
Development of a Secure Website to Facilitate Information Sharing in Families at High Risk of Bowel Cancer—The Familyweb Study


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
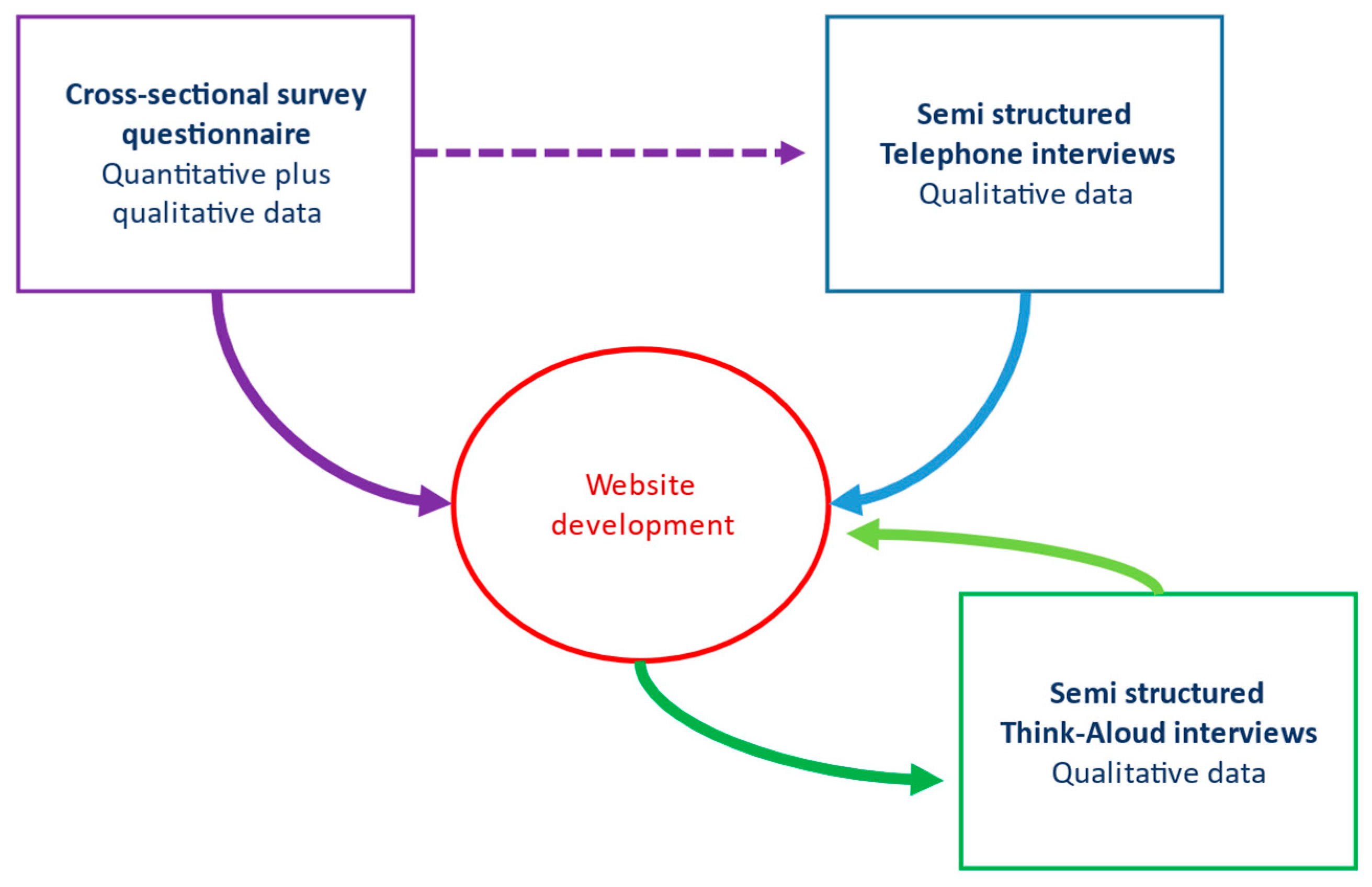
2.1. Design
2.2. Aims and Objectives
- Explore the perspectives of patients, including their experiences of how they received information about the familial diagnosis themselves;
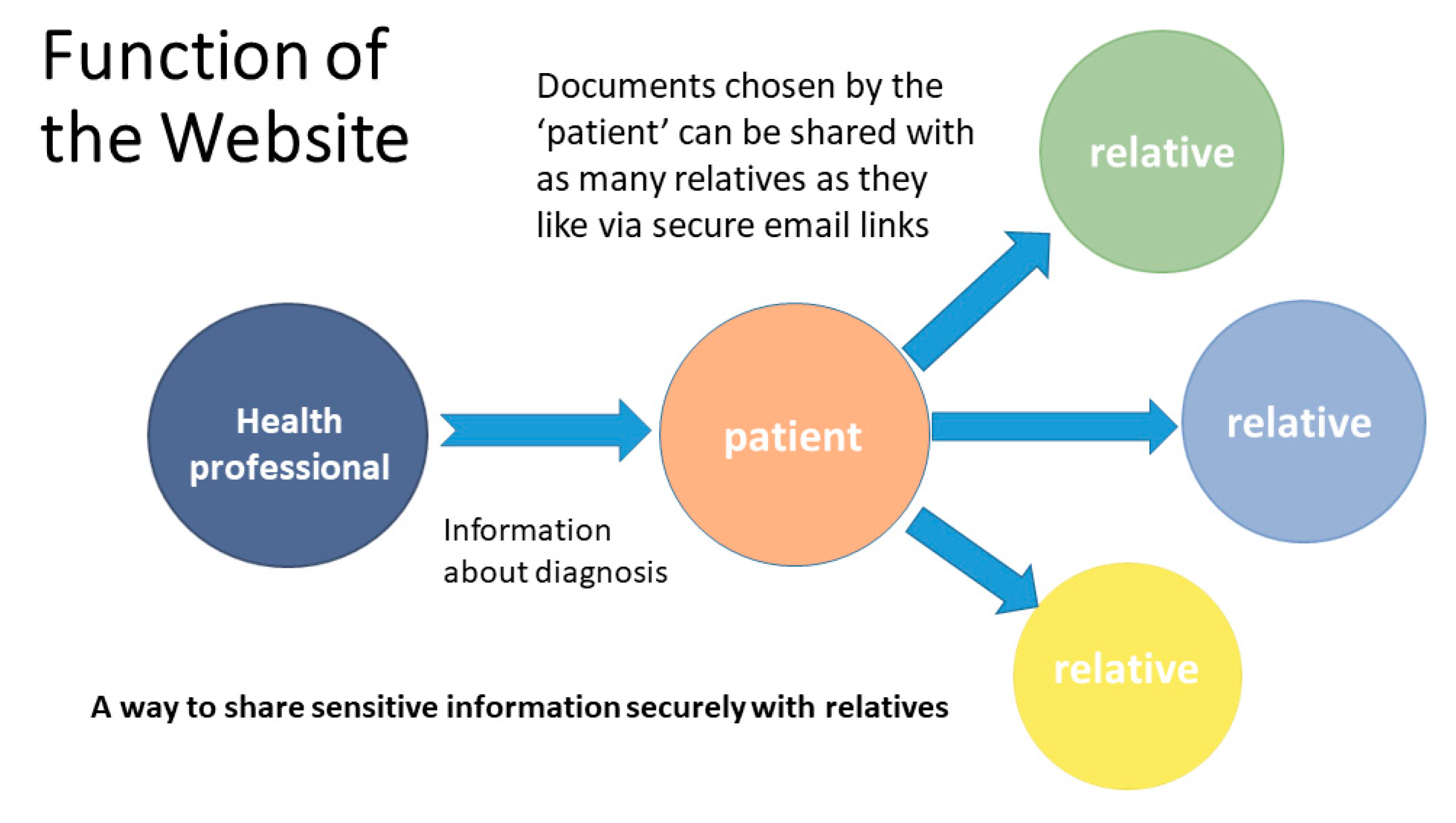
- Explore patients’ views about a secure website that provided a platform for patients to share documents about their diagnosis with their relatives;
- Investigate the feasibility and acceptability of sharing electronic documents regarding a familial diagnosis securely online using the purpose built website;
- Test the website’s function and acceptability with research participants [60] (p. 98).
2.3. Ethical Approval
2.4. Phase 1: Anonymous Cross-Sectional Survey
2.4.1. Inclusion and Exclusion Criteria for Phases 1 and 2
2.4.2. Recruitment to Phases 1 and 2
2.4.3. Data Collection Phase 1 Survey
2.4.4. Data Analysis Phase 1 Survey
2.4.5. Recruitment Phase 2 Telephone Interviews
2.4.6. Sampling and Data Collection Telephone Interviews
2.4.7. Data Analysis Phase 2
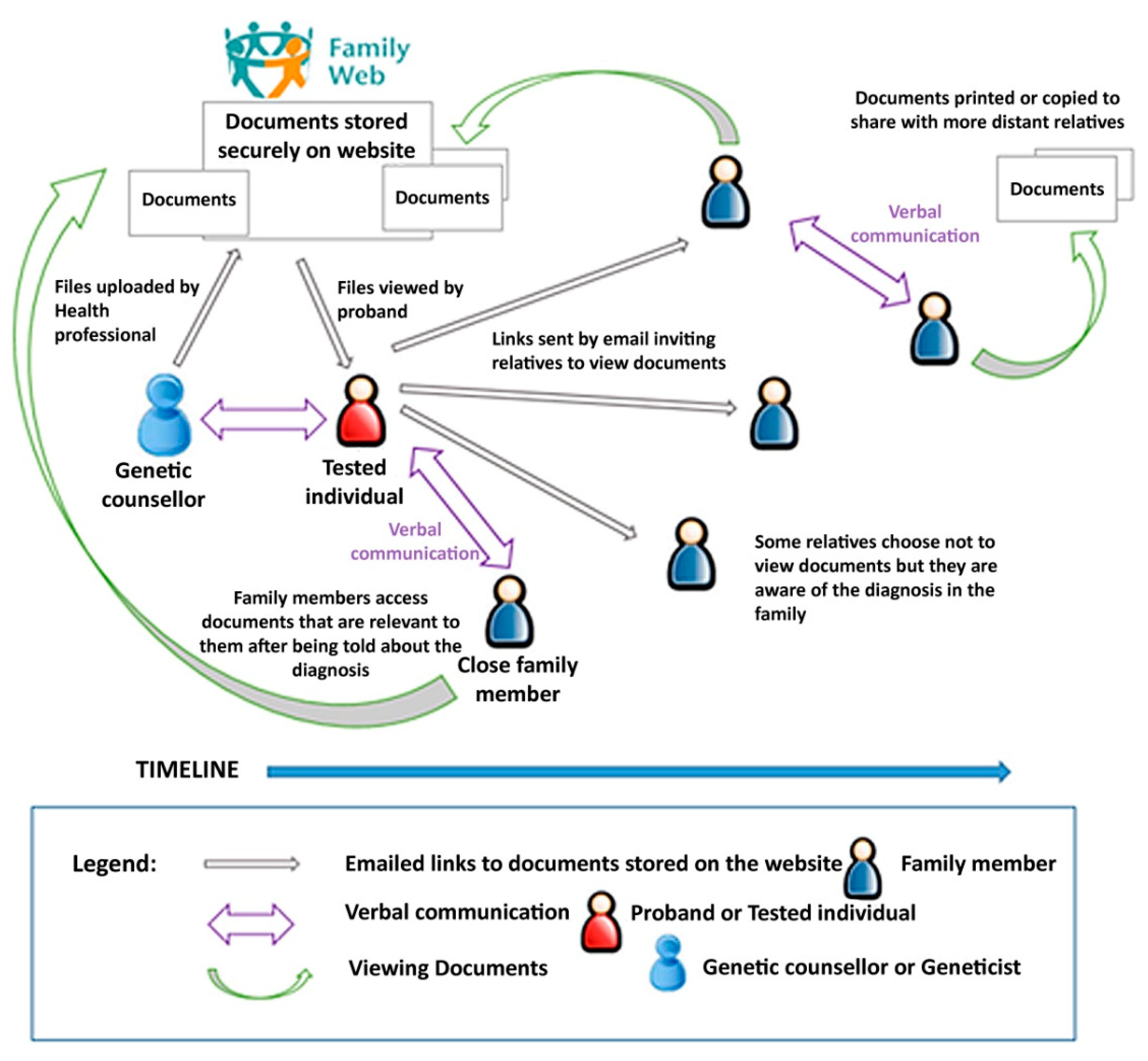
2.5. Website Development
2.6. Phase 3: Think-Aloud Interviews to Test Website Function
2.6.1. Data Collection
2.6.2. Phase 3 Data Analysis
3. Results
3.1. Phase 1 Survey
“Informal advice about how to broach this subject with relatives, some of whom I do not see often and who are not local to my area. The ‘To whom it may concern’ letter is rather too formal in my opinion”.Survey Participant 49 [60]
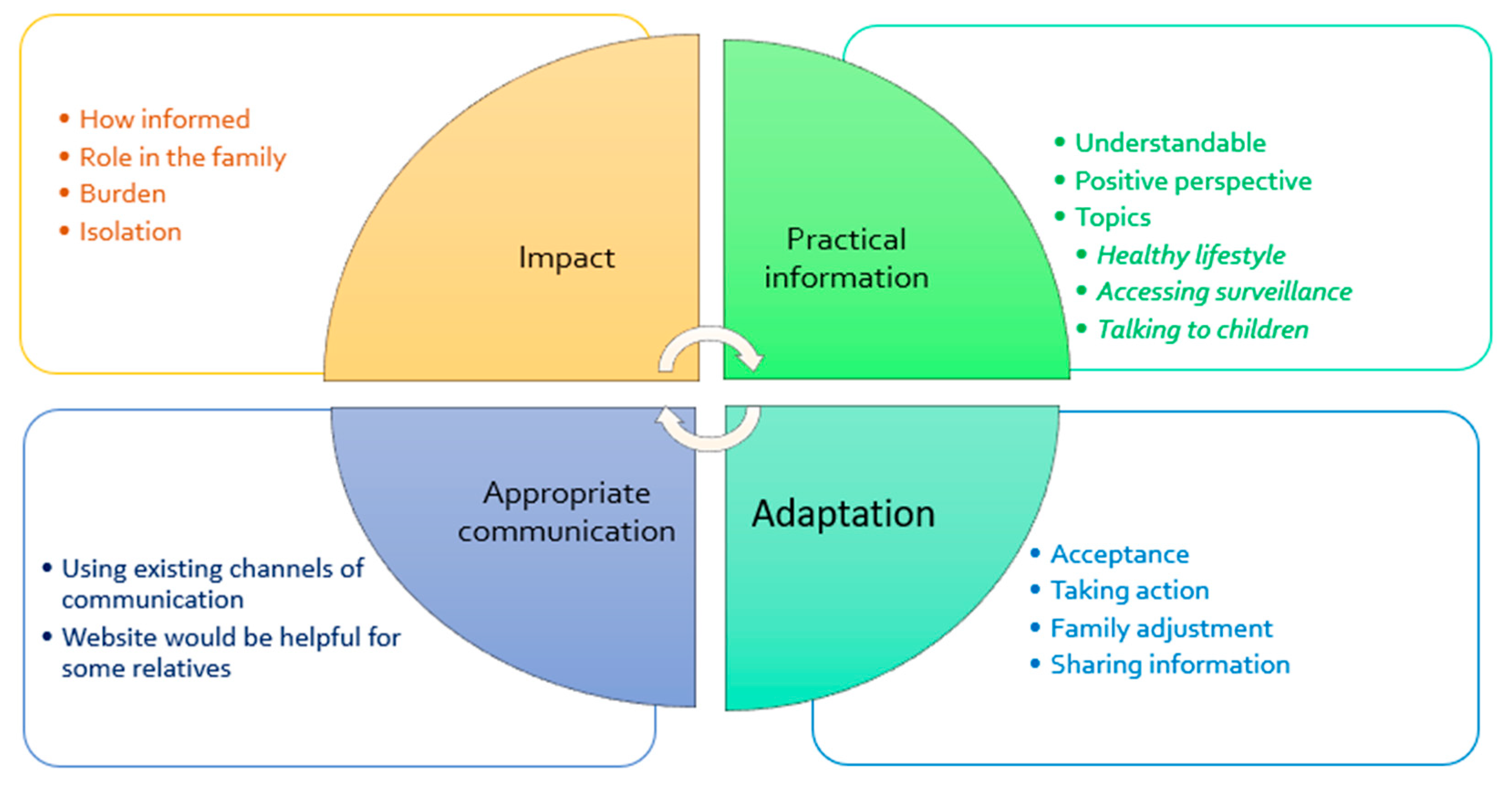
3.2. Phase 2 Telephone Interviews
“I would use whatever was appropriate to the person I was talking to. So, you know, if I was trying to explain to my father then I would use a patient information leaflet. If I was trying to explain to my nieces, then I would say “Look at this website””.[60]
“once he gets to that point where he feels “I can face it now” he can go and have a look and he can find the information but he needs to do it in his own time”.(Interview Subject 12) [60]
3.3. Results Phase 3 Think-Aloud Interviews
“I think the content looks really good and the way it is laid out is really good, it is really clear…… It’s not instantly clear what it is regarding… is this just about people with bowel cancer awareness?”.Luke (#2)
“This is my favourite page of it all because these are the questions that I have had to go away and find answers to myself”.Oliver (#1)
“How to get the right screening is quite important. Obviously diet, lifestyle, alcohol but the screening is what is most important. People want to know what they have to do.”Jenny (#11)
“I would put that right at the top. Something like.. healthy diet, exercise, everything that is good for everyone but you are at higher risk and it makes even more of a difference for you.”
4. Discussion
4.1. Practical Advice and the Theory of Planned Behaviour
4.2. Information That Is Trustworthy and Accurate
4.3. Positive Framing of Information
4.4. Study Limitations
4.5. Research Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| 1. Who first told you that there was a risk of bowel cancer in your family? Please tick one: □ Your doctor (General Practitioner “GP”) □ Specialist doctor (e.g., surgeon, gastroenterologist, oncologist, etc.) □ Genetics specialist (e.g., medical doctor or genetic counsellor) □ Another healthcare professional □ Your relative, can you tell us who? (e.g., mother, brother, cousin?) Other person, please tell us who? (e.g., friend or charity advisor?) □ Can’t remember Please answer the next questions (2, 3 & 4) only if you were told about the increased risk by a healthcare professional 2. Did you feel well supported at that time? Yes/No/Not sure 3. Please give suggestions below if you think that this could have been done better? 4. Are you the first person in your family to be told that there is an increased risk of cancer in the family? Yes/No/Don’t know 5. Please can you tell us what written information you received when you were told about your risk of cancer? Tick all that apply □ None received □ General information about the condition □ Specific information about your family □ A copy of your family tree indicating who had cancer □ A copy of your family tree showing who could have bowel screening □ A ‘Dear Relative’ or ‘To Whom it May Concern’ letter to give to your relatives □ Other—Please give details 6. Did you get the information you wanted? □ None of what I wanted □ Some of what I wanted □ Most of what I wanted □ All of what I wanted 6a. If you didn’t get all the information you wanted at that time, what other information might have been helpful? Please tell us… 7. If you have found additional information about the shared risk of cancer in your family, who provided that information? Tick all that apply □ Your doctor, surgeon or other health professional □ Other relatives □ Friends □ Support group or charity meeting □ Internet website □ Social media □ Library 8. If you found out more information via the Internet, what websites or social media were particularly helpful? Please give details below: 9. Would you like to receive information in other ways? Yes/No/Don’t know If yes, would this be □ Via a website □ By Email □ Social media □ In a follow-up appointment □ Other—Please state We would like to know if other forms of information for patients could make it easier to share information in the family. Below, we ask you to think about other ways that your doctor or genetic counsellor could give you information. Then please can you rate how helpful these might be to you and your relatives? 10. Please indicate how helpful you think this would be for the different ways of getting information by making a cross on each of the scales below: a. A paper leaflet which has general information about an increased risk of bowel cancer, the implications for relatives and the screening available? b. A secure email which has more specific information about your increased risk, the implications for your relatives and the screening advised? c. A password protected website which has more specific information about your increased risk, the implications for your relatives and the screening advised ? d. A follow-up appointment in the hospital clinic where you are given specific information about your increased risk, the implications for your relatives and the screening advised? e. A follow-up telephone call where you are given specific information about your increased risk, the implications for your relatives and the screening advised? 11. What issues would you like more information about? Please tick all that apply □ Talking to children □ Healthy lifestyle □ How can I help my relatives who live abroad □ How to find out more about genetic testing □ Other issues Please give us more details about any of the issues that concern you in the box below: 12. How many of your relatives are aware of the increased risk of cancer in the family? So, as far as you know □ All □ Most (please tick the one which applies) □ Some □ None □ I don’t know 13. If you have experienced any difficulties sharing information with your relatives about the increased risk can you tell us what those difficulties were? Please give details below, or pass on to the next question if there were no difficulties 14. Can you suggest ways in which your health professional could help you or your family more? Please give suggestions below. |
| Final page of the questionnaire was of demographic questions |
References
- Foulkes, W.D. Inherited Susceptibility to Common Cancers. New Engl. J. Med. 2008, 359, 2143–2153. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer Incidence and Mortality Rates and Trends--An Update. Cancer Epidemiol. Biomark. Prev. 2015, 25, 16–27. [Google Scholar] [CrossRef]
- Møller, P.; Seppälä, T.; Bernstein, I.; Holinski-Feder, E.; Sala, P.; Evans, D.G.; Lindblom, A.; Macrae, F.; Blanco, I.; Sijmons, R. Cancer incidence and survival in Lynch syndrome patients receiving colonoscopic and gynaecological surveillance: First report from the prospective Lynch syndrome database. Gut 2017, 66, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Grosse, S.D.; Rogowski, W.H.; Ross, L.F.; Cornel, M.C.; Dondorp, W.J.; Khoury, M.J. Population Screening for Genetic Disorders in the 21st Century: Evidence, Economics, and Ethics. Public Heal. Genom. 2010, 13, 106–115. [Google Scholar] [CrossRef]
- Seppälä, T.T.; Pylvänäinen, K.; Mecklin, J.-P. Uptake of genetic testing by the children of Lynch syndrome variant carriers across three generations. Eur. J. Hum. Genet. 2017, 25, 1237–1245. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Newton, K.; Gréen, K.; Lalloo, F.; Evans, G.; Evans, D.G.; Hill, J. Colonoscopy screening compliance and outcomes in patients with Lynch syndrome. Color. Dis. 2014, 17, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Vasen, H.F.A.; Velthuizen, M.E.; Kleibeuker, J.H.; Menko, F.H.; Nagengast, F.M.; Cats, A.; Jong, A.E.V.D.M.-D.; Breuning, M.H.; Roukema, A.J.; Van Leeuwen-Cornelisse, I.; et al. Hereditary cancer registries improve the care of patients with a genetic predisposition to cancer: Contributions from the Dutch Lynch syndrome registry. Fam. Cancer 2016, 15, 429–435. [Google Scholar] [CrossRef]
- Petersen, H.V.; Frederiksen, B.L.; Lautrup, C.K.; Lindberg, L.J.; Ladelund, S.; Nilbert, M. Unsolicited information letters to increase awareness of Lynch syndrome and familial colorectal cancer: Reactions and attitudes. Fam. Cancer 2018, 18, 43–51. [Google Scholar] [CrossRef]
- Adelson, M.; Pannick, S.; East, J.E.; Risby, P.; Dawson, P.; Monahan, K.J. UK colorectal cancer patients are inadequately assessed for Lynch syndrome. Front. Gastroenterol. 2013, 5, 31–35. [Google Scholar] [CrossRef]
- Monahan, K.J.; Alsina, D.; Bach, S.; Buchanan, J.; Burn, J.; Clark, S.; Dawson, P.; De Souza, B.; Din, F.V.N.; Dolwani, S.; et al. Urgent improvements needed to diagnose and manage Lynch syndrome. BMJ 2017, 356, j1388. [Google Scholar] [CrossRef]
- Sharaf, R.N.; Myer, P.; Stave, C.D.; Diamond, L.C.; Ladabaum, U. Uptake of Genetic Testing by Relatives of Lynch Syndrome Probands: A Systematic Review. Clin. Gastroenterol. Hepatol. 2013, 11, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Menko, F.H.; Ter Stege, J.A.; Van Der Kolk, L.E.; Jeanson, K.N.; Schats, W.; Moha, D.A.; Bleiker, E.M.A. The uptake of presymptomatic genetic testing in hereditary breast-ovarian cancer and Lynch syndrome: A systematic review of the literature and implications for clinical practice. Fam. Cancer 2018, 18, 127–135. [Google Scholar] [CrossRef]
- Snowsill, T.M.; Ryan, N.A.J.; Crosbie, E.J.; Frayling, I.M.; Evans, D.G.; Hyde, C.J. Cost-effectiveness analysis of reflex testing for Lynch syndrome in women with endometrial cancer in the UK setting. PLoS ONE 2019, 14, e0221419. [Google Scholar] [CrossRef]
- Kang, Y.; Killen, J.; Caruana, M.; Simms, K.; Taylor, N.; Frayling, I.M.; Snowsill, T.; Huxley, N.; Coupe, V.M.; Hughes, S.; et al. The predicted impact and cost-effectiveness of systematic testing of people with incident colorectal cancer for Lynch syndrome. Med. J. Aust. 2019, 212, 72–81. [Google Scholar] [CrossRef]
- Cowley, L. What can we Learn from Patients’ Ethical Thinking about the right ‘not to know’in Genomics? Lessons from Cancer Genetic Testing for Genetic Counselling. Bioethics 2016, 30, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Dheensa, S.; Lucassen, A.; Fenwick, A. Limitations and Pitfalls of Using Family Letters to Communicate Genetic Risk: A Qualitative Study with Patients and Healthcare Professionals. J. Genet. Couns. 2018, 27, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Snyder, C.; Hampel, H. Hereditary Colorectal Cancer Syndromes. Semin. Oncol. Nurs. 2019, 35, 58–78. [Google Scholar] [CrossRef]
- Campbell-Salome, G.; Buchanan, A.H.; Hallquist, M.L.; Rahm, A.K.; Rocha, H.; Sturm, A.C. Uncertainty management for individuals with Lynch Syndrome: Identifying and responding to healthcare barriers. Patient Educ. Couns. 2021, 104, 403–412. [Google Scholar] [CrossRef]
- Schwiter, R.; Rahm, A.K.; Williams, J.L.; Sturm, A.C. How Can We Reach At-Risk Relatives? Efforts to Enhance Communication and Cascade Testing Uptake: A Mini-Review. Curr. Genet. Med. Rep. 2018, 6, 21–27. [Google Scholar] [CrossRef]
- De Geus, E.; Aalfs, C.M.; Verdam, M.G.; De Haes, H.C.; Smets, E.M. Informing relatives about their hereditary or familial cancer risk: Study protocol for a randomized controlled trial. Trials 2014, 15, 86. [Google Scholar] [CrossRef]
- De Geus, E.; Eijzenga, W.; Menko, F.H.; Sijmons, R.H.; De Haes, H.C.J.M.; Aalfs, C.M.; Smets, E.M.A. Design and Feasibility of an Intervention to Support Cancer Genetic Counselees in Informing their At-Risk Relatives. J. Genet. Couns. 2016, 25, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, J.; Metcalfe, S.; Gaff, C.; Donath, S.; Delatycki, M.B.; Winship, I.; Skene, L.; Aitken, M.; Halliday, J. Outcomes of a randomised controlled trial of a complex genetic counselling intervention to improve family communication. Eur. J. Hum. Genet. 2016, 24, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, J.M.; Metcalfe, S.A.; Aitken, M.; Donath, S.M.; Gaff, C.L.; Winship, I.M.; Delatycki, M.B.; Skene, L.L.; McClaren, B.J.; Paul, J.L.; et al. Improving family communication after a new genetic diagnosis: A randomised controlled trial of a genetic counselling intervention. BMC Med. Genet. 2014, 15, 33. [Google Scholar] [CrossRef]
- Eisler, I.; Ellison, M.; Flinter, F.; Grey, J.; Hutchison, S.; Jackson, C.; Longworth, L.; MacLeod, R.; McAllister, M.; Metcalfe, A.; et al. Developing an intervention to facilitate family communication about inherited genetic conditions, and training genetic counsellors in its delivery. Eur. J. Hum. Genet. 2016, 24, 794–802. [Google Scholar] [CrossRef]
- Montgomery, S.V.; Barsevick, A.M.; Egleston, B.L.; Bingler, R.; Ruth, K.; Miller, S.M.; Malick, J.; Cescon, T.P.; Daly, M.B. Preparing individuals to communicate genetic test results to their relatives: Report of a randomized control trial. Fam. Cancer 2013, 12, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Bodurtha, J.N.; McClish, D.; Gyure, M.; Corona, R.; Krist, A.H.; Rodríguez, V.M.; Maibauer, A.M.; Borzelleca, J.; Bowen, D.J.; Quillin, J.M. The KinFact Intervention—A Randomized Controlled Trial to Increase Family Communication About Cancer History. J. Women’s Heal. 2014, 23, 806–816. [Google Scholar] [CrossRef]
- Kardashian, A.; Fehniger, J.; Creasman, J.; Cheung, E.; Beattie, M.S. A Pilot study of the Sharing Risk Information Tool (ShaRIT) for Families with Hereditary Breast and Ovarian Cancer Syndrome. Hered. Cancer Clin. Pr. 2012, 10, 4. [Google Scholar] [CrossRef]
- Smith, R.A. Picking a Frame for Communicating About Genetics: Stigmas or Challenges. J. Genet. Couns. 2007, 16, 289–298. [Google Scholar] [CrossRef]
- Mendes, Á.; Chiquelho, R.; Santos, T.A.; Sousa, L. Supporting families in genetic counselling services: A psychoeducational multifamily discussion group for at-risk colorectal cancer families. J. Fam. Ther. 2015, 37, 343–360. [Google Scholar] [CrossRef]
- Mendes, Álvaro; Chiquelho, R.; Santos, T.A.; Sousa, L. Family matters: Examining a multi-family group intervention for women with BRCA mutations in the scope of genetic counselling. J. Community Genet. 2010, 1, 161–168. [Google Scholar] [CrossRef]
- Katapodi, M.C.; Jung, M.; Schafenacker, A.M.; Milliron, K.J.; E Mendelsohn-Victor, K.; Merajver, S.D.; Northouse, L.L.; Underhill, M.; Son, Y.A. Development of a Web-based Family Intervention for BRCA Carriers and Their Biological Relatives: Acceptability, Feasibility, and Usability Study. JMIR Cancer 2018, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Pearson, J.; McGregor, S.; Cawsey, A.J.; Barrett, A.; Craig, N.; Atkinson, J.M.; Gilmour, W.H.; McEwen, J. Randomised trial of personalised computer based information for cancer patients. BMJ 1999, 319, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Seven, M.; Shah, L.L.; Daack-Hirsch, S.; Yazici, H. Experiences of BRCA1/2 Gene Mutation–Positive Women with Cancer in Communicating Genetic Risk to Their Relatives. Cancer Nurs. 2021, 44, E142–E150. [Google Scholar] [CrossRef]
- Myers, M.; Conrad, P.; Blanco, A.; Terdiman, J. Kintalk: A novel web based communication tool for families with Lynch syndrome to share genetic information. Fam. Cancer 2013, 12, 800. [Google Scholar]
- Myers, M.; Conrad, P.; Terdiman, J. Kintalk.org: Helping Families Communicate Their Genetic Information. Curr. Oncol. 2014, 21, e363. [Google Scholar]
- Hampel, H. Genetic counseling and cascade genetic testing in Lynch syndrome. Fam. Cancer 2016, 15, 423–427. [Google Scholar] [CrossRef]
- Lynch, H.T.; Snyder, C.; Stacey, M.; Olson, B.; Peterson, S.; Buxbaum, S.; Shaw, T.; Lynch, P. Communication and technology in genetic counseling for familial cancer. Clin. Genet. 2014, 85, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Kruk, M.E.; Kelley, E.; Syed, S.B.; Tarp, F.; Addison, T.; Akachi, Y. Measuring quality of health-care services: What is known and where are the gaps? Bull. World Heal. Organ. 2017, 95, 389–389A. [Google Scholar] [CrossRef]
- Jooma, S.; Hahn, M.J.; Hindorff, L.A.; Bonham, V.L. Defining and achieving health equity in genomic medicine. Ethn. Dis. 2019, 29 (Suppl. 1), 173. [Google Scholar] [CrossRef]
- Metcalfe, A. Sharing Genetic Risk Information: Implications for Family Nurses Across the Life Span. J. Fam. Nurs. 2018, 24, 86–105. [Google Scholar] [CrossRef] [PubMed]
- Keenan, K.F.; Simpson, S.A.; Wilson, B.J.; van Teijlingen, E.R.; McKee, L.; Haites, N.; Matthews, E. ’It’s their blood not mine’: Who’s responsible for (not) telling relatives about genetic risk? Health Risk Soc. 2005, 7, 209–226. [Google Scholar] [CrossRef]
- Clarke, A.J.; Wallgren-Pettersson, C. Ethics in genetic counselling. J. Community Genet. 2019, 10, 3–33. [Google Scholar] [CrossRef]
- Seymour, K.C.; Addington-Hall, J.; Lucassen, A.M.; Foster, C.L. What Facilitates or Impedes Family Communication Following Genetic Testing for Cancer Risk? A Systematic Review and Meta-Synthesis of Primary Qualitative Research. J. Genet. Couns. 2010, 19, 330–342. [Google Scholar] [CrossRef]
- Gaff, C.L.; Clarke, A.J.; Atkinson, P.; Sivell, S.; Elwyn, G.; Iredale, R.; Thornton, H.; Dundon, J.; Shaw, C.; Edwards, A. Process and outcome in communication of genetic information within families: A systematic review. Eur. J. Hum. Genet. 2007, 15, 999–1011. [Google Scholar] [CrossRef] [PubMed]
- Goldman, A.; Metcalfe, A.; MacLeod, R. The Process of Disclosure: Mothers’ Experiences of Communicating X-Linked Carrier Risk Information to At-Risk Daughters. J. Genet. Couns. 2018, 27, 1265–1274. [Google Scholar] [CrossRef]
- McAllister, M.; Dearing, A. Patient reported outcomes and patient empowerment in clinical genetics services. Clin. Genet. 2014, 88, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Poushter, J. Smartphone Ownership and Internet Usage Continues to Climb in Emerging Economies but Advanced Economies Still Have Higher Rates of Technology Use. 2016. Available online: http://www.pewglobal.org/2016/02/22/smartphone-ownership-and-internet-usage-continues-to-climb-in-emerging-economies/ (accessed on 14 September 2016).
- Duggan, M. Mobile Messaging and Social Media 2015. Available online: http://www.pewinternet.org/2015/08/19/mobile-messaging-and-social-media-2015/ (accessed on 5 September 2016).
- Ajzen, I. Perceived Behavioral Control, Self-Efficacy, Locus of Control, and the Theory of Planned Behavior1. J. Appl. Soc. Psychol. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Heal. Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Visser, A.; Vrieling, A.; Murugesu, L.; Hoogerbrugge, N.; Kampman, E.; Hoedjes, M. Determinants of adherence to recommendations for cancer prevention among Lynch Syndrome mutation carriers: A qualitative exploration. PLoS ONE 2017, 12, e0178205. [Google Scholar] [CrossRef]
- Borglin, G. The Value of Mixed Methods for Researching Complex Interventions. In Complex Interventions in Health; Routledge: New York, NY, USA, 2015. [Google Scholar]
- Ivankova, N.V.; Creswell, J.W.; Stick, S.L. Using Mixed-Methods Sequential Explanatory Design: From Theory to Practice. Field Methods 2006, 18, 3–20. [Google Scholar] [CrossRef]
- Tashakkori, A.; Teddlie, C. SAGE Handbook of Mixed Methods in Social & Behavioral Research; SAGE Publications, Ltd.: New York, NY, USA, 2010. [Google Scholar]
- Mayoh, J.; Bond, C.S.; Todres, L. An Innovative Mixed Methods Approach to Studying the Online Health Information Seeking Experiences of Adults With Chronic Health Conditions. J. Mix. Methods Res. 2011, 6, 21–33. [Google Scholar] [CrossRef]
- Bryman, A. Integrating quantitative and qualitative research: How is it done? Qual. Res. 2006, 6, 97–113. [Google Scholar] [CrossRef]
- CRD. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; Centre for Reviews and Dissemination: York, UK, 2009. [Google Scholar]
- Bowen, D.J.; Albrecht, T.; Hay, J.; Eggly, S.; Harris-Wei, J.; Meischke, H.; Burke, W. Communication Among Melanoma Family Members. J. Heal. Commun. 2017, 22, 198–204. [Google Scholar] [CrossRef]
- Bowen, D.J.; Hay, J.L.; Harris-Wai, J.N.; Meischke, H.; Burke, W. All in the family? Communication of cancer survivors with their families. Fam. Cancer 2017, 16, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S. Supporting Information Sharing in Families at Risk of Bowel Cancer through a Secure Website. Ph.D. Thesis, University of Plymouth, Plymouth, UK, 2018. [Google Scholar]
- Stern, M.J.; Bilgen, I.; Dillman, D.A. The State of Survey Methodology Challenges, Dilemmas, and New Frontiers in the Era of the Tailored Design. Field Methods 2014, 26, 284–301. [Google Scholar] [CrossRef]
- Creswell, J.W.; Hirose, M. Mixed methods and survey research in family medicine and community health. Fam. Med. Community Heal. 2019, 7, e000086. [Google Scholar] [CrossRef]
- Rea, A.; Marshall, K.; Farrell, D. Capability of web-based survey software: An empirical review. Am. J. Bus. 2021, ahead-of-p. [Google Scholar] [CrossRef]
- Cormier, J.; Iorio-Morin, C.; Mathieu, D.; Ducharme, S. Psychiatric Neurosurgery: A Survey on the Perceptions of Psychiatrists and Residents. Can. J. Neurol. Sci. J. Can. des Sci. Neurol. 2019, 46, 303–310. [Google Scholar] [CrossRef]
- Cohen, S.A.; Leininger, A. The genetic basis of Lynch syndrome and its implications for clinical practice and risk management. Appl. Clin. Genet. 2014, 7, 147–158. [Google Scholar] [CrossRef]
- Boone, H.N.; Boone, D.A. Analyzing likert data. J. Ext. 2012, 50, 1–5. [Google Scholar]
- Joffe, H.; Yardley, L. 4. Content and Thematic Analysis. In Research Methods for Clinical and Health Psychology; Sage: Thousand Oaks, CA, USA, 2004; pp. 56–68. [Google Scholar]
- Leech, N.L.; Onwuegbuzie, A.J. Beyond constant comparison qualitative data analysis: Using NVivo. Sch. Psychol. Q. 2011, 26, 70–84. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. NVivo Qualitative Data analysis Software, 10th ed.; QSR International Pty Ltd: Victoria, Australia, 2012. [Google Scholar]
- Colton, D.; Covert, R.W. Designing and Constructing Instruments for Social Research and Evaluation; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Onwuegbuzie, A.; Collins, K. A Typology of Mixed Methods Sampling Designs in Social Science Research. Qual. Rep. 2015, 12, 281–316. [Google Scholar] [CrossRef]
- Boyatzis, R.E. Transforming Qualitative Information: Thematic Analysis and Code Development; Sage Publications: London, UK, 1998. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Procedures and Techniques for Developing Grounded Theory; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- National Data Guardian. Review of Data Security, Consent and Opt-Outs; UK Government: London, UK, 2016. [Google Scholar]
- Caldicott, F. Caldicott Review: Information Governance in the Health and Care System; National Data Guardian, Ed.; UK Government: London, UK, 2013. [Google Scholar]
- McDermott, L.; The eCRT Research Team; Yardley, L.; Little, P.; Ashworth, M.; Gulliford, M. Developing a computer delivered, theory based intervention for guideline implementation in general practice. BMC Fam. Pr. 2010, 11, 90. [Google Scholar] [CrossRef] [PubMed]
- LogMeIn. GoToMeeting Software Online Platform. 2017. Available online: https://www.logmeininc.com/about-us (accessed on 6 October 2017).
- Sadasivam, R.S.; DeLaughter, K.; Crenshaw, K.; Sobko, H.J.; Williams, J.H.; Coley, H.L.; Ray, M.N.; Ford, D.E.; Allison, J.J.; Houston, T.K.; et al. Development of an Interactive, Web-Delivered System to Increase Provider–Patient Engagement in Smoking Cessation. J. Med. Internet Res. 2011, 13, e87. [Google Scholar] [CrossRef] [PubMed]
- Vaismoradi, M.; Jones, J.; Turunen, H.; Snelgrove, S. Theme development in qualitative content analysis and thematic analysis. J. Nurs. Educ. Pr. 2015, 6, 100. [Google Scholar] [CrossRef]
- Burn, J.; Gerdes, A.-M.; Macrae, F.; Mecklin, J.-P.; Moeslein, G.; Olschwang, S.; Eccles, D.; Evans, D.G.; Maher, E.R.; Bertario, L.; et al. Long-term effect of aspirin on cancer risk in carriers of hereditary colorectal cancer: An analysis from the CAPP2 randomised controlled trial. Lancet 2011, 378, 2081–2087. [Google Scholar] [CrossRef]
- Ouakrim, D.A.; Dashti, S.G.; Chau, R.; Buchanan, D.D.; Clendenning, M.; Rosty, C.; Winship, I.M.; Young, J.P.; Giles, G.; Leggett, B.; et al. Aspirin, Ibuprofen, and the Risk for Colorectal Cancer in Lynch Syndrome. J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef]
- Otten, E.; Plantinga, M.; Birnie, E.; Verkerk, M.A.; Lucassen, A.M.; Ranchor, A.V.; Van Langen, I.M. Is there a duty to recontact in light of new genetic technologies? A systematic review of the literature. Genet. Med. 2014, 17, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Nazi, K.M. The Personal Health Record Paradox: Health Care Professionals’ Perspectives and the Information Ecology of Personal Health Record Systems in Organizational and Clinical Settings. J. Med. Internet Res. 2013, 15, e70. [Google Scholar] [CrossRef] [PubMed]
- Pentz, R.D.; Peterson, S.K.; Watts, B.; Vernon, S.W.; Lynch, P.M.; Koehly, L.M.; Gritz, E.R. Hereditary Nonpolyposis Colorectal Cancer Family Members’ Perceptions about the Duty to Inform and Health Professionals’ Role in Disseminating Genetic Information. Genet. Test. 2005, 9, 261–268. [Google Scholar] [CrossRef]
- Gorrie, A.; Archibald, A.D.; Ioannou, L.; Curnow, L.; McClaren, B. Exploring approaches to facilitate family communication of genetic risk information after cystic fibrosis population carrier screening. J. Community Genet. 2018, 9, 71–80. [Google Scholar] [CrossRef]
- Sustersic, M.; Gauchet, A.; Foote, A.; Bosson, J.-L. How best to use and evaluate Patient Information Leaflets given during a consultation: A systematic review of literature reviews. Heal. Expect. 2016, 20, 531–542. [Google Scholar] [CrossRef]
- Dilzell, K.; Kingham, K.; Ormond, K.; Ladabaum, U. Evaluating the utilization of educational materials in communicating about Lynch syndrome to at-risk relatives. Fam. Cancer 2014, 13, 381–389. [Google Scholar] [CrossRef]
- Metcalfe, A.; Plumridge, G.; Coad, J.; Shanks, A.; Gill, P. Parents’ and children’s communication about genetic risk: A qualitative study, learning from families’ experiences. Eur. J. Hum. Genet. 2011, 19, 640–646. [Google Scholar] [CrossRef] [PubMed]
- McAllister, M. Predictive Genetic Testing and Beyond: A Theory of Engagement. J. Heal. Psychol. 2002, 7, 491–508. [Google Scholar] [CrossRef]
- Lafreniere, D.; Bouchard, K.; Godard, B.; Simard, J.; Dorval, M. Family communication following BRCA1/2 genetic testing: A close look at the process. J. Genet. Couns. 2013, 22, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Koehly, L.M.; Peters, J.A.; Kenen, R.; Hoskins, L.M.; Ersig, A.L.; Kuhn, N.R.; Loud, J.T.; Greene, M.H. Characteristics of Health Information Gatherers, Disseminators, and Blockers Within Families at Risk of Hereditary Cancer: Implications for Family Health Communication Interventions. Am. J. Public Heal. 2009, 99, 2203–2209. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M. Why People Use Health Services. Milbank Q. 2005, 83. [Google Scholar] [CrossRef]
- Stoffel, E.M.; Murphy, C.C. Epidemiology and Mechanisms of the Increasing Incidence of Colon and Rectal Cancers in Young Adults. Gastroenterol. 2020, 158, 341–353. [Google Scholar] [CrossRef]
- Heinlen, C.; Hovick, S.R.; Brock, G.N.; Klamer, B.G.; Toland, A.E.; Senter, L. Exploring genetic counselors’ perceptions of usefulness and intentions to use refined risk models in clinical care based on the Technology Acceptance Model (TAM). J. Genet. Couns. 2019, 28, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Mendes, Á.; Metcalfe, A.; Paneque, M.; Sousa, L.; Clarke, A.J.; Sequeiros, J. Communication of Information about Genetic Risks: Putting Families at the Center. Fam. Process. 2017, 57, 836–846. [Google Scholar] [CrossRef]
- Suthers, G.K.; Armstrong, J.; McCormack, J.; Trott, D. Letting the family know: Balancing ethics and effectiveness when notifying relatives about genetic testing for a familial disorder. J. Med. Genet. 2006, 43, 665–670. [Google Scholar] [CrossRef]
- Aktan-Collan, K.; Haukkala, A.; Pylvanainen, K.; Jarvinen, H.J.; Aaltonen, L.A.; Peltomaki, P.; Rantanen, E.; Kaariainen, H.; Mecklin, J.-P. Direct contact in inviting high-risk members of hereditary colon cancer families to genetic counselling and DNA testing. J. Med. Genet. 2007, 44, 732–738. [Google Scholar] [CrossRef]
- Safarova, M.S.; Kullo, I.J. Lessening the Burden of Familial Hypercholesterolemia Using Health Information Technology. Circ. Res. 2018, 122, 26–27. [Google Scholar] [CrossRef] [PubMed]
- Bental, D.S.; Cawsey, A.; Jones, R. Patient information systems that tailor to the individual. Patient Educ. Couns. 1999, 36, 171–180. [Google Scholar] [CrossRef]
- Jacobs, R.J.; Lou, J.Q.; Ownby, R.L.; Caballero, J. A systematic review of eHealth interventions to improve health literacy. Heal. Inform. J. 2014, 22, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Neuhauser, L.; Kreps, G.L. Online cancer communication: Meeting the literacy, cultural and linguistic needs of diverse audiences. Patient Educ. Couns. 2008, 71, 365–377. [Google Scholar] [CrossRef]
- Norman, M.L.; Malcolmson, J.; Armel, S.R.; Gillies, B.; Ou, B.; Thain, E.; McCuaig, J.M.; Kim, R.H. Stay at home: Implementation and impact of virtualising cancer genetic services during COVID-19. J. Med. Genet. 2020. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.L.; Rahm, A.K.; Zallen, D.T.; Stuckey, H.; Fultz, K.; Fan, A.L.; Bonhag, M.; Feldman, L.; Segal, M.M.; Williams, M.S. Impact of a Patient-Facing Enhanced Genomic Results Report to Improve Understanding, Engagement, and Communication. J. Genet. Couns. 2018, 27, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Clipper, B. The Influence of the COVID-19 Pandemic on Technology: Adoption in Health Care. Nurse Lead. 2020, 18, 500–503. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Interview | Area of Site | Suggestions for Improvement | Changed |
|---|---|---|---|
| #4, #6, #9, #10 | Home page | Need to say what people can do, what they can find on the site, at a glance list showing relevance to users. | Bullet points added with short cuts to provide quick access to different parts of the site. |
| #4, #7 #2, #4 | About Family Web | Banner picture too big, you have to scroll down to see text. More explanation needed about what website function is. | Some pictures removed or reduced in size. Graphic created to show function of the website. |
| #4 | Account information | Banner picture unnecessary, just obscures information | Banner picture removed |
| #7, #12 #1, #6 | Patient sign up | Problems with creating username Need more directions for sign-up | Added statement that username must be in lower case letters Text added to explain account activation needed before use. More detail added to the instructions. |
| #9 #4, #5 | Document sharing | No partner as option in drop down list of relatives Blue folder icon meaningless | ‘Partner’ added as an option to drop-down list Change blue folder icon to ‘Share Files’ |
| #4, #6, #6, #10, #11 #2 #7 | Living your life | Disliked biological mechanisms graphic. Screening very important so wanted more information about it. Information about aspirin & CAPP3 Some pictures distract from the text. | Biological mechanisms graphic moved to another page. Added more information about colonoscopy Information about aspirin added Picture reduced in size |
| #6 | Useful websites | More links to different sites wanted | More websites added, including link to CAPP3 study and NICE guidelines re tumour testing. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goodman, S.; Skirton, H.; Jackson, L.; Jones, R.B. Development of a Secure Website to Facilitate Information Sharing in Families at High Risk of Bowel Cancer—The Familyweb Study. Cancers 2021, 13, 2404. https://doi.org/10.3390/cancers13102404
Goodman S, Skirton H, Jackson L, Jones RB. Development of a Secure Website to Facilitate Information Sharing in Families at High Risk of Bowel Cancer—The Familyweb Study. Cancers. 2021; 13(10):2404. https://doi.org/10.3390/cancers13102404
Chicago/Turabian StyleGoodman, Selina, Heather Skirton, Leigh Jackson, and Ray B. Jones. 2021. "Development of a Secure Website to Facilitate Information Sharing in Families at High Risk of Bowel Cancer—The Familyweb Study" Cancers 13, no. 10: 2404. https://doi.org/10.3390/cancers13102404
APA StyleGoodman, S., Skirton, H., Jackson, L., & Jones, R. B. (2021). Development of a Secure Website to Facilitate Information Sharing in Families at High Risk of Bowel Cancer—The Familyweb Study. Cancers, 13(10), 2404. https://doi.org/10.3390/cancers13102404