
Quantification of Cancer-Developing Idiopathic Pulmonary Fibrosis Using Whole-Lung Texture Analysis of HRCT Images

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
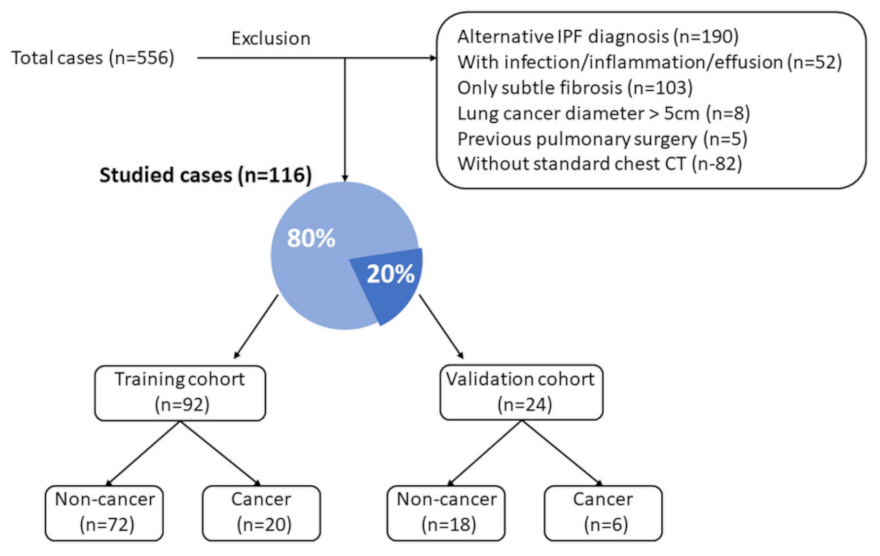
2.1. Patient Selection
2.2. CT Imaging Acquisition Protocols
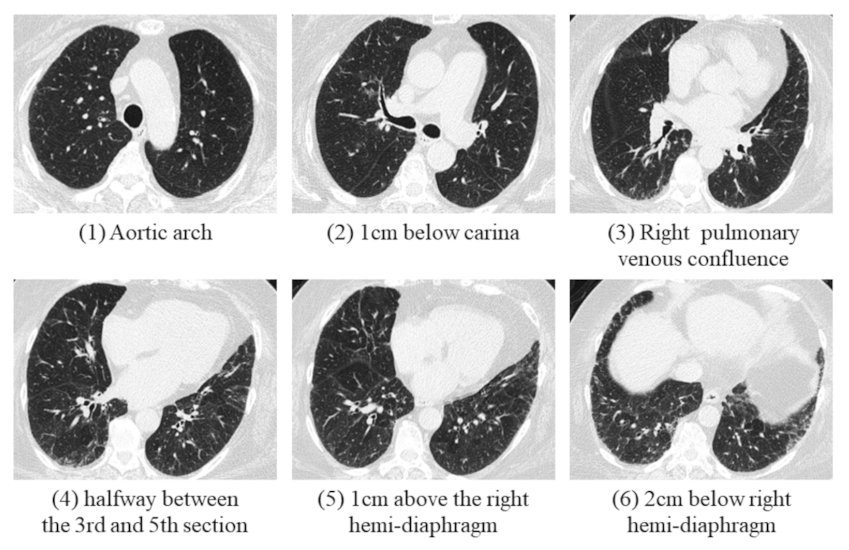
2.3. Image Interpretation
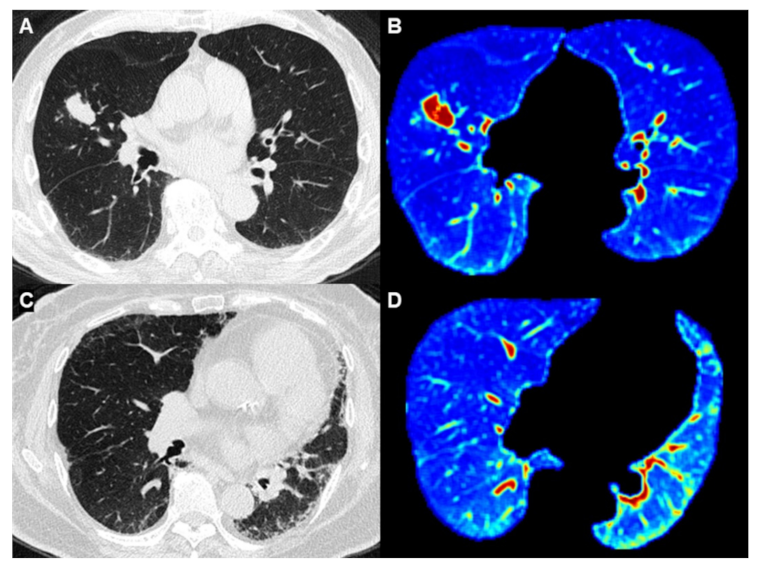
2.4. State-of-the-Art Algorithm for Whole-Lung Parenchyma CT Analysis
2.5. Statistical Analyses
3. Results
3.1. Basic Characteristics
3.2. Inter-Rater Reliability of the Fibrotic Score
3.3. Radiomics Feature Selection for Classifying Cancer and Non-Cancer Groups
3.4. Diagnostic Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Raghu, G.; Amatto, V.C.; Behr, J.; Stowasser, S. Comorbidities in idiopathic pulmonary fibrosis patients: A systematic literature review. Eur. Respir. J. 2015, 46, 1113–1130. [Google Scholar] [CrossRef] [PubMed]
- Kato, E.; Takayanagi, N.; Takaku, Y.; Kagiyama, N.; Kanauchi, T.; Ishiguro, T.; Sugita, Y. Incidence and predictive factors of lung cancer in patients with idiopathic pulmonary fibrosis. ERJ Open Res. 2018, 4, 00111-2016. [Google Scholar] [CrossRef]
- Le Jeune, I.; Gribbin, J.; West, J.; Smith, C.; Cullinan, P.; Hubbard, R. The incidence of cancer in patients with idiopathic pulmonary fibrosis and sarcoidosis in the UK. Respir. Med. 2007, 101, 2534–2540. [Google Scholar] [CrossRef] [Green Version]
- Ozawa, Y.; Suda, T.; Naito, T.; Enomoto, N.; Hashimoto, D.; Fujisawa, T.; Nakamura, Y.; Inui, N.; Nakamura, H.; Chida, K. Cumulative incidence of and predictive factors for lung cancer in IPF. Respirology 2009, 14, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Collard, H.R.; Ward, A.J.; Lanes, S.; Hayflinger, C.D.; Rosenberg, D.M.; Hunsche, E. Burden of illness in idiopathic pulmonary fibrosis. J. Med. Econ. 2012, 15, 829–835. [Google Scholar] [CrossRef]
- Kreuter, M.; Ehlers-Tenenbaum, S.; Schaaf, M.; Oltmanns, U.; Palmowski, K.; Hoffman, H.; Schabel, P.A.; Heußel, C.-P.; Puderbach, M.; Herth, F.J.F.; et al. Treatment and outcome of lung cancer in idiopathic interstitial pneumonias. Sarcoidosis. Vasc. Diffuse Lung. Dis. 2015, 31, 266–274. [Google Scholar] [PubMed]
- Watanabe, A.; Miyajima, M.; Mishina, T.; Nakazawa, J.; Harada, R.; Kawaharada, N.; Higami, T. Surgical treatment for primary lung cancer combined with idiopathic pulmonary fibrosis. Gen. Thorac. Cardiovasc. Surg. 2013, 61, 254–261. [Google Scholar] [CrossRef]
- Tomassetti, S.; Gurioli, C.; Ryu, J.; Decker, P.A.; Ravaglia, C.; Tantalocco, P.; Buccioli, M.; Piciucchi, S.; Sverzellati, N.; Dubini, A.; et al. The impact of lung cancer on survival of idiopathic pulmonary fibrosis. Chest 2015, 147, 157–164. [Google Scholar] [CrossRef]
- Lee, T.; Park, J.Y.; Lee, H.Y.; Cho, Y.-J.; Yoon, H.I.; Lee, J.H.; Jheon, S.; Lee, C.-T.; Park, J.S. Lung cancer in patients with idiopathic pulmonary fibrosis: Clinical characteristics and impact on survival. Respir. Med. 2014, 108, 1549–1555. [Google Scholar] [CrossRef] [Green Version]
- Martini, K.; Baessler, B.; Bogowicz, M.; Blüthgen, C.; Mannil, M.; Tanadini-Lang, S.; Schniering, J.; Maurer, B.; Frauenfelder, T. Applicability of radiomics in interstitial lung disease associated with systemic sclerosis: Proof of concept. Eur. Radiol. 2021, 31, 1987–1998. [Google Scholar] [CrossRef] [PubMed]
- Mannil, M.; von Spiczak, J.; Manka, R.; Alkadhi, H. Texture Analysis and Machine Learning for Detecting Myocardial Infarction in Noncontrast Low-Dose Computed Tomography: Unveiling the Invisible. Invest. Radiol. 2018, 53, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Yasaka, K.; Akai, H.; Nojima, M.; Shinozaki-Ushiku, A.; Fukayama, M.; Nakajima, J.; Ohtomo, K.; Kiryu, S. Quantitative computed tomography texture analysis for estimating histological subtypes of thymic epithelial tumors. Eur. J. Radiol. 2017, 92, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Wibmer, A.; Hricak, H.; Gondo, T.; Matsumoto, K.; Veeraraghavan, H.; Fehr, D.; Zheng, J.; Goldman, D.; Moskowitz, C.; Fine, S.W.; et al. Haralick texture analysis of prostate MRI: Utility for differentiating non-cancerous prostate from prostate cancer and differentiating prostate cancers with different Gleason scores. Eur. Radiol. 2015, 25, 2840–2850. [Google Scholar] [CrossRef] [PubMed]
- Diehn, M.; Nardini, C.; Wang, D.S.; McGovern, S.; Jayaraman, M.; Liang, Y.; Aldape, K.; Cha, S.; Kuo, M.D. Identification of noninvasive imaging surrogates for brain tumor gene-expression modules. Proc. Natl. Acad. Sci. USA 2008, 105, 5213–5218. [Google Scholar] [CrossRef] [Green Version]
- Stefano, A.; Gioè, M.; Russo, G.; Palmucci, S.; Torrisi, S.E.; Bignardi, S.; Basile, A.; Comelli, A.; Benfante, V.; Sambataro, G.; et al. Performance of Radiomics Features in the Quantification of Idiopathic Pulmonary Fibrosis from HRCT. Diagnostics 2020, 10, 306. [Google Scholar] [CrossRef]
- Fraser, E.; St Noble, V.; Hoyles, R.K.; Benamore, R.; Ho, L.P. Readily accessible CT scoring method to quantify fibrosis in IPF. BMJ Open Respir. Res. 2020, 7, e000584. [Google Scholar] [CrossRef]
- Goh, N.S.; Desai, S.R.; Veeraraghavan, S.; Hansell, D.M.; Copley, S.J.; Maher, T.M.; Corte, T.J.; Sander, C.R.; Ratoff, C.R.; Devaraj, A.; et al. Interstitial lung disease in systemic sclerosis: A simple staging system. Am. J. Respir. Crit. Care Med. 2008, 177, 1248–1254. [Google Scholar] [CrossRef]
- Koyama, H.; Ohno, Y.; Yamazaki, Y.; Nogami, M.; Kusaka, A.; Murase, K.; Sugimura, K. Quantitatively assessed CT imaging measures of pulmonary interstitial pneumonia: Effects of reconstruction algorithms on histogram parameters. Eur. J. Radiol. 2010, 74, 142–146. [Google Scholar] [CrossRef]
- Orlandi, I.; Camiciottoli, G.; Diciotti, S.; Bartolucci, M.; Cavigli, E.; Nacci, F.; Matucci-Cerinic, M.; Villari, N.; Mascalchi, M. Thin-section and low-dose volumetric computed tomographic densitometry of the lung in systemic sclerosis. J. Comput. Assist. Tomogr. 2006, 30, 823–827. [Google Scholar] [CrossRef]
- Best, A.C.; Lynch, A.M.; Bozic, C.M.; Miller, D.; Grunwald, G.K.; Lynch, D.A. Quantitative CT indexes in idiopathic pulmonary fibrosis: Relationship with physiologic impairment. Radiology 2003, 228, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Scharm, S.C.; Vogel-Claussen, J.; Schaefer-Prokop, C.; Dettmer, S.; Knudsen, L.; Jonigk, D.; Fuge, J.; Apel, R.-M.; Welte, T.; Wacker, F.; et al. Quantification of dual-energy CT-derived functional parameters as potential imaging markers for progression of idiopathic pulmonary fibrosis. Eur. Radiol. 2021, 31, 6640–6651. [Google Scholar] [CrossRef]
- Iwasawa, T.; Okudela, K.; Takemura, T.; Fukuda, T.; Matsushita, S.; Baba, T.; Ogura, T.; Tajiri, M.; Yoshizawa, A. Computer-aided Quantification of Pulmonary Fibrosis in Patients with Lung Cancer: Relationship to Disease-free Survival. Radiology 2019, 292, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Chae, H.D.; Park, C.M.; Park, S.J.; Lee, S.M.; Kim, K.G.; Goo, J.M. Computerized texture analysis of persistent part-solid ground-glass nodules: Differentiation of preinvasive lesions from invasive pulmonary adenocarcinomas. Radiology 2014, 273, 285–293. [Google Scholar] [CrossRef]
- Kamiya, A.; Murayama, S.; Kamiya, H.; Yamashiro, T.; Oshiro, Y.; Tanaka, N. Kurtosis and skewness assessments of solid lung nodule density histograms: Differentiating malignant from benign nodules on CT. Jpn. J. Radiol. 2014, 32, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Awai, K.; Mori, T.; Kawanaka, K.; Yamashita, Y.; Nomori, H. Differential diagnosis of ground-glass opacity nodules: CT number analysis by three-dimensional computerized quantification. Chest 2007, 132, 984–990. [Google Scholar] [CrossRef]
- Tsubakimoto, M.; Yamashiro, T.; Tamashiro, Y.; Murayama, S. Quantitative CT density histogram values and standardized uptake values of FDG-PET/CT with respiratory gating can distinguish solid adenocarcinomas from squamous cell carcinomas of the lung. Eur. J. Radiol. 2018, 100, 108–115. [Google Scholar] [CrossRef]
- Antoniou, K.M.; Tomassetti, S.; Tsitoura, E.; Vancheri, C. Idiopathic pulmonary fibrosis and lung cancer: A clinical and pathogenesis update. Curr. Opin. Pulm. Med. 2015, 21, 626–633. [Google Scholar] [CrossRef]
- Drakopanagiotakis, F.; Xifteri, A.; Polychronopoulos, V.; Bouros, D. Apoptosis in lung injury and fibrosis. Eur. Respir. J. 2008, 32, 1631–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-Cancer Group (n = 90) | Cancer Group (n = 26) | p Value | ||
|---|---|---|---|---|---|
| Age | 73.9 ± | 8.6 | 71.0 ± | 10.4 | 0.153 |
| Gender (M) | 56 | (62.2%) | 24 | (92.3%) | <0.001 * |
| Smoke | 26 | (28.9%) | 17 | (65.4%) | 0.001 * |
| 1 FVC (%) | 87.0 ± | 24.6 | 94.8 ± | 22.1 | 0.239 |
| 2 FEV1 (%) | 90.2 ± | 26.6 | 92.6 ± | 21.5 | 0.732 |
| 3 DLCO (%) | 64.4 ± | 22.6 | 56.6 ± | 28.5 | 0.373 |
| 4 TLC (%) | 78.7 ± | 19.1 | 81.1 ± | 12.1 | 0.628 |
| Fibrotic score | 21.7 ± | 11.5 | 16.3 ± | 11.5 | 0.038 * |
| Emphysema (%) | 6.7 ± | 6.1 | 9.00 ± | 7.00 | 0.101 |
| Lung volume (mL) | 3080.7 ± | 943.5 | 3952.6 ± | 930.4 | <0.001 * |
| Metric | Features | Non-Cancer Group | Cancer Group | p Value |
|---|---|---|---|---|
| First order | Energy | 2.11 × 1012 | 2.73 × 1012 | <0.001 * |
| Entropy | 8.83 | 8.66 | 0.283 | |
| Kurtosis | 18.81 | 22.99 | 0.029 * | |
| Skewness | 4.54 | 5.11 | 0.054 | |
| Mean | −392.59 | −415.87 | 0.574 | |
| Standard deviation | 401.30 | 377.47 | 0.092 | |
| Median | −517.07 | −521.57 | 0.905 | |
| 10th percentile | −716.30 | −717.56 | 0.97 | |
| 90th percentile | 105.02 | −2.07 | 0.135 | |
| Autocorrelation | 650.74 | 614.40 | 0.507 | |
| Second order (1 GLCM) | Cluster Prominence | 754,964.35 | 728,921.73 | 0.696 |
| Cluster shade | 12,719.60 | 11,644.99 | 0.268 | |
| Contrast | 84.35 | 78.68 | 0.381 | |
| Correlation | 1.27 | 1.22 | 0.115 | |
| Difference Entropy | 7.12 | 7.05 | 0.556 | |
| Difference Variance | 46.55 | 43.58 | 0.347 | |
| Dissimilarity | 8.43 | 8.18 | 0.502 | |
| Homogeneity | 0.70 | 0.70 | 0.992 | |
| 2 IMC1 | −0.15 | −0.13 | 0.054 | |
| 2 IMC2 | 1.29 | 1.22 | 0.064 | |
| Inverse difference | 0.70 | 0.70 | 0.992 | |
| Maximum probability | 0.04 | 0.04 | 0.667 | |
| Sum average | 66.76 | 65.56 | 0.665 | |
| Sum entropy | 10.32 | 10.11 | 0.221 | |
| Sum of squares | 119.17 | 103.23 | 0.086 | |
| Sum variance | 392.33 | 334.26 | 0.073 |
| Characteristic | Univariate Regression Analysis | Multivariate Regression Analysis | ||||
|---|---|---|---|---|---|---|
| OR | (95% CI) | p Value | OR | (95% CI) | p Value | |
| Smoke | 4.28 | (1.51–12.12) | 0.006 | 3.22 | (1.05–9.87) | 0.041 * |
| Energy | 1.52 | (1.14–2.05) | 0.001 | 1.02 | (0.93–1.11) | 0.012 * |
| Kurtosis | 1.08 | (1.01–1.15) | 0.034 | 1.03 | (0.95–1.11) | 0.508 |
| Characteristics | Cut-Off | AUC | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|---|---|
| Gender (M) | 0.66 [0.55–0.75] | 90.0 | 41.7 | 52.2 | |
| Smoke | 0.66 [0.56–0.76] | 55.0 | 77.8 | 72.8 | |
| Emphysema (%) | 7.6 | 0.67 [0.56–0.76] | 60.0 | 75.0 | 70.7 |
| Energy | 2.2 × 1012 | 0.73 [0.63–0.82] | 85.0 | 59.7 | 69.6 |
| Kurtosis | 18.3 | 0.66 [0.55–0.75] | 80.0 | 54.2 | 58.7 |
| Characteristics | Sensitivity (%) | Specificity (%) | Accuracy (%) |
|---|---|---|---|
| Gender (M) | 100 | 27.8 | 45.8 |
| Smoke | 100 | 44.4 | 58.3 |
| Emphysema (%) | 33.3 | 61.1 | 54.2 |
| Energy | 83.3 | 38.9 | 50.0 |
| Kurtosis | 83.3 | 44.4 | 54.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, C.-H.; Liu, Y.-C.; Wan, Y.-L.; Yun, C.-H.; Wu, W.-J.; López-González, R.; Huang, W.-M. Quantification of Cancer-Developing Idiopathic Pulmonary Fibrosis Using Whole-Lung Texture Analysis of HRCT Images. Cancers 2021, 13, 5600. https://doi.org/10.3390/cancers13225600
Liang C-H, Liu Y-C, Wan Y-L, Yun C-H, Wu W-J, López-González R, Huang W-M. Quantification of Cancer-Developing Idiopathic Pulmonary Fibrosis Using Whole-Lung Texture Analysis of HRCT Images. Cancers. 2021; 13(22):5600. https://doi.org/10.3390/cancers13225600
Chicago/Turabian StyleLiang, Chia-Hao, Yung-Chi Liu, Yung-Liang Wan, Chun-Ho Yun, Wen-Jui Wu, Rafael López-González, and Wei-Ming Huang. 2021. "Quantification of Cancer-Developing Idiopathic Pulmonary Fibrosis Using Whole-Lung Texture Analysis of HRCT Images" Cancers 13, no. 22: 5600. https://doi.org/10.3390/cancers13225600
APA StyleLiang, C.-H., Liu, Y.-C., Wan, Y.-L., Yun, C.-H., Wu, W.-J., López-González, R., & Huang, W.-M. (2021). Quantification of Cancer-Developing Idiopathic Pulmonary Fibrosis Using Whole-Lung Texture Analysis of HRCT Images. Cancers, 13(22), 5600. https://doi.org/10.3390/cancers13225600