
Multimodal Web-Based Intervention for Cancer-Related Cognitive Impairment in Breast Cancer Patients: Cog-Stim Feasibility Study Protocol

 , , ,
, , ,
Abstract
:Simple Summary
Abstract

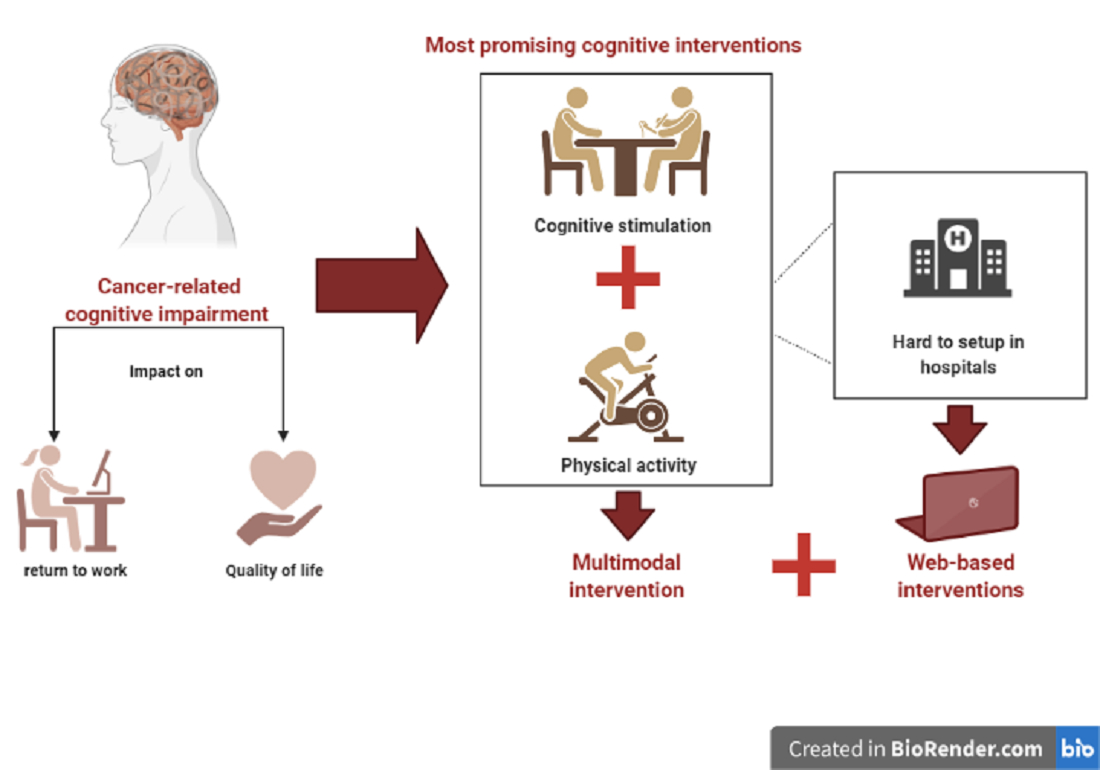
1. Introduction
2. Materials and Methods
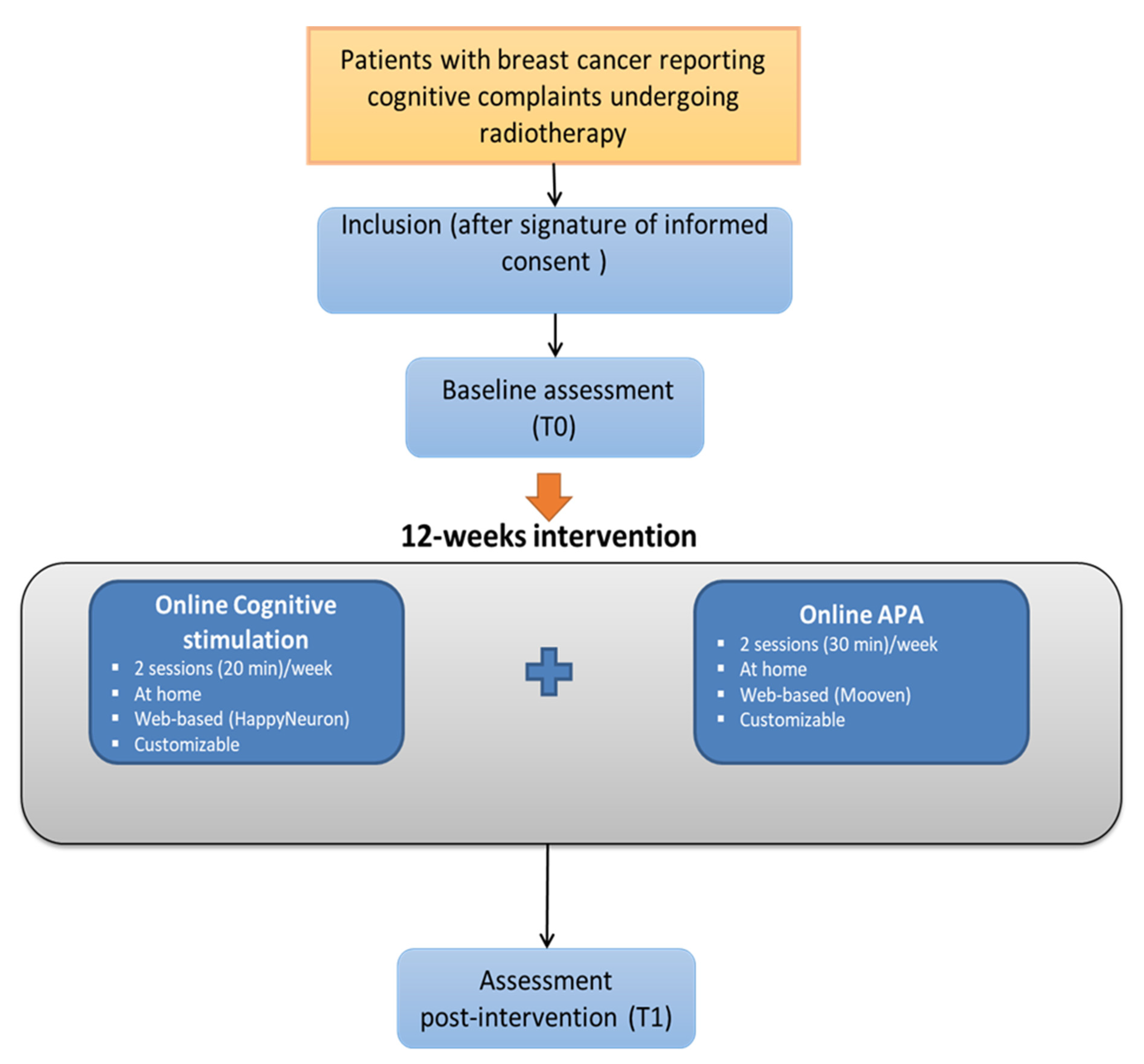
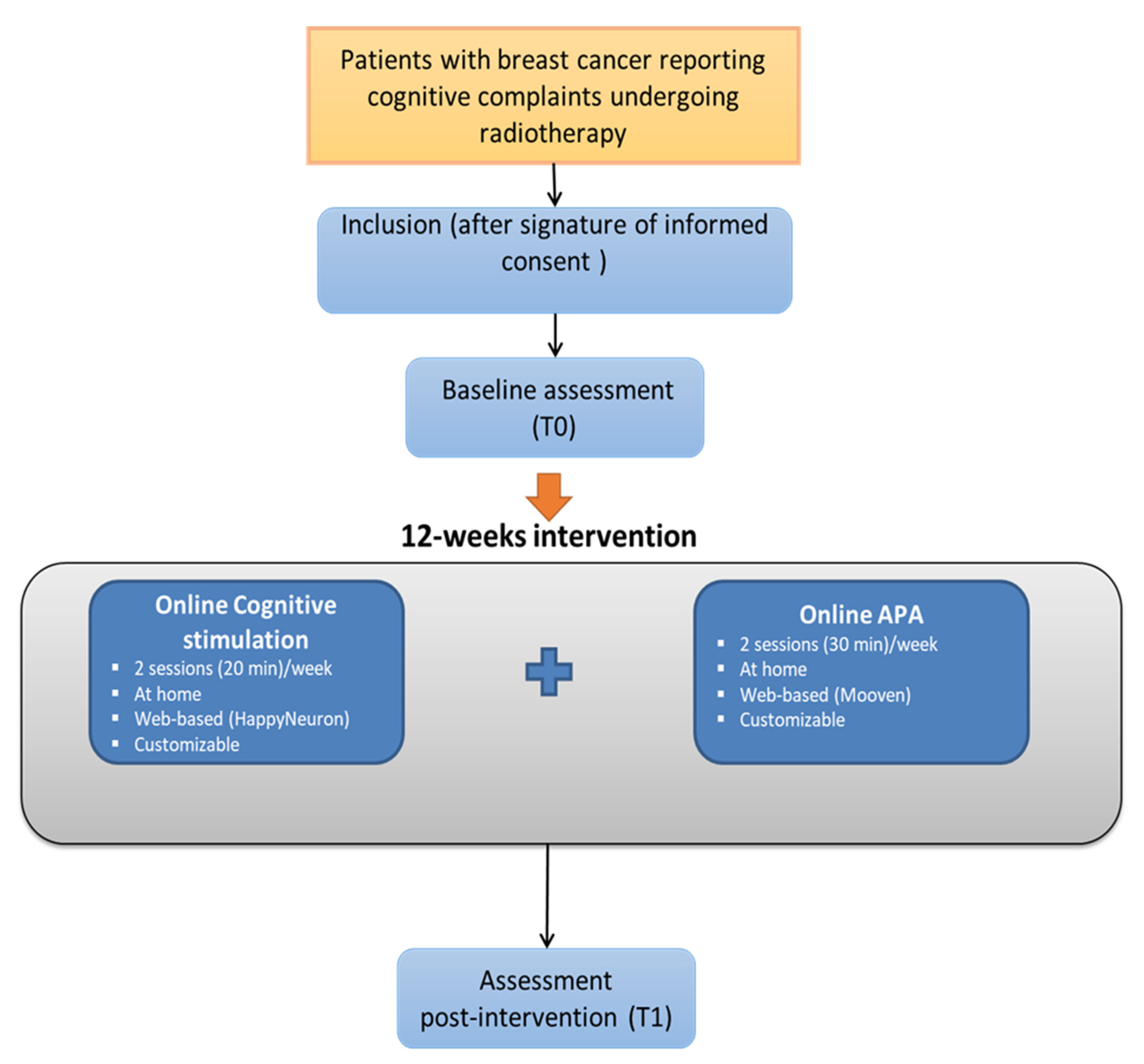
2.1. Study design
2.2. Objectives
2.2.1. Primary Outcome
2.2.2. Secondary Outcomes
- (1)
- To evaluate the proportion of acceptance (attrition) of the study among breast cancer patients starting adjuvant radiotherapy, and according to previous adjuvant chemotherapy. The number of patients contacted, program rejection and acceptance rates, as well as reasons for rejection will be recorded, along with the presence or absence of prior chemotherapy treatment.
- (2)
- To evaluate patients’ satisfaction regarding the proposed intervention program (frequency, duration, content of the sessions, whether the moment to initiate cognitive rehabilitation throughout the oncologic management is appropriate, obstacles to access and use the different software, and the perceived usefulness of the program). This information will be collected using a 13-item questionnaire, developed in our institution for this study.
- (3)
- To identify barriers to accessing the program (impossibility or inability to use the computer, no access to internet connections etc.) or to achieve its completion (motives of non-eligibility, non-participation, and drop-out, etc.). This information will be collected and stored by the neuropsychologist throughout the research program;
- (4)
- To evaluate exercise intensity and training burden and its possible impact on adherence to the protocol. This information will be collected by the APA specialist and stored on the Mooven App.
2.3. Participants: Recruitment and Procedure
2.4. Inclusion Criteria
2.5. Assessments
- Verbal Memory (VBM), which investigates word recognition and words memorization ability (immediate and delayed recall);
- Visual Memory (VIM), which investigates recognition and memorization of geometric shapes (immediate and delayed recall);
- Finger Tapping (FTT), for motor speed and fine motor control assessment;
- Symbol Digit (SDC) to investigate information processing speed, complex attention, visual-perceptual speed and complex information processing speed-accuracy;
- Stroop test (ST) for simple and complex reaction time, inhibition/disinhibition abilities, processing speed and frontal or executive skills assessment;
- Shifting Attention (SAT) to assess executive functions, decision making and reaction time;
- Continuous Performance (CPT) for sustained attention, impulsivity and choice reaction time.
2.6. The Multimodal Web-Based Intervention
2.6.1. Cognitive Stimulation—HappyNeuron Platform®
2.6.2. Adapted Physical Activity Training—Mooven® Platform
2.7. Statistical Analysis
- social barriers (patients living in remote areas with a poor internet connection, patients with limited access to computer material or low skills in informatics, etc., resulting in selection bias of more affluent women and social inequalities in the access to the program),
- technological barriers (patients with limited skills in informatics, inappropriate material),
- or availability barriers (already in an APA or cognitive training program, program too demanding/exhausting, not available enough to complete it, not the good time during cancer therapeutic management to propose cognitive management, etc.).
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Janelsins, M.C.; Heckler, C.E.; Peppone, L.J.; Kamen, C.; Mustian, K.M.; Mohile, S.G.; Magnuson, A.; Kleckner, I.R.; Guido, J.J.; Young, K.L. Cognitive Complaints in Survivors of Breast Cancer after Chemotherapy Compared with Age-Matched Controls: An Analysis from a Nationwide, Multicenter, Prospective Longitudinal Study. J. Clin. Oncol. 2017, 35, 506. [Google Scholar] [CrossRef]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; De Ruiter, M.; Castel, H. Cancer-Related Cognitive Impairment: An Update on State of the Art, Detection, and Management Strategies in Cancer Survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bower, J.E. Behavioral Symptoms in Breast Cancer Patients and Survivors: Fatigue, Insomnia, Depression, and Cognitive Disturbance. J. Clin. Oncol. 2008, 26, 768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrington, C.B.; Hansen, J.A.; Moskowitz, M.; Todd, B.L.; Feuerstein, M. It’s Not over When It’s over: Long-Term Symptoms in Cancer Survivors—A Systematic Review. Int. J. Psychiatry Med. 2010, 40, 163–181. [Google Scholar] [CrossRef] [PubMed]
- Stein, K.D.; Syrjala, K.L.; Andrykowski, M.A. Physical and Psychological Long-term and Late Effects of Cancer. Cancer 2008, 112, 2577–2592. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.M.; Jim, H.S.; Small, B.J.; Laronga, C.; Andrykowski, M.A.; Jacobsen, P.B. Cognitive Functioning after Cancer Treatment: A 3-Year Longitudinal Comparison of Breast Cancer Survivors Treated with Chemotherapy or Radiation and Noncancer Controls. Cancer 2012, 118, 1925–1932. [Google Scholar] [CrossRef] [Green Version]
- Shibayama, O.; Yoshiuchi, K.; Inagaki, M.; Matsuoka, Y.; Yoshikawa, E.; Sugawara, Y.; Akechi, T.; Wada, N.; Imoto, S.; Murakami, K.; et al. Association between Adjuvant Regional Radiotherapy and Cognitive Function in Breast Cancer Patients Treated with Conservation Therapy. Cancer Med. 2014, 3, 702–709. [Google Scholar] [CrossRef]
- Ahles, T.A.; Root, J.C.; Ryan, E.L. Cancer- and Cancer Treatment–Associated Cognitive Change: An Update on the State of the Science. J. Clin. Oncol. 2012, 30, 3675–3686. [Google Scholar] [CrossRef]
- Lange, M.; Hardy-Léger, I.; Licaj, I.; Pistilli, B.; Rigal, O.; Le Fel, J.; Lévy, C.; Capel, A.; Coutant, C.; Meyer, J.; et al. Cognitive Impairment in Patients with Breast Cancer before Surgery: Results from a CANTO Cohort Subgroup. Cancer Epidemiol. Biomarkers Prev. 2020, 29, 1759–1766. [Google Scholar] [CrossRef]
- Joly, F.; Giffard, B.; Rigal, O.; De Ruiter, M.B.; Small, B.J.; Dubois, M.; LeFel, J.; Schagen, S.B.; Ahles, T.A.; Wefel, J.S.; et al. Impact of Cancer and Its Treatments on Cognitive Function: Advances in Research From the Paris International Cognition and Cancer Task Force Symposium and Update Since 2012. J. Pain Symptom Manag. 2015, 50, 830–841. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.S. Cancer- and Chemotherapy-Related Cognitive Changes: The Patient Experience. Semin. Oncol. Nurs. 2013, 29, 300–307. [Google Scholar] [CrossRef]
- Koppelmans, V.; Breteler, M.; Boogerd, W.; Seynaeve, C.; Gundy, C.; Schagen, S. Neuropsychological Performance in Survivors of Breast Cancer More than 20 Years after Adjuvant Chemotherapy. J. Clin. Oncol. 2012, 30, 1080–1086. [Google Scholar] [CrossRef]
- Yamada, T.H.; Denburg, N.L.; Beglinger, L.J.; Schultz, S.K. Neuropsychological Outcomes of Older Breast Cancer Survivors: Cognitive Features Ten or More Years after Chemotherapy. J. Neuropsychiatry Clin. Neurosci. 2010, 22, 48–54. [Google Scholar] [CrossRef]
- Selamat, M.H.; Loh, S.Y.; Mackenzie, L.; Vardy, J. Chemobrain Experienced by Breast Cancer Survivors: A Meta-Ethnography Study Investigating Research and Care Implications. PLoS ONE 2014, 9, e108002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boykoff, N.; Moieni, M.; Subramanian, S.K. Confronting Chemobrain: An in-Depth Look at Survivors’ Reports of Impact on Work, Social Networks, and Health Care Response. J. Cancer Surviv. 2009, 3, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downie, F.P.; Mar Fan, H.G.; Houédé-Tchen, N.; Yi, Q.; Tannock, I.F. Cognitive Function, Fatigue, and Menopausal Symptoms in Breast Cancer Patients Receiving Adjuvant Chemotherapy: Evaluation with Patient Interview after Formal Assessment. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2006, 15, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Le Fel, J.; Daireaux, A.; Vandenbosshe, S.; Heutte, N.; Rigal, O.; Rovira, K.; Joly, F.; Roy, V. Impact Des Traitements En Cancérologie Sur Les Fonctions Cognitives: Le Point de Vue Des Patients, Leur Attente et Leur Souhait de Participer à Des Ateliers de Rééducation Cognitive. Bull. Cancer 2013, 100, 223–229. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; de Boer, A.; Spelten, E.; Sprangers, M.A.G.; Verbeek, J.H.A.M. The Role of Neuropsychological Functioning in Cancer Survivors’ Return to Work One Year after Diagnosis. Psychooncology 2009, 18, 589–597. [Google Scholar] [CrossRef]
- Cheung, Y.T.; Shwe, M.; Chui, W.K.; Chay, W.Y.; Ang, S.F.; Dent, R.A.; Yap, Y.S.; Lo, S.K.; Ng, R.C.H.; Chan, A. Effects of Chemotherapy and Psychosocial Distress on Perceived Cognitive Disturbances in Asian Breast Cancer Patients. Ann. Pharmacother. 2012, 46, 1645–1655. [Google Scholar] [CrossRef]
- Munir, F.; Burrows, J.; Yarker, J.; Kalawsky, K.; Bains, M. Women’s Perceptions of Chemotherapy-Induced Cognitive Side Affects on Work Ability: A Focus Group Study. J. Clin. Nurs. 2010, 19, 1362–1370. [Google Scholar] [CrossRef] [Green Version]
- Von Ah, D.; Habermann, B.; Carpenter, J.S.; Schneider, B.L. Impact of Perceived Cognitive Impairment in Breast Cancer Survivors. Eur. J. Oncol. Nurs. 2013, 17, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Lonkhuizen, P.J.C.; Klaver, K.M.; Wefel, J.S.; Sitskoorn, M.M.; Schagen, S.B.; Gehring, K. Interventions for Cognitive Problems in Adults with Brain Cancer: A Narrative Review. Eur. J. Cancer Care 2019, 28, e13088. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.J.; McCarthy, A.L.; Devenish, J.; Sullivan, K.A.; Chan, A. Systematic Review of Pharmacologic and Non-Pharmacologic Interventions to Manage Cognitive Alterations after Chemotherapy for Breast Cancer. Eur. J. Cancer 2015, 51, 437–450. [Google Scholar] [CrossRef] [Green Version]
- Olsson Möller, U.; Beck, I.; Rydén, L.; Malmström, M. A Comprehensive Approach to Rehabilitation Interventions Following Breast Cancer Treatment—A Systematic Review of Systematic Reviews. BMC Cancer 2019, 19, 472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, H.A.; Richard, N.M.; Edelstein, K. Cognitive Rehabilitation for Cancer-Related Cognitive Dysfunction: A Systematic Review. Support. Care Cancer 2019, 27, 3253–3279. [Google Scholar] [CrossRef] [PubMed]
- Vance, D.E.; Frank, J.S.; Bail, J.; Triebel, K.L.; Niccolai, L.M.; Gerstenecker, A.; Meneses, K. Interventions for Cognitive Deficits in Breast Cancer Survivors Treated with Chemotherapy. Cancer Nurs. 2017, 40, E11–E27. [Google Scholar] [CrossRef]
- Curlik, D.M.; Shors, T.J. Training Your Brain: Do Mental and Physical (MAP) Training Enhance Cognition through the Process of Neurogenesis in the Hippocampus? Neuropharmacology 2013, 64, 506–514. [Google Scholar] [CrossRef]
- Fissler, P.; Küster, O.; Schlee, W.; Kolassa, I.-T. Novelty Interventions to Enhance Broad Cognitive Abilities and Prevent Dementia. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2013; Volume 207, pp. 403–434. ISBN 978-0-444-63327-9. [Google Scholar]
- Bamidis, P.D.; Fissler, P.; Papageorgiou, S.G.; Zilidou, V.; Konstantinidis, E.I.; Billis, A.S.; Romanopoulou, E.; Karagianni, M.; Beratis, I.; Tsapanou, A.; et al. Gains in Cognition through Combined Cognitive and Physical Training: The Role of Training Dosage and Severity of Neurocognitive Disorder. Front. Aging Neurosci. 2015, 7, 152. [Google Scholar] [CrossRef] [Green Version]
- Bamidis, P.D.; Vivas, A.B.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountas, A.; Papageorgiou, S.G. A Review of Physical and Cognitive Interventions in Aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef] [PubMed]
- Hötting, K.; Röder, B. Beneficial Effects of Physical Exercise on Neuroplasticity and Cognition. Neurosci. Biobehav. Rev. 2013, 37, 2243–2257. [Google Scholar] [CrossRef]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical Activity to Improve Cognition in Older Adults: Can Physical Activity Programs Enriched with Cognitive Challenges Enhance the Effects? A Systematic Review and Meta-Analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.; Park, J.H.; Na, H.R.; Hiroyuki, S.; Kim, G.M.; Jung, M.K.; Kim, W.K.; Park, K.W. Combined Intervention of Physical Activity, Aerobic Exercise, and Cognitive Exercise Intervention to Prevent Cognitive Decline for Patients with Mild Cognitive Impairment: A Randomized Controlled Clinical Study. J. Clin. Med. 2019, 8, 940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of Combined Physical and Cognitive Training on Cognition: A Systematic Review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, L.L.F.; Barnett, F.; Yau, M.K.; Gray, M.A. Effects of Combined Cognitive and Exercise Interventions on Cognition in Older Adults with and without Cognitive Impairment: A Systematic Review. Ageing Res. Rev. 2014, 15, 61–75. [Google Scholar] [CrossRef]
- Medrano, J.; Brown, J.; Shackelford, D.; Beebe, C.; Brennecke, A. The Effects of a Twelve-Week Aerobic and Cognitive Training Intervention on Cognitive Function in Cancer Survivors. Ursidae Undergrad. Res. J. Univ. North. Colo. 2014, 4, 1. [Google Scholar]
- Peterson, B.M.; Johnson, C.; Case, K.R.; Shackelford, D.Y.; Brown, J.M.; Lalonde, T.L.; Hayward, R. Feasibility of a Combined Aerobic and Cognitive Training Intervention on Cognitive Function in Cancer Survivors: A Pilot Investigation. Pilot Feasibility Stud. 2018, 4, 50. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The More the Better? A Meta-Analysis on Effects of Combined Cognitive and Physical Intervention on Cognition in Healthy Older Adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef]
- Luxton. Artificial Intelligence in Behavioral and Mental Health Care; Academic Press: Cambridge, MA, USA, 2015; ISBN 978-0-12-800792-1. [Google Scholar]
- Barak, A.; Hen, L.; Boniel-Nissim, M.; Shapira, N. A Comprehensive Review and a Meta-Analysis of the Effectiveness of Internet-Based Psychotherapeutic Interventions. J. Technol. Hum. Serv. 2008, 26, 109–160. [Google Scholar] [CrossRef]
- Marks, I.M.; Cavanagh, K.; Gega, L. Hands-on Help: Computer-Aided Psychotherapy; Psychology Press: Oxfordshire, UK, 2007; ISBN 1-135-43045-4. [Google Scholar]
- Murray, E.; Burns, J.; Tai, S.S.; Lai, R.; Nazareth, I. Interactive Health Communication Applications for People with Chronic Disease. Cochrane Database Syst. Rev. 2004, 4. [Google Scholar] [CrossRef]
- Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. EHealth for Improving Quality of Life in Breast Cancer Patients: A Systematic Review. Cancer Treat. Rev. 2019, 74, 1–14. [Google Scholar] [CrossRef]
- Bellens, A.; Roelant, E.; Sabbe, B.; Peeters, M.; van Dam, P.A. A Video-Game Based Cognitive Training for Breast Cancer Survivors with Cognitive Impairment: A Prospective Randomized Pilot Trial. Breast 2020, 53, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Bray, V.J.; Dhillon, H.M.; Bell, M.L.; Kabourakis, M.; Fiero, M.H.; Yip, D.; Boyle, F.; Price, M.A.; Vardy, J.L. Evaluation of a Web-Based Cognitive Rehabilitation Program in Cancer Survivors Reporting Cognitive Symptoms after Chemotherapy. Am. Soc. Clin. Oncol. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conklin, H.M.; Ogg, R.J.; Ashford, J.M.; Scoggins, M.A.; Zou, P.; Clark, K.N.; Martin-Elbahesh, K.; Hardy, K.K.; Merchant, T.E.; Jeha, S. Computerized Cognitive Training for Amelioration of Cognitive Late Effects among Childhood Cancer Survivors: A Randomized Controlled Trial. J. Clin. Oncol. 2015, 33, 3894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damholdt, M.; Mehlsen, M.; O’Toole, M.; Andreasen, R.; Pedersen, A.; Zachariae, R. Web-Based Cognitive Training for Breast Cancer Survivors with Cognitive Complaints-a Randomized Controlled Trial: Web-Based Cognitive Training for Breast Cancer Survivors. Psychooncology. 2016, 25, 1293–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, M.; Hardy-Léger, I.; Rigal, O.; Licaj, I.; Dauchy, S.; Levy, C.; Noal, S.; Segura, C.; Delcambre, C.; Allouache, D.; et al. Cognitive Rehabilitation Program to Improve Cognition of Cancer Patients Treated with Chemotherapy: A 3-arm Randomized Trial. Cancer 2020, 126, 5328–5336. [Google Scholar] [CrossRef]
- Gehring, K.; Stuiver, M.M.; Visser, E.; Kloek, C.; van den Bent, M.; Hanse, M.; Tijssen, C.; Rutten, G.-J.; Taphoorn, M.J.B.; Aaronson, N.K.; et al. A Pilot Randomized Controlled Trial of Exercise to Improve Cognitive Performance in Patients with Stable Glioma: A Proof of Concept. NeuroOncology 2020, 22, 103–115. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Ariza-García, A.; Díaz-Rodríguez, L.; Del-Moral-Ávila, R.; Arroyo-Morales, M. Telehealth System: A Randomized Controlled Trial Evaluating the Impact of an Internet-Based Exercise Intervention on Quality of Life, Pain, Muscle Strength, and Fatigue in Breast Cancer Survivors: Telehealth System in Breast Cancer. Cancer 2016, 122, 3166–3174. [Google Scholar] [CrossRef]
- Barello, S.; Triberti, S.; Graffigna, G.; Libreri, C.; Serino, S.; Hibbard, J.; Riva, G. EHealth for Patient Engagement: A Systematic Review. Front. Psychol. 2016, 6, 2013. [Google Scholar] [CrossRef] [Green Version]
- Haberlin, C.; O’Dwyer, T.; Mockler, D.; Moran, J.; O’Donnell, D.M.; Broderick, J. The Use of EHealth to Promote Physical Activity in Cancer Survivors: A Systematic Review. Support. Care Cancer 2018, 26, 3323–3336. [Google Scholar] [CrossRef]
- Lange, M.; Heutte, N.; Morel, N.; Eustache, F.; Joly, F.; Giffard, B. Cognitive Complaints in Cancer: The French Version of the Functional Assessment of Cancer Therapy–Cognitive Function (FACT-Cog), Normative Data from a Healthy Population. Neuropsychol. Rehabil. 2016, 26, 392–409. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Roussel, M.; Godefroy, O. La Batterie GRECOGVASC: Evaluation et Diagnostic Des Troubles Neurocognitifs Vasculaires Avec Ou sans Contexte d’accident Vasculaire Cérébral; De Boeck Superieur: Bruxelles, Belgium, 2016; ISBN 2-35327-358-0. [Google Scholar]
- Gualtieri, C.; Johnson, L. Reliability and Validity of a Computerized Neurocognitive Test Battery, CNS Vital Signs. Arch. Clin. Neuropsychol. 2006, 21, 623–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joly, F.; Lange, M.; Rigal, O.; Correia, H.; Giffard, B.; Beaumont, J.L.; Clisant, S.; Wagner, L. French Version of the Functional Assessment of Cancer Therapy–Cognitive Function (FACT-Cog) Version 3. Support. Care Cancer 2012, 20, 3297–3305. [Google Scholar] [CrossRef] [PubMed]
- Razavi, D.; Delvaux, N.; Farvacques, C.; Robaye, E. Validation de La Version Française Du HADS Dans Une Population de Patients Cancéreux Hospitalisés. Rev. Psychol. Appliquée 1989, 39, 295–307. [Google Scholar]
- Yellen, S.B.; Cella, D.F.; Webster, K.; Blendowski, C.; Kaplan, E. Measuring Fatigue and Other Anemia-Related Symptoms with the Functional Assessment of Cancer Therapy (FACT) Measurement System. J. Pain Symptom Manag. 1997, 13, 63–74. [Google Scholar] [CrossRef]
- Morin, C.M. Insomnia: Psychological Assessment and Management; Guilford Press: New York, NY, USA, 1993; ISBN 0-89862-210-7. [Google Scholar]
- Ancellin, R.; Gaillot-de Saintignon, J. Bénéfices de l’activité Physique Pendant et Après Cancer: Des Connaissances Scientifiques Aux Repères Pratiques. Oncologie 2017, 19, 95–107. [Google Scholar] [CrossRef]
- Mustian, K.M.; Sprod, L.K.; Janelsins, M.; Peppone, L.J.; Mohile, S. Physical Exercise, Activity and Kinesiology (PEAK) Laboratory, James P Wilmot Cancer Center, University of Rochester School of Medicine and Dentistry, Rochester, New York, US Exercise Recommendations for Cancer-Related Fatigue, Cognitive Impairment, Sleep Problems, Depression, Pain, Anxiety, and Physical Dysfunction—A Review. Oncol. Hematol. Rev. US 2012, 8, 81. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A. American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef]
- Borg, G.A.V. Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Licaj, I.; Clarisse, B.; Humbert, X.; Grellard, J.; Tron, L.; Joly, F. Cognitive Complaints in Cancer Survivors and Expectations for Support: Results from a Web–Based Survey. Cancer Med. 2019, 8, 2654–2663. [Google Scholar] [CrossRef] [Green Version]
- Buchanan, N.D.; Dasari, S.; Rodriguez, J.L.; Smith, J.L.; Hodgson, M.E.; Weinberg, C.R.; Sandler, D.P. Post-Treatment Neurocognition and Psychosocial Care among Breast Cancer Survivors. Am. J. Prev. Med. 2015, 49, S498–S508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffiths, F.; Lindenmeyer, A.; Powell, J.; Lowe, P.; Thorogood, M. Why Are Health Care Interventions Delivered over the Internet? A Systematic Review of the Published Literature. J. Med. Internet Res. 2006, 8, e10. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Data Collection | Before Inclusion | Baseline Assessment (T0) | Assessment Post-Intervention (T1) |
|---|---|---|---|
| Signature of Informed Consent |  | ||
| Clinical Examination Including medical history ECOG and vital signs | | ||
| Cognitive Assessment AND Quality of Life Questionnaires | |||
| FACT-COG | | | |
| MoCA | | ||
| CNS Vital signs battery | | | |
| HADS, FACIT-F, ISI | | | |
| Patient’s Satisfaction | |
| Cognitive Domains Trained | Exercises |
|---|---|
| Memory (Verbal and Visual) | Words, Where are you? Elephant Memory Shapes and Colours Heraldry Displaced Characters Displaced Images N-Back Around the World in 80 trips I Remember You! Restaurant An American in Paris Find Your Way! Chunking Objects, Where are You? |
| Executive functions | Towers of Hanoi |
| Basketball in New-York | |
| Hurry for Change! | |
| Attention | Pay Attention! |
| Private Eye! | |
| Sound Check! | |
| Ancient Writing | |
| Information processing speed | Two-Timing |
| Under Pressure | |
| Gulf Stream | |
| Catch the Ladybug! | |
| Language | Split words |
| Embroidery | |
| Secret files | |
| Speak Your Mind! | |
| Decipher | |
| Writing in the Stars | |
| This Story is Full of Blanks! | |
| Which One is Alike? | |
| Logic | The Right Count |
| Countdown | |
| Ready, Steady, Count! | |
| visuospatial abilities | Sleight of Hands |
| Entangled Figures | |
| Point of View | |
| Turn Around and Around |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Binarelli, G.; Lange, M.; Dos Santos, M.; Grellard, J.-M.; Lelaidier, A.; Tron, L.; Lefevre Arbogast, S.; Clarisse, B.; Joly, F. Multimodal Web-Based Intervention for Cancer-Related Cognitive Impairment in Breast Cancer Patients: Cog-Stim Feasibility Study Protocol. Cancers 2021, 13, 4868. https://doi.org/10.3390/cancers13194868
Binarelli G, Lange M, Dos Santos M, Grellard J-M, Lelaidier A, Tron L, Lefevre Arbogast S, Clarisse B, Joly F. Multimodal Web-Based Intervention for Cancer-Related Cognitive Impairment in Breast Cancer Patients: Cog-Stim Feasibility Study Protocol. Cancers. 2021; 13(19):4868. https://doi.org/10.3390/cancers13194868
Chicago/Turabian StyleBinarelli, Giulia, Marie Lange, Mélanie Dos Santos, Jean-Michel Grellard, Anaïs Lelaidier, Laure Tron, Sophie Lefevre Arbogast, Benedicte Clarisse, and Florence Joly. 2021. "Multimodal Web-Based Intervention for Cancer-Related Cognitive Impairment in Breast Cancer Patients: Cog-Stim Feasibility Study Protocol" Cancers 13, no. 19: 4868. https://doi.org/10.3390/cancers13194868
APA StyleBinarelli, G., Lange, M., Dos Santos, M., Grellard, J.-M., Lelaidier, A., Tron, L., Lefevre Arbogast, S., Clarisse, B., & Joly, F. (2021). Multimodal Web-Based Intervention for Cancer-Related Cognitive Impairment in Breast Cancer Patients: Cog-Stim Feasibility Study Protocol. Cancers, 13(19), 4868. https://doi.org/10.3390/cancers13194868