MRI-Based Radiomics Input for Prediction of 2-Year Disease Recurrence in Anal Squamous Cell Carcinoma

 , , , ,
, , , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patients Characteristics
2.2. Outcome
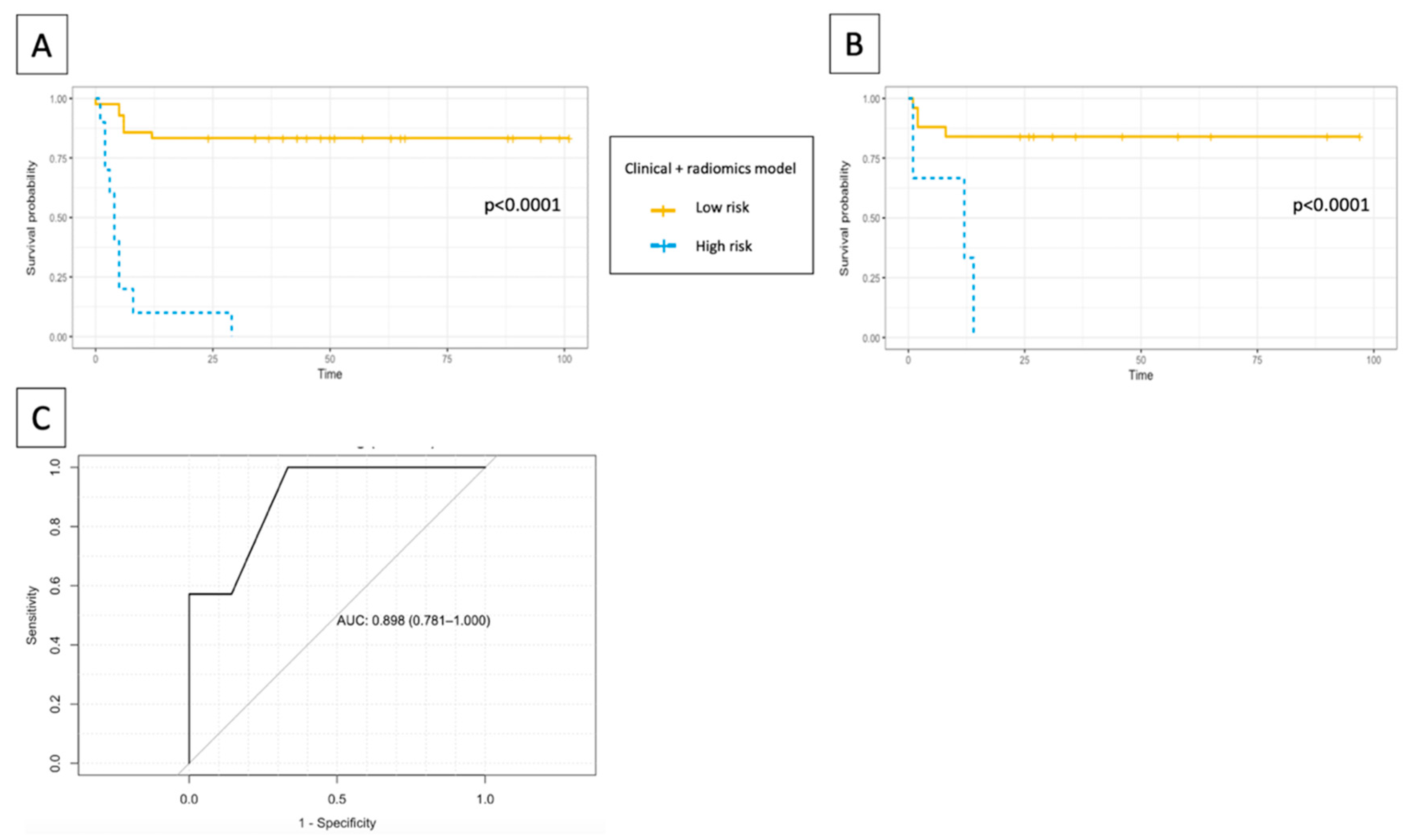
2.3. Logistic Regression
2.4. Inter-Reader Variability
3. Discussion
4. Materials and Methods
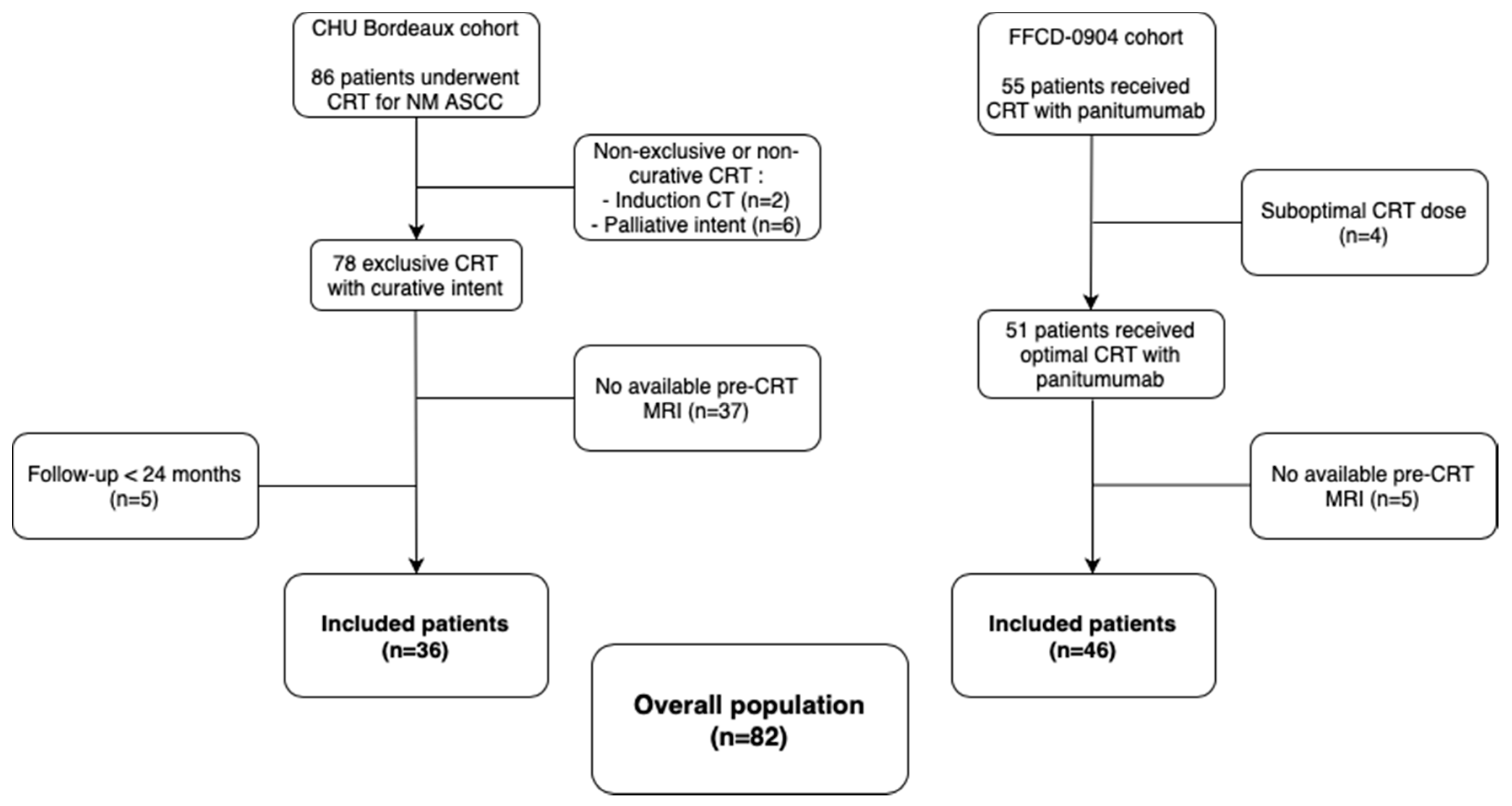
4.1. Patient Selection
4.2. Outcome
4.3. MRI
4.4. Clinical Features and Treatment-Related Data
4.5. Chemo-Radiotherapy
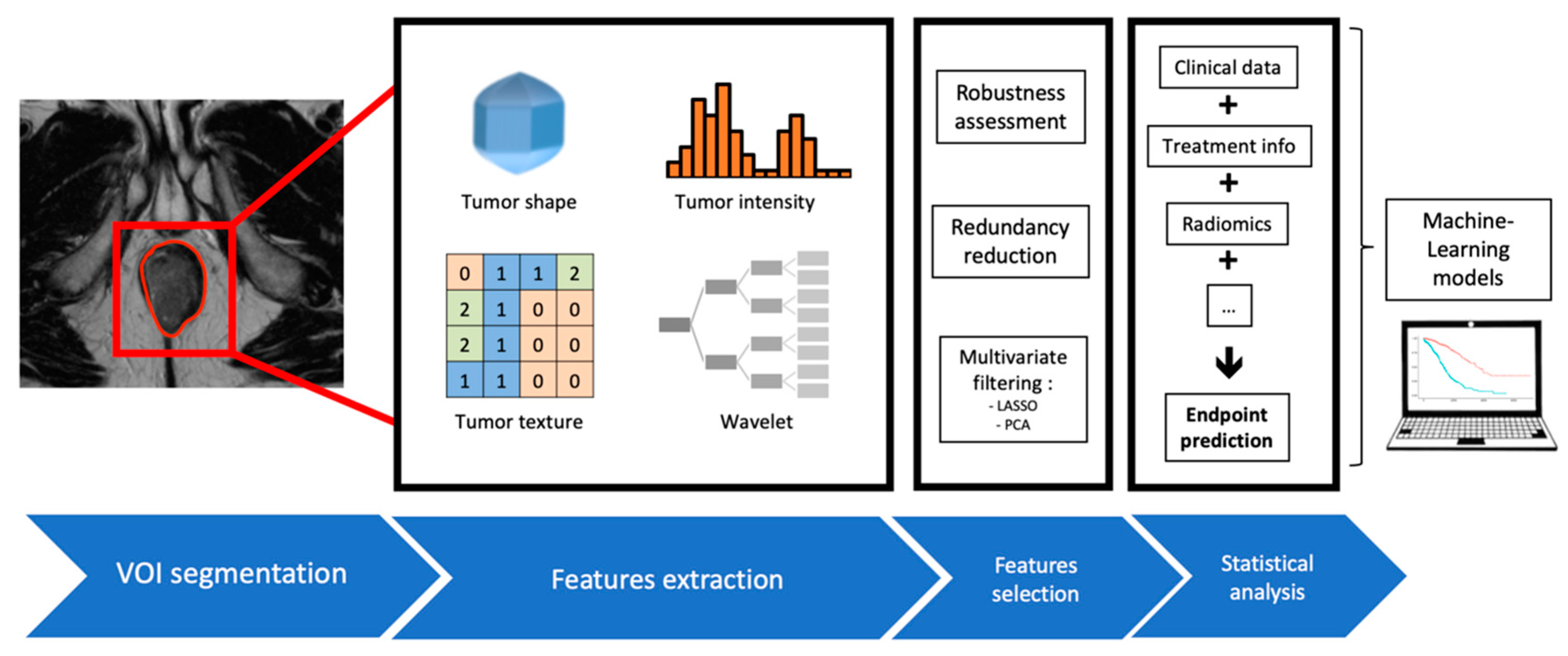
4.6. Tumor Delineation
4.7. MRI Presampling
4.8. Radiomic Features
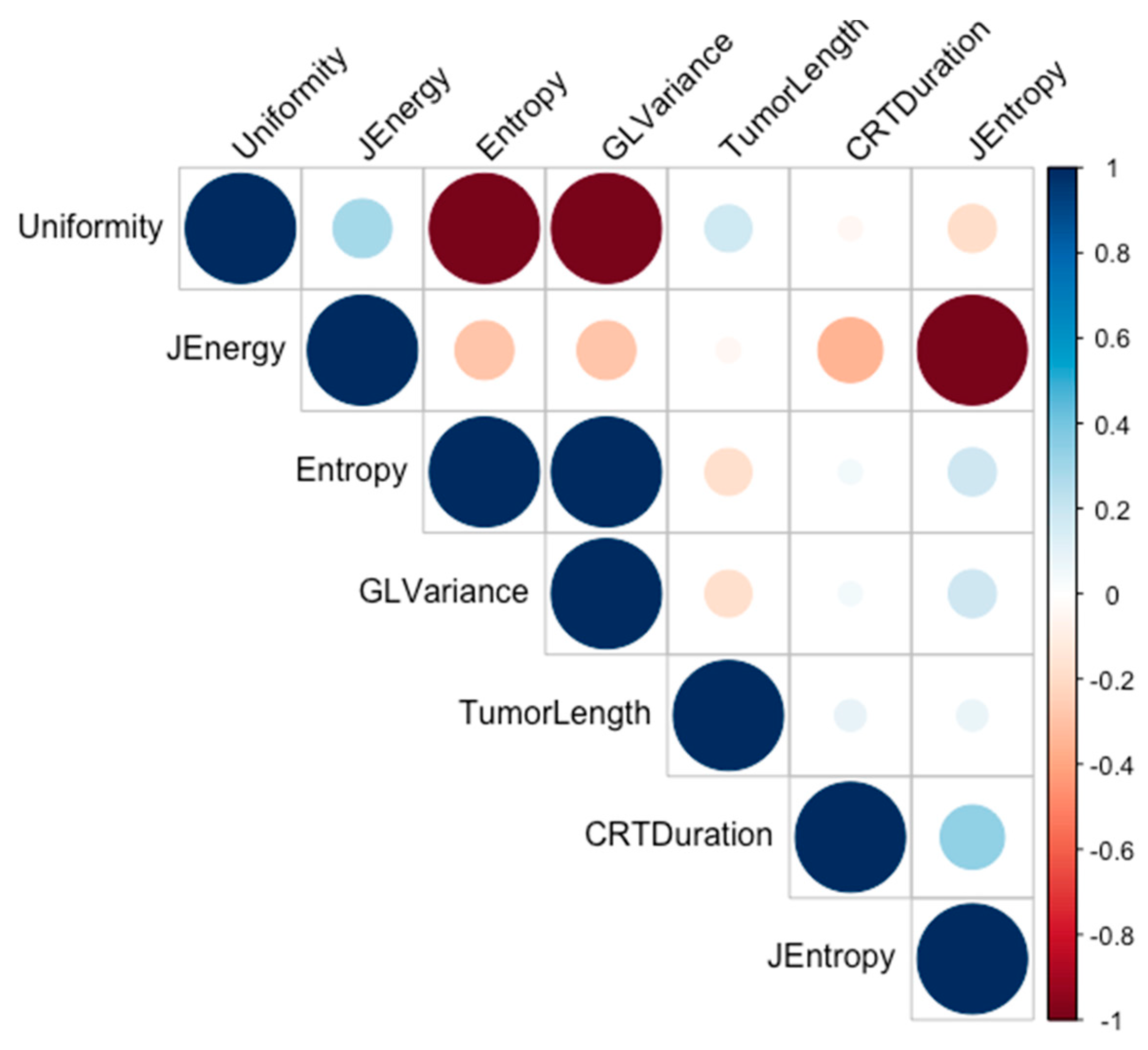
4.9. Statistical Analysis and Feature Selection
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Bosset, J.F.; Pavy, J.J.; Roelofsen, F.; Bartelink, H. Combined radiotherapy and chemotherapy for anal cancer EORTC Radiotherapy and Gastrointestinal Cooperative Groups. Lancet 1997, 349, 205–206. [Google Scholar] [CrossRef]
- UKCCCR. Epidermoid anal cancer: Results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Coordinating Committee on Cancer Research. Lancet 1996, 348, 1049–1054. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Nilsson, P.J.; Aschele, C.; Goh, V.; Peiffert, D.; Cervantes, A.; Arnold, D.; European Society for Medical Oncology (ESMO), European Society of Surgical Oncology (ESSO), European Society of Radiotherapy and Oncology (ESTRO). Anal cancer: ESMO-ESSO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Eur. J. Surg. Oncol. 2014, 40, 1165–1176. [Google Scholar] [CrossRef] [PubMed]
- Ajani, J.A.; Winter, K.A.; Gunderson, L.L.; Pedersen, J.; Benson, A.B.; Thomas, C.R.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; Willett, C. Fluorouracil, mitomycin, and radiotherapy vs. fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: A randomized controlled trial. JAMA 2008, 299, 1914–1921. [Google Scholar] [CrossRef]
- James, R.D.; Glynne-Jones, R.; Meadows, H.M.; Cunningham, D.; Myint, A.S.; Saunders, M.P.; Maughan, T.; McDonald, A.; Essapen, S.; Leslie, M.; et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): A randomised, phase 3, open-label, 2 × 2 factorial trial. Lancet Oncol. 2013, 14, 516–524. [Google Scholar] [CrossRef]
- Shridhar, R.; Shibata, D.; Chan, E.; Thomas, C.R. Anal cancer: Current standards in care and recent changes in practice. CA Cancer. J. Clin. 2015, 65, 139–162. [Google Scholar] [CrossRef]
- Renehan, A.G.; Saunders, M.P.; Schofield, P.F.; O’Dwyer, S.T. Patterns of local disease failure and outcome after salvage surgery in patients with anal cancer. Br. J. Surg. 2005, 92, 605–612. [Google Scholar] [CrossRef]
- Northover, J.; Glynne-Jones, R.; Sebag-Montefiore, D.; James, R.; Meadows, H.; Wan, S.; Jitlal, M.; Ledermann, J. Chemoradiation for the treatment of epidermoid anal cancer: 13- year follow-up of the first randomised UKCCCR Anal Cancer Trial (ACT I). Br. J. Cancer 2010, 102, 1123–1128. [Google Scholar] [CrossRef]
- Peiffert, D.; Tournier-Rangeard, L.; Gérard, J.P.; Lemanski, C.; Francois, E.; Giovannini, M.; Cvitkovic, F.; Mirabel, X.; Bouche, O.; Luporsi, E.; et al. Induction chemotherapy and dose intensification of the radiation boost in locally advanced anal canal carcinoma: Final analysis of the randomized UNICANCER ACCORD 03 trial. J. Clin. Oncol. 2012, 30, 1941–1948. [Google Scholar] [CrossRef]
- Garg, M.K.; Zhao, F.; Sparano, J.A.; Palefsky, J.; Whittington, R.; Mitchell, E.P.; Mulcahy, M.F.; Armstrong, K.I.; Nabbout, N.H.; Kalnicki, S.; et al. Cetuximab Plus Chemoradiotherapy in Immunocompetent Patients with Anal Carcinoma: A Phase II Eastern Cooperative Oncology Group–American College of Radiology Imaging Network Cancer Research Group Trial (E3205). J. Clin. Oncol. 2017, 35, 718. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Lee, J.Y.; Palefsky, J.; Henry, D.H.; Wachsman, W.; Rajdev, L.; Aboulafia, D.; Ratner, L.; Fitzgerald, T.J.; Kachnic, L.; et al. Cetuximab Plus Chemoradiotherapy for HIV-Associated Anal Carcinoma: A Phase II AIDS Malignancy Consortium Trial. J. Clin. Oncol. 2017, 35, 727. [Google Scholar] [CrossRef] [PubMed]
- Sclafani, F.; Rao, S. Systemic Therapies for Advanced Squamous Cell Anal Cancer. Curr. Oncol. Rep. 2018, 20, 53. [Google Scholar] [CrossRef] [PubMed]
- Vendrely, V.; Lemanski, C.; Gnep, K.; Barbier, E.; Hajbi, F.E.; Lledo, G.; Dahan, L.; Terrebonne, E.; Manfredi, S.; Mirabel, X.; et al. Anti-epidermal growth factor receptor therapy in combination with chemoradiotherapy for the treatment of locally advanced anal canal carcinoma: Results of a phase I dose-escalation study with panitumumab (FFCD 0904). Radiother. Oncol. 2019, 140, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Bian, J.J.; Almhanna, K. Anal cancer and immunotherapy-are we there yet? Transl. Gastroenterol. Hepatol. 2019, 4, 57. [Google Scholar] [CrossRef]
- Bibault, J.E.; Xing, L.; Giraud, P.; El Ayachy, R.; Giraud, N.; Decazes, P.; Burgun, A.; Giraud, P. Radiomics: A primer for the radiation oncologist. Cancer Radiother. 2020, 24, 403–410. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Kourou, K. Machine learning applications in cancer prognosis and prediction. Comput. Struct. Biotechnol. J. 2015, 13, 8–17. [Google Scholar] [CrossRef]
- Schick, U.; Lucia, F.; Dissaux, G.; Visvikis, D.; Badic, B.; Masson, I.; Pradier, O.; Bourbonne, V.; Hatt, M. MRI-derived radiomics: Methodology and clinical applications in the field of pelvic oncology. BJR Br. J. Radiol. 2019, 92, 20190105. [Google Scholar] [CrossRef]
- Giraud, N.; Sargos, P.; Leduc, N.; Saut, O.; Vuong, T.; Vendrely, V. Radiomics and Machine Learning in Anal Squamous Cell Carcinoma: A New Step for Personalized Medicine? Appl. Sci. 2020, 10, 1988. [Google Scholar] [CrossRef]
- Bartelink, H.; Roelofsen, F.; Eschwege, F.; Rougier, P.; Bosset, J.F.; Gonzalez, D.G.; Peiffert, D.; Van Glabbeke, M.; Pierart, M. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: Results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J. Clin. Oncol. 1997, 15, 2040–2049. [Google Scholar] [PubMed]
- Myerson, R.J.; Kong, F.; Birnbaum, E.H.; Fleshman, J.W.; Kodner, I.J.; Picus, J.; Ratkin, G.A.; Read, T.E.; Walz, B.J. Radiation therapy for epidermoid carcinoma of the anal canal, clinical and treatment factors associated with outcome. Radiother. Oncol. J. Eur. Soc. Radiol. Oncol. 2001, 61, 15–22. [Google Scholar] [CrossRef]
- Faivre, J.C.; Peiffert, D.; Vendrely, V.; Lemanski, C.; Hannoun-Levi, J.M.; Mirabel, X.; Stanbury, T.; Salleron, J.; Guillemin, F. Prognostic factors of colostomy free survival in patients presenting with locally advanced anal canal carcinoma: A pooled analysis of two prospective trials (KANAL 2 and ACCORD 03). Radiother. Oncol. 2018, 129, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Toh, E.; Wilson, J.; Sebag-Montefiore, D.; Botterill, I. Neutrophil:lymphocyte ratio as a simple and novel biomarker for prediction of locoregional recurrence after chemoradiotherapy for squamous cell carcinoma of the anus. Colorectal Dis. 2014, 16, O90–O97. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Han, X.; Li, Y.; Zhu, K.; Yu, J. Survival prediction models for patients with anal carcinoma receiving definitive chemoradiation: A population based study. Oncol. Lett. 2019, 19, 1443–1451. [Google Scholar] [CrossRef]
- Hocquelet, A.; Auriac, T.; Perier, C.; Dromain, C.; Meyer, M.; Pinaquy, J.B.; Denys, A.; Trillaud, H.; De Senneville, B.D.; Vendrely, V. Pre-treatment magnetic resonance-based texture features as potential imaging biomarkers for predicting event free survival in anal cancer treated by chemoradiotherapy. Eur. Radiol. 2018, 28, 2801–2811. [Google Scholar] [CrossRef]
- Owczarczyk, K.; Prezzi, D.; Cascino, M.; Kozarski, R.; Gaya, A.; Siddique, M.; Cook, G.J.; Glynne-Jones, R.; Goh, V. MRI heterogeneity analysis for prediction of recurrence and disease free survival in anal cancer. Radiother. Oncol. 2019, 134, 119–126. [Google Scholar] [CrossRef]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. Man. Cybern. 1973, SMC-3, 610–621. [Google Scholar] [CrossRef]
- Mehta, S.; Ramey, S.J.; Kwon, D.; Rich, B.J.; Ahmed, A.A.; Wolfson, A.; Yechieli, R.; Portelance, L.; Mellon, E.A. Impact of radiotherapy duration on overall survival in squamous cell carcinoma of the anus. J. Gastrointest. Oncol. 2020, 11, 277–290. [Google Scholar] [CrossRef]
- del Campo, E.R.; Matzinger, O.; Haustermans, K.; Peiffert, D.; Glynne-Jones, R.; Winter, K.A.; Konski, A.A.; Ajani, J.A.; Bosset, J.F.; Hannoun-Levi, J.M.; et al. Pooled Analysis of external-beam RADiotherapy parameters in phase II and phase III trials in radiochemotherapy in Anal Cancer (PARADAC). Eur. J. Cancer 2019, 121, 130–143. [Google Scholar] [CrossRef]
- Serup-Hansen, E.; Linnemann, D.; Skovrider-Ruminski, W.; Høgdall, E.; Geertsen, P.F.; Havsteen, H. Human Papillomavirus Genotyping and p16 Expression as Prognostic Factors for Patients with American Joint Committee on Cancer Stages I to III Carcinoma of the Anal Canal. JCO J. Clin. Oncol. 2014, 32, 1812–1817. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, D.C.; Williams, A.; Allan, K.; Stokoe, J.; Jackson, T.; Linsdall, S.; Bailey, C.M.; Summers, J. p16INK4A, p53, EGFR expression and KRAS mutation status in squamous cell cancers of the anus: Correlation with outcomes following chemo-radiotherapy. Radiother. Oncol. 2013, 109, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.M.; Goh, V.; Sebag-Montefiore, D.; Gilbert, D.C. Biomarkers in anal cancer: From biological understanding to stratified treatment. Br. J. Cancer 2017, 116, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Zou, K.H.; Warfield, S.K.; Bharatha, A.; Tempany, C.M.; Kaus, M.R.; Haker, S.J.; Wells, W.M., 3rd; Jolesz, F.A.; Kikinis, R. Statistical validation of image segmentation quality based on a spatial overlap index. Acad. Radiol. 2004, 11, 178–189. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bordeaux Cohort (n = 36) | FFCD Cohort (n = 46) | p-Value | |
|---|---|---|---|
| Age at diagnosis (mean, years) | 62.3 | 60.1 | 0.39 |
| Sex: | 0.96 | ||
| - F | 30/36 (83.3%) | 37/46 (80.4%) | |
| - M | 6/36 (16.7%) | 9/46 (19.6%) | |
| HIV status: | 0.79 | ||
| - Positive | 1/36 (2.8%) | 3/46 (6.5%) | |
| - Negative | 35/36 (97.2%) | 43/46 (93.5%) | |
| Tumor length (mean, mm) | 51.2 | 47.5 | 0.40 |
| Pre-rectal tumor infiltration | 16/36 (44.4%) | 13/46 (28.2%) | 0.20 |
| T-stage: | 0.44 | ||
| - cT1-2 | 11/36 (30.6%) | 19/46 (41.2%) | |
| - cT3-4 | 25/36 (69.4%) | 27/46 (58.7%) | |
| N-stage: | 1 | ||
| - cN0 | 10/36 (27.8%) | 12/46 (26.1%) | |
| - cN+ | 26/36 (72.2%) | 34/46 (73.9%) | |
| AJCC groupings: | 0.20 | ||
| - I | 1/36 (2.8%) | 0/46 (0%) | |
| - IIa | 4/36 (11.1%) | 5/46 (10.9%) | |
| - IIb | 1/36 (2.8%) | 4/46 (8.7%) | |
| - IIIa | 6/36 (16.7%) | 14/46 (30.4%) | |
| - IIIb | 4/36 (11.1%) | 3/46 (6.5%) | |
| - IIIc | 20/36 (55.5%) | 20/46 (43.5%) | |
| 2-year DFS | 23/36 (63.9%) | 35/46 (76.1%) | 0.34 |
| FO_Uniformity | Sum of the squares of each intensity value. A greater uniformity implies a greater homogeneity or a smaller range of discrete intensity values. | |
| FO_Entropy | Randomness in the image values, with ϵ an arbitrarily small positive number (≈2.2 × 10−16). | |
| GLCM_JointEnergy | Measure of homogeneous patterns in the image. A greater energy implies more intensity value pairs that neighbor each other at higher frequencies. | |
| GLCM_JointEntropy | Measure of the variability in neighborhood intensity values. | |
| GLRLM_GrayLevelVariance | Variance in gray level intensities for the zones. |
| Variable | Univariate Analysis | Best Cut-Off | p-Value | Multivariate Analysis | |||
|---|---|---|---|---|---|---|---|
| AUC | Se (%) | Sp (%) | Odds-Ratio | p-Value | |||
| Tumor length (mm) | 0.71 (0.56–0.86) | 71 | 65 | 49 | 0.01 | 5.75 | 0.036 |
| CRT duration (days) | 0.67 (0.52–0.83) | 82 | 51 | 50.5 | 0.043 | ||
| FO_Entropy | 0.67 (0.51–0.84) | 59 | 87 | 0.992 | 0.045 | 0.12 | 0.026 |
| GLCM_JointEnergy | 0.67 (0.50–0.84) | 41 | 95 | 0.317 | 0.047 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giraud, N.; Saut, O.; Aparicio, T.; Ronchin, P.; Bazire, L.-A.; Barbier, E.; Lemanski, C.; Mirabel, X.; Etienne, P.-L.; Lièvre, A.; et al. MRI-Based Radiomics Input for Prediction of 2-Year Disease Recurrence in Anal Squamous Cell Carcinoma. Cancers 2021, 13, 193. https://doi.org/10.3390/cancers13020193
Giraud N, Saut O, Aparicio T, Ronchin P, Bazire L-A, Barbier E, Lemanski C, Mirabel X, Etienne P-L, Lièvre A, et al. MRI-Based Radiomics Input for Prediction of 2-Year Disease Recurrence in Anal Squamous Cell Carcinoma. Cancers. 2021; 13(2):193. https://doi.org/10.3390/cancers13020193
Chicago/Turabian StyleGiraud, Nicolas, Olivier Saut, Thomas Aparicio, Philippe Ronchin, Louis-Arnaud Bazire, Emilie Barbier, Claire Lemanski, Xavier Mirabel, Pierre-Luc Etienne, Astrid Lièvre, and et al. 2021. "MRI-Based Radiomics Input for Prediction of 2-Year Disease Recurrence in Anal Squamous Cell Carcinoma" Cancers 13, no. 2: 193. https://doi.org/10.3390/cancers13020193
APA StyleGiraud, N., Saut, O., Aparicio, T., Ronchin, P., Bazire, L.-A., Barbier, E., Lemanski, C., Mirabel, X., Etienne, P.-L., Lièvre, A., Cacheux, W., Darut-Jouve, A., De la Fouchardière, C., Hocquelet, A., Trillaud, H., Charleux, T., Breysacher, G., Argo-Leignel, D., Tessier, A., ... Vendrely, V. (2021). MRI-Based Radiomics Input for Prediction of 2-Year Disease Recurrence in Anal Squamous Cell Carcinoma. Cancers, 13(2), 193. https://doi.org/10.3390/cancers13020193