
Predictive Role of Leptin Receptor (Ob-R) Overexpression in Patients with Early Breast Cancer Receiving Neoadjuvant Systemic Treatment

Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Patient Population and Treatment
2.3. Procedures
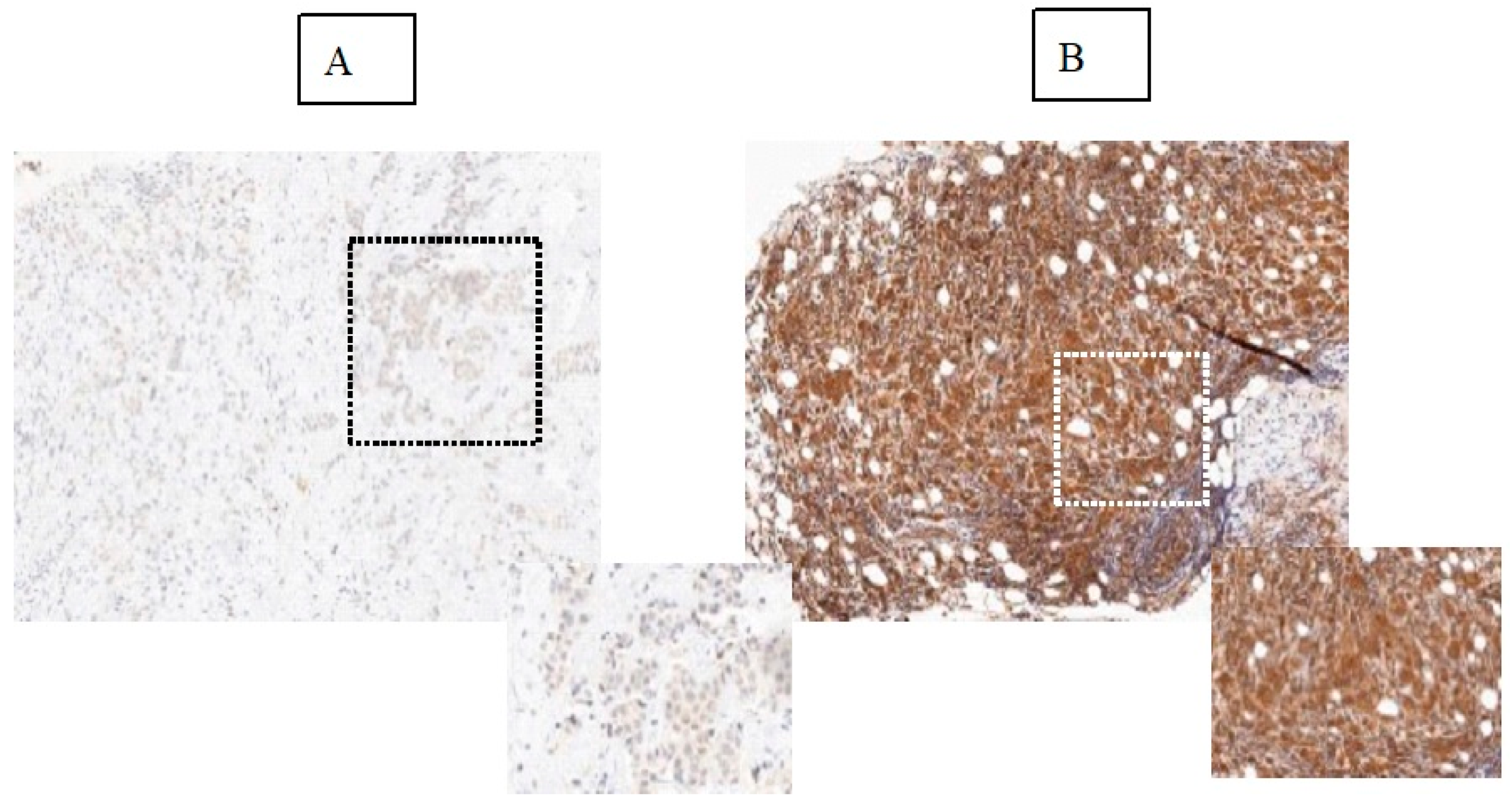
2.4. Ob-R Expression by Immunohistochemical Analysis
2.5. Endpoints and Definitions
2.6. Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. Ob-R Overexpression Is a Significant Predictive Factor for pCR in the Global Breast Cancer Population
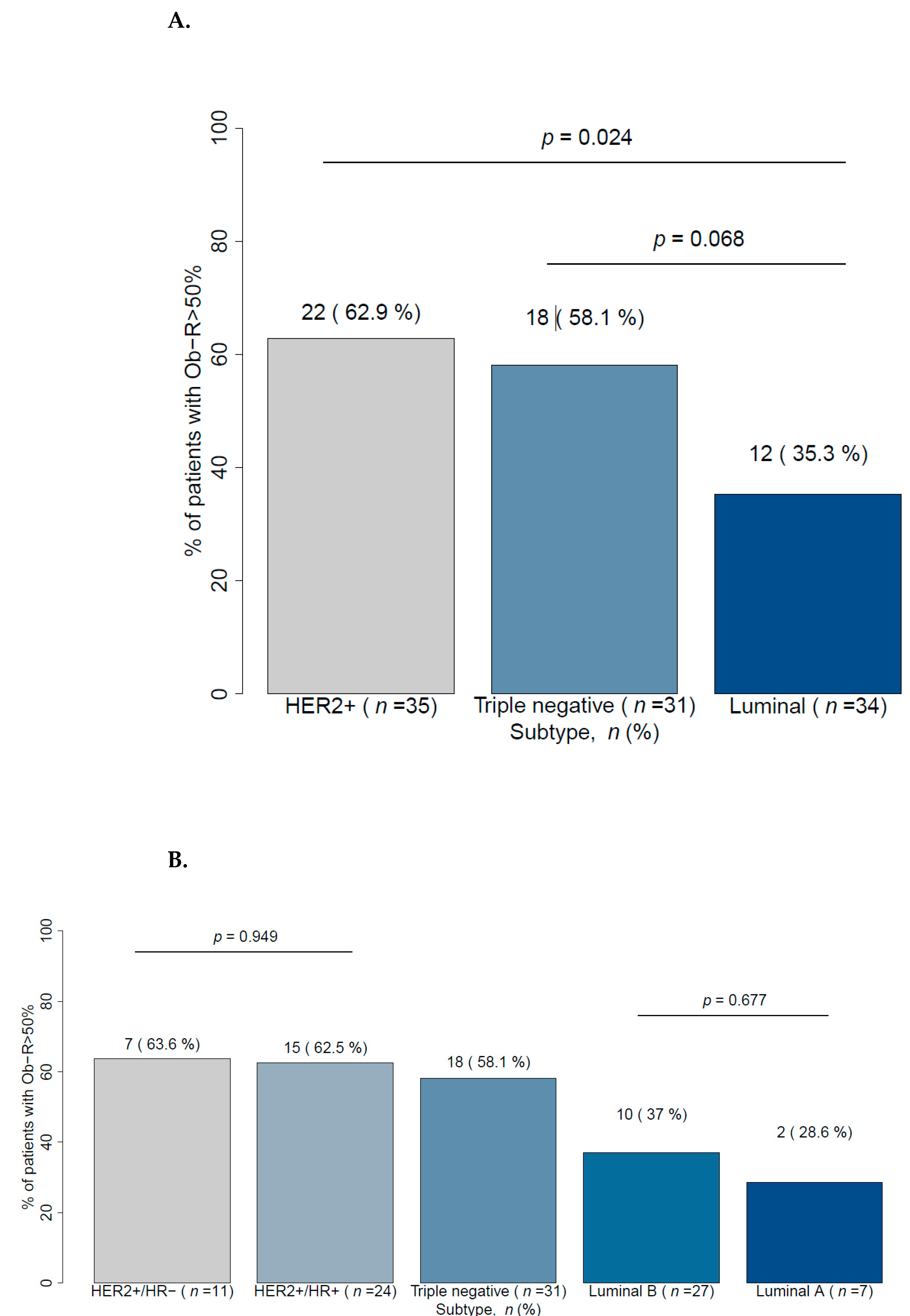
3.3. HER2 and TNBC Breast Cancer Show High Levels of Ob-R
3.4. The Correlation between Ob-R Overexpression and pCR Rate Depends on the Breast Cancer Subtype
3.5. Ob-R Overexpression Is Highly Correlated to Age and Menopausal Status in Breast Cancer
3.6. Ob-R Overexpression Is Significantly Associated with BMI in Breast Cancer Patients
3.7. Ob-R Overexpression Showed Not Association with Mammographic Breast Density (MBD)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.; Zackrisson, S.; Senkus, E. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loibl, S.; Denkert, C.; von Minckwitz, G. Neoadjuvant treatment of breast cancer—Clinical and research perspective. Breast 2015, 24, S73–S77. [Google Scholar] [CrossRef]
- Harbeck, N. Emerging strategies in neoadjuvant treatment of patients with HER2-positive early breast cancer. Breast 2019, 48 (Suppl. 1), S97–S102. [Google Scholar] [CrossRef] [Green Version]
- Loibl, S.; von Minckwitz, G.; Untch, M.; Denkert, C.; German Breast Group. Predictive factors for response to neoadjuvant therapy in breast cancer. Oncol. Res. Treat. 2014, 37, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhang, X.; Hao, Y.; Li, J. Obesity-related protein biomarkers for predicting breast cancer risk: An overview of systematic reviews. Breast Cancer 2021, 28, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Shukla, S.; Sinha, S.; Meeran, S.M. Role of adipokines and cytokines in obesity-associated breast cancer: Therapeutic targets. Cytokine Growth Factor Rev. 2013, 24, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Morley, T.S.; Kim, M.; Clegg, D.J.; Scherer, P.E. Obesity and cancer–mechanisms underlying tumour progression and recurrence. Nat. Rev. Endocrinol. 2014, 10, 455–465. [Google Scholar] [CrossRef] [Green Version]
- Cleary, M.P.; Phillips, F.C.; Getzin, S.C.; Jacobson, T.L.; Jacobson, M.K.; Christensen, T.A.; Juneja, S.C.; Grande, J.P.; Maihle, N.J. Genetically Obese MMTV-TGF-α/Lep ob Lep ob Female Mice do not Develop Mammary Tumors. Breast Cancer Res. Treat. 2003, 77, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Cleary, M.P.; Juneja, S.C.; Phillips, F.C.; Hu, X.; Grande, J.P.; Maihle, N.J. Leptin receptor-deficient MMTV-TGF-alpha/Lepr(db)Lepr(db) female mice do not develop oncogene-induced mammary tumors. Exp. Biol. Med. 2004, 229, 182–193. [Google Scholar] [CrossRef]
- Ray, A.; Cleary, M.P. The potential role of leptin in tumor invasion and metastasis. Cytokine Growth Factor Rev. 2017, 38, 80–97. [Google Scholar] [CrossRef] [PubMed]
- Maffei, M.; Halaas, J.; Ravussin, E.; Pratley, R.E.; Lee, G.H.; Zhang, Y.; Fei, H.; Kim, S.; Lallone, R.; Ranganathan, S.; et al. Leptin levels in human and rodent: Measurement of plasma leptin and ob RNA in obese and weight-reduced subjects. Nat. Med. 1995, 1, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Frederich, R.C.; Hamann, A.; Anderson, S.; Löllmann, B.; Lowell, B.B.; Flier, J.S. Leptin levels reflect body lipid content in mice: Evi-dence for diet-induced resistance to leptin action. Nat. Med. 1995, 1, 1311–1314. [Google Scholar] [CrossRef] [PubMed]
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L.; et al. Serum immunoreactive-leptin concen-trations in normal-weight and obese humans. N. Engl. J. Med. 1996, 334, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Bjørbaek, C.; Uotani, S.; da Silva, B.; Flier, J.S. Divergent signaling capacities of the long and short isoforms of the leptin receptor. J. Biol. Chem. 1997, 272, 32686–32695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, R.; Brakenhielm, E.; Wahlestedt, C.; Thyberg, J.; Cao, Y. Leptin induces vascular permeability and synergistically stimulates angiogenesis with FGF-2 and VEGF. Proc. Natl. Acad. Sci. USA 2001, 98, 6390–6395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, I.; Catalano, S.; Gelsomino, L.; Marsico, S.; Giordano, C.; Panza, S.; Bonofiglio, D.; Bossi, G.; Covington, K.R.; Fuqua, S.A.; et al. Leptin mediates tumor-stromal interactions that promote the invasive growth of breast cancer cells. Cancer Res. 2012, 72, 1416–1427. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, M.; Kitayama, J.; Nagawa, H. Enhanced Expression of Leptin and Leptin Receptor (OB-R) in Human Breast Cancer. Clin. Cancer Res. 2004, 10, 4325–4331. [Google Scholar] [CrossRef] [Green Version]
- D’Orsi, C.J.; Sickles, E.A.; Mendelson, E.B.; Morris, E.A. ACR BI-RADS Atlas: Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Wolff, A.C.; Hammond, M.E.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; American Society of Clinical Oncology; College of American Pathologists. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J. Clin. Oncol. 2007, 25, 118–145. [Google Scholar] [CrossRef] [Green Version]
- Coates, A.S.; Winer, E.P.; Goldhirsch, A.; Gelber, R.D.; Gnant, M.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J.; Members, P.; André, F.; et al. Tailoring therapies—improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann. Oncol. 2015, 26, 1533–1546. [Google Scholar] [CrossRef]
- Cheang, M.C.; Chia, S.K.; Voduc, D.; Gao, D.; Leung, S.; Snider, J.; Watson, M.; Davies, S.; Bernard, P.S.; Parker, J.S.; et al. Ki67 index, HER2 status, and prognosis of patients with luminal B breast cancer. J. Natl. Cancer Inst. 2009, 101, 736–750. [Google Scholar] [CrossRef] [Green Version]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.-J.; Albain, K.S.; Andre, F.; Bergh, J.; et al. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Garofalo, C.; Koda, M.; Cascio, S.; Sulkowska, M.; Kanczuga-Koda, L.; Golaszewska, J.; Russo, A.; Sulkowski, S.; Surmacz, E. Increased Expression of Leptin and the Leptin Receptor as a Marker of Breast Cancer Progression: Possible Role of Obesity-Related Stimuli. Clin. Cancer Res. 2006, 12, 1447–1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, Y.; Dong, Q.; Ji, H.; Sang, M.; Ding, Y.; Zhao, M.; Yang, H.; Geng, C. The Effect of the Leptin and Leptin Receptor Expression on the Efficacy of Neoadjuvant Chemotherapy in Breast Cancer. Med Sci. Monit. 2019, 25, 3005–3013. [Google Scholar] [CrossRef] [PubMed]
- Farrington, C.P.; Manning, G. Test statistics and sample size formulae for comparative binomial trials with null hypothesis of non-zero risk difference or non-unity relative risk. Stat. Med. 1990, 9, 1447–1454. [Google Scholar] [CrossRef]
- Phung, M.T.; Tin, S.T.; Elwood, J.M. Prognostic models for breast cancer: A systematic review. BMC Cancer 2019, 19, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Reis, F.J.C.; Wishart, G.C.; Dicks, E.M.; Greenberg, D.; Rashbass, J.; Schmidt, M.K.; Broek, A.J.V.D.; Ellis, I.O.; Green, A.; Rakha, E.; et al. An updated PREDICT breast cancer prognostication and treatment benefit prediction model with independent validation. Breast Cancer Res. 2017, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Ahima, R.S.; Flier, J.S. Leptin. Annu. Rev. Physiol. 2000, 62, 413–437. [Google Scholar] [CrossRef] [Green Version]
- Blüher, M.; Mantzoros, C.S. From leptin to other adipokines in health and disease: Facts and expectations at the beginning of the 21st century. Metabolism 2015, 64, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Li, M.-D. Leptin and Beyond: An Odyssey to the Central Control of Body Weight. Yale J. Boil. Med. 2011, 84, 1–7. [Google Scholar]
- Ihle, J.N. Cytokine receptor signalling. Nat. Cell Biol. 1995, 377, 591–594. [Google Scholar] [CrossRef]
- Jardé, T.; Caldefie-Chézet, F.; Damez, M.; Mishellany, F.; Penault-Llorca, F.; Guillot, J.; Vasson, M.P. Leptin and leptin receptor in-volvement in cancer development: A study on human primary breast carcinoma. Oncol. Rep. 2008, 19, 905–911. [Google Scholar] [PubMed] [Green Version]
- Kim, H.S. Leptin and Leptin Receptor Expression in Breast Cancer. Cancer Res. Treat. 2009, 41, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.C.; Huang, K.W.; Liu, C.W.; Chang, Y.C.; Lin, W.M.; Yang, T.Y.; Hsiao, M. Leptin signaling axis specifically associates with clini-cal prognosis and is multifunctional in regulating cancer progression. Oncotarget 2018, 9, 17210–17219. [Google Scholar] [CrossRef] [Green Version]
- Fiorio, E.; Mercanti, A.; Terrasi, M.; Micciolo, R.; Remo, A.; Auriemma, A.; Molino, A.; Parolin, V.; Di Stefano, B.; Bonetti, F.; et al. Leptin/HER2 crosstalk in breast cancer: In vitro study and preliminary in vivoanalysis. BMC Cancer 2008, 8, 305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, X.H.; Gu, J.C.; Bai, Q.Y.; Yu, W. Overexpression of leptin and leptin receptors in breast cancer positively correlates with clini-copathological features. Chin. Med. J. 2009, 122, 3078–3081. [Google Scholar] [PubMed]
- Wagner, K.-U.; Rui, H. Jak2/Stat5 Signaling in Mammogenesis, Breast Cancer Initiation and Progression. J. Mammary Gland. Biol. Neoplasia 2008, 13, 93–103. [Google Scholar] [CrossRef]
- Boothby-Shoemaker, W.; Benham, V.; Paithankar, S.; Shankar, R.; Chen, B.; Bernard, J.J. The Relationship between Leptin, the Leptin Receptor and FGFR1 in Primary Human Breast Tumors. Cells 2020, 9, 2224. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | All Patients * (n = 100) | With pCR * (n = 43) | Without pCR * (n = 57) | p-Value |
|---|---|---|---|---|
| Age, years | ||||
| Median (range) | 46 (29–81) | 46 (29–81) | 47 (33–73) | 0.427 |
| <50 years | 59 (59) | 28 (47.5) | 31 (52.5) | 0.281 |
| ≥50 years | 41 (41) | 15 (36.6) | 26 (63.4) | - |
| Menopausal status, n (%) | ||||
| Premenopausal | 65 (65) | 31 (47.7) | 34 (52.3) | 0.199 |
| Postmenopausal | 35 (35) | 12 (34.3) | 23 (65.7) | - |
| Height (cm) | ||||
| Median (range) | 164 (141–181) | 163 (141–181) | 164 (152–176) | 0.63 |
| Weight (kg) | ||||
| Median (range) | 62 (42–98) | 62 (42–98) | 63 (46–92) | 0.44 |
| BMI, n (%) | ||||
| Normal <25 | 68 (68) | 31 (45.6) | 37 (54.4) | 0.447 |
| Overweight / obesity | 32 (32) | 12 (37.5) | 20 (62.5) | - |
| MBD, n (%) | ||||
| A-B | 17 (17) | 8 (47.1) | 9 (52.9) | 0.731 |
| C-D | 80 (80) | 34 (42.5) | 46 (57.5) | - |
| Missing | 3 (3) | 1 (33.3) | 2 (66.7) | |
| Cancer subtype, n (%) | ||||
| HER2+ | 35 (35) | 20 (57.1) | 15 (42.9) | 0.01 |
| Triple negative | 31 (31) | 17 (54.8) | 14 (45.2) | 0.03 |
| Luminal | 34 (34) | 6 (17.6) | 28 (82.4) | - |
| Histological grade, n (%) | ||||
| G2 | 41 (41) | 16 (39) | 25 (61) | 0.198 |
| G3 | 55 (55) | 27 (49.1) | 28 (50.9) | - |
| Gx | 4 (4) | 0 (0) | 4 (100) | |
| T-score, n (%) | ||||
| T1-2 | 83 (83) | 37 (44.6) | 46 (55.4) | 0.915 |
| T3-4 | 13 (13) | 6 (46.2) | 7 (53.8) | |
| Tx | 4 (4) | 0 (0) | 4 (100) | |
| Nodal status, n (%) | ||||
| N0 | 50 (50) | 23 (46) | 27 (54) | 0.733 |
| N1 | 47 (47) | 20 (42.6) | 27 (57.4) | - |
| Nx | 3 (3) | 0 (0) | 3 (100) | |
| Ob-R cell positivity, n (%) | ||||
| ≤50% | 48 (48) | 13 (27.1) | 35 (72.9) | 0.002 |
| >50% | 52 (52) | 30 (57.7) | 22 (42.3) | - |
| Outcome: Ob-R > 50% | (A) Univariate Analyses | |||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p-Value | ||||
| Patients with < 50 y | 2.9 | 1.3 to 6.67 | 0.011 | |||
| Premenopausal status | 3.03 | 1.32 to 6.67 | 0.011 | |||
| Patients with BMI > 25 | 1.88 | 0.8 to 4.5 | 0.152 | |||
| Cancer type | ||||||
| HER2+ vs. Luminal | 3.10 | 1.18 to 8.52 | 0.024 | |||
| Triple negative vs. Luminal | 2.54 | 0.94 to 7.08 | 0.068 | |||
| Outcome: Ob-R > 50% | (B) Multivariate Analyses | |||||
| Menopausal Status as Factor | Age as Factor | |||||
| OR | 95%CI | p-Value | OR | 95%CI | p-Value | |
| Patients < 50 y | - | - | - | 5 | 2 to 14.3 | 0.001 |
| Premenopausal status | 5 | 2 to 14.3 | 0.001 | - | - | - |
| BMI > 25 | 3.52 | 1.35 to 11.88 | 0.017 | 3.50 | 1.27 to 10.54 | 0.019 |
| Cancer type | ||||||
| HER2+ vs. Luminal | 5.91 | 0.12 to 3.13 | 0.002 | 6.82 | 2.18 to 24.21 | 0.002 |
| TNBC vs. Luminal | 2.87 | 0.07 to 1.71 | 0.058 | 2.66 | 0.9 to 8.08 | 0.077 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Estévez, L.; Calvo, I.; Pérez, S.; Gallegos, I.; Díaz, E.; Sampayo-Cordero, M.; Oltra, S.S.; Moreno-Bueno, G. Predictive Role of Leptin Receptor (Ob-R) Overexpression in Patients with Early Breast Cancer Receiving Neoadjuvant Systemic Treatment. Cancers 2021, 13, 3269. https://doi.org/10.3390/cancers13133269
García-Estévez L, Calvo I, Pérez S, Gallegos I, Díaz E, Sampayo-Cordero M, Oltra SS, Moreno-Bueno G. Predictive Role of Leptin Receptor (Ob-R) Overexpression in Patients with Early Breast Cancer Receiving Neoadjuvant Systemic Treatment. Cancers. 2021; 13(13):3269. https://doi.org/10.3390/cancers13133269
Chicago/Turabian StyleGarcía-Estévez, Laura, Isabel Calvo, Silvia Pérez, Isabel Gallegos, Eva Díaz, Miguel Sampayo-Cordero, Sara S Oltra, and Gema Moreno-Bueno. 2021. "Predictive Role of Leptin Receptor (Ob-R) Overexpression in Patients with Early Breast Cancer Receiving Neoadjuvant Systemic Treatment" Cancers 13, no. 13: 3269. https://doi.org/10.3390/cancers13133269
APA StyleGarcía-Estévez, L., Calvo, I., Pérez, S., Gallegos, I., Díaz, E., Sampayo-Cordero, M., Oltra, S. S., & Moreno-Bueno, G. (2021). Predictive Role of Leptin Receptor (Ob-R) Overexpression in Patients with Early Breast Cancer Receiving Neoadjuvant Systemic Treatment. Cancers, 13(13), 3269. https://doi.org/10.3390/cancers13133269