
Dedicated Axillary MRI-Based Radiomics Analysis for the Prediction of Axillary Lymph Node Metastasis in Breast Cancer


 , , ,
, , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patients Characteristics
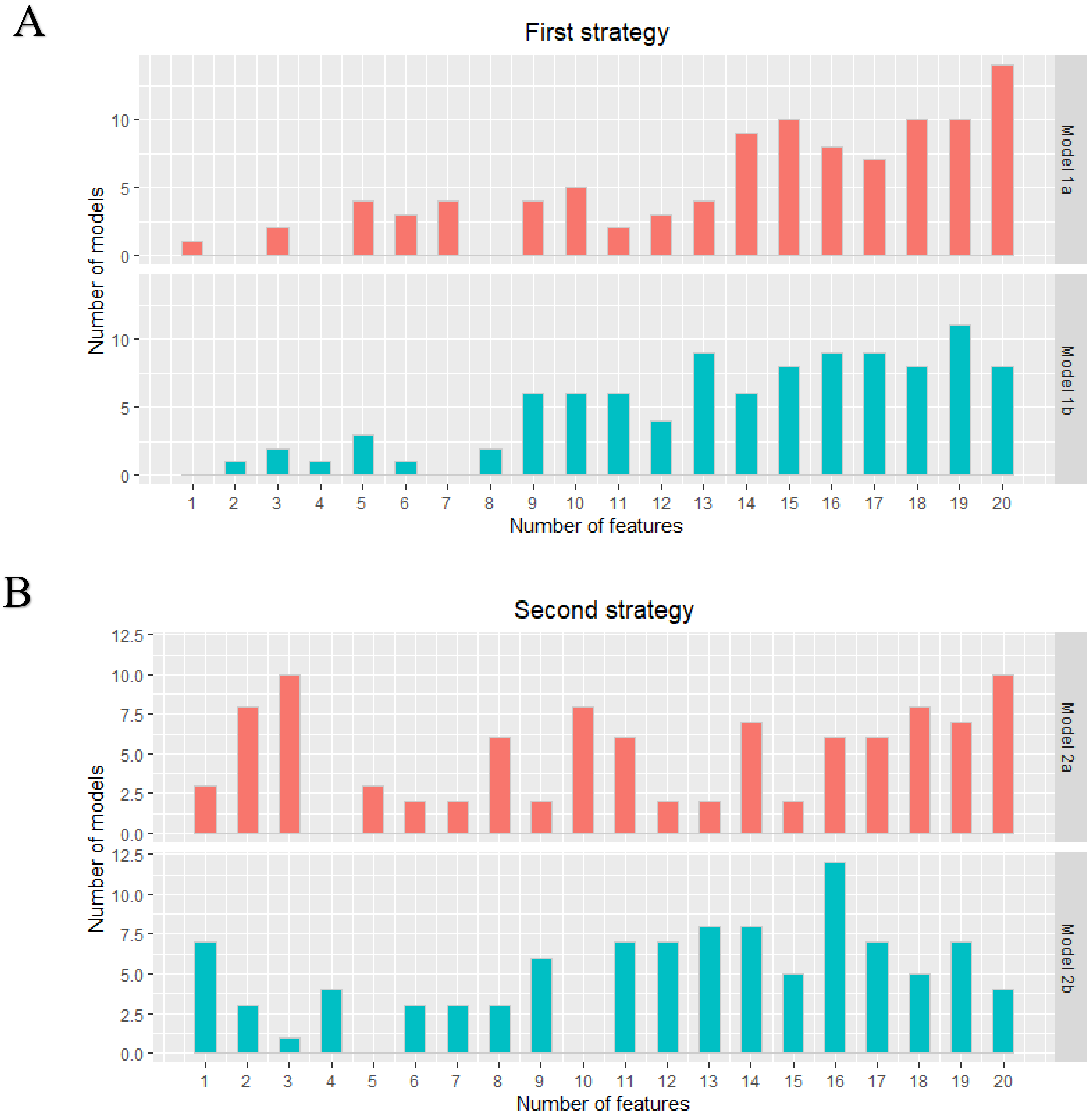
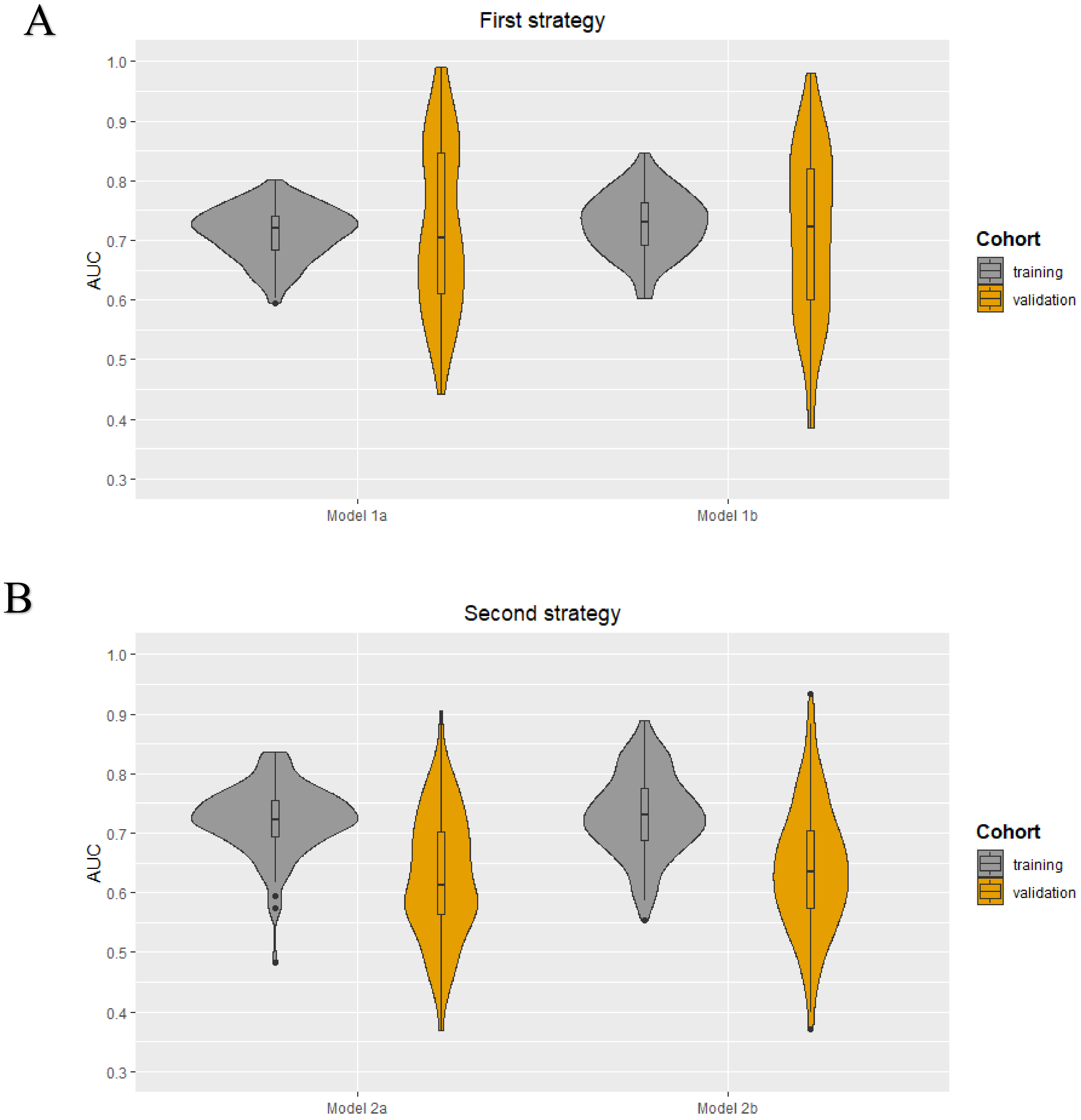
2.2. Radiomics Feature Extraction and Model Development
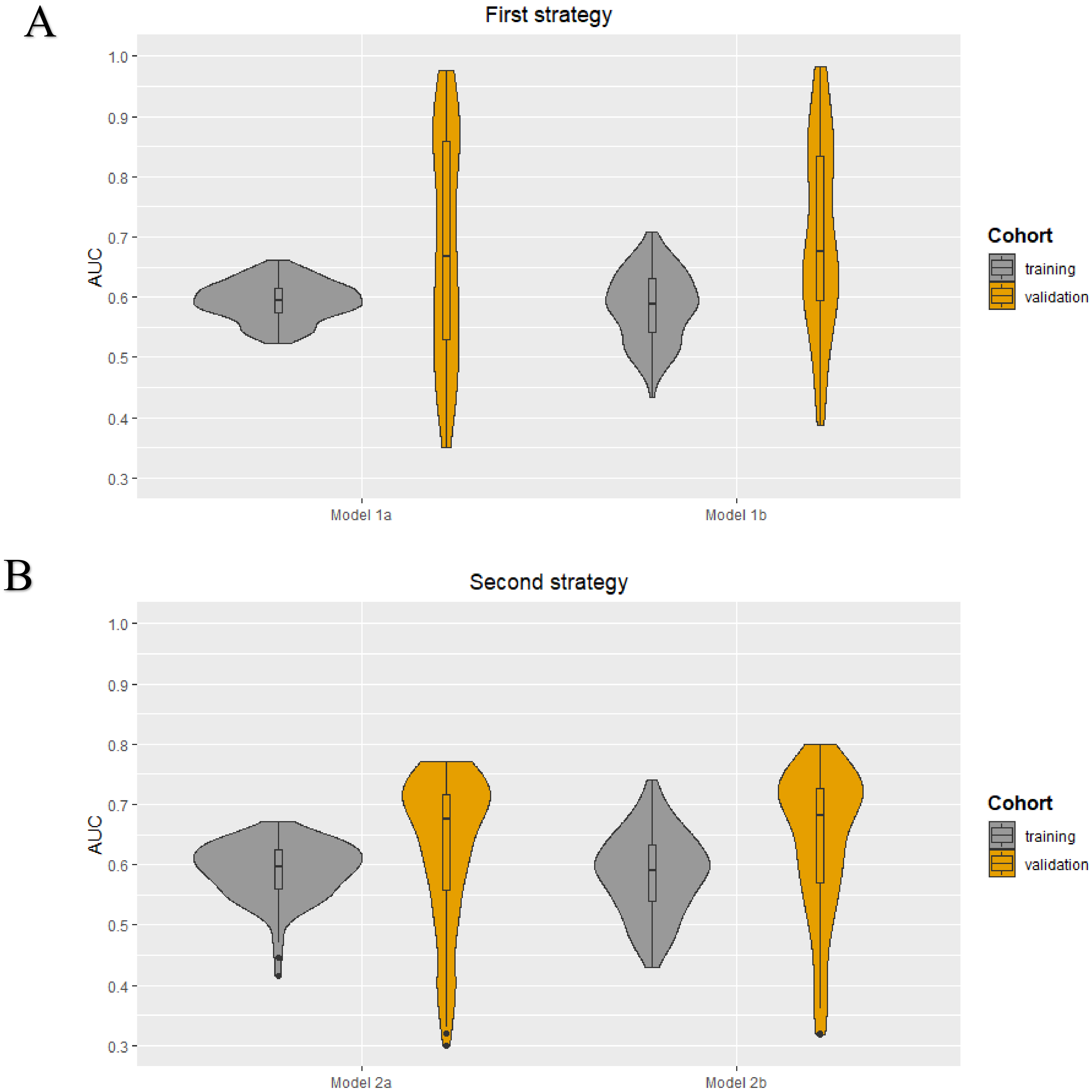
2.3. Radiomics Subanalysis
2.4. Clinical Model Development
2.5. RQS and TRIPOD
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. Clinical and Pathological Characteristics
4.3. MRI Acquisition
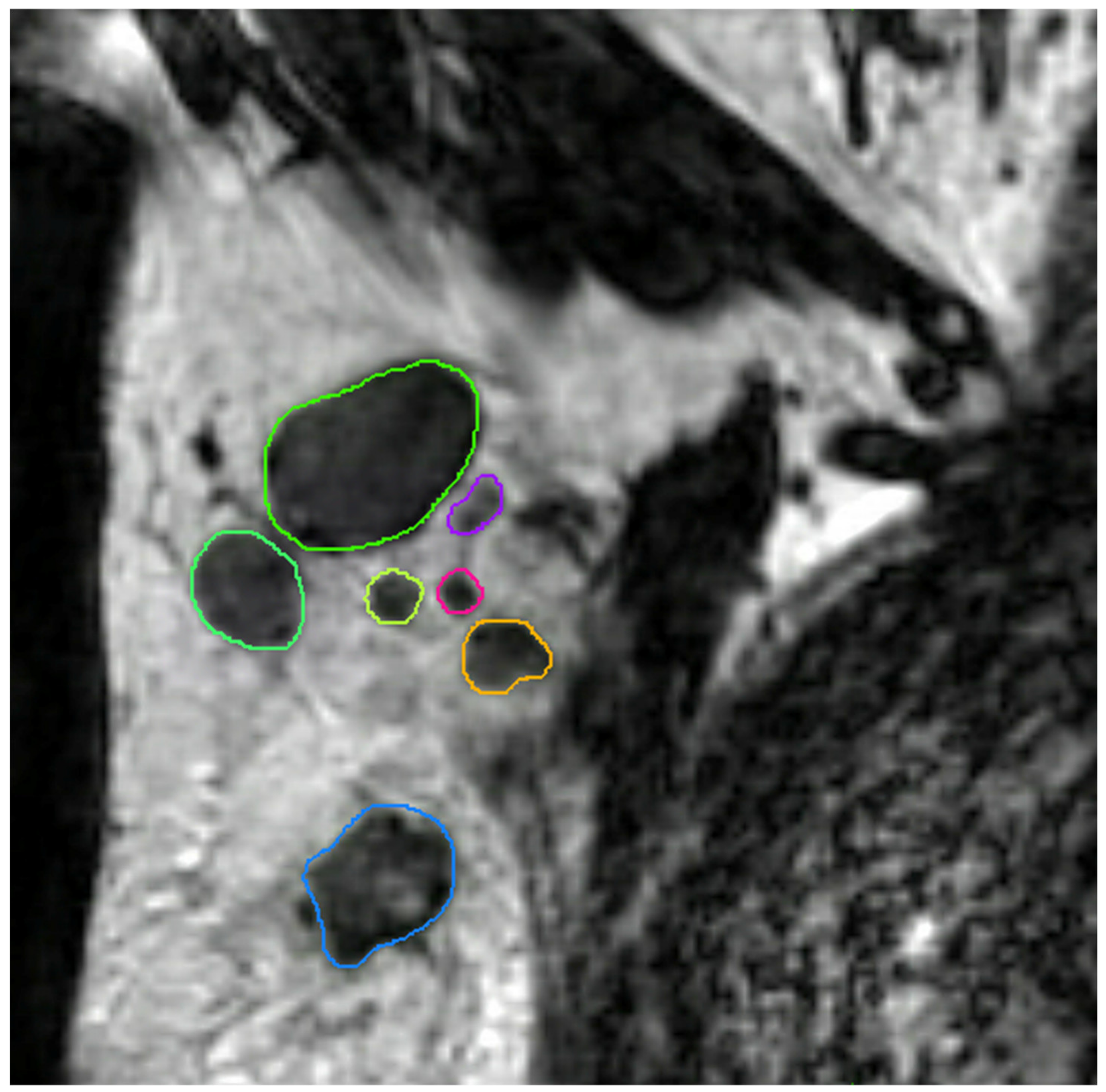
4.4. MRI Lymph Node Delineation
4.5. MRI Preprocessing and Feature Extraction
4.6. Radiomics Feature Selection and Model Development
4.7. Radiomics Subanalysis
4.8. Clinical Model Development
4.9. Statistical Analyses and Study Evaluation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beenken, S.W.; Urist, M.M.; Zhang, Y.; Desmond, R.; Krontiras, H.; Medina, H.; Bland, K.I. Axillary lymph node status, but not tumor size, predicts locoregional recurrence and overall survival after mastectomy for breast cancer. Ann. Surg. 2003, 237, 732–738. [Google Scholar] [CrossRef]
- Soerjomataram, I.; Louwman, M.W.; Ribot, J.G.; Roukema, J.A.; Coebergh, J.W. An overview of prognostic factors for long-term survivors of breast cancer. Breast Cancer Res. Treat. 2008, 107, 309–330. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.L.; Allen, C.; Henson, D.E. Relation of tumor size, lymph node status, and survival in 24,740 breast cancer cases. Cancer 1989, 63, 181–187. [Google Scholar] [CrossRef]
- Fisher, B.; Bauer, M.; Wickerham, D.L.; Redmond, C.K.; Fisher, E.R.; Cruz, A.B.; Foster, R.; Gardner, B.; Lerner, H.; Margolese, R.; et al. Relation of number of positive axillary nodes to the prognosis of patients with primary breast cancer. An NSABP update. Cancer 1983, 52, 1551–1557. [Google Scholar] [CrossRef]
- Surveillance, Epidemiology, and End Results Program (SEER). Table 4.13: Cancer of the Female Breast (Invasive). 5-Year Relative and Period Survival by Race, Diagnosis Year, Age and Stage at Diagnosis. In: SEER Cancer Statistics Review (CSR) 1975-2012. Available online: https://seer.cancer.gov/archive/csr/1975_2012/browse_csr.php?sectionSEL=4&pageSEL=sect_04_table.13.html (accessed on 31 May 2020).
- Senkus, E.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rutgers, E.; Zackrisson, S.; Cardoso, F.; Committee, E.G. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. S5), v8–v30. [Google Scholar] [CrossRef]
- Caudle, A.S.; Cupp, J.A.; Kuerer, H.M. Management of axillary disease. Surg. Oncol. Clin. N. Am. 2014, 23, 473–486. [Google Scholar] [CrossRef]
- Sardanelli, F.; Boetes, C.; Borisch, B.; Decker, T.; Federico, M.; Gilbert, F.J.; Helbich, T.; Heywang-Kobrunner, S.H.; Kaiser, W.A.; Kerin, M.J.; et al. Magnetic resonance imaging of the breast: Recommendations from the EUSOMA working group. Eur. J. Cancer 2010, 46, 1296–1316. [Google Scholar] [CrossRef] [PubMed]
- Van Nijnatten, T.J.A.; Ploumen, E.H.; Schipper, R.J.; Goorts, B.; Andriessen, E.H.; Vanwetswinkel, S.; Schavemaker, M.; Nelemans, P.; de Vries, B.; Beets-Tan, R.G.H.; et al. Routine use of standard breast MRI compared to axillary ultrasound for differentiating between no, limited and advanced axillary nodal disease in newly diagnosed breast cancer patients. Eur. J. Radiol. 2016, 85, 2288–2294. [Google Scholar] [CrossRef]
- Kvistad, K.A.; Rydland, J.; Smethurst, H.B.; Lundgren, S.; Fjosne, H.E.; Haraldseth, O. Axillary lymph node metastases in breast cancer: Preoperative detection with dynamic contrast-enhanced MRI. Eur. Radiol. 2000, 10, 1464–1471. [Google Scholar] [CrossRef]
- Murray, A.D.; Staff, R.T.; Redpath, T.W.; Gilbert, F.J.; Ah-See, A.K.; Brookes, J.A.; Miller, I.D.; Payne, S. Dynamic contrast enhanced MRI of the axilla in women with breast cancer: Comparison with pathology of excised nodes. Br. J. Radiol. 2002, 75, 220–228. [Google Scholar] [CrossRef]
- Schipper, R.J.; Paiman, M.L.; Beets-Tan, R.G.; Nelemans, P.J.; de Vries, B.; Heuts, E.M.; van de Vijver, K.K.; Keymeulen, K.B.; Brans, B.; Smidt, M.L.; et al. Diagnostic Performance of Dedicated Axillary T2- and Diffusion-weighted MR Imaging for Nodal Staging in Breast Cancer. Radiology 2015, 275, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Feng, Q.; Yang, W.; Lu, Z.; Deng, C.; Zhang, L.; Lian, Z.; Liu, J.; Luo, X.; Pei, S.; et al. Preoperative prediction of sentinel lymph node metastasis in breast cancer based on radiomics of T2-weighted fat-suppression and diffusion-weighted MRI. Eur. Radiol. 2018, 28, 582–591. [Google Scholar] [CrossRef]
- Han, L.; Zhu, Y.; Liu, Z.; Yu, T.; He, C.; Jiang, W.; Kan, Y.; Dong, D.; Tian, J.; Luo, Y. Radiomic nomogram for prediction of axillary lymph node metastasis in breast cancer. Eur. Radiol. 2019, 29, 3820–3829. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.B.; Wang, T.; Yang, L.F.; Wang, Y.B.; Li, H.M.; Zhou, X.B.; Zhao, W.L.; Ren, J.C.; Li, X.Y.; Tian, J.; et al. Preoperative Prediction of Axillary Lymph Node Metastasis in Breast Cancer Using Mammography-Based Radiomics Method. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Yu, F.H.; Wang, J.X.; Ye, X.H.; Deng, J.; Hang, J.; Yang, B. Ultrasound-based radiomics nomogram: A potential biomarker to predict axillary lymph node metastasis in early-stage invasive breast cancer. Eur. J. Radiol. 2019, 119, 108658. [Google Scholar] [CrossRef]
- Liu, C.; Ding, J.; Spuhler, K.; Gao, Y.; Serrano Sosa, M.; Moriarty, M.; Hussain, S.; He, X.; Liang, C.; Huang, C. Preoperative prediction of sentinel lymph node metastasis in breast cancer by radiomic signatures from dynamic contrast-enhanced MRI. J. Magn. Reson. Imaging 2019, 49, 131–140. [Google Scholar] [CrossRef]
- Chai, R.M.; Ma, H.; Xu, M.J.; Arefan, D.; Cui, X.Y.; Liu, Y.; Zhang, L.N.; Wu, S.D.; Xu, K. Differentiating axillary lymph node metastasis in invasive breast cancer patients: A comparison of radiomic signatures from multiparametric breast MR sequences. J. Magn. Reson. Imaging 2019, 50, 1125–1132. [Google Scholar] [CrossRef]
- Tan, H.N.; Gan, F.W.; Wu, Y.P.; Zhou, J.; Tian, J.; Lin, Y.S.; Wang, M.Y. Preoperative Prediction of Ancillary Lymph Node Metastasis in Breast Carcinoma Using Radiomics Features Based on the Fat-Suppressed T2 Sequence. Acad. Radiol. 2020, 27, 1217–1225. [Google Scholar] [CrossRef]
- Court, L.E.; Fave, X.; Mackin, D.; Lee, J.; Yang, J.Z.; Zhang, L.F. Computational resources for radiomics. Transl. Cancer Res. 2016, 5, 340–348. [Google Scholar] [CrossRef]
- Ho, T.Y.; Chao, C.H.; Chin, S.C.; Ng, S.H.; Kang, C.J.; Tsang, N.M. Classifying Neck Lymph Nodes of Head and Neck Squamous Cell Carcinoma in MRI Images with Radiomic Features. J. Digit. Imaging 2020, 33, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, J.; Dan, Y.; Yao, Y.; Dai, W.; Cai, G.; Yang, G.; Tong, T. A clinical-radiomics nomogram for the preoperative prediction of lymph node metastasis in colorectal cancer. J. Transl. Med. 2020, 18, 46. [Google Scholar] [CrossRef]
- Samiei, S.; Smidt, M.L.; Vanwetswinkel, S.; Engelen, S.M.E.; Schipper, R.J.; Lobbes, M.B.I.; van Nijnatten, T.J.A. Diagnostic performance of standard breast MRI compared to dedicated axillary MRI for assessment of node-negative and node-positive breast cancer. Eur. Radiol. 2020, 30, 4212–4222. [Google Scholar] [CrossRef] [PubMed]
- Buvat, I.; Orlhac, F. The Dark Side of Radiomics: On the Paramount Importance of Publishing Negative Results. J. Nucl. Med. 2019, 60, 1543–1544. [Google Scholar] [CrossRef]
- Saha, A.; Grimm, L.J.; Harowicz, M.; Ghate, S.V.; Kim, C.; Walsh, R.; Mazurowski, M.A. Interobserver variability in identification of breast tumors in MRI and its implications for prognostic biomarkers and radiogenomics. Med. Phys. 2016, 43, 4558. [Google Scholar] [CrossRef] [PubMed]
- Granzier, R.W.Y.; Verbakel, N.M.H.; Ibrahim, A.; van Timmeren, J.E.; van Nijnatten, T.J.A.; Leijenaar, R.T.H.; Lobbes, M.B.I.; Smidt, M.L.; Woodruff, H.C. MRI-based radiomics in breast cancer: Feature robustness with respect to inter-observer segmentation variability. Sci. Rep. 2020, 10, 14163. [Google Scholar] [CrossRef]
- Van Nijnatten, T.J.A.; Schipper, R.J.; Lobbes, M.B.I.; van Roozendaal, L.M.; Voo, S.; Moossdorff, M.; Paiman, M.L.; de Vries, B.; Keymeulen, K.; Wildberger, J.E.; et al. Diagnostic performance of gadofosveset-enhanced axillary MRI for nodal (re)staging in breast cancer patients: Results of a validation study. Clin. Radiol. 2018, 73, 168–175. [Google Scholar] [CrossRef]
- Schipper, R.J.; Smidt, M.L.; van Roozendaal, L.M.; Castro, C.J.; de Vries, B.; Heuts, E.M.; Keymeulen, K.B.; Wildberger, J.E.; Lobbes, M.B.; Beets-Tan, R.G. Noninvasive nodal staging in patients with breast cancer using gadofosveset-enhanced magnetic resonance imaging: A feasibility study. Investig. Radiol. 2013, 48, 134–139. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Racine, J.S. RStudio: A platform-independent IDE for R and Sweave. J. Appl. Econom. 2012, 27, 167–172. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| No. of patients | 75 |
| Age (years) (median; IQR) | 61 (51–68) |
| Clinical tumor size (mm) (median, IQR) | 19 (13–28) |
| Clinical tumor stage (%) | |
| T1 | 41 (54.7) |
| T2 | 32 (42.7) |
| T3 | 2 (2.6) |
| Clinical nodal stage (%) | |
| N0 | 68 (90.7) |
| N1 | 7 (9.3) |
| Tumor histology (%) | |
| Invasive ductal | 55 (73.3) |
| Invasive lobular | 11 (14.7) |
| Mixed invasive ductal & lobular | 3 (4.0) |
| Other | 6 (8.0) |
| Tumor grade (%) | |
| 1 | 17 (22.7) |
| 2 | 42 (56.0) |
| 3 | 16 (21.3) |
| Breast cancer subtype (%) | |
| ER + HER2− | 55 (73.3) |
| ER + HER2+ | 6 (9.0) |
| ER − HER2+ | 2 (2.7) |
| Triple-negative | 11 (14.7) |
| Not determined | 1 (1.3) |
| Axillary surgery (%) | |
| SLNB | 8 (10.7) |
| ALND | 67 (89.3) |
| Diagnostic Parameters | Training | Validation | Training | Validation | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sens (%) | Spec (%) | PPV (%) | NPV (%) | Sens (%) | Spec (%) | PPV (%) | NPV (%) | Sens (%) | Spec (%) | PPV (%) | NPV (%) | Sens (%) | Spec (%) | PPV (%) | NPV (%) | |
| First Strategy | ||||||||||||||||
| Model 1a | Model 1b | |||||||||||||||
| Minimum | 30 | 71 | 46 | 62 | 0 | 78 | 0 | 98 | 53 | 50 | 55 | 72 | 0 | 57 | 0 | 98 |
| Median | 47 | 81 | 61 | 72 | 33 | 90 | 2 | 99 | 66 | 67 | 67 | 80 | 50 | 75 | 1 | 99 |
| Maximum | 66 | 91 | 78 | 79 | 100 | 97 | 22 | 100 | 83 | 85 | 83 | 88 | 100 | 88 | 10 | 100 |
| Second Strategy | ||||||||||||||||
| Model 2a | Model 2b | |||||||||||||||
| Minimum | 7 | 58 | 25 | 54 | 0 | 33 | 0 | 22 | 48 | 46 | 52 | 68 | 0 | 0 | 0 | 0 |
| Median | 50 | 81 | 62 | 74 | 33 | 76 | 50 | 71 | 66 | 68 | 67 | 80 | 64 | 60 | 50 | 75 |
| Maximum | 74 | 93 | 80 | 83 | 82 | 100 | 100 | 88 | 82 | 92 | 90 | 89 | 100 | 100 | 100 | 100 |
| Diagnostic Parameters | Training | Validation | Training | Validation | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sens (%) | Spec (%) | PPV (%) | NPV (%) | Sens (%) | Spec (%) | PPV (%) | NPV (%) | Sens (%) | Spec (%) | PPV (%) | NPV (%) | Sens (%) | Spec (%) | PPV (%) | NPV (%) | |
| First Strategy | ||||||||||||||||
| Model 1a | Model 1b | |||||||||||||||
| Minimum | 18 | 64 | 42 | 65 | 0 | 40 | 0 | 99 | 31 | 46 | 41 | 42 | 0 | 14 | 0 | 97 |
| Median | 50 | 86 | 68 | 72 | 0 | 91 | 0 | 99 | 58 | 74 | 70 | 64 | 50 | 64 | 1 | 99 |
| Maximum | 64 | 93 | 71 | 78 | 100 | 99 | 18 | 100 | 71 | 92 | 85 | 73 | 100 | 88 | 9 | 100 |
| Second Strategy | ||||||||||||||||
| Model 2a | Model 2b | |||||||||||||||
| Minimum | 0 | 55 | 48 | 61 | 0 | 0 | 10 | 34 | 33 | 45 | 43 | 43 | 0 | 0 | 10 | 0 |
| Median | 42 | 85 | 68 | 72 | 39 | 80 | 69 | 73 | 57 | 75 | 70 | 63 | 61 | 53 | 43 | 67 |
| Maximum | 65 | 100 | 73 | 80 | 100 | 100 | 73 | 84 | 73 | 91 | 86 | 74 | 100 | 100 | 100 | 86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samiei, S.; Granzier, R.W.Y.; Ibrahim, A.; Primakov, S.; Lobbes, M.B.I.; Beets-Tan, R.G.H.; van Nijnatten, T.J.A.; Engelen, S.M.E.; Woodruff, H.C.; Smidt, M.L. Dedicated Axillary MRI-Based Radiomics Analysis for the Prediction of Axillary Lymph Node Metastasis in Breast Cancer. Cancers 2021, 13, 757. https://doi.org/10.3390/cancers13040757
Samiei S, Granzier RWY, Ibrahim A, Primakov S, Lobbes MBI, Beets-Tan RGH, van Nijnatten TJA, Engelen SME, Woodruff HC, Smidt ML. Dedicated Axillary MRI-Based Radiomics Analysis for the Prediction of Axillary Lymph Node Metastasis in Breast Cancer. Cancers. 2021; 13(4):757. https://doi.org/10.3390/cancers13040757
Chicago/Turabian StyleSamiei, Sanaz, Renée W. Y. Granzier, Abdalla Ibrahim, Sergey Primakov, Marc B. I. Lobbes, Regina G. H. Beets-Tan, Thiemo J. A. van Nijnatten, Sanne M. E. Engelen, Henry C. Woodruff, and Marjolein L. Smidt. 2021. "Dedicated Axillary MRI-Based Radiomics Analysis for the Prediction of Axillary Lymph Node Metastasis in Breast Cancer" Cancers 13, no. 4: 757. https://doi.org/10.3390/cancers13040757
APA StyleSamiei, S., Granzier, R. W. Y., Ibrahim, A., Primakov, S., Lobbes, M. B. I., Beets-Tan, R. G. H., van Nijnatten, T. J. A., Engelen, S. M. E., Woodruff, H. C., & Smidt, M. L. (2021). Dedicated Axillary MRI-Based Radiomics Analysis for the Prediction of Axillary Lymph Node Metastasis in Breast Cancer. Cancers, 13(4), 757. https://doi.org/10.3390/cancers13040757