
A Warp-Knitted Light-Emitting Fabric-Based Device for In Vitro Photodynamic Therapy: Description, Characterization, and Application on Human Cancer Cell Lines

 , , ,
, , , 

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Discussion of Illumination Parameters
2.1.1. Low-Irradiance Relevance for In Vitro 5-ALA PDT
2.1.2. Temperature-Related Issues of In Vitro 5-ALA PDT Using Low Irradiance
Preventing Cells from Reaching Room Temperature
Temperature Dependence of the Effects of PDT
2.2. Device Description
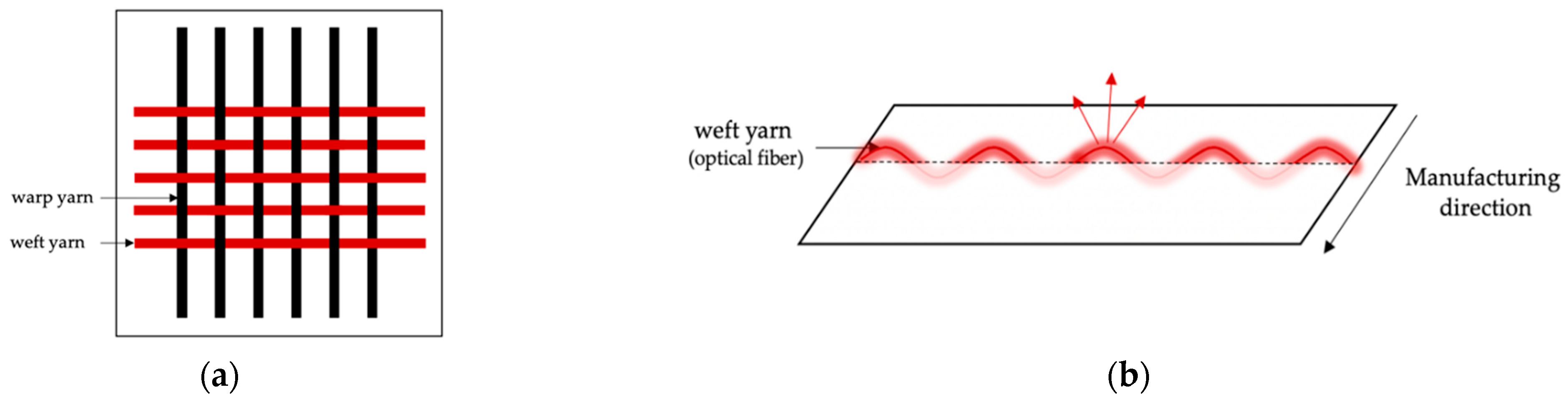
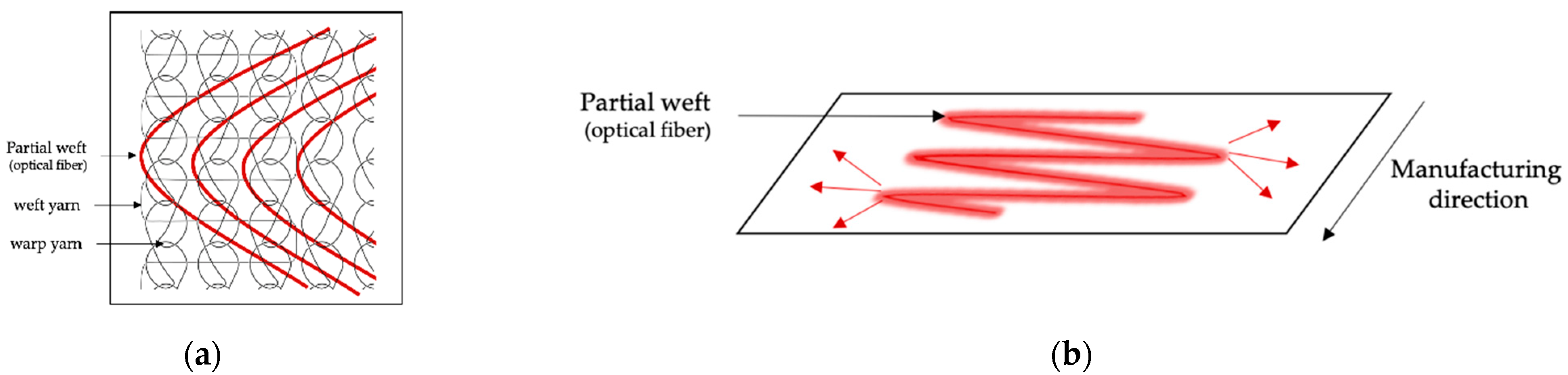
2.2.1. Light-Emitting Fabric-Based Technologies
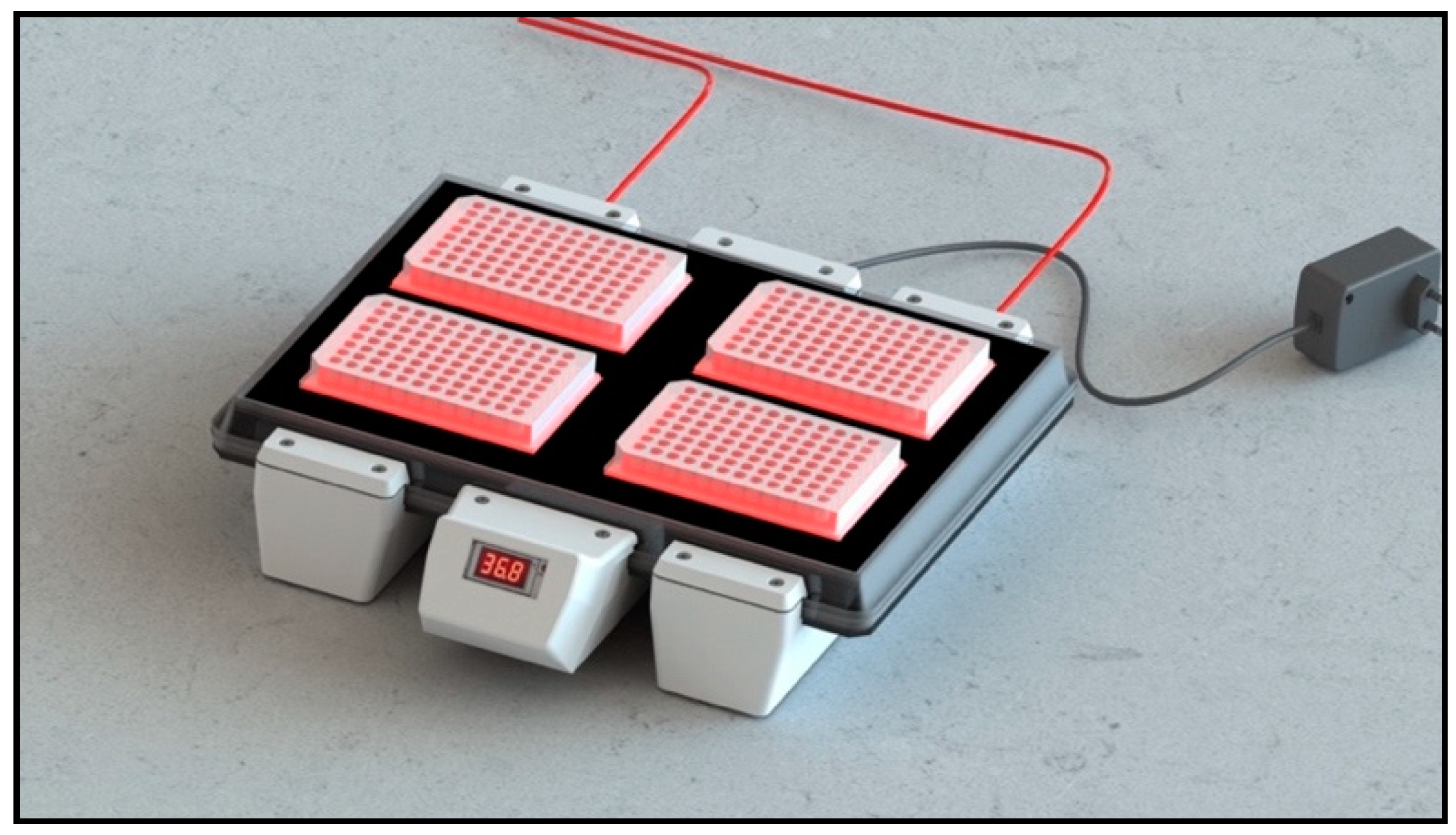
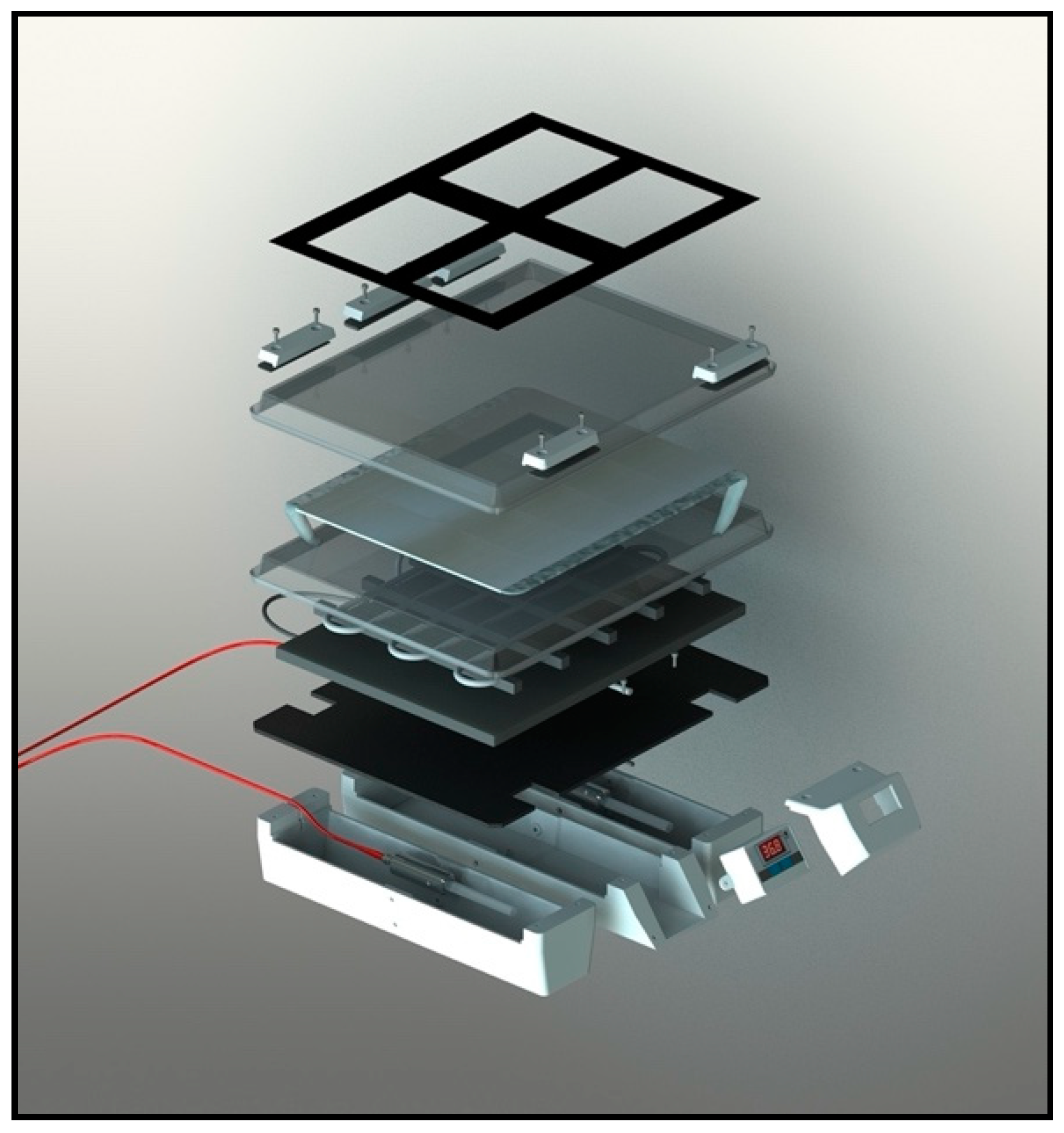
2.2.2. Structure of CELL-LEF
2.2.3. Light Supply of CELL-LEF
2.3. Optical Characterization of Device
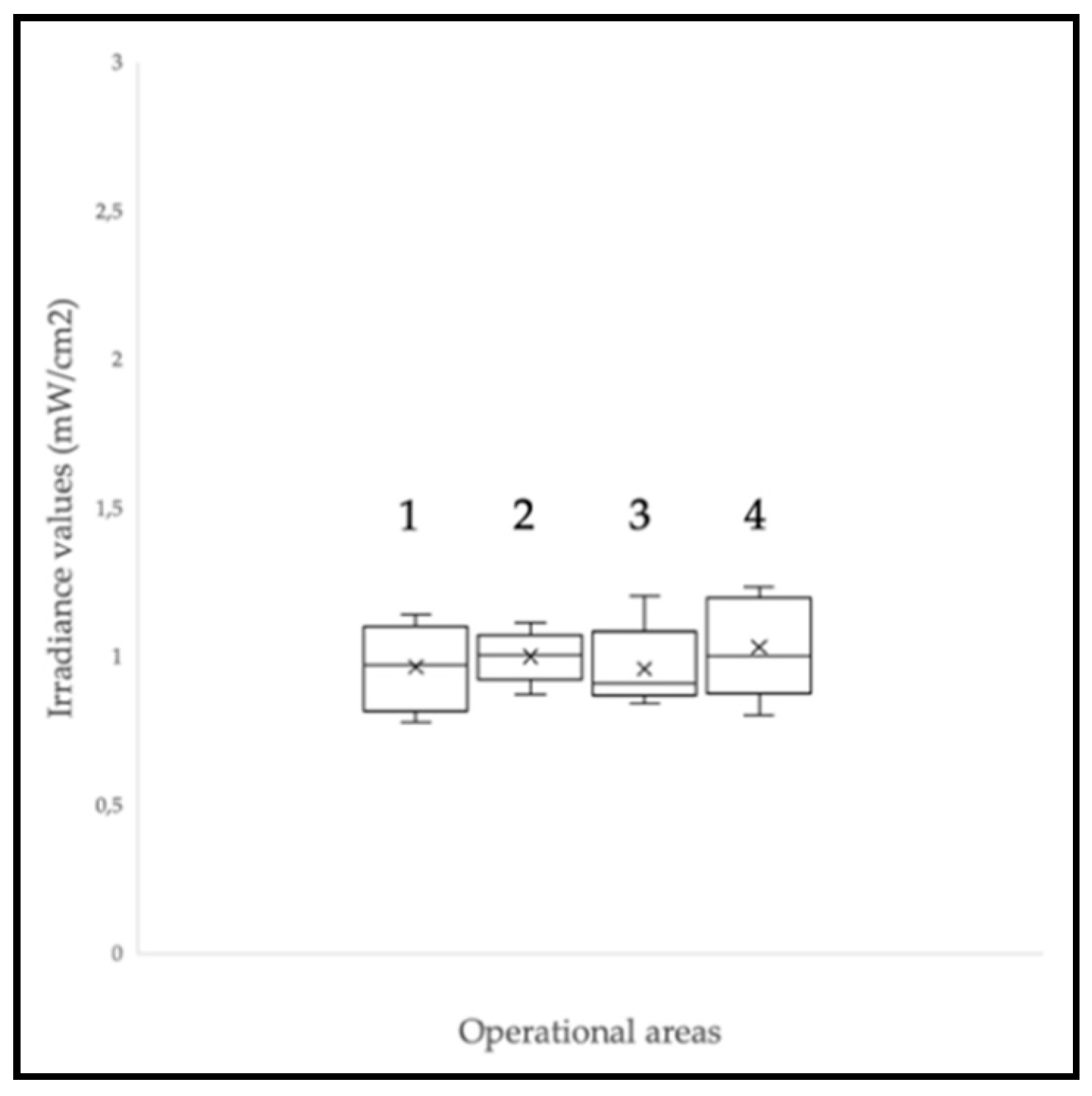
2.3.1. Irradiance Level at the CELL-LEF Surface
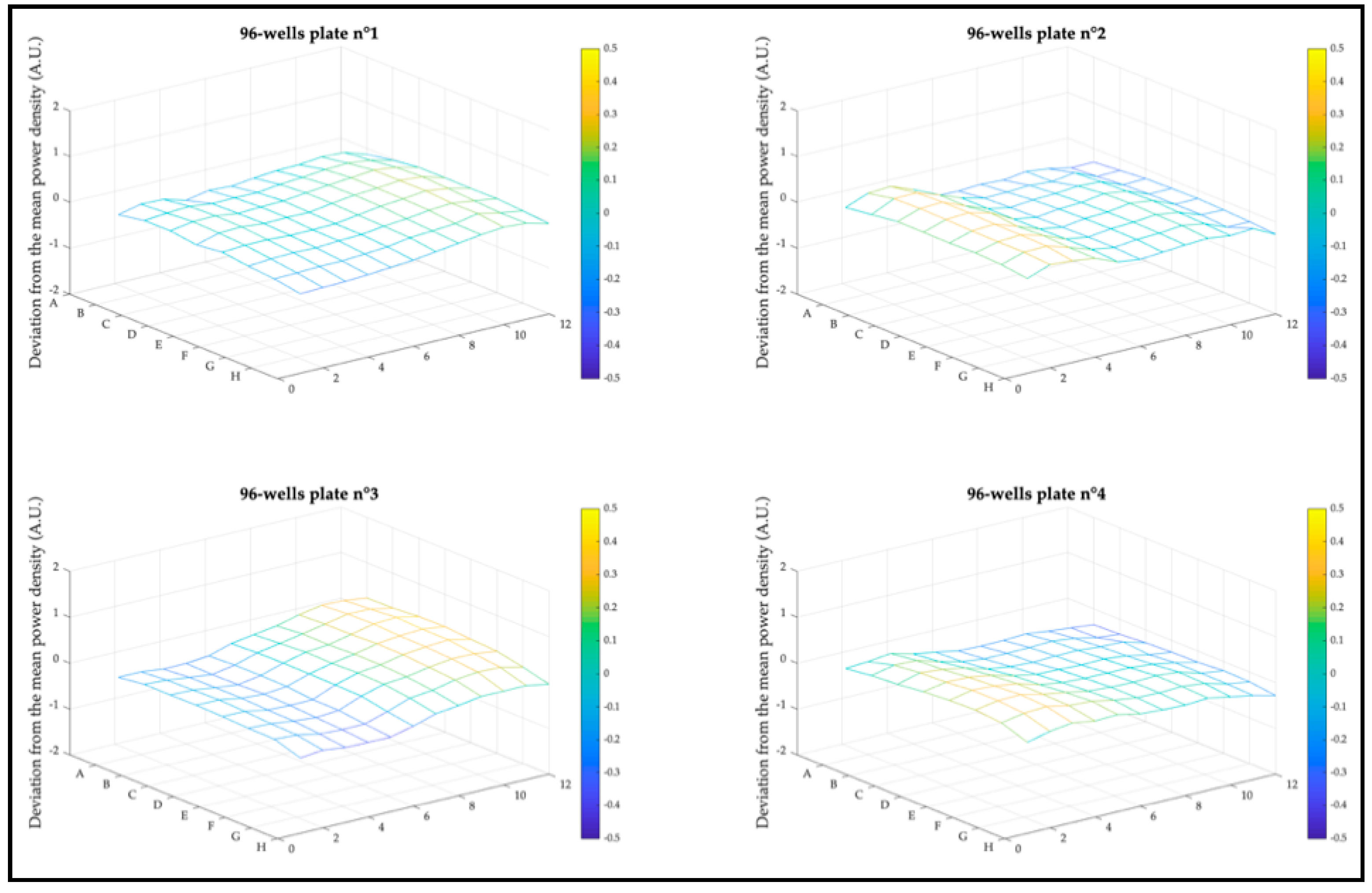
2.3.2. Irradiance Distribution in 96-Well Plates
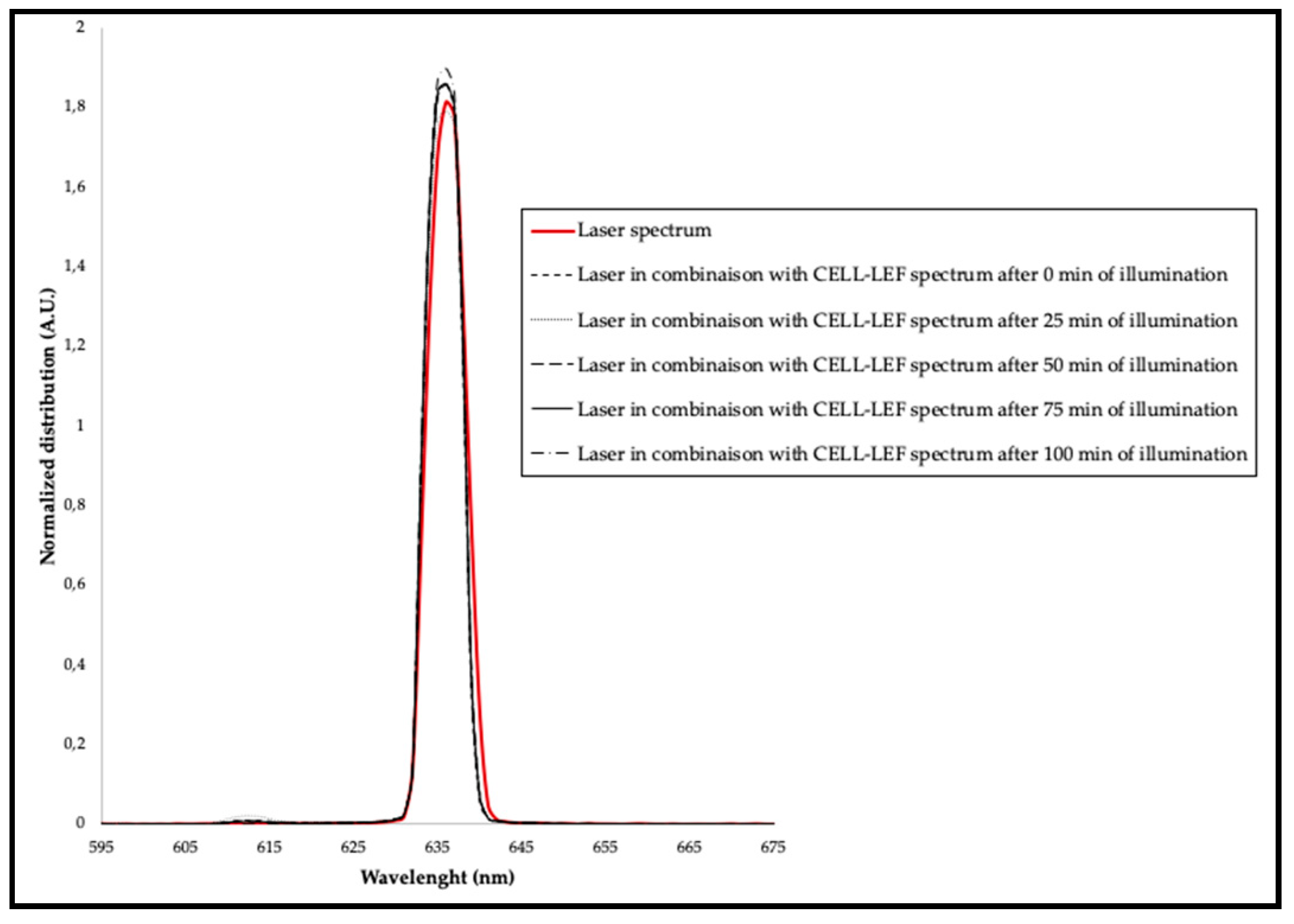
2.3.3. Spectral Distribution
2.3.4. Accessible Emission and User Safety
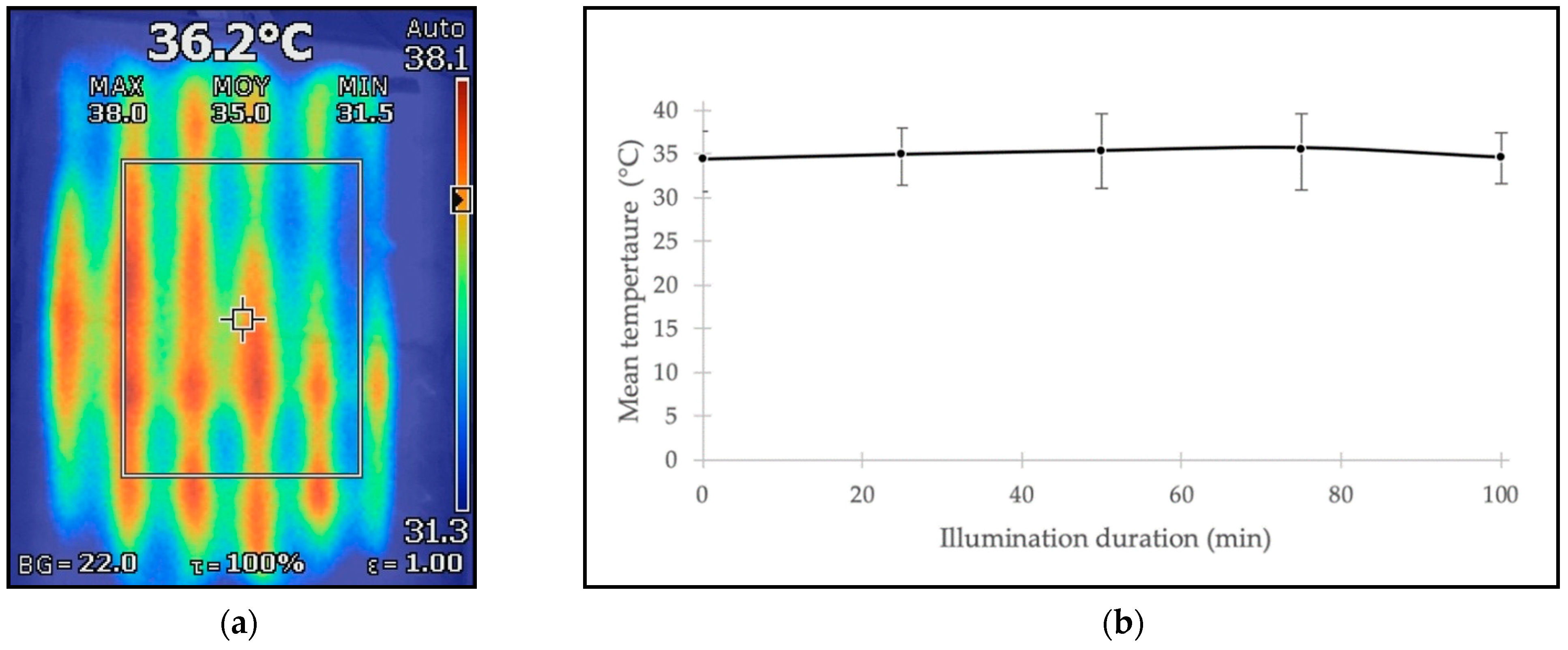
2.4. Thermal Characterization of Device
2.5. In Vitro Cytotoxic PDT Study Using CELL-LEF
2.5.1. Cell Culture and Photosensitization
2.5.2. Photodynamic Therapy Protocols
Concentration and Light Dose
Fractionation
2.5.3. Viability Assays
2.5.4. Statistical Analysis
3. Results
3.1. Optical Characterization of Device
3.1.1. Irradiance Level at the CELL-LEF Surface
3.1.2. Irradiance Distribution in 96-Well Plates
3.1.3. Spectral Distribution
3.1.4. Accessible Emission and User Safety
3.2. Thermal Characterization of Device
3.3. In Vitro Cytotoxic PDT Study Using CELL-LEF
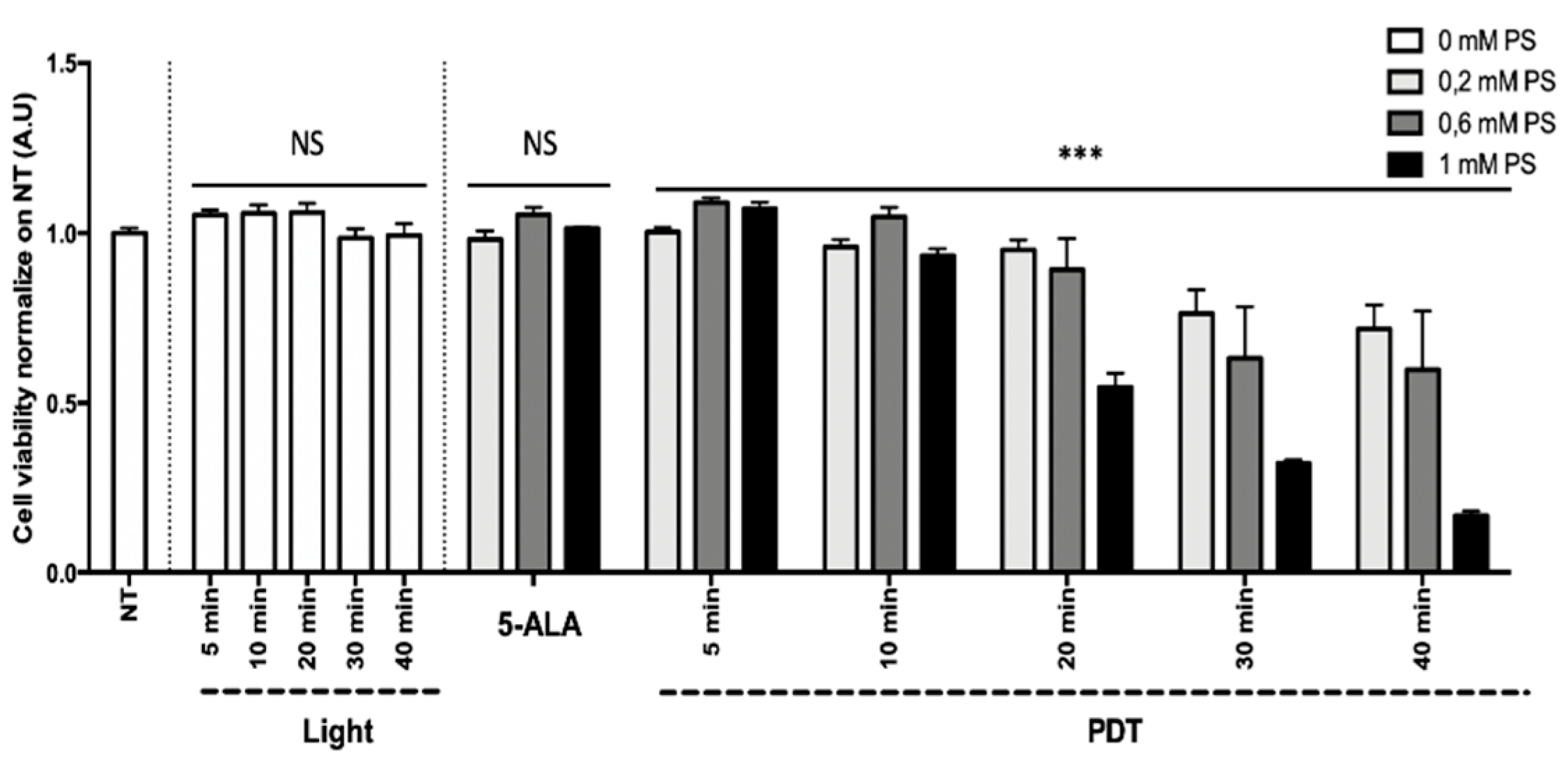
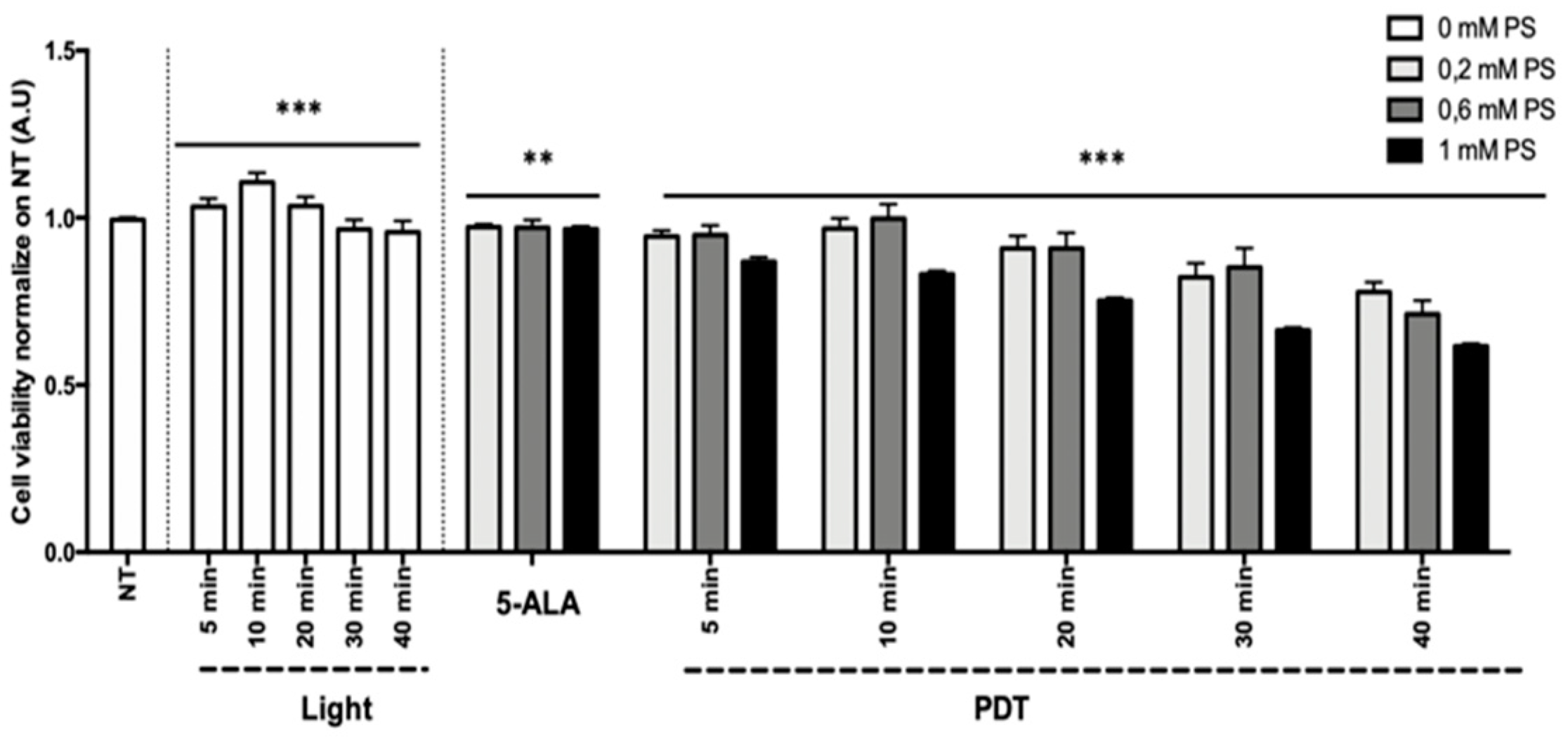
3.3.1. Concentration and Light Dose
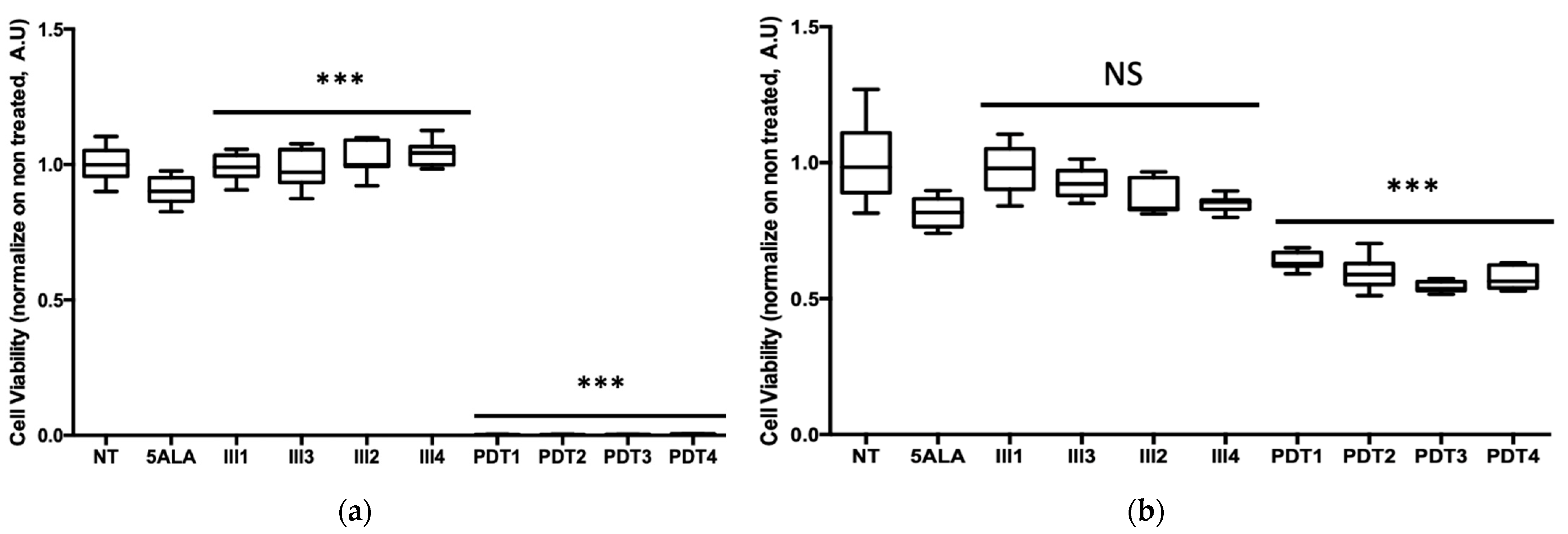
3.3.2. Fractionation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic therapy of cancer: An update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef]
- Sliney, D.H. Radiometric Quantities and Units Used in Photobiology and Photochemistry: Recommendations of the Commission Internationale de l’Eclairage (International Commission on Illumination). Photochem. Photobiol. 2007, 83, 425–432. [Google Scholar] [CrossRef]
- Chilakamarthi, U.; Giribabu, L. Photodynamic Therapy: Past, Present and Future. Chem. Rec. 2017, 17, 775–802. [Google Scholar] [CrossRef]
- Schaberle, F.A. Assessment of the actual light dose in photodynamic therapy. Photodiagnosis Photodyn. Ther. 2018, 23, 75–77. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.W.; Kim, J.H.; Park, K. In Vitro Photodynamic Effects of the Inclusion Nanocomplexes of Glucan and Chlorin e6 on Atherogenic Foam Cells. Int. J. Mol. Sci. 2020, 22, 177. [Google Scholar] [CrossRef] [PubMed]
- Bulin, A.-L.; Broekgaarden, M.; Simeone, D.; Hasan, T. Low dose photodynamic therapy harmonizes with radiation therapy to induce beneficial effects on pancreatic heterocellular spheroids. Oncotarget 2019, 10, 2625–2643. [Google Scholar] [CrossRef]
- Meier, D.; Campanile, C.; Botter, S.M.; Born, W.; Fuchs, B. Cytotoxic Efficacy of Photodynamic Therapy in Osteosarcoma Cells In Vitro. J. Vis. Exp. 2014, 18, e51213. [Google Scholar] [CrossRef] [PubMed]
- Zhu, T.C.; Kim, M.M.; Jacques, S.L.; Penjweini, R.; Dimofte, A.; Finlay, J.C.; Simone, C.; Cengel, K.A.; Friedberg, J. Real-time treatment light dose guidance of Pleural PDT: An update. Proc. SPIE Int. Soc. Opt. Eng. 2015, 9308, 930809. [Google Scholar] [CrossRef]
- Vahabi, S.; Fekrazad, R.; Ayremlou, S.; Taheri, S.; Zangeneh, N. The Effect of Antimicrobial Photodynamic Therapy with Radachlorin and Toluidine Blue on Streptococcus Mutans: An in Vitro Study. J. Dent. 2011, 8, 48–54. [Google Scholar]
- Mathews, M.S.; Angell-Petersen, E.; Sanchez, R.; Sun, C.-H.; Vo, V.; Hirschberg, H.; Madsen, S.J. The effects of ultra low fluence rate single and repetitive photodynamic therapy on glioma spheroids. Lasers Surg. Med. 2009, 41, 578–584. [Google Scholar] [CrossRef]
- Liu, T.; Wu, L.Y.; Choi, J.K.; Berkman, C.E. In vitro targeted photodynamic therapy with a pyropheophorbide-a conjugated inhibitor of prostate-specific membrane antigen. Prostate 2009, 69, 585–594. [Google Scholar] [CrossRef]
- Winther, J. Photodynamic therapy effect in an intraocular retinoblastoma-like tumour assessed by an in vivo to in vitro colony forming assay. Br. J. Cancer 1989, 59, 869–872. [Google Scholar] [CrossRef] [PubMed]
- Rossi, F.; Campbell, D.; Pottier, R.; Kennedy, J.; Dickson, E. In vitro studies on the potential use of 5-aminolaevulinic acid-mediated photodynamic therapy for gynaecological tumours. Br. J. Cancer 1996, 74, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Wyld, L.; Reed, M.; Brown, N. The influence of hypoxia and pH on aminolaevulinic acid-induced photodynamic therapy in bladder cancer cells in vitro. Br. J. Cancer 1998, 77, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Vignion-Dewalle, A.; Baert, G.; Thecua, E.; Lecomte, F.; Vicentini, C.; Abi-Rached, H.; Mortier, L.; Mordon, S. Comparison of 10 efficient protocols for photodynamic therapy of actinic keratosis: How relevant are effective light dose and local damage in predicting the complete response rate at 3 months? Lasers Surg. Med. 2018, 50, 576–589. [Google Scholar] [CrossRef]
- Moseley, H. Light distribution and calibration of commercial PDT LED arrays. Photochem. Photobiol. Sci. 2005, 4, 911–914. [Google Scholar] [CrossRef]
- Kim, M.M.; Darafsheh, A. Light Sources and Dosimetry Techniques for Photodynamic Therapy. Photochem. Photobiol. 2020, 96, 280–294. [Google Scholar] [CrossRef]
- Dupont, C.; Mordon, S.; Deleporte, P.; Reyns, N.; Vermandel, M. A novel device for intraoperative photodynamic therapy dedicated to glioblastoma treatment. Futur. Oncol. 2017, 13, 2441–2454. [Google Scholar] [CrossRef]
- Kruijt, B.; van der Snoek, E.M.; Sterenborg, H.; Amelink, A.; Robinson, D.J. A dedicated applicator for light delivery and monitoring of PDT of intra-anal intraepithelial neoplasia. Photodiagnosis Photodyn. Ther. 2010, 7, 3–9. [Google Scholar] [CrossRef]
- Soergel, P.; Wang, X.; Stepp, H.; Hertel, H.; Hillemanns, P. Photodynamic therapy of cervical intraepithelial neoplasia with hexaminolevulinate. Lasers Surg. Med. 2008, 40, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Nyst, H.J.; Van Veen, R.L.P.; Tan, I.B.; Peters, R.; Spaniol, S.; Robinson, D.J.; Stewart, F.A.; Levendag, P.C.; Sterenborg, H. Performance of a dedicated light delivery and dosimetry device for photodynamic therapy of nasopharyngeal carcinoma: Phantom and volunteer experiments. Lasers Surg. Med. 2007, 39, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Guyon, L.; Lesage, J.C.; Betrouni, N.; Mordon, S. Development of a new illumination procedure for photodynamic therapy of the abdominal cavity. J. Biomed. Opt. 2012, 17, 0380011–0380018. [Google Scholar] [CrossRef] [PubMed]
- Vicentini, C.; Vignion-Dewalle, A.; Thecua, E.; LeComte, F.; Maire, C.; Deleporte, P.; Béhal, H.; Kerob, D.; Duhamel, A.; Mordon, S.; et al. Photodynamic therapy for actinic keratosis of the forehead and scalp: A randomized, controlled, phaseIIclinical study evaluating the noninferiority of a new protocol involving irradiation with a light-emitting, fabric-based device (the Flexitheralight protocol) compared with the conventional protocol involving irradiation with the AktiliteCL128 lamp. Br. J. Dermatol. 2019, 180, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Gilaberte, Y. Light-emitting textiles: An innovative and friendly way to perform photodynamic therapy. Br. J. Dermatol. 2019, 182, 11–12. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, C.; Mordon, S.; Lesage, J.C.; Koncar, V. New design of textile light diffusers for photodynamic therapy. Mater. Sci. Eng. C 2013, 33, 1170–1175. [Google Scholar] [CrossRef]
- Mordon, S.; Cochrane, C.; Tylcz, J.B.; Betrouni, N.; Mortier, L.; Koncar, V. Light emitting fabric technologies for photodynamic therapy. Photodiagnosis Photodyn. Ther. 2015, 12, 1–8. [Google Scholar] [CrossRef]
- Vignion-Dewalle, A.-S.; Vicentini, C.; Baert, G.; Thécua, E.; LeComte, F.; Mortier, L.; Mordon, S.R. Photodynamic therapy for actinic keratosis: A trend towards a decrease in irradiance without loss of efficacy for a better tolerability. In Proceedings of the 17th International Photodynamic Association World Congress, Cambridge, MA, USA, 28 June–4 July 2019. [Google Scholar] [CrossRef]
- Baddour, R.E.; Dadani, F.N.; Kolios, M.C.; Bisland, S.K. High-Frequency Ultrasound Assessment of Antimicrobial Photodynamic Therapy In Vitro. J. Biol. Phys. 2007, 33, 61–66. [Google Scholar] [CrossRef][Green Version]
- Mima, E.G.D.O.; Pavarina, A.C.; Ribeiro, D.G.; Dovigo, L.N.; Vergani, C.E.; Bagnato, V.S. Effectiveness of Photodynamic Therapy for the Inactivation ofCandidaspp. on Dentures:In Vitro Study. Photomed. Laser Surg. 2011, 29, 827–833. [Google Scholar] [CrossRef]
- Langmack, K.; Mehta, R.; Twyman, P.; Norris, P. Topical photodynamic therapy at low fluence rates—Theory and practice. J. Photochem. Photobiol. B: Biol. 2001, 60, 37–43. [Google Scholar] [CrossRef]
- Mordon, S.; Vignion-Dewalle, A.S.; Abi-Rached, H.; Thecua, E.; LeComte, F.; Vicentini, C.; Deleporte, P.; Béhal, H.; Kerob, D.; Hommel, T.; et al. The conventional protocol vs. a protocol including illumination with a fabric-based biophotonic device (the Phosistos protocol) in photodynamic therapy for actinic keratosis: A randomized, controlled, noninferiority clinical study. Br. J. Dermatol. 2019, 182, 76–84. [Google Scholar] [CrossRef]
- Apalla, Z.; Sotiriou, E.; Panagiotidou, D.; Lefaki, I.; Goussi, C.; Ioannides, D. The impact of different fluence rates on pain and clinical outcome in patients with actinic keratoses treated with photodynamic therapy. Photodermatol. Photoimmunol. Photomed. 2011, 27, 181–185. [Google Scholar] [CrossRef]
- Vermandel, M.; Quidet, M.; Vignion-Dewalle, A.-S.; Leroy, H.-A.; Leroux, B.; Mordon, S.; Reyns, N. Comparison of different treatment schemes in 5-ALA interstitial photodynamic therapy for high-grade glioma in a preclinical model: An MRI study. Photodiagnosis Photodyn. Ther. 2018, 25, 166–176. [Google Scholar] [CrossRef]
- Guo, H.-W.; Lin, L.-T.; Chen, P.-H.; Ho, M.-H.; Huang, W.-T.; Lee, Y.-J.; Chiou, S.-H.; Hsieh, Y.-S.; Dong, C.-Y.; Wang, H.-W. Low-fluence rate, long duration photodynamic therapy in glioma mouse model using organic light emitting diode (OLED). Photodiagnosis Photodyn. Ther. 2015, 12, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Gholam, P.; Bosselmann, I.; Enk, A.H.; Dick, J. Low irradiance compared with conventional photodynamic therapy in the treatment of actinic keratoses. Photodermatol. Photoimmunol. Photomed. 2018, 35, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Fonda-Pascual, P.; Alegre-Sánchez, A.; Harto-Castaño, A.; Moreno-Arrones, O.M.; Pérez-García, B.; González-Morales, M.L.; Ortega, C.P.; Gilaberte-Calzada, Y.; Aguilera, J.; Olasolo, P.J.; et al. Low-level light-assisted photodynamic therapy using a wearable cap-like device for the treatment of actinic keratosis of the scalp. Photodiagnosis Photodyn. Ther. 2018, 25, 136–141. [Google Scholar] [CrossRef]
- Hartl, B.A.; Hirschberg, H.; Marcu, L.; Cherry, S.R. Characterizing low fluence thresholds for in vitro photodynamic therapy. Biomed. Opt. Express 2015, 6, 770–779. [Google Scholar] [CrossRef] [PubMed]
- A Morton, C. A synthesis of the world’s guidelines on photodynamic therapy for non-melanoma skin cancer. G. Ital. di Dermatol. e Venereol. 2018, 153, 783–792. [Google Scholar] [CrossRef]
- Friedberg, J.S.; Mick, R.; Stevenson, J.; Metz, J.; Zhu, T.; Buyske, J.; Sterman, D.H.; I Pass, H.; Glatstein, E.; Hahn, S.M. A phase I study of Foscan-mediated photodynamic therapy and surgery in patients with mesothelioma. Ann. Thorac. Surg. 2003, 75, 952–959. [Google Scholar] [CrossRef]
- Van Straten, D.; Mashayekhi, V.; De Bruijn, H.S.; Oliveira, S.; Robinson, D.J. Oncologic Photodynamic Therapy: Basic Principles, Current Clinical Status and Future Directions. Cancers 2017, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Austin, E.; Jagdeo, J. An In Vitro Approach to Photodynamic Therapy. J. Vis. Exp. 2018, 138, e58190. [Google Scholar] [CrossRef]
- Busch, T.M.; Wileyto, E.P.; Emanuele, M.J.; Del Piero, F.; Marconato, L.; Glatstein, E.; Koch, C.J. Photodynamic therapy creates fluence rate-dependent gradients in the intratumoral spatial distribution of oxygen. Cancer Res. 2002, 62, 7273–7279. [Google Scholar] [PubMed]
- Henderson, B.W.; Busch, T.M.; Snyder, J.W. Fluence rate as a modulator of PDT mechanisms. Lasers Surg. Med. 2006, 38, 489–493. [Google Scholar] [CrossRef]
- Seshadri, M.; Bellnier, D.; Vaughan, L.A.; Spernyak, J.A.; Mazurchuk, R.; Foster, T.; Henderson, B.W. Light Delivery over Extended Time Periods Enhances the Effectiveness of Photodynamic Therapy. Clin. Cancer Res. 2008, 14, 2796–2805. [Google Scholar] [CrossRef]
- Bisland, S.; Lilge, L.; Lin, A.; Rusnov, R.; Wilson, B. Metronomic PDT as a New Paradigm for Photodynamic Therapy: Rationale and Pre-Clinical Evaluation of Technical Feasibility for Treating Malignant Brain Tumors. Photochem. Photobiol. 2004, 80, 22–30. [Google Scholar] [CrossRef]
- Wilson, B.C.; Patterson, M. The physics, biophysics and technology of photodynamic therapy. Phys. Med. Biol. 2008, 53, R61–R109. [Google Scholar] [CrossRef]
- Curnow, A.; McIlroy, B.W.; Postle-Hacon, M.J.; MacRobert, A.J.; Bown, S.G. Light dose fractionation to enhance photodynamic therapy using 5-aminolevulinic acid in the normal rat colon. Photochem. Photobiol. 1999, 69, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Wulf, H.C. Daylight PDT acts by continuous activation of PpIX. Photodiagnosis Photodyn. Ther. 2019, 27, A1–A2. [Google Scholar] [CrossRef]
- Wulf, H.; Heerfordt, I.; Philipsen, P. How Much Protoporphyrin IX Must Be Activated to Obtain Full Efficacy of Methyl Aminolevulinate Photodynamic Therapy? Implication for Treatment Modifications. Pharm. 2021, 14, 333. [Google Scholar] [CrossRef]
- Rieder, C. Effect of hypothermia (20–25 °C) on mitosis in PtK1 cells. Cell Biol. Int. Rep. 1981, 5, 563–573. [Google Scholar] [CrossRef]
- Christensen, T.; Wahl, A.; Smedshammer, L. Effects of haematoporphyrin derivative and light in combination with hyperthermia on cells in culture. Br. J. Cancer 1984, 50, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wu, Q.; Jiang, S.; Liu, X.; Xiong, L.; Xia, Y.; Chen, A.C.-H. The influence of temperature on 5-aminolevulinic acid-based photodynamic reaction in keratinocytes in vitro. Photodermatol. Photoimmunol. Photomed. 2010, 26, 83–88. [Google Scholar] [CrossRef]
- Agrawal, G.P. Fiber-Optic Communication Systems; Wiley: Hoboken, NJ, USA, 2002; Volume 222. [Google Scholar]
- Tankere, J.; Boucard, N.; Mignot, E.; Donge, C. Structure Textile Lumineux Intégrant des Fibres Optiques. Patent Number WO2016097524A1, 23 March 2016. [Google Scholar]
- Daniel, M. Light Emitting Fabric. U.S. Patent US4234907A, 18 November 1980. [Google Scholar]
- Barbe, C.; Brochier, C.; Chevalier, D.; Morange, J. Method for producing a lighting device and resulting device. U.S. Patent US20180143367A1, 18 August 2020. [Google Scholar]
- Bernasson, A.; Peuvergne, H. Fibre Optique a Eclairage Lateral Multi-Ponctuel. Patent Number WO1995016877A1, 22 June 1995. [Google Scholar]
- Kenneth, J.E.; Franklin, J.B.; Smith, G.B. Improvements in Side-Scattering Light Guides. Patent Number WO2004023181, 18 March 2004. [Google Scholar]
- Schrank, V.; Beer, M.; Beckers, M.; Gries, T. Polymer-optical fibre (POF) integration into textile fabric structures. In Polymer Optical Fibres; Woodhead Publishing: Sawston, UK, 2016; pp. 337–348. [Google Scholar] [CrossRef]
- Quandt, B.M.; Pfister, M.S.; Lübben, J.F.; Spano, F.; Rossi, R.M.; Bona, G.-L.; Boesel, L.F. POF-yarn weaves: Controlling the light out-coupling of wearable phototherapy devices. Biomed. Opt. Express 2017, 8, 4316–4330. [Google Scholar] [CrossRef]
- Shen, J.; Chui, C.; Tao, X. Luminous fabric devices for wearable low-level light therapy. Biomed. Opt. Express 2013, 4, 2925–2937. [Google Scholar] [CrossRef] [PubMed]
- Oguz, Y.; Cochrane, C.; Koncar, V.; Mordon, S.R. Doehlert experimental design applied to optimization of light emitting textile structures. Opt. Fiber Technol. 2016, 30, 38–47. [Google Scholar] [CrossRef]
- Endruweit, A.; Long, A.C.; Johnson, M.S. Textile composites with integrated optical fibres: Quantification of the influence of single and multiple fibre bends on the light transmission using a Monte Carlo ray-tracing method. Smart Mater. Struct. 2007, 17. [Google Scholar] [CrossRef]
- Selm, B.; Rothmaier, M. Radiation properties of two types of luminous textile devices containing plastic optical fibers. In Microtechnologies for the New Millennium 2003; SPIE: Bellingham, WA, USA, 2007; Volume 6593. [Google Scholar]
- Selm, B.; Rothmaier, M.; Camenzind, M.; Khan, T.; Walt, H. Novel flexible light diffuser and irradiation properties for photodynamic therapy. J. Biomed. Opt. 2007, 12, 034024-1–034024-7. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Khan, T.; Unternährer, M.; Buchholz, J.; Kaser-Hotz, B.; Selm, B.; Rothmaier, M.; Walt, H. Performance of a contact textile-based light diffuser for photodynamic therapy. Photodiagnosis Photodyn. Ther. 2006, 3, 51–60. [Google Scholar] [CrossRef]
- Gong, Z.; Xiang, Z.; Ouyang, X.; Zhang, J.; Lau, N.; Zhou, J.; Chan, C.C. Wearable Fiber Optic Technology Based on Smart Textile: A Review. Mater. 2019, 12, 3311. [Google Scholar] [CrossRef]
- Plümpe, M.; Beckers, M.; Mecnika, V.; Seide, G.; Gries, T.; Bunge, C.-A. Applications of polymer-optical fibres in sensor technology, lighting and further applications. In Polymer Optical Fibres; Woodhead Publishing: Sawston, UK, 2016; pp. 311–335. [Google Scholar] [CrossRef]
- Baydoun, M.; Moralès, O.; Frochot, C.; Ludovic, C.; Leroux, B.; Thecua, E.; Ziane, L.; Grabarz, A.; Kumar, A.; De Schutter, C.; et al. Photodynamic Therapy Using a New Folate Receptor-Targeted Photosensitizer on Peritoneal Ovarian Cancer Cells Induces the Release of Extracellular Vesicles with Immunoactivating Properties. J. Clin. Med. 2020, 9, 1185. [Google Scholar] [CrossRef]
- Quilbe, A.; Moralès, O.; Baydoun, M.; Kumar, A.; Mustapha, R.; Murakami, T.; Leroux, B.; De Schutter, C.; Thecua, E.; Ziane, L.; et al. An Efficient Photodynamic Therapy Treatment for Human Pancreatic Adenocarcinoma. J. Clin. Med. 2020, 9, 192. [Google Scholar] [CrossRef] [PubMed]
- Ioannides, N.; Chunga, E.B.; Bachmatiuk, A.; Gonzalezmartinez, I.G.; Trzebicka, B.; Adebimpe, D.; Kalymnios, D.; Rümmeli, M.H. Approaches to mitigate polymer-core loss in plastic optical fibers: A review. Mater. Res. Express 2014, 1, 032002. [Google Scholar] [CrossRef]
- Durana, G.; Zubia, J.; Arrue, J.; Aldabaldetreku, G.; Mateo, J. Dependence of bending losses on cladding thickness in plastic optical fibers. Appl. Opt. 2003, 42, 997–1002. [Google Scholar] [CrossRef]
- Abo-Zeid, M.; Abo-Elfadl, M.T.; Mostafa, S.M. Photodynamic therapy using 5-aminolevulinic acid triggered DNA damage of adenocarcinoma breast cancer and hepatocellular carcinoma cell lines. Photodiagnosis Photodyn. Ther. 2018, 21, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Firdous, S.; Nawaz, M.; Ikram, M.; Ahmed, M. In vitro study of cell death with 5-aminolevulinic acid based photodynamic therapy to improve the efficiency of cancer treatment. Laser Phys. 2012, 22, 626–633. [Google Scholar] [CrossRef]
- Fakhar-E-Alam, M.; Atif, M.; AlSalhi, M.; Siddique, M.; Kishwar, S.; Qadir, M.I.; Willander, M. Role of ALA sensitivity in HepG2 cell in the presence of diode laser. Laser Phys. 2011, 21, 972–980. [Google Scholar] [CrossRef]
- Yow, C.M.N.; Wong, C.K.; Huang, Z.; Ho, R.J. Study of the efficacy and mechanism of ALA-mediated photodynamic therapy on human hepatocellular carcinoma cell. Liver Int. 2007, 27, 201–208. [Google Scholar] [CrossRef]
- Shinoda, Y.; Kato, D.; Ando, R.; Endo, H.; Takahashi, T.; Tsuneoka, Y.; Fujiwara, Y. Systematic Review and Meta-Analysis of In Vitro Anti-Human Cancer Experiments Investigating the Use of 5-Aminolevulinic Acid (5-ALA) for Photodynamic Therapy. Pharmaceuticals 2021, 14, 229. [Google Scholar] [CrossRef] [PubMed]
- Schipmann, S.; Müther, M.; Stögbauer, L.; Zimmer, S.; Brokinkel, B.; Holling, M.; Grauer, O.; Molina, E.S.; Warneke, N.; Stummer, W. Combination of ALA-induced fluorescence-guided resection and intraoperative open photodynamic therapy for recurrent glioblastoma: Case series on a promising dual strategy for local tumor control. J. Neurosurg. 2021, 134, 426–436. [Google Scholar] [CrossRef]
- Vermandel, M.; Dupont, C.; Lecomte, F.; Leroy, H.-A.; Tuleasca, C.; Mordon, S.; Hadjipanayis, C.G.; Reyns, N. Standardized intraoperative 5-ALA photodynamic therapy for newly diagnosed glioblastoma patients: A preliminary analysis of the INDYGO clinical trial. J. Neuro-Oncology 2021, 152, 501–514. [Google Scholar] [CrossRef]
- Koike, Y. Fundamentals of Plastic Optical Fibers; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Aldabaldetreku, G.; Durana, G.; Zubia, J.; Arrue, J. Analytical expression for measurement of intrinsic coupling loss in multistep index optical fibers. J. Light. Technol. 2006, 24, 1364–1375. [Google Scholar] [CrossRef]
- Loke, M.-Y.; McMullin, J. Simulation and measurement of radiation loss at multimode fiber macrobends. J. Light. Technol. 1990, 8, 1250–1256. [Google Scholar] [CrossRef]
- Losada, M.; Garcés, I.; Mateo, J.; Salinas, I.; Lou, J.; Zubia, J. Mode coupling contribution to radiation losses in curvatures for high and low numerical aperture plastic optical fibers. J. Light. Technol. 2002, 20, 1160–1164. [Google Scholar] [CrossRef]
- LED Box. Available online: https://loja.biolambda.com/led-box- (accessed on 29 March 2021).
- ML8500—Automatic Biomedical Illumination. Available online: https://www.modulight.com/ml8500/ (accessed on 29 March 2021).
- Hu, Y.; Wang, K.; Zhu, T.C. A light blanket for intraoperative photodynamic therapy. In Photodynamic Therapy: Back to the Future; International Society for Optics and Photonics: Bellingham, WA, USA, 2009; Volume 7380, p. 73801W. [Google Scholar] [CrossRef]
- Chamberlain, S.; Bellnier, D.; Yendamuri, S.; Lindenmann, J.; Demmy, T.; Nwogu, C.; Ramer, M.; Tworek, L.; Oakley, E.; Bs, M.M.; et al. An Optical Surface Applicator for Intraoperative Photodynamic Therapy. Lasers Surg. Med. 2020, 52, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Ogonowska, P.; Woźniak, A.; Pierański, M.K.; Wasylew, T.; Kwiek, P.; Brasel, M.; Grinholc, M.; Nakonieczna, J. Application and characterization of light-emitting diodes for photodynamic inactivation of bacteria. Light. Res. Technol. 2018, 51, 612–624. [Google Scholar] [CrossRef]
- Chen, H.; Yeh, T.-H.; He, J.; Zhang, C.; Abbel, R.; Hamblin, M.R.; Huang, Y.; Lanzafame, R.J.; Stadler, I.; Celli, J.; et al. Flexible quantum dot light-emitting devices for targeted photomedical applications. J. Soc. Inf. Disp. 2018, 26, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Juzeniene, A.; Juzenas, P.; Bronshtein, I.; Vorobey, A.; Moan, J. The influence of temperature on photodynamic cell killing in vitro with 5-aminolevulinic acid. J. Photochem. Photobiol. B: Biol. 2006, 84, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Curnow, A.; Haller, J.; Bown, S. Oxygen monitoring during 5-aminolaevulinic acid induced photodynamic therapy in normal rat colon: Comparison of continuous and fractionated light regimes. J. Photochem. Photobiol. B Biol. 2000, 58, 149–155. [Google Scholar] [CrossRef]
- Tetard, M.-C.; Vermandel, M.; Leroy, H.-A.; Leroux, B.; Maurage, C.-A.; Lejeune, J.-P.; Mordon, S.; Reyns, N.; Information, P.E.K.F.C. Interstitial 5-ALA photodynamic therapy and glioblastoma: Preclinical model development and preliminary results. Photodiagnosis Photodyn. Ther. 2016, 13, 218–224. [Google Scholar] [CrossRef]
- Farrar, M. Turning up the heat: Mechanistic insights into thermal photodynamic therapy. Br. J. Dermatol. 2016, 175, 458–459. [Google Scholar] [CrossRef]
- Shin, D.; Nguyen, L.; Le, M.T.; Ju, D.; Le, J.N.; Berg, K.; Hirschberg, H. The effects of low irradiance long duration photochemical internalization on glioma spheroids. Photodiagnosis Photodyn. Ther. 2019, 26, 442–447. [Google Scholar] [CrossRef]
- Kirino, I.; Fujita, K.; Sakanoue, K.; Sugita, R.; Yamagishi, K.; Takeoka, S.; Fujie, T.; Uemoto, S.; Morimoto, Y. Metronomic photodynamic therapy using an implantable LED device and orally administered 5-aminolevulinic acid. Sci. Rep. 2020, 10, 22017. [Google Scholar] [CrossRef]
- Wiegell, S.; Hædersdal, M.; Philipsen, P.A.; Eriksen, P.; Enk, C.; Wulf, H. Continuous activation of PpIX by daylight is as effective as and less painful than conventional photodynamic therapy for actinic keratoses; a randomized, controlled, single-blinded study. Br. J. Dermatol. 2008, 158, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Attili, S.K.; Lesar, A.; McNeill, A.; Camacho-Lopez, M.; Moseley, H.; Ibbotson, S.; Samuel, I.; Ferguson, J. An open pilot study of ambulatory photodynamic therapy using a wearable low-irradiance organic light-emitting diode light source in the treatment of nonmelanoma skin cancer. Br. J. Dermatol. 2009, 161, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Geralde, M.C.; Leite, I.S.; Inada, N.; Salina, A.C.G.; Medeiros, A.I.; Kuebler, W.M.; Kurachi, C.; Bagnato, V.S. Pneumonia treatment by photodynamic therapy with extracorporeal illumination - an experimental model. Physiol. Rep. 2017, 5, e13190. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Identification | Parameter | Emissions | Exposure Limits |
|---|---|---|---|
| UV | 5 × 10−7 | 5 × 10−3 | |
| 4.8 × 10−4 | 10 | ||
| IR | 8.7 × 10−5 | 100 | |
| Blue light | 0.238 | 100 | |
| Retinal thermal | 3111 | 28,000 | |
| 1.61 | 6000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thécua, E.; Ziane, L.; Grolez, G.P.; Fagart, A.; Kumar, A.; Leroux, B.; Baert, G.; Deleporte, P.; Vermandel, M.; Vignion-Dewalle, A.-S.; et al. A Warp-Knitted Light-Emitting Fabric-Based Device for In Vitro Photodynamic Therapy: Description, Characterization, and Application on Human Cancer Cell Lines. Cancers 2021, 13, 4109. https://doi.org/10.3390/cancers13164109
Thécua E, Ziane L, Grolez GP, Fagart A, Kumar A, Leroux B, Baert G, Deleporte P, Vermandel M, Vignion-Dewalle A-S, et al. A Warp-Knitted Light-Emitting Fabric-Based Device for In Vitro Photodynamic Therapy: Description, Characterization, and Application on Human Cancer Cell Lines. Cancers. 2021; 13(16):4109. https://doi.org/10.3390/cancers13164109
Chicago/Turabian StyleThécua, Elise, Laurine Ziane, Guillaume Paul Grolez, Alexandre Fagart, Abhishek Kumar, Bertrand Leroux, Gregory Baert, Pascal Deleporte, Maximilien Vermandel, Anne-Sophie Vignion-Dewalle, and et al. 2021. "A Warp-Knitted Light-Emitting Fabric-Based Device for In Vitro Photodynamic Therapy: Description, Characterization, and Application on Human Cancer Cell Lines" Cancers 13, no. 16: 4109. https://doi.org/10.3390/cancers13164109
APA StyleThécua, E., Ziane, L., Grolez, G. P., Fagart, A., Kumar, A., Leroux, B., Baert, G., Deleporte, P., Vermandel, M., Vignion-Dewalle, A.-S., Delhem, N., & Mordon, S. (2021). A Warp-Knitted Light-Emitting Fabric-Based Device for In Vitro Photodynamic Therapy: Description, Characterization, and Application on Human Cancer Cell Lines. Cancers, 13(16), 4109. https://doi.org/10.3390/cancers13164109