
Analysis of Italian BRCA1/2 Pathogenic Variants Identifies a Private Spectrum in the Population from the Bergamo Province in Northern Italy

 , , , , , , ,
, , , , , , ,  , , , , , , ,
, , , , , , ,  , add
Show full author list
, add
Show full author list
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Distribution of the PVs Found in BGP
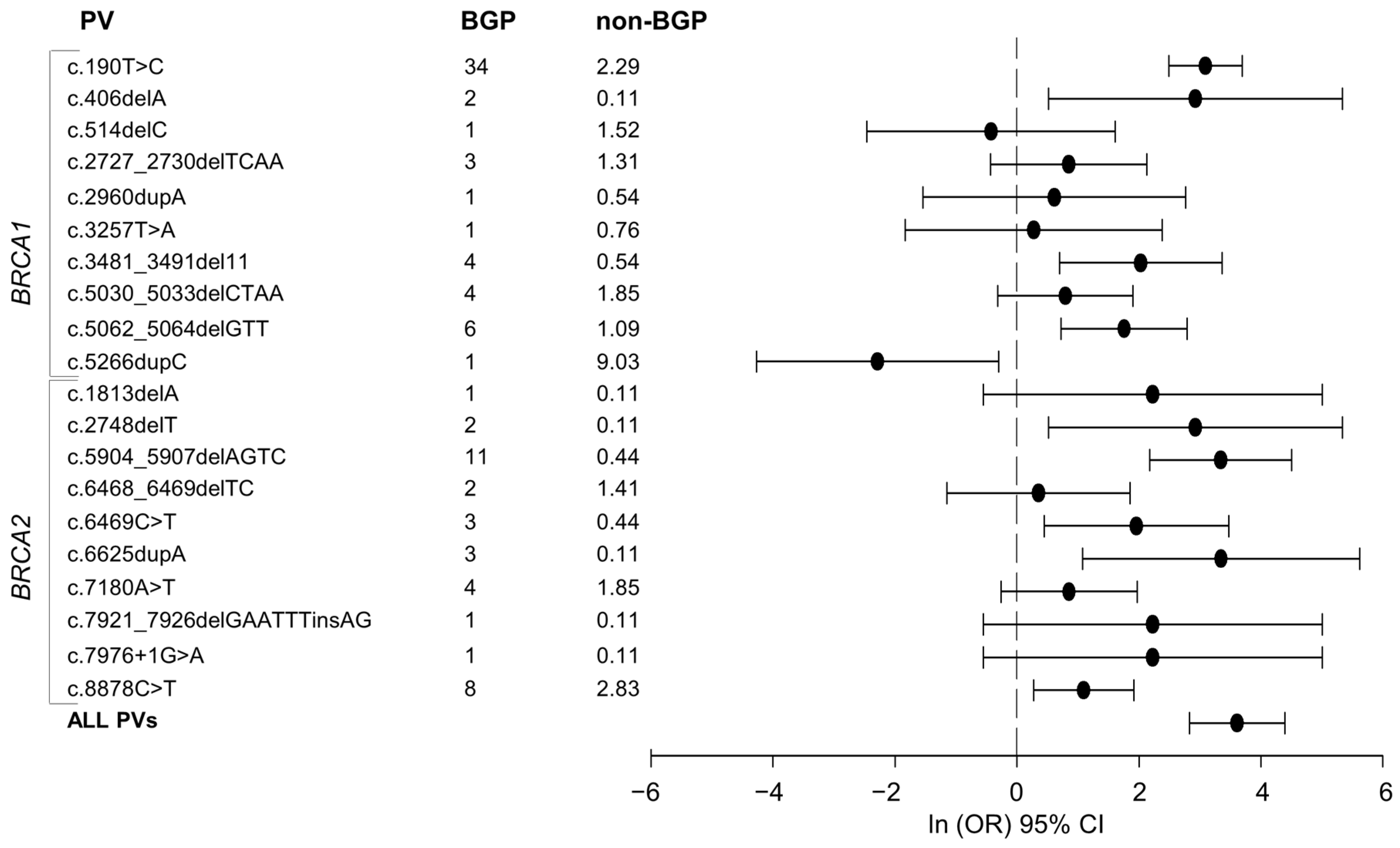
2.2. Comparison between the BGP and Non-BGP PV Spectra
3. Discussion
4. Materials and Methods
4.1. BRCA1/2 PV Carriers
4.2. Heterogeneity of the BRCA1/2 PV Carriers
4.3. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; van Leeuwen, F.E.; Milne, R.L.; Andrieu, N.; et al. Risks of Breast, Ovarian, and Contralateral Breast Cancer for BRCA1 and BRCA2 Mutation Carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Fackenthal, J.D.; Olopade, O.I. Breast cancer risk associated with BRCA1 and BRCA2 in diverse populations. Nat. Rev. Cancer 2007, 7, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Janavicius, R. Founder BRCA1/2 mutations in the Europe: Implications for hereditary breast-ovarian cancer prevention and control. EPMA J. 2010, 1, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, C.; Rahman, N. Genetic predisposition to breast cancer: Past, present, and future. Annu. Rev. Genomics Hum. Genet. 2008, 9, 321–345. [Google Scholar] [CrossRef] [PubMed]
- Roa, B.B.; Boyd, A.A.; Volcik, K.; Richards, C.S. Ashkenazi Jewish population frequencies for common mutations in BRCA1 and BRCA2. Nat. Genet. 1996, 14, 185–187. [Google Scholar] [CrossRef]
- Tonin, P.; Weber, B.; Offit, K.; Couch, F.; Rebbeck, T.R.; Neuhausen, S.; Godwin, A.K.; Daly, M.; Wagner-Costalos, J.; Berman, D.; et al. Frequency of recurrent BRCA1 and BRCA2 mutations in Ashkenazi Jewish breast cancer families. Nat. Med. 1996, 2, 1179–1183. [Google Scholar] [CrossRef]
- Johannesdottir, G.; Gudmundsson, J.; Bergthorsson, J.T.; Arason, A.; Agnarsson, B.A.; Eiriksdottir, G.; Johannsson, O.T.; Borg, A.; Ingvarsson, S.; Easton, D.F.; et al. High prevalence of the 999del5 mutation in icelandic breast and ovarian cancer patients. Cancer Res. 1996, 56, 3663–3665. [Google Scholar]
- Thorlacius, S.; Sigurdsson, S.; Bjarnadottir, H.; Olafsdottir, G.; Jonasson, J.G.; Tryggvadottir, L.; Tulinius, H.; Eyfjord, J.E. Study of a single BRCA2 mutation with high carrier frequency in a small population. Am. J. Hum. Genet. 1997, 60, 1079–1084. [Google Scholar]
- Sarantaus, L.; Huusko, P.; Eerola, H.; Launonen, V.; Vehmanen, P.; Rapakko, K.; Gillanders, E.; Syrjakoski, K.; Kainu, T.; Vahteristo, P.; et al. Multiple founder effects and geographical clustering of BRCA1 and BRCA2 families in Finland. Eur. J. Hum. Genet. 2000, 8, 757–763. [Google Scholar] [CrossRef]
- Hatzikotoulas, K.; Gilly, A.; Zeggini, E. Using population isolates in genetic association studies. Brief. Funct. Genomics 2014, 13, 371–377. [Google Scholar] [CrossRef]
- Xue, Y.; Mezzavilla, M.; Haber, M.; McCarthy, S.; Chen, Y.; Narasimhan, V.; Gilly, A.; Ayub, Q.; Colonna, V.; Southam, L.; et al. Enrichment of low-frequency functional variants revealed by whole-genome sequencing of multiple isolated European populations. Nat. Commun. 2017, 8, 15927. [Google Scholar] [CrossRef] [PubMed]
- Zeggini, E. Using genetically isolated populations to understand the genomic basis of disease. Genome Med. 2014, 6, 83. [Google Scholar] [CrossRef] [PubMed]
- Cocca, M.; Barbieri, C.; Concas, M.P.; Robino, A.; Brumat, M.; Gandin, I.; Trudu, M.; Sala, C.F.; Vuckovic, D.; Girotto, G.; et al. A bird’s-eye view of Italian genomic variation through whole-genome sequencing. Eur. J. Hum. Genet. 2020, 28, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Colonna, V.; Pistis, G.; Bomba, L.; Mona, S.; Matullo, G.; Boano, R.; Sala, C.; Vigano, F.; Torroni, A.; Achilli, A.; et al. Small effective population size and genetic homogeneity in the Val Borbera isolate. Eur. J. Hum. Genet. 2013, 21, 89–94. [Google Scholar] [CrossRef]
- Fiorito, G.; Di Gaetano, C.; Guarrera, S.; Rosa, F.; Feldman, M.W.; Piazza, A.; Matullo, G. The Italian genome reflects the history of Europe and the Mediterranean basin. Eur. J. Hum. Genet. 2016, 24, 1056–1062. [Google Scholar] [CrossRef]
- Grugni, V.; Raveane, A.; Mattioli, F.; Battaglia, V.; Sala, C.; Toniolo, D.; Ferretti, L.; Gardella, R.; Achilli, A.; Olivieri, A.; et al. Reconstructing the genetic history of Italians: New insights from a male (Y-chromosome) perspective. Ann. Hum. Biol. 2018, 45, 44–56. [Google Scholar] [CrossRef]
- Raveane, A.; Aneli, S.; Montinaro, F.; Athanasiadis, G.; Barlera, S.; Birolo, G.; Boncoraglio, G.; Di Blasio, A.M.; Di Gaetano, C.; Pagani, L.; et al. Population structure of modern-day Italians reveals patterns of ancient and archaic ancestries in Southern Europe. Sci. Adv. 2019, 5, eaaw3492. [Google Scholar] [CrossRef]
- Sazzini, M.; Gnecchi Ruscone, G.A.; Giuliani, C.; Sarno, S.; Quagliariello, A.; De Fanti, S.; Boattini, A.; Gentilini, D.; Fiorito, G.; Catanoso, M.; et al. Complex interplay between neutral and adaptive evolution shaped differential genomic background and disease susceptibility along the Italian peninsula. Sci. Rep. 2016, 6, 32513. [Google Scholar] [CrossRef]
- Baudi, F.; Quaresima, B.; Grandinetti, C.; Cuda, G.; Faniello, C.; Tassone, P.; Barbieri, V.; Bisegna, R.; Ricevuto, E.; Conforti, S.; et al. Evidence of a founder mutation of BRCA1 in a highly homogeneous population from southern Italy with breast/ovarian cancer. Hum. Mutat. 2001, 18, 163–164. [Google Scholar] [CrossRef]
- Pisano, M.; Cossu, A.; Persico, I.; Palmieri, G.; Angius, A.; Casu, G.; Palomba, G.; Sarobba, M.G.; Rocca, P.C.; Dedola, M.F.; et al. Identification of a founder BRCA2 mutation in Sardinia. Br. J. Cancer 2000, 82, 553–559. [Google Scholar] [CrossRef]
- Caligo, M.A.; Ghimenti, C.; Cipollini, G.; Ricci, S.; Brunetti, I.; Marchetti, V.; Olsen, R.; Neuhausen, S.; Shattuck-Eidens, D.; Conte, P.F.; et al. BRCA1 germline mutational spectrum in Italian families from Tuscany: A high frequency of novel mutations. Oncogene 1996, 13, 1483–1488. [Google Scholar] [PubMed]
- Papi, L.; Putignano, A.L.; Congregati, C.; Zanna, I.; Sera, F.; Morrone, D.; Falchetti, M.; Turco, M.R.; Ottini, L.; Palli, D.; et al. Founder mutations account for the majority of BRCA1-attributable hereditary breast/ovarian cancer cases in a population from Tuscany, Central Italy. Breast Cancer Res. Treat. 2009, 117, 497–504. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Malacrida, S.; Agata, S.; Callegaro, M.; Casella, C.; Barana, D.; Scaini, M.C.; Manoukian, S.; Oliani, C.; Radice, P.; Barile, M.; et al. BRCA1 p.Val1688del is a deleterious mutation that recurs in breast and ovarian cancer families from Northeast Italy. J. Clin. Oncol. 2008, 26, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Cini, G.; Mezzavilla, M.; Della Puppa, L.; Cupelli, E.; Fornasin, A.; D’Elia, A.V.; Dolcetti, R.; Damante, G.; Bertok, S.; Miolo, G.; et al. Tracking of the origin of recurrent mutations of the BRCA1 and BRCA2 genes in the North-East of Italy and improved mutation analysis strategy. BMC Med. Genet. 2016, 17, 11. [Google Scholar] [CrossRef] [PubMed]
- Caleca, L.; Putignano, A.L.; Colombo, M.; Congregati, C.; Sarkar, M.; Magliery, T.J.; Ripamonti, C.B.; Foglia, C.; Peissel, B.; Zaffaroni, D.; et al. Characterization of an Italian founder mutation in the RING-finger domain of BRCA1. PLoS ONE 2014, 9, e86924. [Google Scholar] [CrossRef] [PubMed]
- Catucci, I.; Casadei, S.; Ding, Y.C.; Volorio, S.; Ficarazzi, F.; Falanga, A.; Marchetti, M.; Tondini, C.; Franchi, M.; Adamson, A.; et al. Haplotype analyses of the c.1027C>T and c.2167_2168delAT recurrent truncating mutations in the breast cancer-predisposing gene PALB2. Breast Cancer Res. Treat. 2016, 160, 121–129. [Google Scholar] [CrossRef]
- Catucci, I.; Peterlongo, P.; Ciceri, S.; Colombo, M.; Pasquini, G.; Barile, M.; Bonanni, B.; Verderio, P.; Pizzamiglio, S.; Foglia, C.; et al. PALB2 sequencing in Italian familial breast cancer cases reveals a high-risk mutation recurrent in the province of Bergamo. Genet. Med. 2014, 16, 688–694. [Google Scholar] [CrossRef][Green Version]
- Laitman, Y.; Friebel, T.M.; Yannoukakos, D.; Fostira, F.; Konstantopoulou, I.; Figlioli, G.; Bonanni, B.; Manoukian, S.; Zuradelli, M.; Tondini, C.; et al. The spectrum of BRCA1 and BRCA2 pathogenic sequence variants in Middle Eastern, North African, and South European countries. Hum. Mutat. 2019, 40, e1–e23. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Friebel, T.M.; Friedman, E.; Hamann, U.; Huo, D.; Kwong, A.; Olah, E.; Olopade, O.I.; Solano, A.R.; Teo, S.H.; et al. Mutational spectrum in a worldwide study of 29,700 families with BRCA1 or BRCA2 mutations. Hum. Mutat. 2018, 39, 593–620. [Google Scholar] [CrossRef]
- Yang, X.; Leslie, G.; Doroszuk, A.; Schneider, S.; Allen, J.; Decker, B.; Dunning, A.M.; Redman, J.; Scarth, J.; Plaskocinska, I.; et al. Cancer Risks Associated With Germline PALB2 Pathogenic Variants: An International Study of 524 Families. J. Clin. Oncol. 2020, 38, 674–685. [Google Scholar] [CrossRef]
- Palmieri, G.; Palomba, G.; Cossu, A.; Pisano, M.; Dedola, M.F.; Sarobba, M.G.; Farris, A.; Olmeo, N.; Contu, A.; Pasca, A.; et al. BRCA1 and BRCA2 germline mutations in Sardinian breast cancer families and their implications for genetic counseling. Ann. Oncol. 2002, 13, 1899–1907. [Google Scholar] [CrossRef] [PubMed]
- De Nicolo, A.; Parisini, E.; Zhong, Q.; Dalla Palma, M.; Stoeckert, K.A.; Domchek, S.M.; Nathanson, K.L.; Caligo, M.A.; Vidal, M.; Cusick, M.E.; et al. Multimodal assessment of protein functional deficiency supports pathogenicity of BRCA1 p.V1688del. Cancer Res. 2009, 69, 7030–7037. [Google Scholar] [CrossRef] [PubMed]
- Barnholtz-Sloan, J.S.; Chakraborty, R.; Sellers, T.A.; Schwartz, A.G. Examining population stratification via individual ancestry estimates versus self-reported race. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1545–1551. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Altman, D.G.; Machin, D.; Bryant, T.N.; Gardner, M.J. Statistics with Confidence, 2nd ed.; BMJ Books: Wiley, UK, 2000; p. 49. [Google Scholar]


{kind=link}
| PVs | Total No. of Carriers | Carrier Distribution (No. of Carriers; Freq%) | Suggested Origin | |
|---|---|---|---|---|
| BGP | Regions | |||
| Common (10) | ||||
| BRCA1:c.190T>C | 55 | (34; 34.0) | Molise (1; 100), Trentino Alto Adige (1; 11.1), Veneto (2; 8.3), Friuli Venezia Giulia (1; 7.1), Lombardy non-BGP (14; 4.8), Piedmont (2; 1.2) | BGP 1 |
| BRCA2:c.5904_5907delAGTC | 15 | (11; 11.0) | Lombardy non-BGP (4; 1.4) | BGP 1 |
| BRCA1:c.2727_2730delTCAA | 15 | (3; 3.0) | Lombardy non-BGP (12; 4.1) | BGP/Lombardy 1 |
| BRCA2:c.6469C>T | 7 | (3; 3.0) | Lombardy non-BGP (4; 1.4) | BGP 1 |
| BRCA2:c.6625dupA | 4 | (3; 3.0) | Lombardy non-BGP (1; 0.3) | BGP 1 |
| BRCA2:c.8878C>T | 34 | (8; 8.0) | Liguria (2; 12.5), Marche (1; 8.3), Lombardy non-BGP (15; 5.1), Veneto (1; 4.2), Piedmont (6; 3.6), Emilia Romagna (1; 2.4) | BGP/Liguria 1 |
| BRCA1:c.5062_5064delGTT | 16 | (6; 6.0) | Trentino Alto Adige (2; 22.2), Veneto (2; 8.3), Lombardy non-BGP (5; 1.7), Piedmont (1; 0.6) | BGP/Trentino Alto Adige 1 |
| BRCA1:c.3481_3491del11 | 9 | (4; 4.0) | Emilia Romagna (3; 7.3), Lombardy non-BGP (2; 0.7) | BGP/Emilia Romagna 2 |
| BRCA1:c.5030_5033delCTAA | 21 | (4; 4.0) | Liguria (3; 18.8), Piedmont (6; 3.6), Sicily (2; 3.2), Emilia Romagna (1; 2.4), Lombardy non-BGP (5; 1.7) | BGP/Liguria 2 |
| BRCA2:c.7180A>T | 20 | (4; 4.0) | Friuli Venezia Giulia (1; 7.1), Lombardy non-BGP (12; 4.1), Piedmont (3; 1.8) | BGP/Friuli Venezia Giulia 1 |
| Rare (15) | ||||
| BRCA1:c.406delA | 3 | (2; 2.0) | Lombardy non-BGP (1; 0.3) | BGP 1 |
| BRCA2:c.2748delT | 3 | (2; 2.0) | Lombardy non-BGP (1; 0.3) | BGP 1 |
| BRCA2:c.5473dupG | 2 | (2; 2.0) | None | BGP 1 |
| BRCA2:c.8085_8086insGG | 2 | (2; 2.0) | None | BGP 1 |
| BRCA1:c.53T>C | 1 | (1; 1.0) | None | BGP 1 |
| BRCA1:c.1961dupA | 1 | (1; 1.0) | None | BGP 2 |
| BRCA1:c.2960dupA | 6 | (1; 1.0) | Lombardy non-BGP (5; 1.7) | BGP/Lombardy 1 |
| BRCA1:c.3257T>A | 8 | (1; 1.0) | Lombardy non-BGP (5; 1.7), Piedmont (2; 1.2) | BGP/Lombardy 1 |
| BRCA2:c.7921_7926delGAATTTinsAG | 2 | (1; 1.0) | Lombardy non-BGP (1; 0.3) | BGP 1 |
| BRCA2:c.7976+1G>A | 2 | (1; 1.0) | Lombardy non-BGP (1; 0.3) | BGP 2 |
| BRCA2:c.8021dupA | 1 | (1; 1.0) | None | BGP 1 |
| BRCA2:c.6468_6469delTC | 15 | (2; 2.0) | Veneto (2; 8.3), Marche (1; 8.3), Tuscany (1; 4.3), Campania (3; 7.5), Apulia (3; 2.1), Piedmont (3; 1.8) | BGP/Campania 1 |
| BRCA2:c.1813delA | 2 | (1; 1.0) | Basilicata (1; 11.1) | BGP/Basilicata 2 |
| BRCA1:c.514delC | 15 | (1; 1.0) | Sicily (8; 12.7), Lombardy non-BGP (4; 1.4), Apulia (1; 1.0), Piedmont (1; 0.6) | Sicily 1 |
| BRCA1:c.5266dupC | 84 | (1; 1.0) | Apulia (31; 30.1), Abruzzo (2; 15.4), Trentino Alto Adige (1; 11.1), Sicily (5; 7.9), Calabria (3; 7.7), Campania (3; 7.5), Lombardy non-BGP (22; 7.5), Piedmont (12; 7.2), Friuli Venezia Giulia (1; 7.1), Liguria (1; 6.3), Emilia Romagna (2; 4.9) | Apulia 2 |
| Non-BGP PV | Non-BGP Carriers (%) | BGP Carriers (%) | BGP—Non-BGP Frequency Difference (95%CI) | p-Value |
|---|---|---|---|---|
| BRCA1:c.5266dupC | 83 (9.0) | 1 (1.0) | −8 (−10.2 to −3.3) | 0.0056 |
| BRCA1:c.190T>C | 21 (2.3) | 34 (34.0) | 31.7 (23.1 to 41.5) | <0.0001 |
| BRCA1:c.5062_5064delGTT | 10 (1.1) | 6 (6.0) | 4.9 (1.6 to 11.4) | 0.0002 |
| BRCA2:c.8878C>T | 26 (2.8) | 8 (8.0) | 5.2 (1.1 to 12.2) | 0.0063 |
| BRCA2:c.7180A>T | 16 (1.7) | 4 (4.0) | 2.3 (−0.4 to 8.1) | 0.1219 |
| BRCA1:c.5030_5033delCTAA | 17 (1.8) | 4 (4.0) | 2.2 (−0.5 to 8) | 0.1509 |
| BRCA1:c.1088delA | 25 (2.7) | 0 (0.0) | −2.7 (−4 to 1.1) | 0.0951 |
| BRCA1:c.181T>G | 20 (2.2) | 0 (0.0) | −2.2 (−3.3 to 1.6) | 0.1361 |
| BRCA2:c.5796_5797delTA | 15 (1.6) | 0 (0.0) | −1.6 (−2.7 to 2.1) | 0.1986 |
| BRCA1:c.3257T>G | 15 (1.6) | 0 (0.0) | −1.6 (−2.7 to 2.1) | 0.1986 |
| Testing-Ascertainment Center | All Carriers | Carriers of BRCA1 PVs (%) | Carriers of BRCA2 PVs (%) |
|---|---|---|---|
| Cogentech-IEO | 353 | 195 (55.2) | 158 (44.8) |
| Cogentech-INT | 309 | 187 (60.5) | 122 (39.5) |
| Cogentech-OPG * | 90 | 53 (58.9) | 38 (41.1) |
| Cogentech-ICH | 61 | 39 (63.9) | 22 (36.1) |
| ACSS * | 206 | 107 (51.9) | 100 (48.1) |
| All cohorts | 1019 * | 581 (57.0) | 440 (43.0) |
| BGP | 100 | 59 (59.0) | 41 (41.0) |
| non-BGP * | 919 | 522 (56.8) | 399 (43.2) |
| All | 1019 * | 581 (57.0) | 440 (43.0) |
| Region | Region of Birth of Carrier Ascertained in | Number of Residents # | Rate * (1:100,000) | |||
|---|---|---|---|---|---|---|
| All Cities | Milan (INT, IEO, ICH) | Turin (ACSS) | Bergamo (OPG) | |||
| Lombardy (Non-BGP) | 293 | 281 | 3 | 9 | 8,987,585 | 3.3 |
| BGP | 100 | 29 | 0 | 71 | 1,116,384 | 9.0 |
| Lazio | 20 | 18 | 2 | 0 | 5,865,544 | 0.3 |
| Campania | 40 | 32 | 7 | 1 | 5,785,861 | 0.7 |
| Sicily | 63 | 50 | 9 | 4 | 4,968,410 | 1.3 |
| Veneto | 24 | 19 | 4 | 1 | 4,907,704 | 0.5 |
| Emilia Romagna | 41 | 35 | 5 | 1 | 4,467,118 | 0.9 |
| Piedmont | 167 | 43 | 124 | 0 | 4,341,375 | 3.9 |
| Apulia | 103 | 85 | 17 | 1 | 4,008,296 | 2.6 |
| Tuscany | 23 | 22 | 1 | 0 | 3,722,729 | 0.6 |
| Calabria | 39 | 27 | 12 | 0 | 1,924,701 | 2.0 |
| Sardinia | 22 | 17 | 3 | 2 | 1,630,474 | 1.4 |
| Liguria | 16 | 13 | 3 | 0 | 1,543,127 | 1.0 |
| Marche | 12 | 11 | 1 | 0 | 1,518,400 | 0.8 |
| Abruzzo | 13 | 10 | 3 | 0 | 1,305,770 | 1.0 |
| Friuli Venezia Giulia | 14 | 8 | 6 | 0 | 1,211,357 | 1.2 |
| Trentino Alto Adige | 9 | 9 | 0 | 0 | 1,074,819 | 0.8 |
| Umbria | 3 | 3 | 0 | 0 | 880,285 | 0.3 |
| Basilicata | 9 | 6 | 3 | 0 | 556,934 | 1.6 |
| Molise | 1 | 1 | 0 | 0 | 302,265 | 0.3 |
| Aosta Valley | 7 | 4 | 3 | 0 | 125,501 | 5.6 |
| All regions (non-BGP) | 919 | 694 | 206 | 19 | 59,128,255 | 1.6 |
| All regions | 1019 | 723 | 206 | 90 | 60,244,639 | 1.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Figlioli, G.; De Nicolo, A.; Catucci, I.; Manoukian, S.; Peissel, B.; Azzollini, J.; Beltrami, B.; Bonanni, B.; Calvello, M.; Bondavalli, D.; et al. Analysis of Italian BRCA1/2 Pathogenic Variants Identifies a Private Spectrum in the Population from the Bergamo Province in Northern Italy. Cancers 2021, 13, 532. https://doi.org/10.3390/cancers13030532
Figlioli G, De Nicolo A, Catucci I, Manoukian S, Peissel B, Azzollini J, Beltrami B, Bonanni B, Calvello M, Bondavalli D, et al. Analysis of Italian BRCA1/2 Pathogenic Variants Identifies a Private Spectrum in the Population from the Bergamo Province in Northern Italy. Cancers. 2021; 13(3):532. https://doi.org/10.3390/cancers13030532
Chicago/Turabian StyleFiglioli, Gisella, Arcangela De Nicolo, Irene Catucci, Siranoush Manoukian, Bernard Peissel, Jacopo Azzollini, Benedetta Beltrami, Bernardo Bonanni, Mariarosaria Calvello, Davide Bondavalli, and et al. 2021. "Analysis of Italian BRCA1/2 Pathogenic Variants Identifies a Private Spectrum in the Population from the Bergamo Province in Northern Italy" Cancers 13, no. 3: 532. https://doi.org/10.3390/cancers13030532
APA StyleFiglioli, G., De Nicolo, A., Catucci, I., Manoukian, S., Peissel, B., Azzollini, J., Beltrami, B., Bonanni, B., Calvello, M., Bondavalli, D., Pasini, B., Vignolo Lutati, F., Ogliara, P., Zuradelli, M., Pensotti, V., De Vecchi, G., Volorio, S., Verderio, P., Pizzamiglio, S., ... Peterlongo, P. (2021). Analysis of Italian BRCA1/2 Pathogenic Variants Identifies a Private Spectrum in the Population from the Bergamo Province in Northern Italy. Cancers, 13(3), 532. https://doi.org/10.3390/cancers13030532