar] [CrossRef]
- Edwards, L.B.; Greeff, L.E. Exploring Grassroots Feedback about Cancer Challenges in South Africa: A Discussion of Themes Derived from Content Thematic Analysis of 316 Photo-Narratives. Pan Afr. Med. J. 2017, 28, 173. [Google Scholar] [CrossRef]
- Nguyen, H.; Butow, P.; Dhillon, H.; Morris, L.; Brown, A.; West, K.; Sundaresan, P. Using Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs) in Routine Head and Neck Cancer Care: What Do Health Professionals Perceive as Barriers and Facilitators? J. Med. Imaging Radiat. Oncol. 2020, 64, 704–710. [Google Scholar] [CrossRef]
- Graupner, C.; Breukink, S.O.; Mul, S.; Claessens, D.; Slok, A.H.M.; Kimman, M.L. Patient-Reported Outcome Measures in Oncology: A Qualitative Study of the Healthcare Professional’s Perspective. Support Care Cancer 2021, 29, 5253–5261. [Google Scholar] [CrossRef]
- Jagsi, R.; Chiang, A.; Polite, B.N.; Medeiros, B.C.; McNiff, K.; Abernethy, A.P.; Zon, R.; Loehrer, P.J. Qualitative Analysis of Practicing Oncologists’ Attitudes and Experiences Regarding Collection of Patient-Reported Outcomes. JOP 2013, 9, e290–e297. [Google Scholar] [CrossRef]
- Nic Giolla Easpaig, B.; Tran, Y.; Bierbaum, M.; Arnolda, G.; Delaney, G.P.; Liauw, W.; Ward, R.L.; Olver, I.; Currow, D.; Girgis, A.; et al. What Are the Attitudes of Health Professionals Regarding Patient Reported Outcome Measures (PROMs) in Oncology Practice? A Mixed-Method Synthesis of the Qualitative Evidence. BMC Health Serv. Res. 2020, 20, 102. [Google Scholar] [CrossRef] [PubMed]
- Rensburg, Z.J. van Levels of Health Literacy and English Comprehension in Patients Presenting to South African Primary Healthcare Facilities. Afr. J. Prim. Health Care Fam. Med. 2020, 12, 6. [Google Scholar] [CrossRef]
- Global Oncology. Cancer Education Materials. Available online: https://globalonc.org/patient-education-materials/ (accessed on 24 October 2019).
- Gardiner, M. Education in Rural Areas; Issues in Education Policy, No. 4; Centre for Education Policy Development: Johannesburg, South Africa, 2008. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Full Cohort n = 196 |
|---|---|
| n (%) | |
| Sex | |
| Female | 152 (77.6) |
| Male | 44 (22.5) |
| Age in years (Median, IQR) | 52.3 (43.3–61.3) |
| Race | |
| Black | 157 (80.1) |
| White | 19 (9.7) |
| Mixed Race | 17 (8.7) |
| Asian | 2 (1.0) |
| Other | 1 (0.5) |
| Primary/Home Language | |
| IsiZulu | 56 (28.6) |
| English | 38 (19.4) |
| Sesotho | 30 (15.4) |
| Sepedi | 10 (5.1) |
| Tsonga | 10 (5.1) |
| Tswana | 10 (5.1) |
| Other | 41 (20.9) |
| Declined to Answer | 1 (0.5) |
| PRS-SA Language Preference | |
| English | 167 (85.2) |
| IsiZulu | 29 (14.8) |
| Response to “How Well Do You Read English?” Question (n = 167) | |
| Very Well | 87 (52.1) |
| Well | 65 (38.9) |
| Not Well | 14 (8.4) |
| Not At All | 1 (0.6) |
| Response to “How Well Do You Read isiZulu?” Question (n = 29) | |
| Very Well | 13 (44.8) |
| Well | 13 (44.8) |
| Not Well | 3 (10.3) |
| Not At All | 0 (0.0) |
| Relationship Status | |
| Single (Never married) | 81 (41.3) |
| Married/Partnered | 72 (36.7) |
| Divorced/Separated | 20 (10.2) |
| Widowed | 23 (11.7) |
| Employment Status | |
| Unemployed | 97 (49.5) |
| Employed | 56 (28.6) |
| Retired | 41 (20.9) |
| Student | 2 (1.0) |
| Cancer Site | |
| Breast | 102 (52.0) |
| Colorectal | 29 (14.8) |
| Kaposi and Other Sarcomas | 11 (5.6) |
| Stomach | 10 (5.1) |
| Prostate | 8 (4.1) |
| Cervical | 7 (3.6) |
| Lung | 7 (3.6) |
| Ovarian | 5 (2.6) |
| Pancreatic and Biliary | 6 (3.1) |
| Liver | 4 (2.0) |
| Head and Neck | 2 (1.0) |
| Skin/Melanoma | 2 (1.0) |
| Esophagus | 1 (0.5) |
| Uterine | 1 (0.5) |
| Vulvar | 1 (0.5) |
| Cancer Treatments Received Prior to Enrollment | |
| Chemotherapy | 41 (20.9) |
| Surgery | 66 (33.7) |
| Radiation | 29 (14.8) |
| Comorbidities (Self-Report) | |
| Hypertension | 48 (24.5) |
| HIV | 33 (16.8) |
| Diabetes | 13 (6.6) |
| Asthma/COPD | 2 (1.0) |
| Another Cancer | 1 (0.5) |
| Anchor Item | ||||
|---|---|---|---|---|
| Symptom | QLQ-C30 Summary Score | ECOG PS (0–1 vs. 2–4) | ||
| r | p-value | Cohen’s d | p-value | |
| Pain | 0.46 | <0.0001 | 0.81 | <0.0001 |
| Fatigue | 0.65 | <0.0001 | 1.17 | <0.0001 |
| Fever | 0.23 | <0.0001 | 0.51 | 0.02 |
| Dyspnea | 0.45 | <0.0001 | 1.36 | <0.0001 |
| Cough | 0.24 | <0.0001 | 0.62 | <0.0001 |
| Oral Mucositis | 0.40 | <0.0001 | - | 0.16 |
| Nausea | 0.56 | <0.0001 | 0.80 | <0.0001 |
| Vomiting | 0.40 | <0.0001 | 1.02 | <0.0001 |
| Diarrhea | 0.17 | <0.0001 | 0.30 | 0.03 |
| Constipation | 0.40 | <0.0001 | 0.50 | 0.002 |
| Peripheral Neuropathy | 0.41 | <0.0001 | 0.60 | 0.003 |
| Symptom | p-Value |
|---|---|
| Pain | <0.0001 |
| Fatigue | <0.0001 |
| Fever | 0.002 |
| Dyspnea | 0.045 |
| Cough | 0.4 |
| Oral Mucositis | 0.0009 |
| Nausea | <0.0001 |
| Vomiting | <0.0001 |
| Diarrhea | <0.0001 |
| Constipation | 0.007 |
| Peripheral Neuropathy | 0.002 |
| Symptom (n = 175) | Any (n, %) | Grade 3–4 (n, %) | ||
|---|---|---|---|---|
| Any | 173 | 98.9% | 110 | 62.9% |
| Pain | 149 | 85.1% | 68 | 38.9% |
| Fatigue | 156 | 89.1% | 61 | 34.9% |
| Constipation | 96 | 54.9% | 33 | 18.9% |
| Peripheral Neuropathy | 116 | 66.3% | 29 | 16.6% |
| Oral Mucositis | 88 | 50.3% | 24 | 13.7% |
| Fever | 72 | 41.1% | 18 | 10.3% |
| Dyspnea | 59 | 33.7% | 16 | 9.1% |
| Vomiting | 77 | 44.0% | 13 | 7.4% |
| Nausea/Anorexia | 121 | 69.1% | 12 | 6.9% |
| Diarrhea | 67 | 38.3% | 6 | 3.4% |
| Cough | 67 | 38.3% | 5 | 2.9% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanchard, C.L.; Mmoledi, K.; Antoni, M.H.; Demetriou, G.; Joffe, M.; Lopes, G.; Ruff, P.; O’Neil, D.S. Validating an Instrument for Direct Patient Reporting of Distress and Chemotherapy-Related Toxicity among South African Cancer Patients. Cancers 2022, 14, 95. https://doi.org/10.3390/cancers14010095
Blanchard CL, Mmoledi K, Antoni MH, Demetriou G, Joffe M, Lopes G, Ruff P, O’Neil DS. Validating an Instrument for Direct Patient Reporting of Distress and Chemotherapy-Related Toxicity among South African Cancer Patients. Cancers. 2022; 14(1):95. https://doi.org/10.3390/cancers14010095
Chicago/Turabian StyleBlanchard, Charmaine L., Keletso Mmoledi, Michael H. Antoni, Georgia Demetriou, Maureen Joffe, Gilberto Lopes, Paul Ruff, and Daniel S. O’Neil. 2022. "Validating an Instrument for Direct Patient Reporting of Distress and Chemotherapy-Related Toxicity among South African Cancer Patients" Cancers 14, no. 1: 95. https://doi.org/10.3390/cancers14010095
APA StyleBlanchard, C. L., Mmoledi, K., Antoni, M. H., Demetriou, G., Joffe, M., Lopes, G., Ruff, P., & O’Neil, D. S. (2022). Validating an Instrument for Direct Patient Reporting of Distress and Chemotherapy-Related Toxicity among South African Cancer Patients. Cancers, 14(1), 95. https://doi.org/10.3390/cancers14010095